Ataxia as the Major Manifestation of Fragile X-Associated Tremor/Ataxia Syndrome (FXTAS): Case Series

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Case Presentation
3.1. Case 1
3.2. Case 2
3.3. Case 3
4. Discussion
4.1. Ataxia in FXTAS
4.2. Evaluation of Ataxia and Contributing Factors for a Faster Progresion in FXTAS
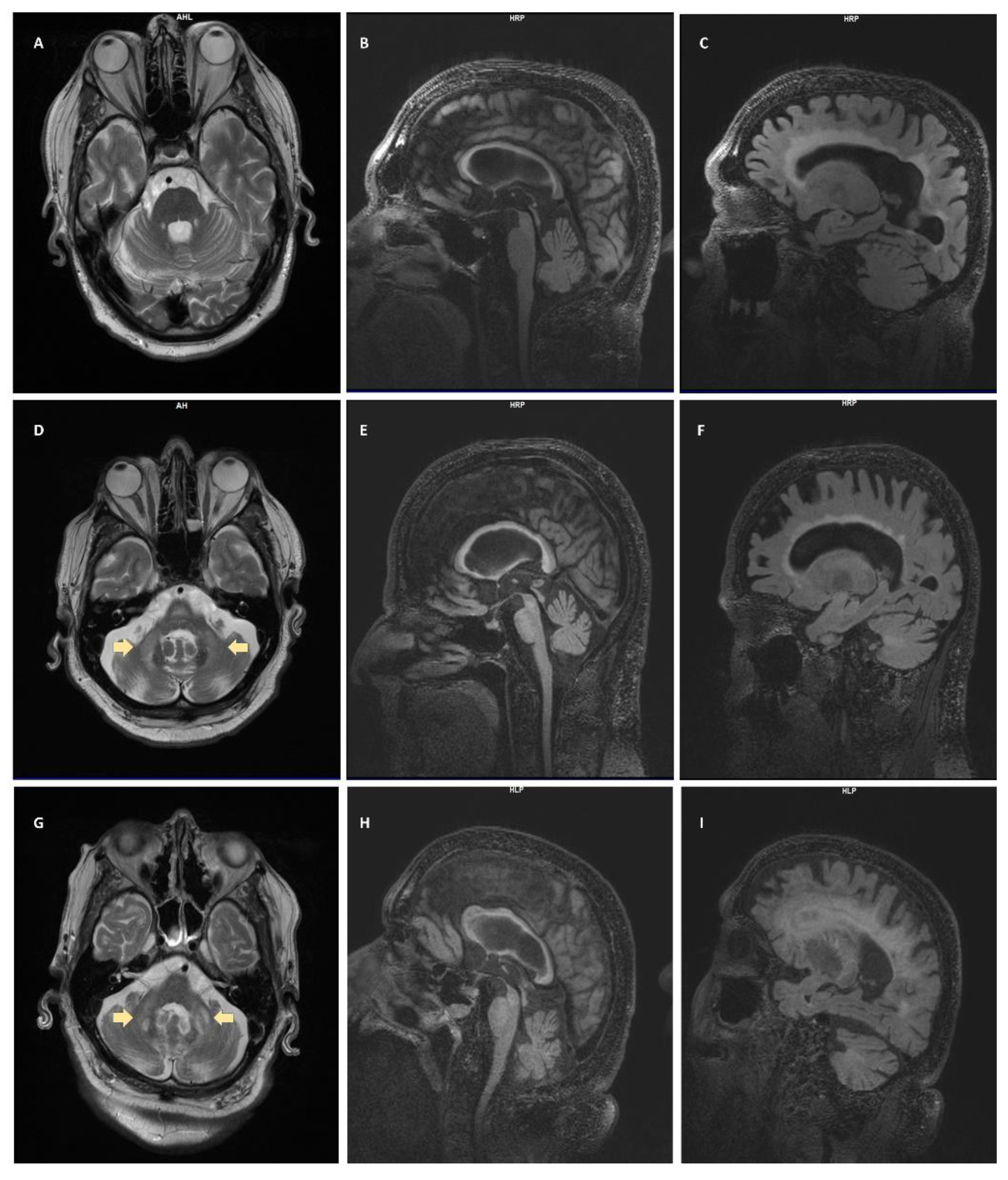
4.3. Neuroradiologic Findings
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hagerman, R.J.; Leehey, M.; Heinrichs, W.; Tassone, F.; Wilson, R.; Hills, J.; Grigsby, J.; Gage, B.; Hagerman, P.J. Intention tremor, parkinsonism, and generalized brain atrophy in male carriers of fragile X. Neurology 2001, 57, 127–130. [Google Scholar] [CrossRef] [PubMed]
- Jacquemont, S.; Hagerman, R.J.; Leehey, M.; Grigsby, J.; Zhang, L.; Brunberg, J.A.; Greco, C.; Des Portes, V.; Jardini, T.; Levine, R.; et al. Fragile X premutation tremor/ataxia syndrome: Molecular, clinical, and neuroimaging correlates. Am. J. Hum. Genet. 2003, 72, 869–878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reiss, A.L.; Freund, L.S.; Baumgardner, T.L.; Abrams, M.T.; Denckla, M.B. Contribution of the FMR1 gene mutation to human intellectual dysfunction. Nat. Genet. 1995, 11, 331–334. [Google Scholar] [CrossRef] [PubMed]
- Tassone, F.; Hagerman, R.J.; Taylor, A.K.; Gane, L.W.; Godfrey, T.E.; Hagerman, P.J. Elevated levels of FMR1 mRNA in carrier males: A new mechanism of involvement in the fragile-X syndrome. Am. J. Hum. Genet. 2000, 66, 6–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hagerman, R.J.; Hagerman, P. Fragile X-associated tremor/ataxia syndrome—Features, mechanisms and management. Nat. Rev. Neurol. 2016, 12, 403–412. [Google Scholar] [CrossRef]
- Jacquemont, S.; Hagerman, R.J.; Leehey, M.; Hall, D.; Levine, R.; Brunberg, J.; Jardini, T.; Gane, L.W.; Harris, S.W.; Herman, K.; et al. Penetrance of the Fragile X–Associated Tremor / Ataxia Syndrome in a Premutation Carrier Population. JAMA 2004, 291, 10. [Google Scholar] [CrossRef] [Green Version]
- Folstein, M.F.; Folestein, S.E.; McHugh, P.R. Mini-mental state: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Drozdick, L.W.; Wahlstrom, D.; Zhu, J.; Weiss, L.G. The Wechsler Adult Intelligence Scale—Fourth Edition and the Wechsler Memory Scale-Fourth Edition. In Contemporary Intellectual Assessment: Theories, Tests, and Issues; Flanagan, D., Harrison, P., Eds.; The Guilford Press: New York, NY, USA, 2012; pp. 197–223. [Google Scholar]
