Obesity and Diabetes: A Sword of Damocles for Future Generations


Department of Pediatrics, University of Chieti, 66100 Chieti, Italy
*
Author to whom correspondence should be addressed.
Biomedicines 2020, 8(11), 478; https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines8110478
Submission received: 14 October 2020
/
Revised: 2 November 2020
/
Accepted: 3 November 2020
/
Published: 6 November 2020
(This article belongs to the Section Molecular and Translational Medicine)
Abstract
:Childhood obesity is one of the most challenging problem of the 21st century. The prevalence has increased, reaching an alarming rate. Furthermore, the problem is global and is also affecting low- and middle-income countries. This global obesity epidemic explains how the roots of cardiovascular disease, the most common cause of mortality among adults, begin in childhood. Overweight and obese children are likely to stay obese into adulthood and to develop noncommunicable diseases such as diabetes and cardiovascular diseases at a younger age. Thus, prevention should be the major goal and should start early in life. The aim of this review is to present an updated framework of the current understanding of the cardiovascular and metabolic risks in obese children and adolescents and to discuss the available therapeutic options.
1. Introduction
Obesity is a multifactorial disease and various genetic, behavioural and sociocultural characteristics can affect its development [1]. The prevalence of obesity in children and youth has reached dramatic dimensions globally and still remains one of the most challenging problems in developed countries [2]. The Global Burden of Disease Study has presented data according to which the prevalence of childhood obesity has doubled in more than 70 countries since 1980 [3]. This global obesity epidemic explains how the roots of cardiovascular disease, the most common cause of mortality among adults, begin in childhood [4]. One predictor of future cardiovascular risk is the Metabolic Syndrome (MetS) [2], a cluster of cardiovascular risk factors including central obesity, hypertension, dyslipidemia and dysglicemia [5]. Furthermore, MetS also correlates with the risk of type 2 diabetes (T2D) [6]. Behavioural and therapeutic interventions have only shown modest success to date. Thus, the prevention of obesity should be the major goal and should start early in life.
2. Definition of Obesity
The World Health Organization (WHO) defines obesity as an excess in the fat mass that is great enough to increase the risk of morbidity, altered physical, psychological or social well-being, and/or mortality [7]. The body mass index (BMI) shows a good correlation with body fat percentage and is used as an index of relative weight [8]; as is well known, the BMI is calculated by dividing the body weight in kilograms by the height in square meters. In general, the BMI estimates adiposity in healthy children, but it may slightly overestimate fatness in children who are short or who have a relatively high muscle mass, and it may underestimate adiposity in children with reduced muscle mass [9]. The BMI of children changes with age in relation to growth, and, consequently, classification is based on the child BMI compared to the age and sex standard, expressed as the Z score [10]. BMI reference standards for children between two and 20 years of age were published in 2000 by the National Center for Health Statistics and the Center for Disease Control and Prevention (CDC) [11]. The WHO also defined BMI cut-offs for children under two years of age [12]. The CDC recommends the use of curves based on the WHO child growth standard for children and toddlers younger than two years and the CDC/National Center for Health Statistics growth references for children two years and older [11,13]. The ability for any of the various childhood BMI cut-offs to predict the presence of adult cardiovascular risk factors or disease remains largely unknown [14]. In some studies, the waist circumference (WC) and waist:height ratio (WHtR) have been shown to predict cardio-metabolic risk, correlating more strongly than BMI with several complications such as insulin resistance (IR), dyslipidemia and nonalcoholic fatty liver disease [15]. It would seem reasonable to include the WC and WHtR calculation in the routine evaluation of overweight and obese children in order to assess abdominal adiposity [14].
3. Epidemiology of Childhood and Adolescent Obesity
In recent decades, obesity in children and adolescents has emerged as a serious health issue worldwide [1]. The Global Burden of Disease Study has systematically evaluated the prevalence of childhood overweight and obesity since 1980 and has shown that obesity prevalence has doubled in more than 70 countries worldwide and has approximately tripled in some developing countries since then [16,17]. In particular, in developed countries the prevalence also increased from 16.9% in 1980 to 23.8% in 2013 for boys and from 16.2% in 1980 to 22.6% in 2013 for girls [3]. In developing countries, the prevalence of overweight and obesity reached 12.9% for boys and 13.4% for girls in 2013 compared with 8.1% for boys and 8.4% for girls in 1980 [3]. In 2015, a total of 107.7 million children (and 603.7 million adults) were classified as obese, corresponding to a worldwide prevalence of childhood overweight and obesity of 23% [16,18]. Furthermore, the prevalence of obesity varies by age: 8.4% of preschool children (age, 2–5 years), 17.7% of school-age children (age, 6–11 years) and 20.5% of adolescents (age, 12–18 years) have obesity in the United States of America (USA) [19]. Despite the recent plateau in the overall prevalence of childhood obesity in the USA, the prevalence of severe obesity (defined in this report as BMI ≥ 95th percentile or BMI ≥ 35 kg/m2) has continued to increase, leading to the emergence of multiple serious comorbidities [19,20]. Obesity-associated comorbidities are primarily related to cardio-metabolic disease and represent the most significant economic and social public health burden of the obesity epidemic [21]. In fact, in 2015 obesity accounted for about four millions deaths worldwide, and 70% were due to cardiovascular disease (CVD) [16,22]. Unfortunately, a high percentage of children with obesity carry their adiposity into adulthood, especially those with the most severe degrees of obesity and those in older age groups [13]. In addition, it has been described that 71% of adolescents with severe obesity continued to have severe obesity in adulthood compared with only 8% of adolescents with mild obesity [23]. As obesity tends to track into adulthood, it is mandatory that prevention and intervention strategies should begin at the earliest possible age [24].
4. Etiology of Obesity
On the basis of etiology, childhood obesity can be subdivided into exogenous and endogenous types [25]. A chronic imbalance between energy intake and expenditure is the cause of exogenous obesity; at variance, endogenous obesity is caused by genetic, syndromic and endocrine causes [25]. To date, children live in an increasingly obesogenic environment where gaining excessive weight is very easy [25]. Children have unhealthy dietary habits (e.g., the consumption of energy-dense food, sugar-sweetened beverages, poor intake of fruits and vegetables, excessive snacking) associated with a lack of physical activity, increased television viewing time and reduced sleep time. These obesogenic individual behaviours are linked to surrounding microenvironments, including family, schools and neighbourhoods and to macroenvironments like the food industries and government [26]. The Task Force for Pediatric Obesity of the Endocrine Society has described obesity-associated endocrine causes or syndromic conditions [27]. Thus, it is important to identify endocrine and syndromic causes in order to manage these specific conditions. Red flags for pathologic obesity that may warrant further investigation include a rapid onset of weight gain, very early age of onset, obesity discordant with parent weights, hypogonadism, short stature/poor linear growth, and the association of dysmorphic features or developmental delay [20]. Physicians should test for endocrine causes (e.g., hypothyroidism, Cushing syndrome, growth hormone deficiency) of obesity when there is evidence of stunted growth relative to the individual’s genetic potential and when there is a decreased growth velocity against the backdrop of a continued weight gain [28]. Among monogenic defects affecting the leptin-melanocortin regulating pathway, the most common are MCR4 mutations (affecting 4% of early onset and childhood severe obesity) [29]. Genetic syndromes generally show characteristic dysmorphic features and/or neurocognitive delay (e.g., Prader–Willi, Bardet–Biedl, WAGR syndrome) [30].
