Autoantibodies as Potential Biomarkers in Breast Cancer



Department of Biomedical Engineering, University of Houston, 3517 Cullen BLVD, SERC 2008, Houston, TX 77204, USA
*
Author to whom correspondence should be addressed.
Biosensors 2018, 8(3), 67; https://0-doi-org.brum.beds.ac.uk/10.3390/bios8030067
Submission received: 14 June 2018
/
Revised: 11 July 2018
/
Accepted: 11 July 2018
/
Published: 13 July 2018
(This article belongs to the Special Issue Biomarkers)
Abstract
:Breast cancer is a major cause of mortality in women; however, technologies for early stage screening and diagnosis (e.g., mammography and other imaging technologies) are not optimal for the accurate detection of cancer. This creates demand for a more effective diagnostic means to replace or be complementary to existing technologies for early discovery of breast cancer. Cancer neoantigens could reflect tumorigenesis, but they are hardly detectable at the early stage. Autoantibodies, however, are biologically amplified and hence may be measurable early on, making them promising biomarkers to discriminate breast cancer from healthy tissue accurately. In this review, we summarized the recent findings of breast cancer specific antigens and autoantibodies, which may be useful in early detection, disease stratification, and monitoring of treatment responses of breast cancer.
1. Introduction
Breast cancer is the prevailing cancer among women in developing and developed countries [1]. As such, screening and early diagnosis with respect to risk stratification are critical for prevention and early intervention of the disease, leading to better therapeutic outcomes [2,3]. Breast cancer itself is genetically heterogeneous and expresses a variety of aberrant proteins that, until recently, were un-utilizable. Of the current commercially available detection methods, mammography is the only screening technology to improve mortality; however, there are clear limitations to the technology [4]. Initially, mammography lacks sensitivity, rendering the technology less beneficial in younger women (ages 40–49 years) [5,6] and, most importantly, ill-suited for detection of node-negative early-stage (T1N0) primary breast cancer (PBC) and ductal carcinoma in situ (DCIS) [7,8]. Additional studies have indicated that mammography can lead to false positive results, despite the poor sensitivity, especially for women who started screening at young ages due to the larger number of mammograms and subsequently higher recall rate [9]. As a consequence, overdiagnosis by mammograms occurs within 1–10% of patients [10]. Additionally, magnetic resonance imaging (MRI) and breast ultrasound, which also contribute to false positives, are used as supplementary diagnosis methods for patients with invasive breast cancer after an initial screening mammography [11]. Recently, however, with the development of next-generation sequencing (NGS) and complementary advanced sequencing technologies, these aforementioned mutated cancer gene sequences are detectable in blood samples from patients and through techniques such as liquid biopsy [12], circulating tumor DNA (ctDNA) [13,14], and cell-free DNA (cfDNA) [15]. However, given the low concentrations of these ctDNAs, amplification steps are usually necessary, complicating and prolonging the detection protocols.
Autoantibodies (AABs) present an alternative to the above with the advantage of minimalist hardware, short time-frames (30 min), and an abundance of targets [16]. These proteins are a selection of antibodies whose associated antigens are produced by the organism’s own cells; the antigens themselves are expressed at low concentrations in healthy cells and overexpressed or aberrantly expressed in cancerous cells. This erroneous expression of antigens is detected by the immune system through methods such as toll-like receptors (TLRs) for the innate response, with the potential to both exacerbate and reverse tumor growth, and the class 2 major histocompatibility complex (MHC) by phosphorylation and or glycosylation of the “normally” expressed antigen, preventing recognition [17,18]. MUC1, for example, an integral membrane protein of the breast, was detected to be overexpressed in 90% of adenocarcinomas and was further linked to tumor aggression [17,19]. Unfortunately, the immune surveillance of breast cancers has been found to be compromised as the IRF7 pathway inside of breast cancer cells is suppressed. This is mitigated by the multicomponent nature of said surveillance system and the fact that the same pathway also governs the metastasis of the cancer alongside the TLRs, allowing for more accurate prognostics [18,20].
Ultimately, the ideal test would accurately identify breast cancers that require intervention, preferably at an early stage, minimizing the amount of surgical and pharmacological treatment, while avoiding overdiagnosis and subsequent overtreatment [21]. Therefore, efficient, low-cost, and highly sensitive technology is needed, particularly for women with early-stage breast cancer.
2. Autoantibodies in Breast Cancer
Current blood-based detection assays are ill-suited for screening, classification, and impacting treatment decisions [22]. This is a consequence of the early breast cancer stages being characterized by minimal disease burden—less than 1 × 106 tumor cells—and low or undetectable serum levels of protein biomarkers, making the monitoring of traditional biomarkers challenging.
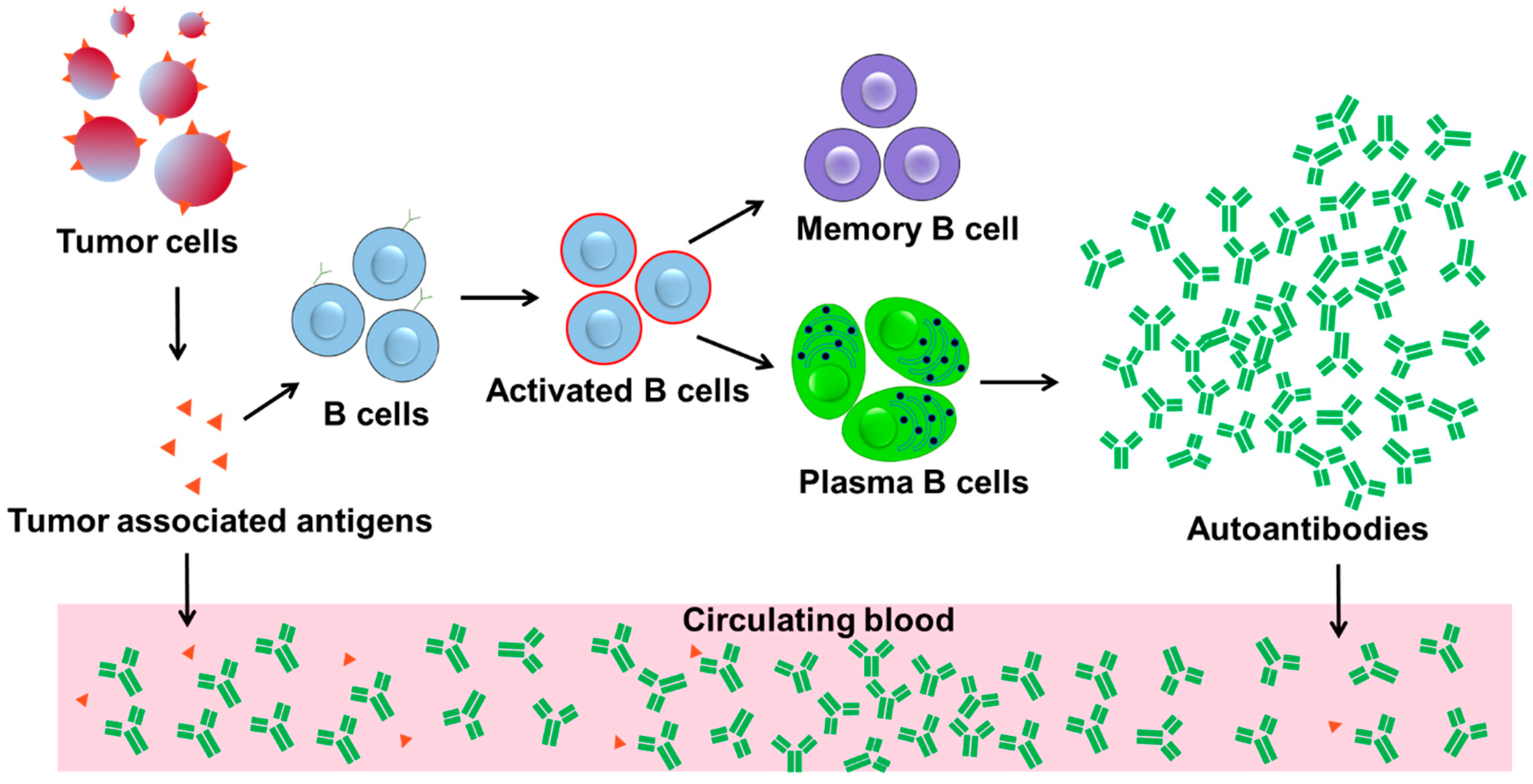
B cells, however, offer a solution to the above problem by class switching to produce high affinity matured autoantibodies, massively abundant high affinity biomarkers, in response to the presence of antigens, which occurs during the early stages of cancers as shown in Figure 1. An individual B cell can produce 5000–20,000 antibodies/min, as well as undergo mitosis every 3 days, further maintaining or enhancing autoantibody production [23,24,25]. The specificity of B cell autoantibody responses to tumor antigens and effective amplification of “tumor signal” can fulfill the desirable features of a biomarker, namely specificity and sensitivity (Figure 1). In fact, specific immune escape events may herald the transition from in situ to invasive breast cancer, which suggest that autoantibody reaction-based assays can be effective for early detection [26]. In particular, the IgG κ chain has been indicated as a prognostic biomarker in breast cancer, with applications in predicting disease response and neoadjuvant chemotherapy efficacy [27,28]. Interestingly, clinical trials have demonstrated higher response rates to immune checkpoint blockade in triple-negative breast cancer (TNBC) tumors when compared with estrogen-receptor positive (ER+) tumors, allowing for potential discrimination [29,30,31].