- Grigsby, J.; Kaye, K. Behavioral Dyscontrol Scale: Manual, 2nd ed.; Ward, CO: BDS Denver, CO, USA, 1996. [Google Scholar]
- First, M.; Williams, J.; Karg, R.; Spitzer, R. Structured Clinical Interview for DSM-5—Research Version (SCID-5 for DSM-5, Research Version; SCID-5-RV); American Psychiatric Association: Arlington, VA, USA, 2015. [Google Scholar]
- Bacalman, S.; Farzin, F.; Bourgeois, J.; Cogswell, J.; Goodlin-Jones, B.; Gane, L.; Grigsby, J.; Leehey, M.; Tassone, F.; Hagerman, R. Psychiatric Phenotype of the Fragile X-Associated Tremor/Ataxia Syndrome (FXTAS) in Males: Newly Described Fronto-Subcortical Dementia. J. Clin. Psychiatry 2006, 67, 87–94. [Google Scholar] [CrossRef]
- Leehey, M.A.; Berry-Kravis, E.; Min, S.-J.; Hall, D.A.; Rice, C.D.; Zhang, L.; Grigsby, J.; Greco, C.M.; Reynolds, A.; Lara, R.; et al. Progression of tremor and ataxia in male carriers of the FMR1 premutation. Mov. Disord. 2007, 22, 203–206. [Google Scholar] [CrossRef]
- Juncos, J.L.; Lazarus, J.T.; Graves-Allen, E.; Shubeck, L.; Rusin, M.; Novak, G.; Hamilton, D.; Rohr, J.; Sherman, S.L. New clinical findings in the fragile X-associated tremor ataxia syndrome (FXTAS). Neurogenetics 2011, 12, 123–135. [Google Scholar] [CrossRef] [Green Version]
- Zhao, C.; Liu, Y.; Wang, Y.; Li, H.; Zhang, B.; Yue, Y.; Zhang, J. A Chinese case of fragile X-associated tremor/ataxia syndrome (FXTAS) with orthostatic tremor:case report and literature review on tremor in FXTAS. BMC Neurol. 2020, 20, 145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leehey, M.A.; Hall, D.A.; Liu, Y.; Hagerman, R.J. Clinical Neurological Phenotype of FXTAS. In FXTAS, FXPOI, and Other Premutation Disorders; Tassone, F., Hall, D.A., Eds.; Springer International Publishing: Berlin/Heidelberg, Germany, 2016; pp. 1–24. [Google Scholar]
- Tassone, F.; Adams, J.; Berry-Kravis, E.M.; Cohen, S.S.; Brusco, A.; Leehey, M.A.; Li, L.; Hagerman, R.J.; Hagerman, P.J. CGG repeat length correlates with age of onset of motor signs of the fragile X-associated tremor/ataxia syndrome (FXTAS). Am. J. Med. Genet. Part B 2007, 144B, 566–569. [Google Scholar] [CrossRef] [PubMed]
- Kamm, C.; Healy, D.G.; Quinn, N.P.; Wüllner, U.; Moller, J.C.; Schols, L.; Geser, F.; Burk, K.; Børglum, A.D.; Pellecchia, M.T.; et al. The fragile X tremor ataxia syndrome in the differential diagnosis of multiple system atrophy: Data from the EMSA Study Group. Brain 2005, 128, 1855–1860. [Google Scholar] [CrossRef] [PubMed]