5. Obesity and Cardiovascular Risk
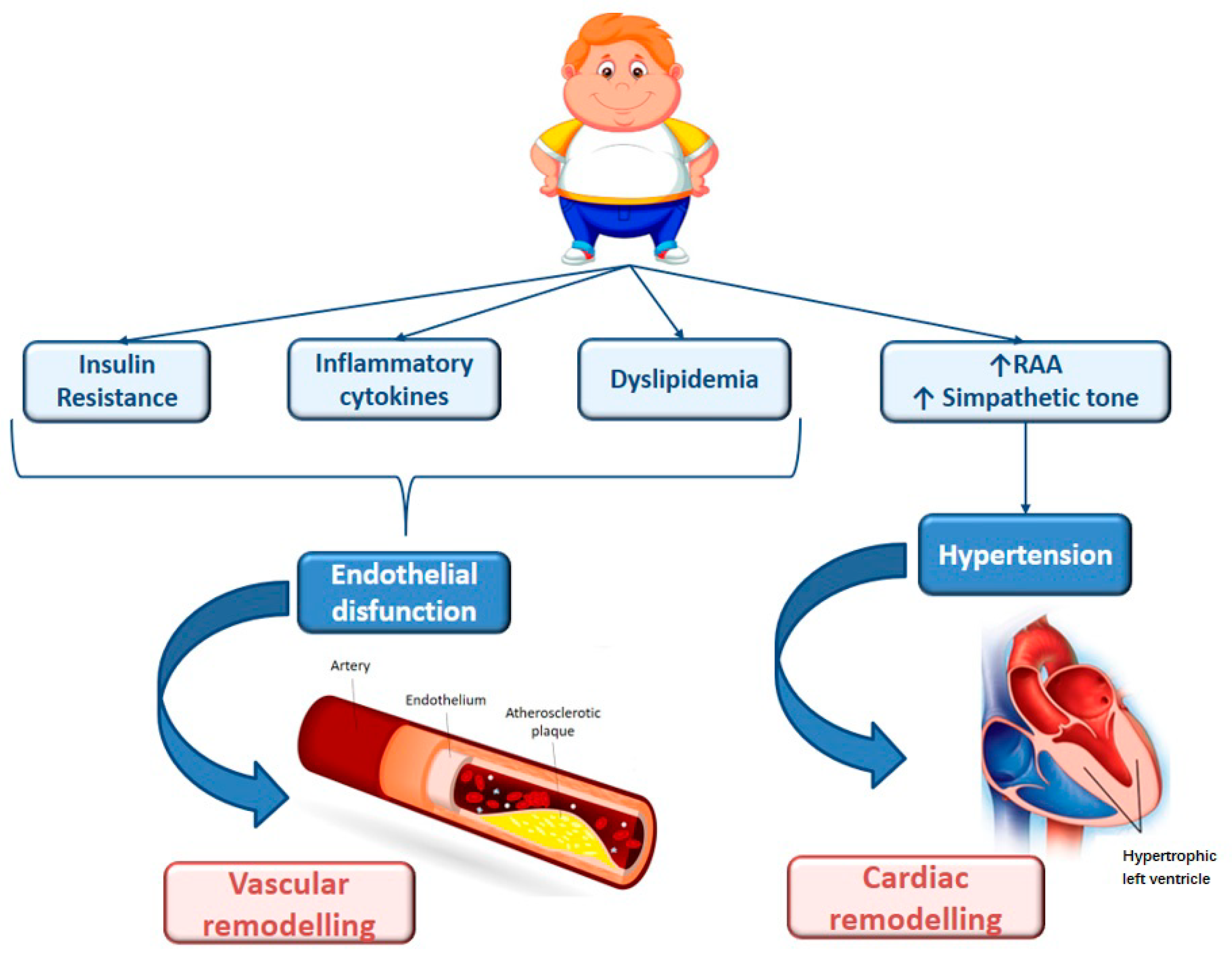
One of the important health implications of obesity in children includes the development of CVD risk factors during childhood and adolescence [31]. CVD is the leading cause of global mortality, accounting for 17.5 million deaths in 2005, and it is projected to rise to 23.6 million deaths by 2030 [32]. Although atherosclerosis manifests clinically in middle and late adulthood, it is well-known that it has a long asymptomatic phase of development, which begins early in life, often during childhood and adolescence [33]. Atherosclerosis begins in childhood with the so called “fatty-streaks” in the intima media of arteries, which may progress into fibrous plaque. The buildup of arterial plaques or their rupture often leads to symptoms of CVD such as angina, myocardial infarction and stroke [33,34]. The first signs of atherosclerosis are described as occurring starting from pregnancy. In fact, foetal studies documented the presence of fatty streak formation in human foetal arteries in over 50% of foetuses of hypercholesterolemic mothers [35]. Moreover, the Fate of early lesion in children (FELIC) study demonstrated that atherosclerosis in children of hypercholesterolemic mothers progresses much more rapidly than it did for children of mothers who had normal cholesterol levels [36]. It seems that foetal lesion formation is associated with genetic programming, which may in turn affect postnatal atherogenesis, supporting the important role of epigenetics in this mechanism [37]. Furthermore, observational studies from autopsies have helped to define the timing, extent and severity of atherosclerotic lesions. In particular, fatty streaks are present from early childhood and are well-established by 20 or 30 years of age, while raised plaques increase in terms of prevalence and extent during the 15–34 year age span [38]. The Bogalusa Heart Study examined the extent of fatty streaks and fibrous plaques in the aorta and coronary arteries of 204 patients (aged 2–39 years) [4]. The prevalence and the extent of atherosclerosis was greater with increasing age, BMI, blood pressure and levels of serum total cholesterol (TC) and low-density lipoprotein cholesterol (LDL-C). In a larger multicentre study of 2876 autopsied young persons aged 15–34 years, the Pathobiological Determinants of Atherosclerosis in Youth (PDAY), obesity was an independent and a prominent risk factor for fatty streaks [39]. The extent of atherosclerotic lesions was associated with a high level of LDL-C and low high-density cholesterol (HDL-C), hypertension, obesity and impaired glucose tolerance. In addition to autopsy findings, studies using noninvasive measures, including carotid intima media thickness (cIMT) and arterial distensibility, have shown anatomic and functional changes of atherosclerosis in youth. cIMT progresses with age and risk factors predict thickness in young adults [40]. The risk factors are the same as those associated with advanced lesions: increased BMI, hypertension, dyslipidemia, IR and cigarette smoking. However, it is important to discern the independent contribution of childhood obesity to CVD and diabetes. The International Childhood Cardiovascular Cohort consortium demonstrated that childhood obesity is a strong independent risk factor for arterial vascular abnormalities [41]. The pathological association of obesity and CVD may be explained by the so-called “adiposopathy”. Abdominal obesity may be the source of mediators, known as adipocytokines, that induce a condition of IR, systemic inflammation and sympathetic activation that, in turn, leads to vascular and cardiac remodelling [42] (Figure 1). This process may be reversible; children with obesity who transitioned to a normal weight status as adults had a risk comparable to persons who were never obese [43]. Therefore, recognizing this process during childhood is the key to adopting measures that will prevent atherosclerosis and eliminate future cardiovascular-related events [14].
6. Dysglycaemia and Insulin Resistance
Dysglycaemia is a term that includes impaired fasting glucose (IFG), impaired glucose tolerance (IGT) and diabetes [44]. The prevalence of IFG and IGT in adolescents with obesity was 16.8% and 6.6%, respectively [45]. The childhood obesity epidemic is associated with a three-fold increase in the prevalence rates of type 2 diabetes in adolescents and young adults over the last three decades [21]. Using a two-hour glucose threshold of more than 140 mg/dL, up to 21% of obese youth are classified as having prediabetes, with a progression to diabetes of 10–15% per year [46]. The onset of T2D occurs mostly in adulthood, while among children it develops during the second decade of life and in middle to late puberty [47]. The pathogenesis of T2D is linked to obesity combined with insulin deficiency [48]. Global adiposity acts as the most important culprit of IR, which appears early in the disease and is primarily compensated by hyperinsulinemia [47]. The relation between obesity and IR is weaker in African American children because of a higher obesity-independent hyperinsulinemia and a poor β-cell adaptation to IR [49,50]. The mechanisms responsible for the development of IR in obese children are not completely understood [51]. Fatty acids, inflammatory cytokines and growth factor are included in the pathogenesis [52,53,54]. Because of the absence of a standardized method to measure insulin sensitivity, an unanimous definition of IR does not exist [51]. IR could be defined as a condition in which greater concentrations of insulin are needed to determine a physiological effect that was previously induced by a lower concentration [55]. The gold standard technique used to evaluate IR is the hyperinsulinemic-euglycemic clamp; however, it is costly and difficult to perform in clinical and research sets [56]. Therefore, several surrogate markers have been proposed, such as the Matsuda index [57] and Homeostatic Model of Assessment-insulin resistance (HOMA-IR) [58]. However, it was proven that the distribution of fat tissue was the crucial factor for developing IR [59]. Children with a high proportion of visceral fat are more insulin-resistant and have a higher plasma glucose in the second hour of the glucose tolerance test [48,60]. The role of visceral adiposity is particularly determinative in pubertal and postpubertal obese children and adolescents, whereas it is a minor determinant of IR in prepubertal children [61]. In adolescents, it is important to highlight that physiological hormonal modifications are responsible for a transient reduction in the whole body insulin sensitivity, which may resolve at the end of puberty [62,63]. Furthermore, it is important to highlight the “obesity paradox”. Patients with a normal weight at the time of diagnosis of T2D had a higher risk of developing a cardiovascular complication, at variance of people with a higher weight during the onset of diabetes [64]. Diabetes can lead to many complications (CVD, nephropathy, retinopathy and microangiopathy), and obesity in children with T2D increases the risk of cardiovascular complications like myocardial infarction, stroke and renal failure. The cardiovascular risk in youth is related both to comorbidities (dyslipidemia, hypertension, nonalcoholic steatosis) and to the hyperglycaemic effect on the vasculature [21].