Furthermore, gene mutations lead to successive generations of neoantigens, while malignant transformation and the associated apoptosis will release excessive antigens. These antigens may trigger the immune system to produce high titers of autoantibodies or tumor-associated autoantibodies (TAABs). These TAABs can be promising biomarkers for early diagnosis of breast cancer based on concentration, which may precede clinical confirmation of cancer by months to years, as the detection of autoantibodies can be performed earlier than the originating tumor-associated antigens (TAAs) assays [2,32,33]. Moreover, there are a plethora of TAABs, which are highly stable in serum and whole-blood compared to other polypeptides [34]. These autoantibodies against TAAs have been verified in breast cancer, as summarized in Table 1. As such, using autoantibody biomarkers to achieve early diagnosis of breast cancer is promising and can reflect clinical responses to immunotherapy, as has been shown in several malignancies [35,36,37]. Therefore, immunoreactive autoantibodies (IR-Abs) of TAAs provide an in vivo amplification of early cancer signals and allow for earlier detection. Furthermore, there is evidence for a specific humoral response against a number of intracellular and surface tumoral antigens related to breast cancer [38,39,40,41,42,43,44,45,46,47,48,49,50,51]. However, these results did not lead to clinically useful biomarkers for early diagnostics of breast cancer due to relatively poor sensitivity and specificity.
An example of a useful autoantibody is heat-shock protein 60 (HSP60), positive in 31% of patients during early-stage breast cancer and 32.6% of patients with DCIS, with a miniscule 4.3% presentation in healthy controls [52,53], which is consistent with Hamrita et al.’s detection of HSP60 in 19 out of 40 invasive breast cancer patients (47.5%) and only 2 out of 42 healthy controls (4.7%) [54]; together, these studies strongly indicate that HSP60 may be a potential TAA for the diagnosis of noninvasive and invasive ductal carcinoma. Additionally, several other autoantigens may be involved in the pathways of breast cancer tumorigenesis, such as those found in the mammalian target of the rapamycin (mTOR) phosphorylation pathway: ribosomal protein S6, eukaryotic elongation factor 2, eukaryotic elongation factor 2 kinase, heat shock protein 90 (HSP90), and the DNA damage/repair pathways, such as Ku protein, topoisomerase I, and the 32-kDa subunit of replication protein A [52,55]. Other proteins not involved in the above pathways have also been found to present in altered expression but have not been validated. A few of these proteins are as follows: keratins, actins, histones, serine/arginine splicing factors, and Ubiquitin [56]. Ultimately, a proteomic autoantibody screening method can open new avenues in uncovering molecular mechanisms of tumorigenesis for breast cancer of varying types. As detailed in a recent systematic review and meta–analysis by Xia and colleagues, autoantibodies against p53, MUC1, HER2, and cyclin B1 are the top 4 among all breast cancer-associated autoantibodies in terms of the frequency of studies. There are considerable variations in terms of sensitivity and specificity of these autoantibodies as potential biomarkers of breast cancer in disease diagnosis [57], which may be due to different study sites, different assay technologies and platforms, different experimental procedures and protocols, and different patient populations. Therefore, it should be pointed out that it is too early to rank the diagnostic values or predictive values of these autoantibodies for clinical use. Standardized assay protocols may be needed and may be helpful in establishing highly accurate and robust autoantibodies as biomarkers of breast cancer. Although the exact function of these autoantibodies is not clear, we could speculate that these autoantibodies may be generated by B cells to neutralize cancer promoting proteins/neo-antigens, in order to suppress cancer growth.
3. Autoantibody Detection in Breast Cancer
Several technologies such as immunosensors, enzyme-linked immunosorbent assay (ELISA), antigen arrays, and bead arrays have been applied to the detection of autoantibodies in breast cancer patients. Immunosensors have been demonstrated to detect autoantibodies in autoimmune disease and have the potential for similar detection of autoantibodies in breast cancer [58]. ELISA, the more traditional immunological assay, has been successfully used to measure the concentration of autoantibodies in breast cancer patients (Table 1). Antigen arrays, an efficient high-throughput technology, can also be used for the same task. As such, technologies like ELISA and antigen arrays can be applied as complements in breast cancer studies. As an example, antigen arrays can be used to discover potential autoantibodies in breast cancer against hundreds and thousands of antigens. After the establishment of an antigen–autoantibody pair, ELISA can be applied for a large cohort of patients and controls so that statistical analysis can be applied to extract meaningful data.
An example of this is HER-2/neu, a breast cancer specific antigen, which Disis et al. identified using ELISA and western blot techniques. Then they discovered autoantibodies against HER-2/neu at the early-stage of breast cancer. These HER-2/neu antibodies in breast cancer patients were correlated with HER-2/neu protein expression and HER-2/neu-positive cancer [59]. Additionally, Mudenda and colleagues reported that autoantibodies to p53 were found in breast cancer patients in all stages of disease progression. Interestingly, in a longitudinal cohort of breast cancer patients, p53 autoantibody levels positively correlated with histology grades and p53 expression in cancer tissues [60].
However, there is no single autoantibody found, which has been used as a clinical biomarker—a consequence of the heterogeneous nature of breast cancer. The proteins in said cancer are aberrantly expressed either post-translationally modified or irregularly regulated in the same type of cancer [52,78]. It has become obvious that a single autoantibody biomarker is not sufficient to provide information about tumor progression [79]. Therefore, a combination of selected autoantibodies arranged as a biomarker panel may be more attractive. Although such an autoantibody panel is not yet available, a bead array panel of 35 tumor-associated antigens was constructed by Kim et al. [43], which possessed a high accuracy of 91.8% by random forest analysis, 91.5% by support vector machine analysis, and 87.6% by linear discriminant analysis in distinguishing breast cancer patients from healthy controls [43].
It should be noted that the cancer antigen 15-3 (CA15-3) and the carcinoembryonic antigen (CEA) have been approved by Food and Drug Administration (FDA) as tumor markers for breast cancer. Additionally, CA125 and malignant tumor-specific growth factor (TSGF) have been suggested as tumor-associated markers [80,81,82]. The investigation of autoantibodies against these cancer antigens can provide valuable information in uncovering disease mechanisms, identifying novel drug targets and establishing diagnostic biomarkers for breast cancer.
4. Technologies for Autoantibody Discovery and Detection in Breast Cancer
During the past decade, several high-throughput technologies have been developed and utilized in the discovery and detection of autoantibodies. Technologies, such as serological analysis of tumor antigens by recombinant cDNA expression cloning (SEREX) [52,83,84], phage display [85,86,87], serological proteome analysis (SERPA) [54,88,89], multiple affinity protein profiling (MAPPing) [90], protein microarrays [91,92,93,94,95,96], and nanoplasmonic sensors [16] have been applied in the study of autoantibody biomarkers of breast cancer [78].
4.1. Serological Analysis of Tumor Antigens by Recombinant cDNA Expression Cloning (SEREX)
In this technology, TAABs are identified by screening patient sera against a cDNA expression library obtained from the autologous tumor tissues [97]. Over 2000 autoantigens are documented in an online database, the Cancer Immunome Database (CID) [98,99,100]. SEREX facilitated the identification of TAAs as possible cancer biomarkers in different types of cancer, such as lung, liver, breast, prostate, ovarian, renal, head, neck, esophageal cancers, leukemia, and melanoma [52,101]. The panel of SEREX-defined immunogenic tumor antigens include Cancer/Testis Antigens (CTAs, e.g., NY-ESO-1, SSX2, MAGE), mutational antigens (e.g., p53), differentiation antigens (e.g., tyrosinase, SOX2, ZIC2), and embryonic proteins [52]. The disadvantage of SEREX lies in that it is time-consuming, labor-intensive and difficult to automate for high-throughput assay. In addition, autoantibodies against post-translational modifications of antigens cannot be detected by SEREX.
There is no doubt that individual assays, such as ELISA, immunosensors [58], or multiplexing bead-based autoantibody assays are important tools for the detection and validation of the level of specific autoantibodies as biomarkers, especially in large cohorts of patients for diagnosis and disease monitoring of breast cancer, as illustrated in Figure 2.
4.2. Serological Proteome Analysis (SERPA)
SERPA is a proteomic approach which combines two-dimensional (2D) electrophoresis, western blotting, and mass spectrometry (MS) [52,88]. Briefly, proteins from tissue or cells are separated by isoelectric and SDS-PAGE gel electrophoresis and transferred onto membranes, followed by probing with sera from patients with cancer. Subsequently, the differentially expressed immunoreactive cancer antigens are excised from the gel and identified by MS. Klade et al. developed SERPA, and identified carbonic anhydrase I (CAI) and smooth muscle protein 22 (SM22) in kidney cancer tissues [102]. Kellner et al. showed that several members of the cytoskeletal family (such as cytokeratin 8, stathmin, and vimentin) are potential TAABs that can distinguish between renal cell carcinoma subtypes and from the normal renal epithelium tissue [103]. Furthermore, when coupled with western blotting for serological screening, 2D gel could be used to detect TAABs that undergo post-translational modifications via MS analysis.
SERPA has been applied in the discovery of autoantibodies in various cancer types, including neuroblastoma, lung cancer, breast cancer, renal cell carcinoma, hepatocellular carcinoma (HCC), and ovarian cancer [104,105,106,107,108]. This technique eases the detection of novel autoantibodies and associated autoantigens as early indicators of tumorigenesis. Several autoantibodies, such as hnRNPK, Mn-SOD, HSP60, and F1-ATPase, were identified in breast cancer using SERPA [54].
4.3. Multiple Affinity Protein Profiling (MAPPing)
MAPPing comprises 2D immunoaffinity chromatography followed by the identification of TAABs by tandem mass spectrometry (2D-LC-MS/MS) [90,109]. In immunoaffinity chromatography, TAAs from cancerous tissues bind to IgG from healthy controls. The unbound fraction of the lysate is then subjected to the 2D immunoaffinity column that contains IgG from cancer patients. TAAs that bind are likely to be cancer-specific and are identified by tandem MS/MS [109].