- Berry-Kravis, E.; Goetz, C.G.; Leehey, M.A.; Hagerman, R.J.; Zhang, L.; Li, L.; Nguyen, D.; Hall, D.A.; Tartaglia, N.; Cogswell, J.; et al. Neuropathic features in fragile X premutation carriers. Am. J. Med. Genet. Part A 2007, 143A, 19–26. [Google Scholar] [CrossRef] [PubMed]
- O’Keefe, J.A.; Robertson, E.E.; Ouyang, B.; Carns, D.; McAsey, A.; Liu, Y.; Swanson, M.; Bernard, B.; Berry-Kravis, E.; Hall, D.A. Cognitive function impacts gait, functional mobility and falls in fragile X-associated tremor/ataxia syndrome. Gait Posture 2018, 66, 288–293. [Google Scholar] [CrossRef] [PubMed]
- Seritan, A.; Cogswell, J.; Grigsby, J. Cognitive Dysfunction in FMR1 Premutation Carriers. Curr. Psychiatry Rev. 2013, 9, 78–84. [Google Scholar]
- Brega, A.; Goodrich, G.; Bennett, R.; Hessl, D.; Engle, K.; Leehey, M.; Bounds, L.; Paulich, M.; Hagerman, R.; Hagerman, P.; et al. The Primary Cognitive Deficit among Males with Fragile X-Associated Tremor/Ataxia Syndrome (FXTAS) is a Dysexecutive Syndrome. J. Clin. Exp. Neuropsychol. 2008, 30, 853–869. [Google Scholar] [CrossRef]
- O’Keefe, J.A.; Robertson-Dick, E.E.; Hall, D.A.; Berry-Kravis, E. Gait and Functional Mobility Deficits in Fragile X-Associated Tremor/Ataxia Syndrome. Cerebellum 2016, 15, 475–482. [Google Scholar] [CrossRef]
- Jacquemont, S.; Leehey, M.A.; Hagerman, R.J.; Beckett, L.A.; Hagerman, P.J. Size bias of fragile X premutation alleles in late-onset movement disorders. J. Med. Genet. 2006, 43, 804–809. [Google Scholar] [CrossRef] [Green Version]
- Leehey, M.A.; Berry-Kravis, E.; Goetz, C.G.; Zhang, L.; Hall, D.A.; Li, L.; Rice, C.D.; Lara, R.; Cogswell, J.; Reynolds, A.; et al. FMR1 CGG repeat length predicts motor dysfunction in premutation carriers. Neurology 2008, 70, 1397–1402. [Google Scholar] [CrossRef]
- Birch, R.C.; Hocking, D.R.; Cornish, K.M.; Menant, J.C.; Georgiou-Karistianis, N.; Godler, D.E.; Wen, W.; Hackett, A.; Rogers, C.; Trollor, J.N. Preliminary evidence of an effect of cerebellar volume on postural sway in FMR1 premutation males. Genes Brain Behav. 2015, 14, 251–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seaquist, E.R. The Final Frontier: How Does Diabetes Affect the Brain? Diabetes 2010, 59, 4–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hajjar, I.; Quach, L.; Yang, F.; Chaves, P.H.; Newman, A.B.; Mukamal, K.; Longstreth, W., Jr.; Inzitari, M.; Lipsitz, L.A. Hypertension, White Matter Hyperintensities, and Concurrent Impairments in Mobility, Cognition, and Mood. Circulation 2011, 123, 858–865. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.; Yun, C.-H.; Thomas, R.J.; Lee, S.H.; Seo, H.S.; Cho, E.R.; Lee, S.K.; Yoon, D.W.; Suh, S.; Shin, C. Obstructive Sleep Apnea as a Risk Factor for Cerebral White Matter Change in a Middle-Aged and Older General Population. Sleep 2013, 36, 709–715. [Google Scholar] [CrossRef] [PubMed]