Disglycaemia and elevated BMI in children are determinants of adverse arterial wall adaptation through the formation of advanced glycation end products, which can lead to coronary artery calcification and increased cIMT [65]. The rapid nature of T2D in children accelerates the progression of micro- and macrovascular complications, but short-term improvement in glycaemia did not decrease the prevalence of cardio-metabolic risk factors [66]. The risk of microvascular disease and death from cardiovascular disease occurs 10–15 years after the onset of the disease [67,68]. Further studies are needed to identify target therapies to reduce this risk [21].
7. Dyslipidemia
Obese children and adolescents have been observed to have a more unfavourable lipid profile than children and adolescents with a normal body weight [69]. The atherogenic lipid pattern associated with childhood obesity consists of a combination of elevated triglycerides (TG), decreased HDL-C and top normal to mildly elevated LDL-C [70]. Although the pathogenetic mechanism of dyslipidemia is multifactorial and still debated, IR has been hypothesized to play a major role in the relationship between dyslipidemia and insulin obesity [71,72]. Some authors observed that children with a greater degree of IR had a higher risk of developing atherogenic dyslipidemia than those with a moderate IR status [72]. Moreover, it has been demonstrated that the TG/HDL ratio is significantly associated with insulin and early signs of vascular damage in obese children [73,74].
The cause of atherogenesis mainly remains the subendothelial retention of LDL-C containing lipoprotein and the decrease in HDL-C particles [75,76]. Small dense LDL-C (SdLDL) show an increased susceptibility to oxidation, thus promoting endothelial damage and infiltrating the arterial wall [77]. The prevalence of SdLDL correlates with IR and visceral adiposity and shows a strong correlation with the common cIMT [78]. In fact, the atherogenicity of the combined dyslipidemia seen with childhood obesity manifests in structural and functional vascular changes assessed noninvasively as increased cIMT and increased arterial stiffness [79]. The longitudinal Young Finns study revealed that, at 21-year follow-up, subjects with a combined dyslipidemia pattern beginning in childhood had significantly increased cIMT compared with normolipemic controls, even after adjustment for other risk factors [80]. In adults, combined dyslipidemia is the most prevalent pattern seen in individuals presenting with early clinical cardiovascular events [81]. Thus, the combined dyslipidemia pattern seen with obesity in childhood is increasing in prevalence and predicts vascular dysfunction in young adulthood and early clinical events in adult life [82].
8. Hypertension
Hypertension in childhood is defined as either a systolic or diastolic blood pressure value greater than or equal to the 95th percentile for sex, age and height on at least three occasions [83]. Historically, childhood hypertension has been considered a rare condition, secondary to renal, cardiac or endocrine disorders. However, the prevalence of primary hypertension in children and youth has increased in parallel with the growing prevalence of overweight and obesity. In fact, to date, 25% of obese children and adolescents suffer from hypertension [84]. In particular, some authors found that each increase by 10 BMI units was associated with an increase in the systolic blood pressure of 10 mmHg and in the diastolic blood pressure of 3 mmHg [85]. Furthermore, the risk remains as children with obesity progress into adulthood [86].
The pathophysiology of hypertension includes the activation of the sympathetic nervous system and of the renin-angiotensin-aldosterone system (RAAS), which increase the intravascular volume and consequently the ventricular preload [84]. Proinflammatory cytokines and oxidative stress contribute to vascular endothelial dysfunction, an impaired local vasodilator response and increased peripheral resistance, particularly with vascular afterload [85]. These changes may induce alterations and remodelling of large vessels and the heart [87]. Some authors described the fact that obese children had a larger left ventricular mass index and an earlier cardiac impairment (systolic and diastolic dysfunctions) compared to healthy controls [88,89]. Furthermore, repetitive obstructive apneas/hypopneas cause dramatic fluctuations in intrathoracic pressure and blood pressure, increased left ventricular preload, left atrial dilatation, arrhythmias (particularly atrial fibrillation), and left ventricular eccentric hypertrophy [90]. The increased ventricular strain persists into adulthood and raises the risk of CVD, but fortunately it is reversible with the normalization of weight [87]. Thus, a timely diagnosis and initiation of treatment are important to reduce the risk of end-organ damage [85].
9. Liver Steatosis
Nonalcoholic fatty liver disease (NAFLD) is a chronic liver disorder that is increasingly prevalent with the worldwide epidemic of obesity. The term NAFLD describes a spectrum of liver pathology ranges from simple steatosis to nonalcoholic steatohepatitis and even cirrhosis [91]. Pediatric obesity increases the risk of hepatic steatosis and steatohepatitis, so that NAFLD occurs in 34% of youth with obesity [92]. The most credited model for the pathogenesis of NAFLD is the ‘‘two-hit’’ theory, where the first hit is represented by the IR, responsible for the abnormalities in lipid storage and lipolysis, which therefore leads to an increased fatty acids flux from adipose tissue to the liver and to the subsequent accumulation of TG into the hepatocytes [93]. The “second hit” might be represented by the oxidative stress, which activates the inflammatory cascade and generates reactive oxygen species such as hydroxyl radicals and superoxide anions, which react with the excess lipid to form peroxides [94,95]. A large body of emerging literature seems to suggest that intestinal microbiota is also involved in the development of obesity and its complications, including obesity-related liver disease [91]. The diagnosis can be difficult and requires a liver biopsy, but elevated aminotransferase in obese children should prompt the clinician to investigate for NAFLD [96].
10. Metabolic Syndrome
Obesity plays a key role in the development of MetS, a complex picture characterized by a combination of risk factors, such as WC, TG, HDL-C, BP and glucose [87].
Data from multiracial cohorts of children have shown that the degree of obesity and the prevalence of MetS are strongly associated [97]. There is currently no consensus guideline for the diagnostic criteria for paediatric MetS [2]. In fact, more than 40 definitions have been reported in children, and most authors have adapted criteria from the adult population [98] (Table 1). The American Heart Association (AHA) adapts the adult definition to the paediatric population [99]. In 2007, the International Diabetes Federation (IDF) provided a definition of MetS for children aged 10–16 years, while adult criteria were still adopted for children older than 16 years [100]. The Identification and prevention of Dietary and lifestyle-induced health Effects In Children and infantS (IDEFICS) consortium recently provided a definition of paediatric Mets using percentiles for each diagnostic criterion [101]. There is a common agreement to include IR, central obesity, hypertension and dyslipidemia as major components of MetS [101]. However, there are certain limitations to the clinical use of this definition due to different applied criteria, heterogeneous cut-off values and missing values for prepubertal children. In addition, some authors propose to include other features in the definition of MetS, such as nonalcoholic fatty liver disease, hyperuricemia and sleep disturbance [51]. The prevalence of MetS in children and youth has been estimated to differ between 6 and 39% depending on which diagnostic criteria are applied [102]. In addition to the degree of obesity, fat distribution also appears to be important. Visceral fat accumulation, independent of BMI, has been shown to be strongly associated with both childhood MetS and CVD later in life [103].
The pathogenesis of MetS is not fully understood, but central obesity appears to be the central driver [5]. Visceral adipocytes release chemo-attractants and cytokines, leading to systemic inflammation [104]. Furthermore, the reduced production of adiponectin and the higher release of free fatty acids increase the oxidative stress [105]. This in turn reduces insulin’s ability to stimulate glucose transporters to the cell surface, causing IR [6].