4.4. Protein Microarray
A novel high-density custom protein microarray, nucleic acid protein programmable array (NAPPA), is fabricated by printing full-length cDNAs encoding the target proteins, and the target proteins are then transcribed and translated by a cell-free system. Tumor antigens from nearly 5000 breast cancer patients at early stages were detected using NAPPA, and 28 antigens were found to be highly responsive to their relevant autoantibodies: ATP6AP1, PDCD6IP, DBT, CSNK1E, FRS3, RAC3, HOXD1, SF3A1, CTBP1, C15orf48, MYOZ2, EIF3E, BAT4, ATF3, BMX, RAB5A, UBAP1, SOX2, GPR157, BDNF, ZMYM6, SLC33A1, TRIM32, ALG10, TFCP2, SERPINH1, SELL, and ZNF510 [91]. Ola Blixt et al. synthesized MUC1 glycopeptides and used a novel microarray to test a large cohort of breast cancer patients and healthy controls. It was found that early-stage breast cancer has more frequent and higher levels of autoantibodies to glycosylated MUC1 compared to healthy controls, which indicates that autoantibodies may reflect disease progression [61].
4.5. Nanoplasmonic Biosensor
The nanoplasmonic biosensor is an etched glass substrate that utilizes the surface plasmons of gold in combination with bound TAAs. The system measures the reflective index of the material at the baseline and as it changes due to local surface bioactivity after the introduction of untreated plasma or sera. The sensitivity of the system is increased through the use of a waveguided light source with limits of detection for GTF2b and EDIL3 antibodies of approximately 10 and 5 ng/mL, respectively. The total time to run the assay is 30 min, and it has the ability to be reused for over 100 cycles [16].
5. Look into the Future
So far, most studies on autoantibodies in breast cancer have focused on their diagnostic values. It should be pointed out that autoantibodies, as important indicators of the function of the immune system, will play more important roles in monitoring drug responses, especially immunotherapy. In the past decade, immunotherapy has been successfully applied in metastatic melanoma with strong clinical responses in malignancies, such as lung, kidney, bladder cancers, and non-metastatic melanoma [110]. Current immunotherapy techniques can be divided into two categories: passive and active. Passive immunotherapy has been successfully applied in clinics, where treatments such as Trastuzumab, known as Herceptin, are applied. Trastuzumab is a monoclonal antibody targeting the extracellular domain of the HER2 protein, and it is the mainstay of passive immunotherapy in HER2-positive breast cancer [111]. The antibody can selectively bind to HER2 receptors to prevent breast cancer cells from proliferating, achieving a therapeutic goal. In 2005, Piccart-Gebhart and colleagues found that one-year treatment with Trastuzumab after chemotherapy significantly improved survival rate for HER2-positive breast cancer [112,113]. Active immunotherapy often refers to cancer vaccines. For example, E75, a human leukocyte antigen (HLA)-A2/A3-restricted immunogenic peptide derived from the HER2 protein, has been used as a vaccine to prevent disease recurrence in high-risk breast cancer patients [114]. Recently, an in situ vaccination was used to trigger a T cell immune response to attack cancer cells (e.g., the combination of a Toll-like receptor 9 (TLR) ligand and an anti-OX40 antibody can successfully cure various types of cancer) [115]. This approach was successfully applied in mouse models; however, more time is required for human trials. More recently, immune checkpoint inhibitors have emerged with promise as a cancer treatment [116,117,118,119]. For example, PD1 has been used to block checkpoint inhibitors preventing the proliferation of tumors and showing encouraging anticancer therapeutic effects [116,117,118,119]. Studies on mutational load, immune profile, and response to immune checkpoint inhibition in a BRCA1-deficient tumor models have provided a rationale for clinical studies of combined immune checkpoint blockade in BRCA1-associated TNBC [120].
Tumor-infiltrating lymphocytes (TIL) [121,122], such as cytotoxic T cells, may predict better patient outcomes and responses to drugs (such as checkpoint blockade therapies); whereas, an increased number of regulatory T cells (Treg: CD4+FoxP3+CD25high) or myeloid-derived suppressor cells (MDSC) may correlate with lower survival rates in cancer and with lower clinical response rates to anti-CTLA-4 antibodies [123,124,125,126]. Also, CD20+ B cells among TIL correlated with favorable prognosis in ovarian cancer [127]. These findings suggest that the specific immune status of patients may be indicative of the capability to respond to and suppress tumor progression. However, immune cell-based detection is largely dependent on flow cytometry, a tedious and complicated operation, especially when multiple staining procedures are needed for various cell subsets and activation states.
As an alternative approach, autoantibody levels in the serum of breast cancer patients could potentially be used to monitor treatment responses during immunotherapy. Combination treatment, such as radiation plus chemotherapy or radiation plus hormonal therapy, resulted in a significant decrease of autoantibodies [62], which indicates that immunotherapy may be beneficial to these patients. Future direction can be focused on the real-time monitoring of tumor-associated autoantibody levels, which may aid immunotherapy.
In conclusion, as the immune system is an indispensable player during tumorigenesis and cancer development, autoantibodies, particularly cancer antigen-specific autoantibodies, may be used as early biomarkers for cancer detection and prevention. More importantly, the detection of these autoantibodies may be indicative of novel treatment strategies (e.g., development of monoclonal antibodies against the same cancer antigen to cure the disease). Also, the development of novel assays for the detection of cancer-specific autoantibodies, such as autoantibody panel array and ultrasensitive immunobiosensors, may provide a powerful complementary strategy to mammography in the screening of suspicious breast cancer patients.
Author Contributions
Writing-Original Draft Preparation, J.Q.; Writing-Review & Editing, T.W., B.K. and Z.-T.L.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Bray, F.; McCarron, P.; Parkin, D.M. The changing global patterns of female breast cancer incidence and mortality. Breast Cancer Res. 2004, 6, 229–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lacombe, J.; Mangé, A.; Solassol, J. Use of autoantibodies to detect the onset of breast cancer. J. Immunol. Res. 2014, 2014, 574981. [Google Scholar] [CrossRef] [PubMed]
- American Cancer Society. Breast Cancer Facts & Figures 2017–2018; American Cancer Society: Atlanta, GA, USA, 2017. [Google Scholar]
- Bleyer, A.; Welch, H.G. Effect of three decades of screening mammography on breast-cancer incidence. N. Engl. J. Med. 2012, 367, 1998–2005. [Google Scholar] [CrossRef] [PubMed]
- Axelrod, D.; Smith, J.; Kornreich, D.; Grinstead, E.; Singh, B.; Cangiarella, J.; Guth, A.A. Breast cancer in young women. J. Am. Coll. Surg. 2008, 206, 1193–1203. [Google Scholar] [CrossRef] [PubMed]
- Berg, W.A. Beyond standard mammographic screening: Mammography at age extremes, ultrasound, and MR imaging. Radiol. Clin. N. Am. 2007, 45, 895–906. [Google Scholar] [CrossRef] [PubMed]
- Kirsh, V.A.; Chiarelli, A.M.; Edwards, S.A.; O’Malley, F.P.; Shumak, R.S.; Yaffe, M.J.; Boyd, N.F. Tumor characteristics associated with mammographic detection of breast cancer in the Ontario breast screening program. J. Natl. Cancer Inst. 2011, 103, 942–950. [Google Scholar] [CrossRef] [PubMed]
- Olson, J.E.; Sellers, T.A.; Scott, C.G.; Schueler, B.A.; Brandt, K.R.; Serie, D.J.; Jensen, M.R.; Wu, F.-F.; Morton, M.J.; Heine, J.J.; et al. The influence of mammogram acquisition on the mammographic density and breast cancer association in the mayo mammography health study cohort. Breast Cancer Res. 2012, 14, R147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oeffinger, K.C.; Fontham, E.T.; Etzioni, R.; Herzig, A.; Michaelson, J.S.; Shih, Y.-C.T.; Walter, L.C.; Church, T.R.; Flowers, C.R.; LaMonte, S.J.; et al. Breast cancer screening for women at average risk: 2015 guideline update from the American Cancer Society. JAMA 2015, 314, 1599–1614. [Google Scholar] [CrossRef] [PubMed]