- Sachdev, P.S. Homocysteine and brain atrophy. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2005, 29, 1152–1161. [Google Scholar] [CrossRef] [PubMed]
- Ligsay, A.; El-Deeb, M.; Salcedo-Arellano, M.J.; Schloemerkemper, N.; Grayson, J.S.; Hagerman, R. General Anesthetic Use in Fragile X Spectrum Disorders. J. Neurosurg. Anesthesiol. 2019, 31, 285–290. [Google Scholar] [CrossRef]
- Muzar, Z.; Adams, P.E.; Schneider, A.; Hagerman, R.J.; Lozano, R. Addictive substances may induce a rapid neurological deterioration in fragile X-associated tremor ataxia syndrome: A report of two cases. Intractable Rare Dis. Res. 2014, 3, 162–165. [Google Scholar] [CrossRef] [Green Version]
- Hall, D.A.; Birch, R.C.; Anheim, M.; Jønch, A.E.; Pintado, E.; O’Keefe, J.; Trollor, J.N.; Stebbins, G.T.; Hagerman, R.J.; Fahn, S.; et al. Emerging topics in FXTAS. J. Neurodev. Disord. 2014, 6, 31. [Google Scholar] [CrossRef] [Green Version]
- Famula, J.L.; McKenzie, F.; McLennan, Y.A.; Grigsby, J.; Tassone, F.; Hessl, D.; Rivera, S.M.; Martinez-Cerdeno, V.; Hagerman, R.J. Presence of middle cerebellar peduncle sign in FMR1 premutation carriers without tremor and ataxia. Front. Neurol. 2018, 9, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Adams, J.S.; Adams, P.E.; Nguyen, D.; Brunberg, J.A.; Tassone, F.; Zhang, W.; Koldewyn, K.; Rivera, S.M.; Grigsby, J.; Zhang, L.; et al. Volumetric brain changes in females with fragile X-associated tremor/ataxia syndrome (FXTAS). Neurology 2007, 69, 851–859. [Google Scholar] [CrossRef]
- Renaud, M.; Perriard, J.; Coudray, S.; Sévin-Allouet, M.; Marcel, C.; Meissner, W.G.; Chanson, J.-B.; Collongues, N.; Philippi, N.; Gebus, O.; et al. Relevance of corpus callosum splenium versus middle cerebellar peduncle hyperintensity for FXTAS diagnosis in clinical practice. J. Neurol. 2015, 262, 435–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hermanson, M.; Jhaveri, M.; Stebbins, G.; Dunn, E.; Merkitch, D.; Berry-Kravis, E.; Hall, D. The Splenium of the Corpus Callosum Sign in Fragile X associated Tremor Ataxia Syndrome (FXTAS) (P2.125). Neurology 2015, 84, P2–P125. [Google Scholar]