11. Lifestyle Changes
Many studies have shown that the weight status in early childhood is a significant predictor for the weight status and associated cardio-metabolic comorbidities later in life [106,107]. Therefore, early intervention could influence future morbidity and mortality as well as improve the quality of life. The first approach to MetS is to try a lifestyle intervention with dietary modifications and increased physical activity [27]. These recommendations are difficult to achieve, especially for adolescents. Thus, the prevention or treatment of childhood obesity should start as early as possible. Due to the fact that therapeutic approaches often only show modest effects, prevention should be the primary goal. The WHO commission suggests individual and community based-prevention strategies to fight the obesity epidemic [108]. Physical activity is not only associated with weight loss but also has a beneficial effect on insulin sensitivity independently from adiposity [109]. The Endocrine Society Clinical Practice Guidelines suggest a minimum of 30 min of moderate to vigorous daily physical activity with a goal of 60 min daily [27]. A combination of low aerobic and resistance exercises is recommended because it seems to improve insulin sensitivity [110]. Furthermore, other health behaviours such as dietary intake and sleeping habits can affect insulin sensitivity. In particular, a short sleep duration (<9 h/day) and sleep apnea are linked to IR [111].
The optimal nutritional management is still debated. The main approach for dietary changes for children and adolescents, recommended by the American Academy of Pediatrics, the AHA and the WHO, is an increase in vegetable and fruit consumption and a reduced intake of saturated fat and sugar [112]. Several studies demonstrated that the consumption of food with a higher fibre intake was associated with a higher insulin sensitivity [113,114]. A diet with a higher fibre intake offers several beneficial effects, such as increased satiety, slowing the absorption of carbohydrates and the bulking effect of adding low-energy food to the diet [115]. Low glycaemic index foods decrease blood glucose and insulin excursion, promote fat oxidation and increase satiety, but their effect on IR is still unclear [116,117]. The most effective interventions are likely to include a combined approach incorporating dietary and physical activity changes [5]. This is due to the fact that an increased energy expenditure may lead to a compensatory increase in food intake [118], while isolated caloric restriction results in a lowering of the basal metabolic rate [119].
12. Pharmacotherapy
Medications are suggested for children and adolescents for whom a lifestyle management of obesity has not resulted in improvement [96]. To date, the only medications approved by the US Food and Drug Administration (FDA) are orlistat and phentermine for adolescents aged >12 years and >16 years, respectively [2]. Metformin has been approved to treat T2D in children 10 years or older, while its effect on weight loss or BMI reduction are rather limited [120]. However, its results show that it is a promising method to improve glucose metabolism and reduce cardio-metabolic risk [121]. Other potential pharmacologic options are glucagon-like peptide-1 (GLP-1) analogues such as liraglutide. They increase the postprandial insulin level, reduce glucagon secretion, delay gastric emptying and induce weight loss through reductions in appetite and energy intake [122]. However, they have been approved by the FDA in addition to lifestyle interventions for the treatment of obese and overweight adults with at least one weight-related coexisting condition [123]. Obese children with dyslipidemia should be treated with statin if a lifestyle modification fails or if LDL levels are higher than 160 mg/dl [27]. If obese children manifest with arterial hypertension, pharmacotherapy might be considered in the second line and should be started with an ACE inhibitor [124].
13. Conclusions
Obesity still remains one of the global burdens in medicine, particularly because of its high prevalence in children and adolescents and its associated cardio-metabolic sequelae [125]. As many obese children remain obese until adulthood and as the first signs of atherosclerosis start in childhood, an early normalization of body weight is becoming necessary and of paramount importance. Regardless of the etiology, all patients should be assessed for modifiable lifestyle risk factors and screened for the complications of obesity [25]. Initial management includes dietary and physical activity changes, while pharmacotherapy is recommended for a small minority of patients. However, intervention strategies have only shown a limited effect to date and cannot prevent long-term consequences [25]. Thus, prevention remains the best approach to halt and reverse the current epidemic of childhood obesity and should start as early in life as possible [2].
Author Contributions
All authors contributed equally to the manuscript and approved the final version ant its submission to the journal.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| MetS | Metabolic Syndrome |
| WHO | World Health Organization |
| BMI | body mass index |
| CDC | Center for Disease Control and Prevention |
| WC | waist circumference |
| WHtR | waist-to-height ratio |
| CVD | cardiovascular disease |
| TC | total cholesterol |
| LDL-C | low-density lipoprotein cholesterol |
| HDL-C | high-density lipoprotein cholesterol |
| PDAY | Pathobiological Determinants of Atherosclerosis in Youth |
| cIMT | carotid intima media thickness |
| IR | insulin resistance |
| IFG | impaired fasting glucose |
| IGT | impaired glucose tolerance |
| T2D | type 2 diabetes |
| HOMA-IR | Homeostatic Model of Assessment-insulin resistance |
| SdLDL-C | Small dense low-density lipoprotein cholesterol |
| TG | triglycerides |
| RAAS | renin-angiotensin-aldosterone system |
| NAFLD | Nonalcoholic fatty liver disease |
| AHA | American Heart Association |
| IDF | International Diabetes Federation |
| IDEFICS | Identification and prevention of Dietary and lifestyle-induced health Effects In Children and infantS |
| FDA | Food and Drug Administration |
| USA | United States of America |
References
- Lee, E.Y.; Yoon, K. Epidemic obesity in children and adolescents: Risk factors and prevention. Front. Med. 2018, 12, 658–666. [Google Scholar] [PubMed]
- Weihe, P.; Weihrauch-Blüher, S. Metabolic Syndrome in Children and Adolescents: Diagnostic Criteria, Therapeutic Options and Perspectives. Curr. Obes. Rep. 2019, 8, 472–479. [Google Scholar] [PubMed]
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F.; et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar]
- Berenson, G.S.; Srinivasan, S.R.; Bao, W.; Newman, W.P.; Tracy, R.E.; Wattigney, W.A. Association between Multiple Cardiovascular Risk Factors and Atherosclerosis in Children and Young Adults. N. Engl. J. Med. 1998, 338, 1650–1656. [Google Scholar] [PubMed]