- Puliti, D.; Duffy, S.W.; Miccinesi, G.; De Koning, H.; Lynge, E.; Zappa, M.; Paci, E. Overdiagnosis in mammographic screening for breast cancer in Europe: A literature review. J. Med. Screen. 2012, 19, 42–56. [Google Scholar] [CrossRef] [PubMed]
- Van Goethem, M.; Tjalma, W.; Schelfout, K.; Verslegers, I.; Biltjes, I.; Parizel, P. Magnetic resonance imaging in breast cancer. Eur. J. Surg. Oncol. 2006, 32, 901–910. [Google Scholar] [CrossRef] [PubMed]
- Diaz, L.A., Jr.; Bardelli, A. Liquid biopsies: Genotyping circulating tumor DNA. J. Clin. Oncol. 2014, 32, 579–586. [Google Scholar] [CrossRef] [PubMed]
- Bettegowda, C.; Sausen, M.; Leary, R.J.; Kinde, I.; Wang, Y.; Agrawal, N.; Bartlett, B.R.; Wang, H.; Luber, B.; Alani, R.M.; et al. Detection of circulating tumor DNA in early-and late-stage human malignancies. Sci. Transl. Med. 2014, 6, 224ra24. [Google Scholar] [CrossRef] [PubMed]
- Dawson, S.-J.; Tsui, D.W.; Murtaza, M.; Biggs, H.; Rueda, O.M.; Chin, S.-F.; Dunning, M.J.; Gale, D.; Forshew, T.; Mahler-Araujo, B.; et al. Analysis of circulating tumor DNA to monitor metastatic breast cancer. N. Engl. J. Med. 2013, 368, 1199–1209. [Google Scholar] [CrossRef] [PubMed]
- Giacona, M.B.; Ruben, G.C.; Iczkowski, K.A.; Roos, T.B.; Porter, D.M.; Sorenson, G.D. Cell-free DNA in human blood plasma: Length measurements in patients with pancreatic cancer and healthy controls. Pancreas 1998, 17, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Soler, M.; Estevez, M.C.; Villar-Vazquez, R.; Casal, J.I.; Lechuga, L.M. Label-free nanoplasmonic sensing of tumor-associate autoantibodies for early diagnosis of colorectal cancer. Anal. Chim. Acta 2016, 930, 31–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaenker, P.; Gray, E.S.; Ziman, M.R. Autoantibody Production in Cancer—The Humoral Immune Response toward Autologous Antigens in Cancer Patients. Autoimmun. Rev. 2016, 15, 477–483. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Jiang, Q.; Zhang, Y.; Liang, H.; Ren, H.; Zhang, D. Toll-like receptors and breast cancer. Integr. Cancer Sci. Therap. 2016, 3, 432–436. [Google Scholar] [CrossRef] [Green Version]
- Yonezawa, S.; Goto, M.; Yamada, N.; Higashi, M.; Nomoto, M. Expression profiles of MUC1, MUC2, and MUC4 mucins in human neoplasms and their relationship with biological behavior. Proteomics 2008, 8, 3329–3341. [Google Scholar] [CrossRef] [PubMed]
- Bidwell, B.N.; Slaney, C.Y.; Withana, N.P.; Forster, S.; Cao, Y.; Loi, S.; Andrews, D.; Mikeska, T.; Mangan, N.E.; Samarajiwa, S.A.; et al. Silencing of Irf7 pathways in breast cancer cells promotes bone metastasis through immune escape. Nat. Med. 2012, 18, 1224–1231. [Google Scholar] [CrossRef] [PubMed]
- Nelson, H.D.; Pappas, M.; Cantor, A.; Griffin, J.; Daeges, M.; Humphrey, L. Harms of breast cancer screening: Systematic review to update the 2009 US Preventive Services Task Force Recommendation. Ann. Intern. Med. 2016, 164, 256–267. [Google Scholar] [CrossRef] [PubMed]
- Smerage, J.B.; Barlow, W.E.; Hortobagyi, G.N.; Winer, E.P.; Leyland-Jones, B.; Srkalovic, G.; Tejwani, S.; Schott, A.F.; O’Rourke, M.A.; Lew, D.L.; et al. Circulating tumor cells and response to chemotherapy in metastatic breast cancer: SWOG S0500. J. Clin. Oncol. 2014, 32, 3483–3489. [Google Scholar] [CrossRef] [PubMed]
- Cenci, S.; Sitia, R. Managing and exploiting stress in the antibody factory. FEBS Lett. 2007, 581, 3652–3657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Förster, I.; Rajewsky, K. The bulk of the peripheral B-cell pool in mice is stable and not rapidly renewed from the bone marrow. Proc. Natl. Acad. Sci. USA 1990, 87, 4781–4784. [Google Scholar] [CrossRef] [PubMed]
- Cooperman, J.; Neely, R.; Teachey, D.T.; Grupp, S.; Choi, J.K. Cell division rates of primary human precursor B cells in culture reflect in vivo rates. Stem Cells 2004, 22, 1111–1120. [Google Scholar] [CrossRef] [PubMed]
- Del Alcazar, C.R.G.; Huh, S.J.; Ekram, M.B.; Trinh, A.; Liu, L.L.; Beca, F.; Zi, X.; Kwak, M.; Bergholtz, H.; Su, Y.; et al. Immune escape in breast cancer during in situ to invasive carcinoma transition. Cancer Discov. 2017, 7, 1098–1115. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.; Böhm, D.; von Törne, C.; Steiner, E.; Puhl, A.; Pilch, H.; Lehr, H.-A.; Hengstler, J.G.; Kölbl, H.; Gehrmann, M. The humoral immune system has a key prognostic impact in node-negative breast cancer. Cancer Res. 2008, 68, 5405–5413. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.; Hellwig, B.; Hammad, S.; Othman, A.; Lohr, M.; Chen, Z.; Boehm, D.; Gebhard, S.; Petry, I.; Lebrecht, A.; et al. A comprehensive analysis of human gene expression profiles identifies stromal immunoglobulin κ C as a compatible prognostic marker in human solid tumors. Clin. Cancer Res. 2012, 18, 2695–2703. [Google Scholar] [CrossRef] [PubMed]
- Hammerl, D.; Smid, M.; Timmermans, A.; Sleijfer, S.; Martens, J.; Debets, R. Breast cancer genomics and immuno-oncological markers to guide immune therapies. Semin. Cancer Biol. 2017. [Google Scholar] [CrossRef] [PubMed]
- Santa-Maria, C.A.; Kato, T.; Park, J.-H.; Flaum, L.E.; Jain, S.; Tellez, C.; Stein, R.M.; Shah, A.N.; Gross, L.; Uthe, R.; et al. Durvalumab and Tremelimumab in Metastatic Breast Cancer (MBC): Immunotherapy and Immunopharmacogenomic Dynamics; American Society of Clinical Oncology: Alexandria, VA, USA, 2017. [Google Scholar]
- Nanda, R.; Liu, M.C.; Yau, C.; Asare, S.; Hylton, N.; Veer, L.V.T.; Perlmutter, J.; Wallace, A.M.; Chien, A.J.; Forero-Torres, A. Pembrolizumab Plus Standard Neoadjuvant Therapy for High-Risk Breast Cancer (BC): Results from I-SPY 2; American Society of Clinical Oncology: Alexandria, VA, USA, 2017. [Google Scholar]
- Wu, J.; Li, X.; Song, W.; Fang, Y.; Yu, L.; Liu, S.; Churilov, L.P.; Zhang, F. The roles and applications of autoantibodies in progression, diagnosis, treatment and prognosis of human malignant tumours. Autoimmun. Rev. 2017, 16, 1270–1281. [Google Scholar] [CrossRef] [PubMed]
- Poletaev, A.; Pukhalenko, A.; Kukushkin, A.; Sviridov, P. Detection of early cancer: Genetics or immunology? Serum autoantibody profiles as markers of malignancy. Anti-Cancer Agents Med. Chem. 2015, 15, 1260–1263. [Google Scholar] [CrossRef]
- Desmetz, C.; Mange, A.; Maudelonde, T.; Solassol, J. Autoantibody signatures: Progress and perspectives for early cancer detection. J. Cell. Mol. Med. 2011, 15, 2013–2024. [Google Scholar] [CrossRef] [PubMed]
- Kipps, T.J.; Tomhave, E.; Chen, P.P.; Carson, D.A. Autoantibody-associated kappa light chain variable region gene expressed in chronic lymphocytic leukemia with little or no somatic mutation. Implications for etiology and immunotherapy. J. Exp. Med. 1988, 167, 840–852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vincent, A.; Irani, S.R.; Lang, B. The growing recognition of immunotherapy-responsive seizure disorders with autoantibodies to specific neuronal proteins. Curr. Opin. Neurol. 2010, 23, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Menoret, A.; Chandawarkar, R.; Srivastava, P. Natural autoantibodies against heat-shock proteins hsp70 and gp96: Implications for immunotherapy using heat-shock proteins. Immunology 2000, 101, 364–370. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, M.E.A.; Abdelhafiz, K. Autoantibodies in the sera of breast cancer patients: Antinuclear and anti-double stranded DNA antibodies as example. J. Cancer Res. Ther. 2015, 11, 341–344. [Google Scholar] [CrossRef] [PubMed]
- Yahalom, G.; Weiss, D.; Novikov, I.; Bevers, T.B.; Radvanyi, L.G.; Liu, M.; Piura, B.; Iacobelli, S.; Sandri, M.T.; Cassano, E.; et al. An antibody-based blood test utilizing a panel of biomarkers as a new method for improved breast cancer diagnosis. Biomark. Cancer 2013, 5, 71–80. [Google Scholar] [CrossRef] [PubMed]