- Hall, D.A.; Robertson, E.; Shelton, A.L.; Losh, M.C.; Mila, M.; Moreno, E.G.; Gomez-Anson, B.; Martínez-Cerdeño, V.; Grigsby, J.; Lozano, R.; et al. Update on the Clinical, Radiographic, and Neurobehavioral Manifestations in FXTAS and FMR1 Premutation Carriers. Cerebellum 2016, 15, 578–586. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.Y.; Hagerman, R.J.; Rivera, S.M. A multimodal imaging analysis of subcortical gray matter in fragile X premutation carriers. Mov. Disord. 2013, 28, 1278–1284. [Google Scholar] [CrossRef]
- Hashimoto, R.; Javan, A.K.; Tassone, F.; Hagerman, R.J.; Rivera, S.M. A voxel-based morphometry study of grey matter loss in fragile X-associated tremor/ataxia syndrome. Brain 2011, 134, 863–878. [Google Scholar] [CrossRef] [Green Version]
- Cohen, S.; Masyn, K.; Adams, J.; Hessl, D.; Rivera, S.; Tassone, F.; Brunberg, J.; DeCarli, C.; Zhang, L.; Cogswell, J.; et al. Molecular and imaging correlates of the fragile X–associated tremor/ataxia syndrome. Neurology 2006, 67, 1426–1431. [Google Scholar] [CrossRef]
- Brunberg, J.A.; Jacquemont, S.; Hagerman, R.J.; Berry-Kravis, E.M.; Grigsby, J.; Leehey, M.A.; Tassone, F.; Brown, W.T.; Greco, C.M.; Hagerman, P.J. Fragile X Premutation Carriers: Characteristic MR Imaging Findings of Adult Male Patients with Progressive Cerebellar and Cognitive Dysfunction. Am. J. Neuroradiol. 2002, 23, 1757–1766. [Google Scholar]
- Ariza, J.; Steward, C.; Rueckert, F.; Widdison, M.; Coffman, R.; Afjei, A.; Noctor, S.C.; Hagerman, R.; Hagerman, P.; Martínez-Cerdeño, V. Dysregulated iron metabolism in the choroid plexus in fragile X-associated tremor/ataxia syndrome. Brain Res. 2015, 1598, 88–96. [Google Scholar] [CrossRef] [Green Version]
- Ariza, J.; Rogers, H.; Hartvigsen, A.; Snell, M.; Dill, M.; Judd, D.; Hagerman, P.; Martínez-Cerdeño, V. Iron accumulation and dysregulation in the putamen in fragile X-associated tremor/ataxia syndrome. Mov. Disord. 2017, 32, 585–591. [Google Scholar] [CrossRef]
- Wang, J.Y.; Hessl, D.; Iwahashi, C.; Cheung, K.; Schneider, A.; Hagerman, R.J.; Hagerman, P.J.; Rivera, S.M. Influence of the fragile X mental retardation (FMR1) gene on the brain and working memory in men with normal FMR1 alleles. Neuroimage 2013, 65, 288–298. [Google Scholar] [CrossRef] [Green Version]