- DeBoer, M.D. Assessing and Managing the Metabolic Syndrome in Children and Adolescents. Nutrients 2019, 11, 1788. [Google Scholar] [CrossRef] [Green Version]
- Shulman, G.I. Ectopic Fat in Insulin Resistance, Dyslipidemia, and Cardiometabolic Disease. N. Engl. J. Med. 2014, 371, 1131–1141. [Google Scholar]
- Obesity: Preventing and managing the global epidemic. Report of a WHO consultation. World Health Organ Tech Rep Ser. 2000, 894, 1–253. [Google Scholar]
- Deurenberg, P.; Weststrate, J.A.; Seidell, J.C. Body mass index as a measure of body fatness: Age- and sex-specific prediction formulas. Br. J. Nutr. 1991, 65, 105–114. [Google Scholar]
- Javed, A.; Jumean, M.; Murad, M.H.; Okorodudu, D.; Kumar, S.; Somers, V.K.; Sochor, O.; Lopez-Jimenez, F. Diagnostic performance of body mass index to identify obesity as defined by body adiposity in children and adolescents: A systematic review and meta-analysis. Pediatr. Obes. 2014, 10, 234–244. [Google Scholar] [PubMed]
- McPhee, P.G.; Singh, S.; Morrison, K.M. Childhood Obesity and Cardiovascular Disease Risk: Working Toward Solutions. Can. J. Cardiol. 2020, 36, 1352–1361. [Google Scholar]
- Kuczmarski, R.J.; Ogden, C.L.; Grummer-Strawn, L.M.; Flegal, K.M.; Guo, S.S.; Wei, R.; Mei, Z.; Curtin, L.R.; Roche, A.F.; Johnson, C.L. CDC growth charts: United States. Adv. data 2000, 2000, 1–27. [Google Scholar]
- WHO Multicentre Growth Reference Study Group; De Onis, M. WHO Child Growth Standards based on length/height, weight and age. Acta Paediatr. 2007, 95, 76–85. [Google Scholar]
- Kumar, S.; Kelly, A.S. Review of Childhood Obesity. Mayo Clin. Proc. 2017, 92, 251–265. [Google Scholar]
- Ayer, J.; Charakida, M.; Deanfield, J.; Celermajer, D.S. Lifetime risk: Childhood obesity and cardiovascular risk. Eur. Heart J. 2015, 36, 1371–1376. [Google Scholar]
- Qiao, Q.; Nyamdorj, R. The optimal cutoff values and their performance of waist circumference and waist-to-hip ratio for diagnosing type II diabetes. Eur. J. Clin. Nutr. 2009, 64, 23–29. [Google Scholar]
- Weihrauch-Blüher, S.; Wiegand, S. Risk Factors and Implications of Childhood Obesity. Curr. Obes. Rep. 2018, 7, 254–259. [Google Scholar]
- Gregg, E.W.; Shaw, J.E. Global Health Effects of Overweight and Obesity. N. Engl. J. Med. 2017, 377, 80–81. [Google Scholar]
- Weihrauch-Blüher, S.; Schwarz, P.; Klusmann, J.-H. Childhood obesity: Increased risk for cardiometabolic disease and cancer in adulthood. Metabolism 2019, 92, 147–152. [Google Scholar]
- Skinner, A.C.; Skelton, J.A. Prevalence and Trends in Obesity and Severe Obesity Among Children in the United States, 1999–2012. JAMA Pediatr. 2014, 168, 561–566. [Google Scholar]
- Dietz, W.H.; Robinson, T.N. Overweight Children and Adolescents. N. Engl. J. Med. 2005, 352, 2100–2109. [Google Scholar]
- Chung, S.T.; Onuzuruike, A.U.; Magge, S.N. Cardiometabolic risk in obese children. Ann. N. Y. Acad. Sci. 2018, 1411, 166–183. [Google Scholar]
- GBD 2015 Obesity Collaborators; Afshin, A.; Forouzanfar, M.H.; Reitsma, M.B.; Sur, P.; Estep, K.; Lee, A.; Marczak, L.; Mokdad, A.H.; Moradi-Lakeh, M.; et al. Health Effects of Overweight and Obesity in 195 Countries over 25 Years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar]
- Lau, E.Y.; Liu, J.; Archer, E.; McDonald, S.M.; Liu, J. Maternal Weight Gain in Pregnancy and Risk of Obesity among Offspring: A Systematic Review. J. Obes. 2014, 2014, 524939. [Google Scholar]
- Gurnani, M.; Birken, C.; Hamilton, J. Childhood obesity: Causes, consequences, and management. Pediatr. Clin. N. Am. 2015, 62, 821–840. [Google Scholar]
- Aggarwal, B.; Jain, V. Obesity in Children: Definition, Etiology and Approach. Indian J. Pediatr. 2018, 85, 463–471. [Google Scholar]
- Swinburn, B.; Egger, G.; Raza, F. Dissecting Obesogenic Environments: The Development and Application of a Framework for Identifying and Prioritizing Environmental Interventions for Obesity. Prev. Med. 1999, 29, 563–570. [Google Scholar]
- Styne, D.M.; Arslanian, S.A.; Connor, E.L.; Farooqi, I.S.; Murad, M.H.; Silverstein, J.H.; Yanovski, J.A. Pediatric Obesity—Assessment, Treatment, and Prevention: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2017, 102, 709–757. [Google Scholar]
- Greydanus, D.E.; Agana, M.; Kamboj, M.K.; Shebrain, S.; Soares, N.; Eke, R.; Patel, D.R. Pediatric obesity: Current concepts. Dis. Mon. 2018, 64, 98–156. [Google Scholar]
- Vaisse, C.; Clement, K.; Durand, E.; Hercberg, S.; Guy-Grand, B.; Froguel, P. Melanocortin-4 receptor mutations are a frequent and heterogeneous cause of morbid obesity. J. Clin. Investig. 2000, 106, 253–262. [Google Scholar]
- Farooqi, I.S.; O’Rahilly, S. Genetics of Obesity in Humans. Endocr. Rev. 2006, 27, 710–718. [Google Scholar]
- Umer, A.; Kelley, G.A.; Cottrell, L.E.; Jr, P.G.; Innes, K.E.; Lilly, C.L. Childhood obesity and adult cardiovascular disease risk factors: A systematic review with meta-analysis. BMC Public Health 2017, 17, 683. [Google Scholar]
- Benjamin, E.J.; Virani, S.S.; Callaway, C.W.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Chiuve, S.E.; Cushman, M.; Delling, F.N.; Deo, R.; et al. Heart disease and stroke statistics—2017 update a report from the American heart association. Circulation 2017, 135, e146–e603. [Google Scholar]
- Hong, Y.M. Atherosclerotic Cardiovascular Disease Beginning in Childhood. Korean Circ. J. 2010, 40, 1–9. [Google Scholar] [PubMed] [Green Version]
- Wilson, D.P. Is atherosclerosis a pediatric disease? In Endotext [Internet]; MDText.com, Inc.: South Dartmouth, MA, USA, 2000. [Google Scholar]
- Napoli, C.; D’Armiento, F.P.; Mancini, F.P.; Postiglione, A.; Witztum, J.L.; Palumbo, G.; Palinski, W. Fatty streak formation occurs in human fetal aortas and is greatly enhanced by maternal hypercholesterolemia. Intimal accumulation of low density lipoprotein and its oxidation precede monocyte recruitment into early atherosclerotic lesions. J. Clin. Investig. 1997, 100, 2680–2690. [Google Scholar]
- Napoli, C.; Glass, C.K.; Witztum, J.L.; Deutsch, R.; D’Armiento, F.P.; Palinski, W. Influence of maternal hypercholesterolaemia during pregnancy on progression of early atherosclerotic lesions in childhood: Fate of Early Lesions in Children (FELIC) study. Lancet 1999, 354, 1234–1241. [Google Scholar]
- Skilton, M.R. Intrauterine Risk Factors for Precocious Atherosclerosis. Pediatrics 2008, 121, 570–574. [Google Scholar]
- McGill, H.C., Jr.; McMahan, C.A.; Herderick, E.E.; Malcom, G.T.; Tracy, R.E.; Strong, J.P. Origin of atherosclerosis in childhood and adolescence. Am. J. Clin. Nutr. 2000, 72, 1307S–1315S. [Google Scholar]
- Zieske, A.W.; Malcom, G.T.; Strong, J.P. Natural history and risk factors of atherosclerosis in children and youth: The PDAY study. Pediatr. Pathol. Mol. Med. 2002, 21, 213–237. [Google Scholar]