- Evans, R.L.; Pottala, J.V.; Egland, K.A. Classifying patients for breast cancer by detection of autoantibodies against a panel of conformation-carrying antigens. Cancer Prev. Res. 2014, 7, 545–555. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Figueroa, J.D.; Wallstrom, G.; Barker, K.; Park, J.G.; Demirkan, G.; Lissowska, J.; Anderson, K.S.; Qiu, J.; LaBaer, J. Plasma autoantibodies associated with basal-like breast cancers. Cancer Epidemiol. Prev. Biomark. 2015, 24, 1332–1340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kostianets, O.; Shyyan, M.; Antoniuk, S.V.; Filonenko, V.; Kiyamova, R. Panel of SEREX-defined antigens for breast cancer autoantibodies profile detection. Biomarkers 2017, 22, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.K.; Lee, J.W.; Park, P.J.; Shin, Y.S.; Lee, W.Y.; Lee, K.A.; Ye, S.; Hyun, H.; Kang, K.N.; Yeo, D.; et al. The multiplex bead array approach to identifying serum biomarkers associated with breast cancer. Breast Cancer Res. 2009, 11, R22. [Google Scholar] [CrossRef] [PubMed]
- Tabuchi, Y.; Shimoda, M.; Kagara, N.; Naoi, Y.; Tanei, T.; Shimomura, A.; Shimazu, K.; Kim, S.J.; Noguchi, S. Protective effect of naturally occurring anti-HER2 autoantibodies on breast cancer. Breast Cancer Res. Treat. 2016, 157, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Atalay, C.; Dogan, L.; Atalay, G. Anti-CENP-B antibodies are associated with prolonged survival in breast cancer. Future Oncol. 2010, 6, 471–477. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.; Gehin, T.; Chevolot, Y.; Souteyrand, E.; Mangé, A.; Solassol, J.; Laurenceau, E. Anti-heat shock protein autoantibody profiling in breast cancer using customized protein microarray. Anal. Bioanal. Chem. 2016, 408, 1497–1506. [Google Scholar] [CrossRef] [PubMed]
- Koziol, J.A.; Zhang, J.-Y.; Casiano, C.A.; Peng, X.-X.; Shi, F.-D.; Feng, A.C.; Chan, E.K.; Tan, E.M. Recursive partitioning as an approach to selection of immune markers for tumor diagnosis. Clin. Cancer Res. 2003, 9, 5120–5126. [Google Scholar] [PubMed]
- Fernández-Madrid, F.; Tang, N.; Alansari, H.; Granda, J.L.; Tait, L.; Amirikia, K.C.; Moroianu, M.; Wang, X.; Karvonen, R.L. Autoantibodies to annexin XI-A and other autoantigens in the diagnosis of breast cancer. Cancer Res. 2004, 64, 5089–5096. [Google Scholar] [CrossRef] [PubMed]
- Chapman, C.; Murray, A.; Chakrabarti, J.; Thorpe, A.; Woolston, C.; Sahin, U.; Barnes, A.; Robertson, J. Autoantibodies in breast cancer: Their use as an aid to early diagnosis. Ann. Oncol. 2007, 18, 868–873. [Google Scholar] [CrossRef] [PubMed]
- Madrid, F.F.; Maroun, M.-C.; Olivero, O.A.; Long, M.; Stark, A.; Grossman, L.I.; Binder, W.; Dong, J.; Burke, M.; Nathanson, S.D.; et al. Autoantibodies in breast cancer sera are not epiphenomena and may participate in carcinogenesis. BMC Cancer 2015, 15, 407. [Google Scholar]
- Coronell, J.A.L.; Syed, P.; Sergelen, K.; Gyurján, I.; Weinhäusel, A. The current status of cancer biomarker research using tumour-associated antigens for minimal invasive and early cancer diagnostics. J. Proteom. 2012, 76, 102–115. [Google Scholar] [CrossRef] [PubMed]
- Tan, H.T.; Low, J.; Lim, S.G.; Chung, M. Serum autoantibodies as biomarkers for early cancer detection. FEBS J. 2009, 276, 6880–6904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Desmetz, C.; Bibeau, F.; Boissiere, F.; Bellet, V.; Rouanet, P.; Maudelonde, T.; Mange, A.; Solassol, J. Proteomics-based identification of HSP60 as a tumor-associated antigen in early stage breast cancer and ductal carcinoma in situ. J. Proteome Res. 2008, 7, 3830–3837. [Google Scholar] [CrossRef] [PubMed]
- Hamrita, B.; Chahed, K.; Kabbage, M.; Guillier, C.L.; Trimeche, M.; Chaïeb, A.; Chouchane, L. Identification of tumor antigens that elicit a humoral immune response in breast cancer patients’ sera by serological proteome analysis (SERPA). Clin. Chim. Acta 2008, 393, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Madrid, F.F. Autoantibodies in breast cancer sera: Candidate biomarkers and reporters of tumorigenesis. Cancer Lett. 2005, 230, 187–198. [Google Scholar]
- Katayama, H.; Boldt, C.; Ladd, J.J.; Johnson, M.M.; Chao, T.; Capello, M.; Suo, J.; Mao, J.; Manson, J.E.; Prentice, R.; et al. An Autoimmune Response Signature Associated with the Development of Triple-Negative Breast Cancer Reflects Disease Pathogenesis. Cancer Res. 2015, 75, 3246–3254. [Google Scholar] [CrossRef] [PubMed]
- Xia, J.; Shi, J.; Wang, P.; Song, C.; Wang, K.; Zhang, J.; Ye, H. Tumour-Associated Autoantibodies as Diagnostic Biomarkers for Breast Cancer: A Systematic Review and Meta-Analysis. Scand. J. Immunol. 2016, 83, 393–408. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Zambrano, A.; Lin, Z.-T.; Xing, Y.; Rippy, J.; Wu, T. Immunosensors for biomarker detection in autoimmune diseases. Arch. Immunol. Therap. Exp. 2017, 65, 111–121. [Google Scholar] [CrossRef] [PubMed]
- Disis, M.L.; Pupa, S.M.; Gralow, J.R.; Dittadi, R.; Menard, S.; Cheever, M.A. High-titer HER-2/neu protein-specific antibody can be detected in patients with early-stage breast cancer. J. Clin. Oncol. 1997, 15, 3363–3367. [Google Scholar] [CrossRef] [PubMed]
- Mudenda, B.; Green, J.; Green, B.; Jenkins, J.; Robertson, L.; Tarunina, M.; Leinster, S. The relationship between serum p53 autoantibodies and characteristics of human breast cancer. Br. J. Cancer 1994, 69, 1115–1119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blixt, O.; Bueti, D.; Burford, B.; Allen, D.; Julien, S.; Hollingsworth, M.; Gammerman, A.; Fentiman, I.; Taylor-Papadimitriou, J.; Burchell, J.M. Autoantibodies to aberrantly glycosylated MUC1 in early stage breast cancer are associated with a better prognosis. Breast Cancer Res. 2011, 13, R25. [Google Scholar] [CrossRef] [PubMed]
- Evans, R.L.; Pottala, J.V.; Nagata, S.; Egland, K.A. Longitudinal autoantibody responses against tumor-associated antigens decrease in breast cancer patients according to treatment modality. BMC Cancer 2018, 18, 119. [Google Scholar] [CrossRef] [PubMed]
- Yi, J.K.; Chang, J.W.; Han, W.; Lee, J.W.; Ko, E.; Kim, D.H.; Bae, J.-Y.; Yu, J.; Lee, C.; Yu, M.-H.; et al. Autoantibody to tumor antigen, alpha 2-HS glycoprotein: A novel biomarker of breast cancer screening and diagnosis. Cancer Epidemiol. Prev. Biomark. 2009, 18, 1357–1364. [Google Scholar] [CrossRef] [PubMed]
- Lu, H.; Ladd, J.; Feng, Z.; Wu, M.; Goodell, V.; Pitteri, S.J.; Li, C.I.; Prentice, R.; Hanash, S.M.; Disis, M.L. Evaluation of known oncoantibodies, HER2, p53, and cyclin B1, in prediagnostic breast cancer sera. Cancer Prev. Res. 2012, 5, 1036–1043. [Google Scholar] [CrossRef] [PubMed]
- Ye, H.U.A.; Sun, C.; Ren, P.; Dai, L.; Peng, B.O.; Wang, K.; Qian, W.E.I.; Zhang, J. Mini-array of multiple tumor-associated antigens (TAAs) in the immunodiagnosis of breast cancer. Oncol. Lett. 2013, 5, 663–668. [Google Scholar] [CrossRef] [PubMed]
- Zuo, X.; Chen, L.; Liu, L.; Zhang, Z.; Zhang, X.; Yu, Q.; Feng, L.; Zhao, X.; Qin, T. Identification of a panel of complex autoantigens (LGALS3, PHB2, MUC1, and GK2) in combination with CA15-3 for the diagnosis of early-stage breast cancer. Tumour Biol. J. Int. Soc. Oncodev. Biol. Med. 2016, 37, 1309–1317. [Google Scholar] [CrossRef] [PubMed]
- Shih, N.Y.; Lai, H.L.; Chang, G.C.; Lin, H.C.; Wu, Y.C.; Liu, J.M.; Liu, K.J.; Tseng, S.W. Anti-alpha-enolase autoantibodies are down-regulated in advanced cancer patients. Jpn. J. Clin. Oncol. 2010, 40, 663–669. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Zhang, R.; Wang, M.; Zhang, Y.; Qi, J.; Li, J. SOX2 autoantibodies as noninvasive serum biomarker for breast carcinoma. Cancer Epidemiol. Biomark. Prev. 2012, 21, 2043–2047. [Google Scholar] [CrossRef] [PubMed]
- Mischo, A.; Kubuschok, B.; Ertan, K.; Preuss, K.D.; Romeike, B.; Regitz, E.; Schormann, C.; de Bruijn, D.; Wadle, A.; Neumann, F.; et al. Prospective study on the expression of cancer testis genes and antibody responses in 100 consecutive patients with primary breast cancer. Int. J. Cancer 2006, 118, 696–703. [Google Scholar] [CrossRef] [PubMed]