- Hashimoto, R.; Srivastava, S.; Tassone, F.; Hagerman, R.J.; Rivera, S.M. Diffusion tensor imaging in male premutation carriers of the fragile X mental retardation gene. Mov. Disord. 2011, 26, 1329–1336. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Case | CGG Repeat Size | Age of Onset | Presenting Neurologic Symptom | Additional Medical Conditions | Labs | MRI Findings | Current FXTAS Stage |
|---|---|---|---|---|---|---|---|
| 1 | 126 | 57 | Gait problems | Skeletal hyperostosis, sleep apnea, erectile dysfunction, minor depression | CBC: normal CMP: normal Homocysteine: 9.2 TSH: normal HbA1C: 5.9% | Ventriculomegaly, WMD, splenium sign, mild–moderate cerebral atrophy | III |
| 2 | 94 | 63 | Gait and balance problems | GERD, hypertension, type 2 DM, hearing loss, swallowing problems | CBC: normal CMP: normal Homocysteine: 14.3 (high) TSH: normal HbA1C: 6.2% | MCP sign, WMD, splenium and genu sign, thinning of corpus callosum ventriculomegaly, prominent perivascular spaces | V |
| 3 | 91 | 62 | Ataxia | CAD, hypertension, hypercholesterolemia, anxiety, irritability, moderate dementia | CBC: normal CMP: normal Homocysteine: 10.7 TSH: normal HbA1C: 6.3% | WMD, splenium sign, cortical atrophy, MCP sign | V |
| Case | BDS-2 | WAIS-IV FSIQ | MMSE | Handedness | Kinesia Rest Tremor | Kinesia Postural Tremor | Kinesia Kinetic Tremor |
|---|---|---|---|---|---|---|---|
| 1 | 20/27 | 107 | 29/30 | Right | RH: 0.06 LH: 0.13 | RH: 0.00 LH: 0.00 | RH: 1.89 LH: 1.89 |
| 2 | 15/27 | 90 | 27/30 | Right | RH: 0.24 LH: 0.23 | RH: 0.22 LH: 0.38 | RH: 1.58 LH: 1.10 |
| 3 | 4/27 | 67 | 18/30 | Left | RH: 0.19 LH: 0.00 | RH: 0.17 LH: 0.04 | RH: 1.28 LH: 1.17 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salcedo-Arellano, M.J.; Cabal-Herrera, A.M.; Tassanakijpanich, N.; McLennan, Y.A.; Hagerman, R.J. Ataxia as the Major Manifestation of Fragile X-Associated Tremor/Ataxia Syndrome (FXTAS): Case Series. Biomedicines 2020, 8, 136. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines8050136
Salcedo-Arellano MJ, Cabal-Herrera AM, Tassanakijpanich N, McLennan YA, Hagerman RJ. Ataxia as the Major Manifestation of Fragile X-Associated Tremor/Ataxia Syndrome (FXTAS): Case Series. Biomedicines. 2020; 8(5):136. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines8050136
Chicago/Turabian StyleSalcedo-Arellano, Maria Jimena, Ana Maria Cabal-Herrera, Nattaporn Tassanakijpanich, Yingratana A. McLennan, and Randi J. Hagerman. 2020. "Ataxia as the Major Manifestation of Fragile X-Associated Tremor/Ataxia Syndrome (FXTAS): Case Series" Biomedicines 8, no. 5: 136. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines8050136