- Park, M.H.; Skow, Á.; De Matteis, S.; Kessel, A.S.; Saxena, S.; Viner, R.M.; Kinra, S. Adiposity and carotid-intima media thickness in children and adolescents: A systematic review. BMC Pediatr. 2015, 15, 161. [Google Scholar]
- Oikonen, M.; Laitinen, T.T.; Magnussen, C.G.; Steinberger, J.; Sinaiko, A.R.; Dwyer, T.; Venn, A.; Smith, K.J.; Hutri-Kähönen, N.; Pahkala, K.; et al. Ideal Cardiovascular Health in Young Adult Populations From the United States, Finland, and Australia and Its Association With cIMT: The International Childhood Cardiovascular Cohort Consortium. J. Am. Heart Assoc. 2013, 2, e000244. [Google Scholar]
- Mangner, N.; Scheuermann, K.; Winzer, E.; Wagner, I.; Hoellriegel, R.; Sandri, M.; Zimmer, M.; Mende, M.; Linke, A.; Kiess, W.; et al. Childhood obesity: Impact on cardiac geometry and function. JACC Cardiovasc. Imaging 2014, 7, 1198–1205. [Google Scholar] [PubMed] [Green Version]
- Peplies, J.; Börnhorst, C.; Günther, K.; Fraterman, A.; Russo, P.; Veidebaum, T.; Tornaritis, M.; De Henauw, S.; Marild, S.; on behalf of the IDEFICS consortium; et al. Longitudinal associations of lifestyle factors and weight status with insulin resistance (HOMA-IR) in preadolescent children: The large prospective cohort study IDEFICS. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 97. [Google Scholar]
- Al Khalifah, R.A.; Thabane, L.; Tarnopolsky, M.A.; Morrison, K.M. The prognosis for glycemic status among children and youth with obesity 2 years after entering a weight management program. Pediatr. Diabetes 2018, 19, 874–881. [Google Scholar]
- Andes, L.J.; Cheng, Y.J.; Rolka, D.B.; Gregg, E.W.; Imperatore, G. Prevalence of Prediabetes Among Adolescents and Young Adults in the United States, 2005–2016. JAMA Pediatr. 2020, 174, e194498. [Google Scholar]
- Weiss, R.; Taksali, S.E.; Tamborlane, W.V.; Burgert, T.S.; Savoye, M.; Caprio, S. Predictors of Changes in Glucose Tolerance Status in Obese Youth. Diabetes Care 2005, 28, 902–909. [Google Scholar]
- Pulgaron, E.R.; Delamater, A.M. Obesity and Type 2 Diabetes in Children: Epidemiology and Treatment. Curr. Diabetes Rep. 2014, 14, 1–12. [Google Scholar]
- Chobot, A.; Górowska-Kowolik, K.; Sokołowska, M.; Jarosz-Chobot, P. Obesity and diabetes-Not only a simple link between two epidemics. Diabetes Metab. Res. Rev. 2018, 34, e3042. [Google Scholar]
- Misra, A.; Vikram, N.K.; Arya, S.; Pandey, R.M.; Dhingra, V.; Chatterjee, A.; Dwivedi, M.; Sharma, R.; Luthra, K.; Guleria, R.; et al. High prevalence of insulin resistance in postpubertal Asian Indian children is associated with adverse truncal body fat patterning, abdominal adiposity and excess body fat. Int. J. Obes. 2004, 28, 1217–1226. [Google Scholar]
- Nightingale, C.M.; Rudnicka, A.R.; Owen, C.G.; Wells, J.C.K.; Sattar, N.; Cook, D.G.; Whincup, P.H. Influence of Adiposity on Insulin Resistance and Glycemia Markers Among U.K. Children of South Asian, Black African-Caribbean, and White European Origin. Diabetes Care 2013, 36, 1712–1719. [Google Scholar]
- Tagi, V.M.; Chiarelli, F. Obesity and insulin resistance in children. Curr. Opin. Pediatr. 2020, 32, 582–588. [Google Scholar]
- Roden, M.; Stingl, H.; Chandramouli, V.; Schumann, W.C.; Hofer, A.; Landau, B.R.; Nowotny, P.; Waldhausl, W.; Shulman, G.I. Effects of free fatty acid elevation on postabsorptive endogenous glucose production and gluconeogenesis in humans. Diabetes 2000, 49, 701–707. [Google Scholar]
- Jais, A.; Brüning, J.C. Hypothalamic inflammation in obesity and metabolic disease. J. Clin. Investig. 2017, 127, 24–32. [Google Scholar]
- Minchenko, D.O.; Tsymbal, D.O.; Davydov, V.V.; Minchenko, D.O. Expression of genes encoding IGF1, IGF2, and IGFBPs in blood of obese adolescents with insulin resistance. Endocr. Regul. 2019, 53, 34–45. [Google Scholar]
- Ighbariya, A.; Weiss, R. Insulin Resistance, Prediabetes, Metabolic Syndrome: What Should Every Pediatrician Know? J. Clin. Res. Pediatr. Endocrinol. 2017, 9, 49–57. [Google Scholar]
- Tagi, V.M.; Giannini, C.; Chiarelli, F. Insulin resistance in children. Front. Endocrinol. (Lausanne) 2019, 10, 342. [Google Scholar]
- Matsuda, M.; DeFronzo, R.A. Insulin sensitivity indices obtained from oral glucose tolerance testing: Comparison with the euglycemic insulin clamp. Diabetes Care 1999, 22, 1462–1470. [Google Scholar]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and β-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar]
- Deeb, A.; Salima, A.; Samia, M.; Ghada, E.; Abubaker, E. Insulin Resistance, Impaired fasting, Glucose Intolerance and Type II Diabetes Mellitus in Overweight and Obese Children in Abu Dhabi. J. Diabetes Obes. 2017, 4, 1–8. [Google Scholar]
- D’Adamo, E.; Caprio, S. Type 2 Diabetes in Youth: Epidemiology and Pathophysiology. Diabetes Care 2011, 34 (Suppl. 2), S161–S165. [Google Scholar]
- Maffeis, C.; Morandi, A. Body composition and insulin resistance in children. Eur. J. Clin. Nutr. 2018, 72, 1239–1245. [Google Scholar]
- Jasik, C.B.; Lustig, R.H. Adolescent Obesity and Puberty: The “Perfect Storm”. Ann. N. Y. Acad. Sci. 2008, 1135, 265–279. [Google Scholar]
- Goran, M.I.; Gower, B.A. Longitudinal Study on Pubertal Insulin Resistance. Diabetes 2001, 50, 2444–2450. [Google Scholar]
- Wilding, J.P.H. The importance of weight management in type 2 diabetes mellitus. Int. J. Clin. Pr. 2014, 68, 682–691. [Google Scholar]
- Giacco, F.; Brownlee, M. Oxidative Stress and Diabetic Complications. Circ. Res. 2010, 107, 1058–1070. [Google Scholar]
- TODAY Study Group. Lipid and Inflammatory Cardiovascular Risk Worsens Over 3 Years in Youth With Type 2 Diabetes: The TODAY clinical trial. Diabetes Care 2013, 36, 1758–1764. [Google Scholar]
- Dabelea, D.; Stafford, J.M.; Mayer-Davis, E.J.; D’Agostino, R.; Dolan, L.; Imperatore, G.; Linder, B.; Lawrence, J.M.; Marcovina, S.M.; Mottl, A.K.; et al. Association of Type 1 Diabetes vs Type 2 Diabetes Diagnosed During Childhood and Adolescence With Complications During Teenage Years and Young Adulthood. JAMA 2017, 317, 825–835. [Google Scholar]
- Amutha, A.; Anjana, R.M.; Venkatesan, U.; Ranjani, H.; Unnikrishnan, R.; Narayan, K.V.; Mohan, V.; Ali, M.K. Incidence of complications in young-onset diabetes: Comparing type 2 with type 1 (the young diab study). Diabetes Res. Clin. Pr. 2017, 123, 1–8. [Google Scholar]
- D’Adamo, E.; Guardamagna, O.; Chiarelli, F.; Bartuli, A.; Liccardo, D.; Ferrari, F.; Nobili, V. Atherogenic Dyslipidemia and Cardiovascular Risk Factors in Obese Children. Int. J. Endocrinol. 2015, 2015, 1–9. [Google Scholar]
- Kwiterovich, P.O., Jr. Recognition and Management of Dyslipidemia in Children and Adolescents. J. Clin. Endocrinol. Metab. 2008, 93, 4200–4209. [Google Scholar]
- Ahrens, W.; Pigeot, I.; Pohlabeln, H.; De Henauw, S.; Lissner, L.; Molnár, D.; Moreno, L.A.; Tornaritis, M.; Veidebaum, T.; on behalf of the IDEFICS consortium; et al. Prevalence of overweight and obesity in European children below the age of 10. Int. J. Obes. 2014, 38 (Suppl. 2), S99–S107. [Google Scholar]