- Chung, J.M.; Jung, Y.; Kim, Y.P.; Song, J.; Kim, S.; Kim, J.Y.; Kwon, M.; Yoon, J.H.; Kim, M.-D.; Lee, J.-K.; et al. Identification of the Thioredoxin-Like 2 Autoantibody as a Specific Biomarker for Triple-Negative Breast Cancer. J. Breast Cancer 2018, 21, 87–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bassaro, L.; Russell, S.J.; Pastwa, E.; Somiari, S.A.; Somiari, R.I. Screening for Multiple Autoantibodies in Plasma of Patients with Breast Cancer. Cancer Genom. Proteom. 2017, 14, 427–435. [Google Scholar]
- Nunna, V.; Jalal, N.; Bureik, M. Anti-CYP4Z1 autoantibodies detected in breast cancer patients. Cell. Mol. Immunol. 2017, 14, 572–574. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Liao, Y.; Xiang, L.; Jiang, K.; Li, S.; Huangfu, M.; Sun, S. A panel of autoantibodies as potential early diagnostic serum biomarkers in patients with breast cancer. Int. J. Clin. Oncol. 2017, 22, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Gupta, P.; Suman, S.; Mishra, M.; Mishra, S.; Srivastava, N.; Kumar, V.; Singh, P.K.; Shukla, Y. Autoantibodies against TYMS and PDLIM1 proteins detected as circulatory signatures in Indian breast cancer patients. Proteom. Clin. Appl. 2016, 10, 564–573. [Google Scholar] [CrossRef] [PubMed]
- Maselli, A.; Capoccia, S.; Pugliese, P.; Raggi, C.; Cirulli, F.; Fabi, A.; Malorni, W.; Pierdominici, M.; Ortona, E. Autoantibodies specific to estrogen receptor alpha act as estrogen agonists and their levels correlate with breast cancer cell proliferation. Oncoimmunology 2016, 5, e1074375. [Google Scholar] [CrossRef] [PubMed]
- Ladd, J.J.; Chao, T.; Johnson, M.M.; Qiu, J.; Chin, A.; Israel, R.; Pitteri, S.J.; Mao, J.; Wu, M.; Amon, L.M.; et al. Autoantibody signatures involving glycolysis and splicesome proteins precede a diagnosis of breast cancer among postmenopausal women. Cancer Res. 2012. [Google Scholar] [CrossRef] [PubMed]
- Mangé, A.; Lacombe, J.; Bascoul-Mollevi, C.; Jarlier, M.; Lamy, P.-J.; Rouanet, P.; Maudelonde, T.; Solassol, J. Serum autoantibody signature of ductal carcinoma in situ progression to invasive breast cancer. Clin. Cancer Res. 2012, 18, 1992–2000. [Google Scholar] [CrossRef] [PubMed]
- Zaenker, P.; Ziman, M.R. Serologic autoantibodies as diagnostic cancer biomarkers—A review. Cancer Epidemiol. Prev. Biomark. 2013, 22, 2161–2181. [Google Scholar] [CrossRef] [PubMed]
- Hanash, S.M.; Pitteri, S.J.; Faca, V.M. Mining the plasma proteome for cancer biomarkers. Nature 2008, 452, 571–579. [Google Scholar] [CrossRef] [PubMed]
- Fu, Y.; Li, H. Assessing clinical significance of serum CA15-3 and carcinoembryonic antigen (CEA) levels in breast cancer patients: A meta-analysis. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2016, 22, 3154–3162. [Google Scholar] [CrossRef]
- O’Hanlon, D.; Kerin, M.; Kent, P.; Maher, D.; Grimes, H.; Given, H. An evaluation of preoperative CA 15-3 measurement in primary breast carcinoma. Br. J. Cancer 1995, 71, 1288–1291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uehara, M.; Kinoshita, T.; Hojo, T.; Akashi-Tanaka, S.; Iwamoto, E.; Fukutomi, T. Long-term prognostic study of carcinoembryonic antigen (CEA) and carbohydrate antigen 15-3 (CA 15-3) in breast cancer. Int. J. Clin. Oncol. 2008, 13, 447–451. [Google Scholar] [CrossRef] [PubMed]
- Stempfer, R.; Syed, P.; Vierlinger, K.; Pichler, R.; Meese, E.; Leidinger, P.; Ludwig, N.; Kriegner, A.; Nöhammer, C.; Weinhäusel, A. Tumour auto-antibody screening: Performance of protein microarrays using SEREX derived antigens. BMC Cancer 2010, 10, 627. [Google Scholar] [CrossRef] [PubMed]
- Uchida, K.; Akita, Y.; Matsuo, K.; Fujiwara, S.; Nakagawa, A.; Kazaoka, Y.; Hachiya, H.; Naganawa, Y.; Oh-iwa, I.; Ohura, K.; et al. Identification of specific autoantigens in Sjögren’s syndrome by SEREX. Immunology 2005, 116, 53–63. [Google Scholar] [CrossRef] [PubMed]
- Payne, A.S.; Ishii, K.; Kacir, S.; Lin, C.; Li, H.; Hanakawa, Y.; Tsunoda, K.; Amagai, M.; Stanley, J.R.; Siegel, D.L. Genetic and functional characterization of human pemphigus vulgaris monoclonal autoantibodies isolated by phage display. J. Clin. Investig. 2005, 115, 888–899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalniņa, Z.; Siliņa, K.; Meistere, I.; Zayakin, P.; Rivosh, A.; Ābols, A.; Leja, M.; Minenkova, O.; Schadendorf, D.; Linē, A. Evaluation of T7 and lambda phage display systems for survey of autoantibody profiles in cancer patients. J. Immunol. Methods 2008, 334, 37–50. [Google Scholar] [CrossRef] [PubMed]
- Blüthner, M.; Bautz, E.K.; Bautz, F.A. Mapping of epitopes recognized by PMScl autoantibodies with gene-fragment phage display libraries. J. Immunol. Methods 1996, 198, 187–198. [Google Scholar] [CrossRef]
- Suzuki, A.; Iizuka, A.; Komiyama, M.; Takikawa, M.; Kume, A.; Tai, S.; Ohshita, C.; Kurusu, A.; Nakamura, Y.; Yamamoto, A.; et al. Identification of melanoma antigens using a Serological Proteome Approach (SERPA). Cancer Genom. Proteom. 2010, 7, 17–23. [Google Scholar]
- Massa, O.; Alessio, M.; Russo, L.; Nardo, G.; Bonetto, V.; Bertuzzi, F.; Paladini, A.; Iafusco, D.; Patera, P.; Federici, G.; et al. Serological Proteome Analysis (SERPA) as a tool for the identification of new candidate autoantigens in type 1 diabetes. J. Proteom. 2013, 82, 263–273. [Google Scholar] [CrossRef] [PubMed]
- Hardouin, J.; Lasserre, J.P.; Canelle, L.; Duchateau, M.; Vlieghe, C.; Choquet-Kastylevsky, G.; Joubert-Caron, R.; Caron, M. Usefulness of autoantigens depletion to detect autoantibody signatures by multiple affinity protein profiling. J. Sep. Sci. 2007, 30, 352–358. [Google Scholar] [CrossRef] [PubMed]
- Anderson, K.S.; Sibani, S.; Wallstrom, G.; Qiu, J.; Mendoza, E.A.; Raphael, J.; Hainsworth, E.; Montor, W.R.; Wong, J.; Park, J.G.; et al. Protein microarray signature of autoantibody biomarkers for the early detection of breast cancer. J. Proteome Res. 2010, 10, 85–96. [Google Scholar] [CrossRef] [PubMed]
- Robinson, W.H.; DiGennaro, C.; Hueber, W.; Haab, B.B.; Kamachi, M.; Dean, E.J.; Fournel, S.; Fong, D.; Genovese, M.C.; De Vegvar, H.E.N.; et al. Autoantigen microarrays for multiplex characterization of autoantibody responses. Nat. Med. 2002, 8, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Hueber, W.; Kidd, B.A.; Tomooka, B.H.; Lee, B.J.; Bruce, B.; Fries, J.F.; Sønderstrup, G.; Monach, P.; Drijfhout, J.W.; Van Venrooij, W.J.; et al. Antigen microarray profiling of autoantibodies in rheumatoid arthritis. Arth. Rheumatol. 2005, 52, 2645–2655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhen, Q.L.; Xie, C.; Wu, T.; Mackay, M.; Aranow, C.; Putterman, C.; Mohan, C. Identification of autoantibody clusters that best predict lupus disease activity using glomerular proteome arrays. J. Clin. Investig. 2005, 115, 3428–3439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hinchliffe, T.E.; Lin, Z.T.; Wu, T. Protein arrays for biomarker discovery in lupus. Proteom. Clin. Appl. 2016, 10, 625–634. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Y.; Wang, H.; Lin, Z.-T.; Hong, X.; Heon, M.; Wu, T. Protein Arrays II: Antigen Arrays. In Functional Genomics; Springer: Berlin, Germany, 2017; pp. 271–277. [Google Scholar]
- Sahin, U.; Türeci, O.; Schmitt, H.; Cochlovius, B.; Johannes, T.; Schmits, R.; Stenner, F.; Luo, G.; Schobert, I.; Pfreundschuh, M. Human neoplasms elicit multiple specific immune responses in the autologous host. Proc. Natl. Acad. Sci. USA 1995, 92, 11810–11813. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Zhang, W.; Cao, X.; Li, F.; Liu, X.; Yao, L. Serological identification of immunogenic antigens in acute monocytic leukemia. Leuk. Res. 2005, 29, 503–509. [Google Scholar] [CrossRef] [PubMed]
- Türeci, Ö.; Usener, D.; Schneider, S.; Sahin, U. Identification of tumor-associated autoantigens with SEREX. In Adoptive Immunotherapy: Methods and Protocols; Springer: Berlin, Germany, 2005; pp. 137–154. [Google Scholar]
- Jongeneel, V. Towards a cancer immunome database. Cancer Immun. Arch. 2001, 1, 3. [Google Scholar]