- Burns, S.F.; Lee, S.; Arslanian, S. In Vivo Insulin Sensitivity and Lipoprotein Particle Size and Concentration in Black and White Children. Diabetes Care 2009, 32, 2087–2093. [Google Scholar] [PubMed] [Green Version]
- Giannini, C.; Santoro, N.; Caprio, S.; Kim, G.; Lartaud, D.; Shaw, M.; Pierpont, B.; Weiss, R. The Triglyceride-to-HDL Cholesterol Ratio. Diabetes Care 2011, 34, 1869–1874. [Google Scholar]
- De Giorgis, T.; Marcovecchio, M.L.; Di Giovanni, I.; Giannini, C.; Chiavaroli, V.; Chiarelli, F.; Mohn, A. Triglycerides-to-HDL ratio as a new marker of endothelial dysfunction in obese prepubertal children. Eur. J. Endocrinol. 2014, 170, 173–180. [Google Scholar]
- Tabas, I.; Williams, K.J.; Borén, J. Subendothelial Lipoprotein Retention as the Initiating Process in Atherosclerosis. Circulation 2007, 116, 1832–1844. [Google Scholar] [PubMed]
- Assmann, G.; Gotto, A.M., Jr. HDL cholesterol and protective factors in atherosclerosis. Circulation 2004, 109, III8–III14. [Google Scholar]
- Nielsen, L.B. Transfer of low density lipoprotein into the arterial wall and risk of atherosclerosis. Atherosclerosis 1996, 123, 1–15. [Google Scholar]
- Herouvi, D.; Karanasios, E.; Karayianni, C.; Karavanaki, K. Cardiovascular disease in childhood: The role of obesity. Eur. J. Pediatr. 2013, 172, 721–732. [Google Scholar]
- Paramsothy, P.; Knopp, R.H.; Bertoni, A.G.; Blumenthal, R.S.; Wasserman, B.A.; Tsai, M.Y.; Rue, T.; Wong, N.D.; Heckbert, S.R. Association of Combinations of Lipid Parameters With Carotid Intima-Media Thickness and Coronary Artery Calcium in the MESA (Multi-Ethnic Study of Atherosclerosis). J. Am. Coll. Cardiol. 2010, 56, 1034–1041. [Google Scholar]
- Juonala, M.; Viikari, J.S.; Rönnemaa, T.; Marniemi, J.; Jula, A.; Loo, B.-M.; Raitakari, O.T. Associations of Dyslipidemias From Childhood to Adulthood With Carotid Intima-Media Thickness, Elasticity, and Brachial Flow-Mediated Dilatation in Adulthood. Arter. Thromb. Vasc. Biol. 2008, 28, 1012–1017. [Google Scholar]
- Kathiresan, S.; Otvos, J.D.; Sullivan, L.M.; Keyes, M.J.; Schaefer, E.J.; Wilson, P.W.; D’Agostino, R.B.; Vasan, R.S.; Robins, S.J. Increased Small Low-Density Lipoprotein Particle Number. Circulation 2006, 113, 20–29. [Google Scholar] [PubMed] [Green Version]
- Kavey, R.-E.W. Combined dyslipidemia in childhood. J. Clin. Lipidol. 2015, 9, S41–S56. [Google Scholar] [PubMed]
- National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents. The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics 2004, 114, 555–576. [Google Scholar]
- Flynn, J.T. The changing face of pediatric hypertension in the era of the childhood obesity epidemic. Pediatr. Nephrol. 2013, 28, 1059–1066. [Google Scholar]
- Wühl, E. Hypertension in childhood obesity. Acta Paediatr. 2018, 108, 37–43. [Google Scholar]
- Hou, Y.; Wang, M.; Yang, L.; Zhao, M.; Yan, Y.; Xi, B. Weight status change from childhood to early adulthood and the risk of adult hypertension. J. Hypertens. 2019, 37, 1239–1243. [Google Scholar]
- DelVecchio, M.; Pastore, C.; Valente, F.; Giordano, P. Cardiovascular Implications in Idiopathic and Syndromic Obesity in Childhood: An Update. Front. Endocrinol. 2020, 11, 330. [Google Scholar]
- Jing, L.; Binkley, C.M.; Suever, J.D.; Umasankar, N.; Haggerty, C.M.; Rich, J.; Nevius, C.D.; Wehner, G.J.; Hamlet, S.M.; Powell, D.K.; et al. Cardiac remodeling and dysfunction in childhood obesity: A cardiovascular magnetic resonance study. J. Cardiovasc. Magn. Reson. 2016, 18, 28. [Google Scholar] [PubMed] [Green Version]
- Alp, H.; Eklioglu, B.S.; Atabek, M.E.; Karaarslan, S.; Baysal, T.; Altin, H.; Karataş, Z.; Şap, F. Evaluation of epicardial adipose tissue, carotid intima-media thickness and ventricular functions in obese children and adolescents. J. Pediatr. Endocrinol. Metab. 2014, 27, 827–835. [Google Scholar]
- Hall, J.E. Pathophysiology of obesity hypertension. Curr. Hypertens. Rep. 2000, 2, 139–147. [Google Scholar]
- Arslan, N. Obesity, fatty liver disease and intestinal microbiota. World J. Gastroenterol. 2014, 20, 16452–16463. [Google Scholar] [PubMed]
- Anderson, E.L.; Howe, L.D.; Jones, H.E.; Higgins, J.P.T.; Lawlor, D.A.; Fraser, A. The Prevalence of Non-Alcoholic Fatty Liver Disease in Children and Adolescents: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0140908. [Google Scholar]
- Donnelly, K.L.; Smith, C.I.; Schwarzenberg, S.J.; Jessurun, J.; Boldt, M.D.; Parks, E.J. Sources of fatty acids stored in liver and secreted via lipoproteins in patients with nonalcoholic fatty liver disease. J. Clin. Investig. 2005, 115, 1343–1351. [Google Scholar] [PubMed]
- Feldstein, A.E.; Bailey, S.M. Emerging Role of Redox Dysregulation in Alcoholic and Nonalcoholic Fatty Liver Disease. Antioxidants Redox Signal. 2011, 15, 421–424. [Google Scholar]
- Kursawe, R.; Santoro, N. Metabolic syndrome in pediatrics. Adv. Clin. Chem. 2014, 65, 91–142. [Google Scholar]
- Wittcopp, C.; Conroy, R. Metabolic Syndrome in Children and Adolescents. Pediatr. Rev. 2016, 37, 193–202. [Google Scholar]
- Weiss, R.; Dziura, J.; Burgert, T.S.; Tamborlane, W.V.; Taksali, S.E.; Yeckel, C.W.; Allen, K.; Lopes, M.; Savoye, M.; Morrison, J.; et al. Obesity and the metabolic syndrome in children and adolescents. N. Engl. J. Med. 2004, 350, 2362–2374. [Google Scholar]
- Ford, E.S.; Li, C. Defining the Metabolic Syndrome in Children and Adolescents: Will the Real Definition Please Stand Up? J. Pediatr. 2008, 152, 160–164. [Google Scholar]
- Expert Panel on Detection, Evaluation and Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [Google Scholar]
- Zimmet, P.; Alberti, K.G.M.; Kaufman, F.; Tajima, N.; Silink, M.; Arslanian, S.; Wong, G.; Bennett, P.; Shaw, J.; Caprio, S.; et al. The metabolic syndrome in children and adolescents? An IDF consensus report. Pediatr. Diabetes 2007, 8, 299–306. [Google Scholar]
- Ahrens, W.; Moreno, L.A.; Marild, S.; Molnar, D.; Siani, A.; De Henauw, S.; Böhmann, J.; Gunther, K.D.; Hadjigeorgiou, C.; on behalf of the IDEFICS consortium; et al. Metabolic syndrome in young children: Definitions and results of the IDEFICS study. Int. J. Obes. 2014, 38 (Suppl. 2), S4–S14. [Google Scholar]
- Reinehr, T.; De Sousa, G.; Toschke, A.M.; Andler, W. Comparison of metabolic syndrome prevalence using eight different definitions: A critical approach. Arch. Dis. Child. 2007, 92, 1067–1072. [Google Scholar]
- Hsieh, S.D.; Ashwell, M.; Muto, T.; Tsuji, H.; Arase, Y.; Murase, T. Urgency of reassessment of role of obesity indices for metabolic risks. Metabolism 2010, 59, 834–840. [Google Scholar] [PubMed]
- Tilg, H.; Moschen, A.R. Inflammatory Mechanisms in the Regulation of Insulin Resistance. Mol. Med. 2008, 14, 222–231. [Google Scholar]
- De Ferranti, S.; Mozaffarian, D. The Perfect Storm: Obesity, Adipocyte Dysfunction, and Metabolic Consequences. Clin. Chem. 2008, 54, 945–955. [Google Scholar]
- Simmonds, M.; Llewellyn, A.; Owen, C.G.; Woolacott, N. Predicting adult obesity from childhood obesity: A systematic review and meta-analysis. Obes. Rev. 2015, 17, 95–107. [Google Scholar] [PubMed] [Green Version]
- Juonala, M.; Magnussen, C.G.; Berenson, G.S.; Venn, A.; Burns, T.L.; Sabin, M.A.; Srinivasan, S.R.; Daniels, S.R.; Davis, P.H.; Chen, W.; et al. Childhood Adiposity, Adult Adiposity, and Cardiovascular Risk Factors. N. Engl. J. Med. 2011, 365, 1876–1885. [Google Scholar]
- World Health Organization. Population-based approaches to childhood obesity prevention; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- Bell, L.M.; Watts, K.; Siafarikas, A.; Thompson, A.; Ratnam, N.; Bulsara, M.; Finn, J.; O’Driscoll, G.; Green, D.J.; Jones, T.W.; et al. Exercise Alone Reduces Insulin Resistance in Obese Children Independently of Changes in Body Composition. J. Clin. Endocrinol. Metab. 2007, 92, 4230–4235. [Google Scholar] [PubMed] [Green Version]
- Nassis, G.P.; Papantakou, K.; Skenderi, K.; Triandafillopoulou, M.; Kavouras, S.A.; Yannakoulia, M.; Chrousos, G.P.; Sidossis, L.S. Aerobic exercise training improves insulin sensitivity without changes in body weight, body fat, adiponectin, and inflammatory markers in overweight and obese girls. Metabolism 2005, 54, 1472–1479. [Google Scholar]
- Sayin, F.K.; Buyukinan, M. Sleep Duration and Media Time Have a Major Impact on Insulin Resistance and Metabolic Risk Factors in Obese Children and Adolescents. Child. Obes. 2016, 12, 272–278. [Google Scholar] [PubMed]
- DeBoer, M.D.; Filipp, S.L.; Musani, S.K.; Sims, M.; Okusa, M.D.; Gurka, M.J. Metabolic Syndrome Severity and Risk of CKD and Worsened GFR: The Jackson Heart Study. Kidney Blood Press. Res. 2018, 43, 555–567. [Google Scholar]
- Carlson, J.J.; Eisenmann, J.C.; Norman, G.J.; Ortiz, K.A.; Young, P.C. Dietary Fiber and Nutrient Density Are Inversely Associated with the Metabolic Syndrome in US Adolescents. J. Am. Diet. Assoc. 2011, 111, 1688–1695. [Google Scholar]
- Davis, J.N.; Alexander, K.E.; Ventura, E.E.; Toledo-Corral, C.M.; Goran, M.I. Inverse relation between dietary fiber intake and visceral adiposity in overweight Latino youth. Am. J. Clin. Nutr. 2009, 90, 1160–1166. [Google Scholar]
- Lin, Y.; Huybrechts, I.; Vereecken, C.; Mouratidou, T.; Valtueña, J.; Kersting, M.; González-Gross, M.; Bolca, S.; Wärnberg, J.; Cuenca-García, M.; et al. Dietary fiber intake and its association with indicators of adiposity and serum biomarkers in European adolescents: The HELENA study. Eur. J. Nutr. 2014, 54, 771–782. [Google Scholar]
- Yancy, W.S., Jr.; Olsen, M.K.; Guyton, J.R.; Bakst, R.P.; Westman, E.C. A low-carbohydrate, ketogenic diet versus a low-fat diet to treat obesity and hyperlipidemia: A randomized, controlled trial. Ann. Intern. Med. 2004, 140, 769–777. [Google Scholar]
- Thomas, D.; Elliott, E.J.; Baur, L.A. Low glycaemic index or low glycaemic load diets for overweight and obesity. Cochrane Database Syst. Rev. 2007, 18, CD005105. [Google Scholar]
- Blundell, J.E.; Stubbs, R.J.; Hughes, D.A.; Whybrow, S.; King, N.A. Cross talk between physical activity and appetite control: Does physical activity stimulate appetite? Proc. Nutr. Soc. 2003, 62, 651–661. [Google Scholar]
- Martin, C.K.; Heilbronn, L.K.; De Jonge, L.; Delany, J.P.; Volaufova, J.; Anton, S.D.; Redman, L.M.; Smith, S.R.; Ravussin, E. Effect of Calorie Restriction on Resting Metabolic Rate and Spontaneous Physical Activity. Obesity (Silver Spring) 2007, 15, 2964–2973. [Google Scholar]
- Bereket, A.; Atay, Z. Current Status of Childhood Obesity and its Associated Morbidities in Turkey. J. Clin. Res. Pediatr. Endocrinol. 2012, 4, 1–7. [Google Scholar]
- Yanovski, J.A.; Krakoff, J.; Salaita, C.G.; McDuffie, J.R.; Kozlosky, M.; Sebring, N.G.; Reynolds, J.C.; Brady, S.M.; Calis, K.A. Effects of Metformin on Body Weight and Body Composition in Obese Insulin-Resistant Children. Diabetes 2011, 60, 477–485. [Google Scholar]
- Knudsen, L.B.; Lau, J. The Discovery and Development of Liraglutide and Semaglutide. Front. Endocrinol. 2019, 10, 155. [Google Scholar]
- Van Can, J.; Sloth, B.; Jensen, C.; Flint, A.; Blaak, E.; Saris, W.H.M. Effects of the once-daily GLP-1 analog liraglutide on gastric emptying, glycemic parameters, appetite and energy metabolism in obese, non-diabetic adults. Int. J. Obes. 2013, 38, 784–793. [Google Scholar]
- Flynn, J.T.; Falkner, B.E. New Clinical Practice Guideline for the Management of High Blood Pressure in Children and Adolescents. Hypertension 2017, 70, 683–686. [Google Scholar] [PubMed]
- Forouzanfar, M.H.; Alexander, L.; Anderson, H.R.; Bachman, V.F.; Biryukov, S.; Brauer, M.; Burnett, R.; Casey, D.; Coates, M.M.; Cohen, A.; et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks in 188 countries, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 386, 2287–2323. [Google Scholar] [PubMed] [Green Version]
Figure 1.
Risk factors for cardiovascular remodelling in obese children. The arrow means that there is an increase in sympathetic tone and in the activity of RAA system.
Figure 1.
Risk factors for cardiovascular remodelling in obese children. The arrow means that there is an increase in sympathetic tone and in the activity of RAA system.


{kind=link}
Table 1.
Definition of metabolic syndrome in children.
| Cook et al., 2003 (NCEP) | Weiss et al., 2004 (NCEP) | Zimmet et al., 2007 (IDF) | Ahrens et al., 2014 (IDEFICS) | |
|---|---|---|---|---|
| WC | ≥90° ptc | ≥90° ptc | ≥90°(95°) ptc | |
| SBP | ≥90° ptc | ≥95° ptc | ≥130 mmHg | ≥90°(95°) ptc |
| DBP | ≥90° ptc | ≥95° ptc | ≥85 mmHg | ≥90°(95°) ptc |
| TG | ≥1.24 mmol/L | ≥95° ptc | ≥1.7 mmol/L | ≥90°(95°) ptc |
| HDL-C | ≤1.03 mmol/L | ≤5° ptc | ≤1.03 mmol/L | ≤10°(5°) ptc |
| Glucose homeostasis | IFG ≥ 6.11 mmol/L | IGT (ADA criteria) | IFG ≥ 5.6 mmol/L | HOMA-IR or IFG ≥90° (95°) ptc |
| BMI | Z score ≥ 2 |
ptc: percentile; WC: waist circumference; SBP: systolic blood pressure; DBP: diastolic blood pressure; TG triglycerides, HDL-C: high-density lipoprotein cholesterol; BMI: body mass index; IFG: fasting glucose; IGT: impaired glucose tolerance; HOMA-IR: Homeostatic Model Assessment of Insulin Resistance; NCEP: National Cholesterol Education Program; IDF: International Diabetes Federation; IDEFICS: Identification and prevention of Dietary and lifestyle-induced health Effects In Children and infantS.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Angi, A.; Chiarelli, F. Obesity and Diabetes: A Sword of Damocles for Future Generations. Biomedicines 2020, 8, 478. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines8110478
AMA Style
Angi A, Chiarelli F. Obesity and Diabetes: A Sword of Damocles for Future Generations. Biomedicines. 2020; 8(11):478. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines8110478
Chicago/Turabian StyleAngi, Alessia, and Francesco Chiarelli. 2020. "Obesity and Diabetes: A Sword of Damocles for Future Generations" Biomedicines 8, no. 11: 478. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines8110478
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.