- Krackhardt, A.M.; Witzens, M.; Harig, S.; Hodi, F.S.; Zauls, A.J.; Chessia, M.; Barrett, P.; Gribben, J.G. Identification of tumor-associated antigens in chronic lymphocytic leukemia by SEREX. Blood 2002, 100, 2123–2131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klade, C.S.; Voss, T.; Krystek, E.; Ahorn, H.; Zatloukal, K.; Pummer, K.; Adolf, G.R. Identification of tumor antigens in renal cell carcinoma by serological proteome analysis. Proteom. Int. Ed. 2001, 1, 890–898. [Google Scholar] [CrossRef]
- Kellner, R.; Lichtenfels, R.; Atkins, D.; Bukur, J.; Ackermann, A.; Beck, J.; Brenner, W.; Melchior, S.; Seliger, B. Targeting of tumor associated antigens in renal cell carcinoma using proteome-based analysis and their clinical significance. Proteomics 2002, 2, 1743–1751. [Google Scholar] [CrossRef]
- Canelle, L.; Bousquet, J.; Pionneau, C.; Deneux, L.; Imam-Sghiouar, N.; Caron, M.; Joubert-Caron, R. An efficient proteomics-based approach for the screening of autoantibodies. J. Immunol. Methods 2005, 299, 77–89. [Google Scholar] [CrossRef] [PubMed]
- Le Naour, F.; Hohenkirk, L.; Grolleau, A.; Misek, D.E.; Lescure, P.; Geiger, J.D.; Hanash, S.; Beretta, L. Profiling changes in gene expression during differentiation and maturation of monocyte-derived dendritic cells using both oligonucleotide microarrays and proteomics. J. Biol. Chem. 2001, 276, 17920–17931. [Google Scholar] [CrossRef] [PubMed]
- Prasannan, L.; Misek, D.E.; Hinderer, R.; Michon, J.; Geiger, J.D.; Hanash, S.M. Identification of β-tubulin isoforms as tumor antigens in neuroblastoma. Clin. Cancer Res. 2000, 6, 3949–3956. [Google Scholar] [PubMed]
- Brichory, F.; Beer, D.; LeNaour, F.; Giordano, T.; Hanash, S. Proteomics-based identification of protein gene product 9.5 as a tumor antigen that induces a humoral immune response in lung cancer. Cancer Res. 2001, 61, 7908–7912. [Google Scholar] [PubMed]
- Canelle, L.; Bousquet, J.; Pionneau, C.; Hardouin, J.; Choquet-Kastylevsky, G.; Joubert-Caron, R.; Caron, M. A proteomic approach to investigate potential biomarkers directed against membrane-associated breast cancer proteins. Electrophoresis 2006, 27, 1609–1616. [Google Scholar] [CrossRef] [PubMed]
- Hardouin, J.; Lasserre, J.P.; Sylvius, L.; Joubert-Caron, R.; Caron, M. Cancer Immunomics. Ann. N. Y. Acad. Sci. 2007, 1107, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.P.; Kurzrock, R. PD-L1 expression as a predictive biomarker in cancer immunotherapy. Mol. Cancer Ther. 2015, 14, 847–856. [Google Scholar] [CrossRef] [PubMed]
- Romond, E.H.; Perez, E.A.; Bryant, J.; Suman, V.J.; Geyer, C.E., Jr.; Davidson, N.E.; Tan-Chiu, E.; Martino, S.; Paik, S.; Kaufman, P.A.; et al. Trastuzumab plus adjuvant chemotherapy for operable HER2-positive breast cancer. N. Engl. J. Med. 2005, 353, 1673–1684. [Google Scholar] [CrossRef] [PubMed]
- Piccart-Gebhart, M.J.; Procter, M.; Leyland-Jones, B.; Goldhirsch, A.; Untch, M.; Smith, I.; Gianni, L.; Baselga, J.; Bell, R.; Jackisch, C.; et al. Trastuzumab after adjuvant chemotherapy in HER2-positive breast cancer. N. Engl. J. Med. 2005, 353, 1659–1672. [Google Scholar] [CrossRef] [PubMed]
- Vogel, C.L.; Cobleigh, M.A.; Tripathy, D.; Gutheil, J.C.; Harris, L.N.; Fehrenbacher, L.; Slamon, D.J.; Murphy, M.; Novotny, W.F.; Burchmore, M.; et al. Efficacy and safety of trastuzumab as a single agent in first-line treatment of HER2-overexpressing metastatic breast cancer. J. Clin. Oncol. 2002, 20, 719–726. [Google Scholar] [CrossRef] [PubMed]
- Mittendorf, E.; Clifton, G.; Holmes, J.; Schneble, E.; van Echo, D.; Ponniah, S.; Peoples, G. Final report of the phase I/II clinical trial of the E75 (nelipepimut-S) vaccine with booster inoculations to prevent disease recurrence in high-risk breast cancer patients. Ann. Oncol. 2014, 25, 1735–1742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sagiv-Barfi, I.; Czerwinski, D.K.; Levy, S.; Alam, I.S.; Mayer, A.T.; Gambhir, S.S.; Levy, R. Eradication of spontaneous malignancy by local immunotherapy. Sci. Transl. Med. 2018, 10, eaan4488. [Google Scholar] [CrossRef] [PubMed]
- Loi, S.; Dushyanthen, S.; Beavis, P.A.; Salgado, R.; Denkert, C.; Savas, P.; Combs, S.; Rimm, D.L.; Giltnane, J.M.; Estrada, M.V. RAS/MAPK activation is associated with reduced tumor-infiltrating lymphocytes in triple-negative breast cancer: Therapeutic cooperation between MEK and PD-1/PD-L1 immune checkpoint inhibitors. Clin. Cancer Res. 2016, 22, 1499–1509. [Google Scholar] [CrossRef] [PubMed]
- Pardoll, D.M. The blockade of immune checkpoints in cancer immunotherapy. Nat. Rev. Cancer 2012, 12, 252–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bouffet, E.; Larouche, V.; Campbell, B.B.; Merico, D.; de Borja, R.; Aronson, M.; Durno, C.; Krueger, J.; Cabric, V.; Ramaswamy, V.; et al. Immune checkpoint inhibition for hypermutant glioblastoma multiforme resulting from germline biallelic mismatch repair deficiency. J. Clin. Oncol. 2016, 34, 2206–2211. [Google Scholar] [CrossRef] [PubMed]
- Postow, M.A.; Callahan, M.K.; Wolchok, J.D. Immune checkpoint blockade in cancer therapy. J. Clin. Oncol. 2015, 33, 1974–1982. [Google Scholar] [CrossRef] [PubMed]
- Nolan, E.; Savas, P.; Policheni, A.N.; Darcy, P.K.; Vaillant, F.; Mintoff, C.P.; Dushyanthen, S.; Mansour, M.; Pang, J.-M.B.; Fox, S.B.; et al. Combined immune checkpoint blockade as a therapeutic strategy for BRCA1-mutated breast cancer. Sci. Transl. Med. 2017, 9, eaal4922. [Google Scholar] [CrossRef] [PubMed]
- Galon, J.; Costes, A.; Sanchez-Cabo, F.; Kirilovsky, A.; Mlecnik, B.; Lagorce-Pagès, C.; Tosolini, M.; Camus, M.; Berger, A.; Wind, P.; et al. Type, density, and location of immune cells within human colorectal tumors predict clinical outcome. Science 2006, 313, 1960–1964. [Google Scholar] [CrossRef] [PubMed]
- Pagès, F.; Berger, A.; Camus, M.; Sanchez-Cabo, F.; Costes, A.; Molidor, R.; Mlecnik, B.; Kirilovsky, A.; Nilsson, M.; Damotte, D.; et al. Effector memory T cells, early metastasis, and survival in colorectal cancer. N. Engl. J. Med. 2005, 353, 2654–2666. [Google Scholar] [CrossRef] [PubMed]
- Ji, R.-R.; Chasalow, S.D.; Wang, L.; Hamid, O.; Schmidt, H.; Cogswell, J.; Alaparthy, S.; Berman, D.; Jure-Kunkel, M.; Siemers, N.O.; et al. An immune-active tumor microenvironment favors clinical response to ipilimumab. Cancer Immunol. Immunother. 2012, 61, 1019–1031. [Google Scholar] [CrossRef] [PubMed]
- Whiteside, T.L.; Mandapathil, M.; Szczepanski, M.; Szajnik, M. Mechanisms of tumor escape from the immune system: Adenosine-producing Treg, exosomes and tumor-associated TLRs. Bull. Cancer 2011, 98, E25–E31. [Google Scholar] [PubMed]
- Lança, T.; Silva-Santos, B. The split nature of tumor-infiltrating leukocytes: Implications for cancer surveillance and immunotherapy. Oncoimmunology 2012, 1, 717–725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meyer, C.; Cagnon, L.; Costa-Nunes, C.M.; Baumgaertner, P.; Montandon, N.; Leyvraz, L.; Michielin, O.; Romano, E.; Speiser, D.E. Frequencies of circulating MDSC correlate with clinical outcome of melanoma patients treated with ipilimumab. Cancer Immunol. Immunother. 2014, 63, 247–257. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, J.S.; Sahota, R.A.; Milne, K.; Kost, S.E.; Nesslinger, N.J.; Watson, P.H.; Nelson, B.H. CD20+ tumor-infiltrating lymphocytes have an atypical CD27− memory phenotype and together with CD8+ T cells promote favorable prognosis in ovarian cancer. Clin. Cancer Res. 2012, 18, 3281–3292. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Schematic diagram of autoantibody production and amplification by cancer antigen stimulation. B cells produce many copies of autoantibodies during immune responses, which amplify the cancer antigen “signal”, becoming detectable during early-stage breast cancer. In comparison, the concentration of antigens is too low to be detected in the same timeframe.
Figure 1.
Schematic diagram of autoantibody production and amplification by cancer antigen stimulation. B cells produce many copies of autoantibodies during immune responses, which amplify the cancer antigen “signal”, becoming detectable during early-stage breast cancer. In comparison, the concentration of antigens is too low to be detected in the same timeframe.

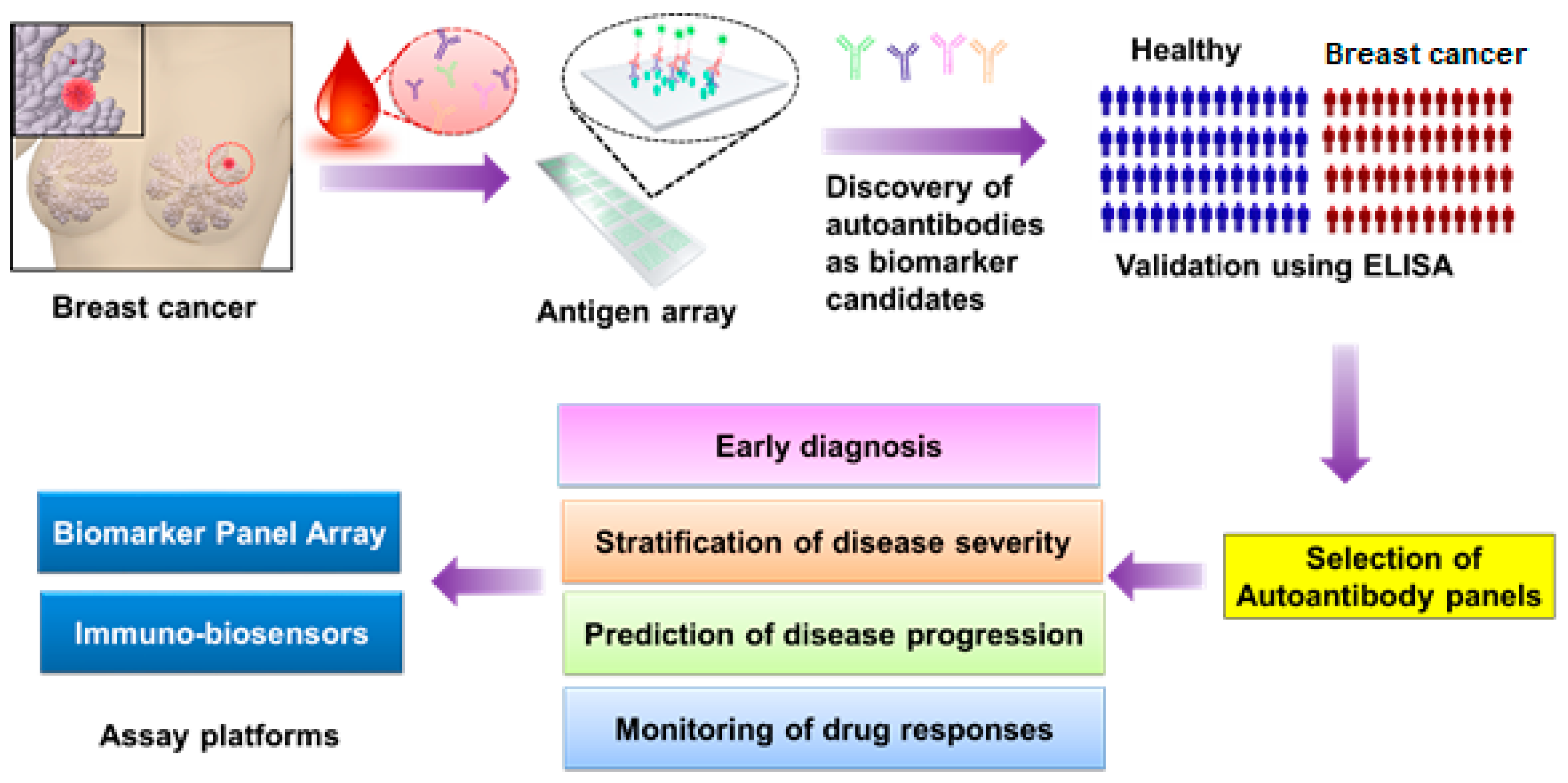
Figure 2.
Flowchart of autoantibody biomarker discovery and detection in breast cancer using antigen arrays and ELISA. First, a drop of blood from breast cancer (BC) patients is subjected to an antigen array for a high-throughput screening of autoantibodies that specifically bind to breast cancer antigens on an array. Second, promising autoantibody candidates are selected from the array screening and validated in a large cohort of patients using ELISA, which can be used for early diagnosis, disease stratification, prediction of disease progression, or monitoring of drug responses. Finally, according to the function of each autoantibody biomarker or biomarker panel, biosensors or autoantigen-panel chips could be designed and fabricated for clinical use in breast cancer.
Figure 2.
Flowchart of autoantibody biomarker discovery and detection in breast cancer using antigen arrays and ELISA. First, a drop of blood from breast cancer (BC) patients is subjected to an antigen array for a high-throughput screening of autoantibodies that specifically bind to breast cancer antigens on an array. Second, promising autoantibody candidates are selected from the array screening and validated in a large cohort of patients using ELISA, which can be used for early diagnosis, disease stratification, prediction of disease progression, or monitoring of drug responses. Finally, according to the function of each autoantibody biomarker or biomarker panel, biosensors or autoantigen-panel chips could be designed and fabricated for clinical use in breast cancer.


{kind=link}
{kind=link}
Table 1.
Tumor-associated autoantibodies in breast cancer.
| Autoantibodies/Antigens | Detection Method | Patient Cohort (N) | Reference |
|---|---|---|---|
| ANGPTL4, DKK1, GAL1, MUC1, GFRA1, GRN, and LRRC15 | ELISA | Breast cancer (200), controls (200) | [40] |
| CTAG1B, CTAG2, TP53, RNF216, PPHLN1, PIP4K2C, ZBTB16, TAS2R8, WBP2NL, DOK2, PSRC1, MN1 and TRIM21 | Protein array | Basal-like breast cancer (BLBC, 45), controls (45) | [41] |
| HSPB1, HSPD1, HSP70, HSP90, HSPA5, HSP90B1 and HSP110 | Protein microarray | Breast cancer (50), controls (26) | [46] |
| HER-2/neu | ELISA | Breast cancer (107), healthy controls (200) | [59] |
| p53 | ELISA | Breast cancer (182); Healthy controls (76) | [60] |
| MUC1 | ELISA, Peptide array | Breast cancer (395); Healthy controls (99) | [61] |
| A1AT, ANGPTL4, CAPC, CST2, DKK1, GFRA1, GRN, LGALS3, LRP10 and GRP78 | Luminex multiplex bead assay | Breast cancer, longitudinal (200) | [62] |
| alpha 2-HS glycoprotein | ELISA | Breast cancer (81), Healthy controls (73) | [63] |
| HER-2, p53, CEA, Cyclin B1 | ELISA, protein array | Breast cancer: controls Training set: 98: 98 Validation Set: 20:20; 33:45 | [64] |
| p53, c-myc, HER-2, NY-ESO-1, BRCA1, BRCA2 and MUC1 | ELISA | Primary breast cancer (97), ductal carcinoma in situ (40), normal (94) | [49] |
| PPIA, PRDX2, and FKBP52 | ELISA | Primary breast cancer (60), carcinoma in situ (82), controls (93) | [53] |
| HSP60 | ELISA | Ductal carcinoma in situ (DCIS) (49), early stage breast cancer (58), other cancers (20), healthy controls (93) | [53] |
| IMP1, p62, Koc, p53, c-myc, surviving, p16, cyclin B1, cyclin D1, and CDK2 | Mini-array, ELISA | Breast cancer (41), controls (82) | [65] |
| CA15-3, LGALS3, PHB2, MUC1, and GK2 | Protein array | Breast cancer (100), controls (50) | [66] |
| alpha-enolase (ENO1) | ELISA | Breast cancer (178), controls (99) | [67] |
| SOX2 | ELISA | Breast cancer (282), benign disease (78), healthy (194) | [68] |
| SCP-1, SSX-2 and NY-ESO-1 | ELISA | Breast cancer patients (100) | [69] |
| Thioredoxin-like 2 (TXNL2) | Protein array, dot blot | Discovery phase, breast cancer (<10) | [70] |
| interleukin 29, osteoprotegerin, survivin, growth hormone, and resistin | Autoantibody Profiling System (APS) | Discovery phase, breast cancer (<10) | [71] |
| CYP4Z1 | ELISA | Breast cancer (19), controls (11) | [72] |
| p16, c-myc, TP53, and ANXA-1 | ELISA | Breast cancer (102), controls (146) | [73] |
| Thymidylate synthase (TYMS) and C-terminal LIM domain protein 1 (PDLIM1) | ELISA | Breast cancer (30), controls (30) | [74] |
| Estrogen receptor alpha | ELISA | Breast cancer (48) | [75] |
| ALDOA, ENO1, GAPDH, PKM2, and TPI1 | Proteomics, ELSIA | Prediagnostic ER+/PR+ breast cancer (48), healthy controls (65) | [76] |
| RBP-Jκ, HMGN1, PSRC1, CIRBP, and ECHDC1 | ELISA | Invasive breast cancer (IBC, 59), ductal carcinoma in situ (DCIS, 61) | [77] |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Qiu, J.; Keyser, B.; Lin, Z.-T.; Wu, T. Autoantibodies as Potential Biomarkers in Breast Cancer. Biosensors 2018, 8, 67. https://0-doi-org.brum.beds.ac.uk/10.3390/bios8030067
AMA Style
Qiu J, Keyser B, Lin Z-T, Wu T. Autoantibodies as Potential Biomarkers in Breast Cancer. Biosensors. 2018; 8(3):67. https://0-doi-org.brum.beds.ac.uk/10.3390/bios8030067
Chicago/Turabian StyleQiu, Jingyi, Bailey Keyser, Zuan-Tao Lin, and Tianfu Wu. 2018. "Autoantibodies as Potential Biomarkers in Breast Cancer" Biosensors 8, no. 3: 67. https://0-doi-org.brum.beds.ac.uk/10.3390/bios8030067
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.