Behavioural and Emotional Changes during COVID-19 Lockdown in an Italian Paediatric Population with Neurologic and Psychiatric Disorders

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Measures
2.2.1. The General Questionnaire
2.2.2. Child Behaviour Check List (CBCL)
2.3. The Online Platform: REDCap
2.4. Statistical Methods
3. Results
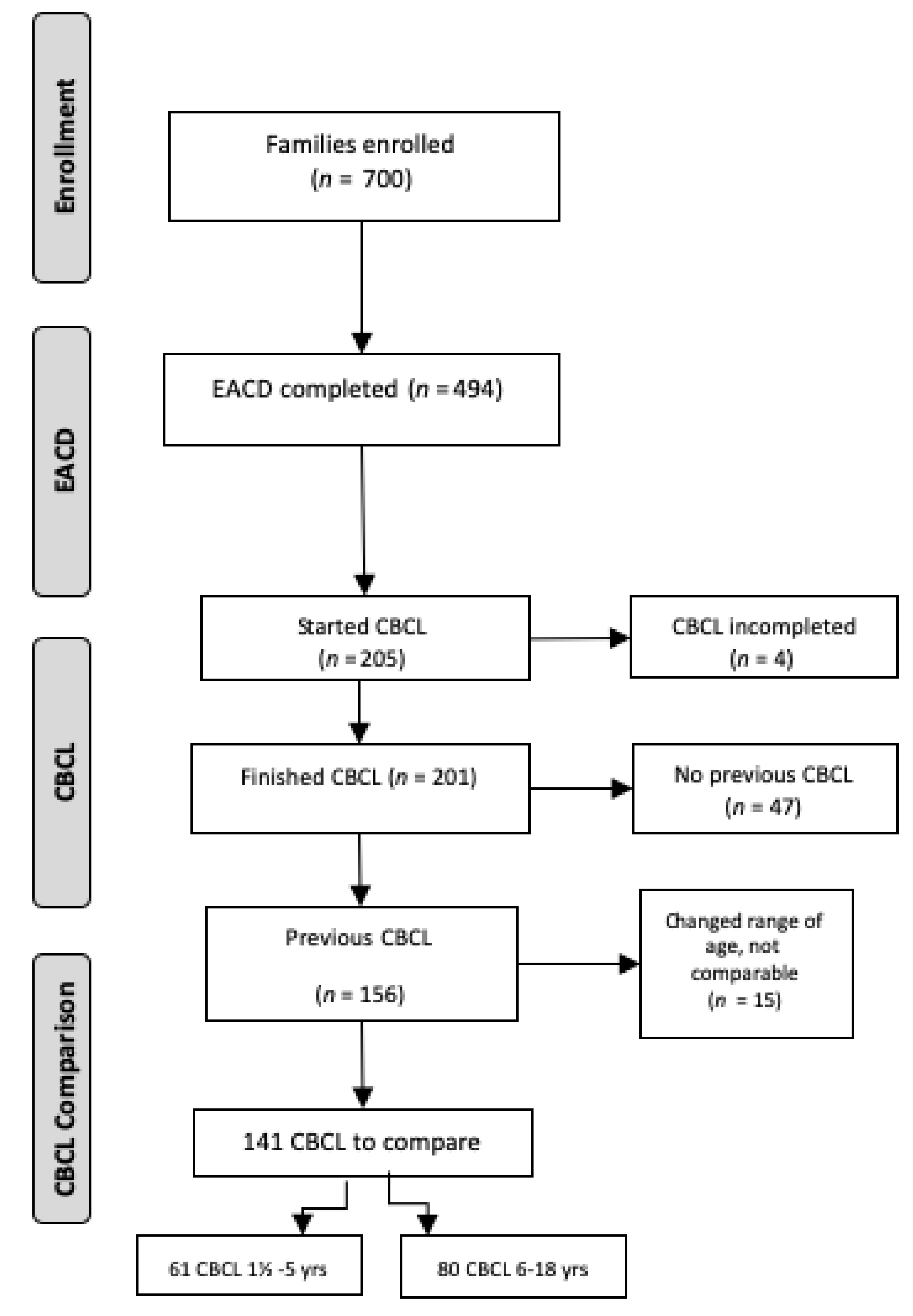
3.1. Enrollment and Population Description
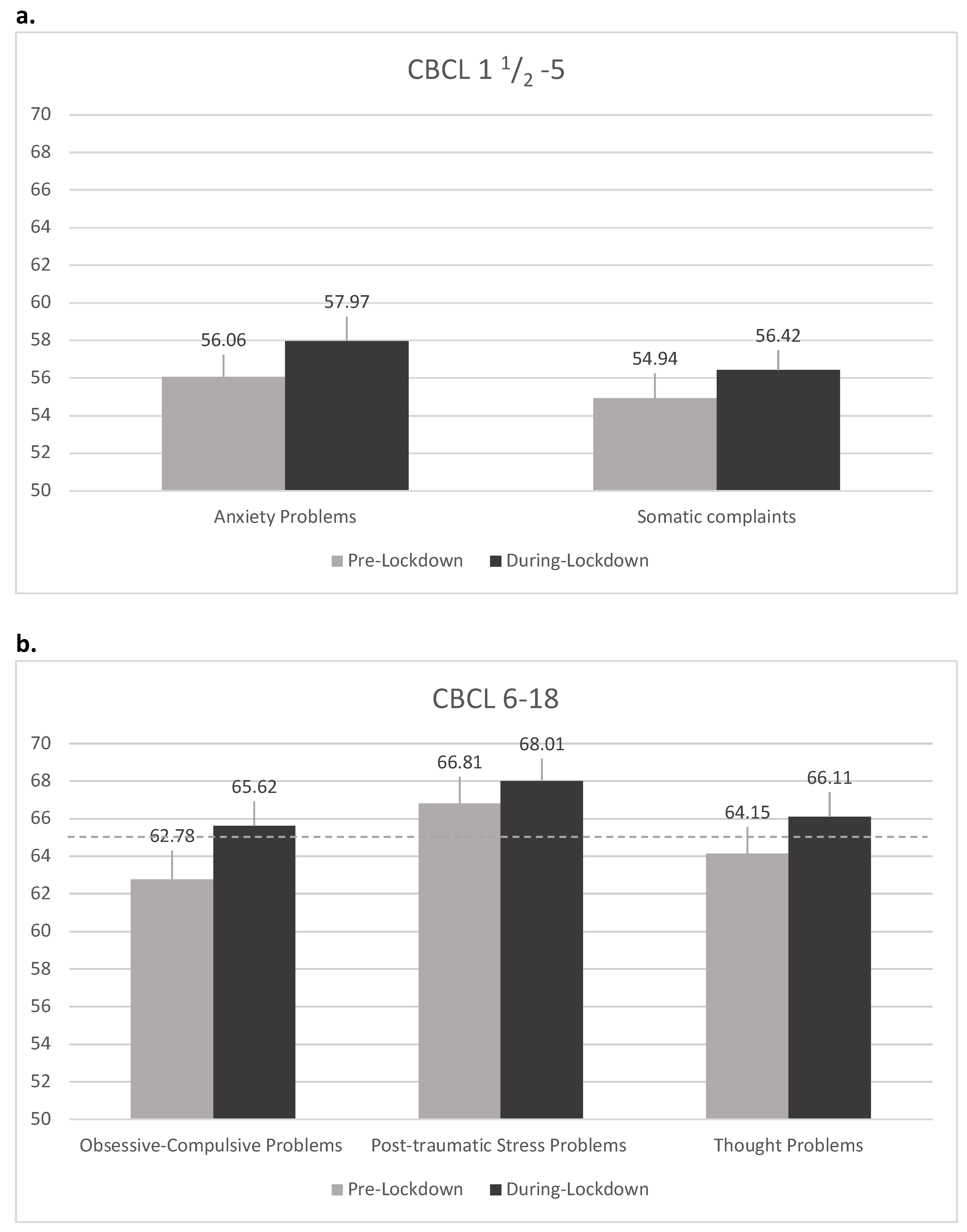
3.2. Pre- vs. During Lockdown Comparisons
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Blendon, R.J.; Benson, J.M.; DesRoches, C.M.; Raleigh, E.; Taylor-Clark, K. The public’s response to severe acute respiratory syndrome in Toronto and the United States. Clin. Infect. Dis. 2004, 38, 925–931. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caleo, G.; Duncombe, J.; Jephcott, F.; Lokuge, K.; Mills, C.; Looijen, E.; Theoharaki, F.; Kremer, R.; Kleijer, K.; Squire, J.; et al. The factors affecting household transmission dynamics and community compliance with Ebola control measures: A mixed-methods study in a rural village in Sierra Leone. BMC Public Health 2018, 18. [Google Scholar] [CrossRef] [PubMed]
- Cava, M.A.; Fay, K.E.; Beanlands, H.J.; McCay, E.A.; Wignall, R. The experience of quarantine for individuals affected by SARS in Toronto. Public Health Nurs. 2005, 22, 398–406. [Google Scholar] [CrossRef] [PubMed]
- DiGiovanni, C.; Conley, J.; Chiu, D.; Zaborski, J. Factors influencing compliance with quarantine in Toronto during the 2003 SARS outbreak. Biosecur. Bioterror. 2004, 2, 265–272. [Google Scholar] [CrossRef]
- Hawryluck, L.; Gold, W.L.; Robinson, S.; Pogorski, S.; Galea, S.; Styra, R. SARS control and psychological effects of quarantine, Toronto, Canada. Emerg. Infect. Dis. 2004, 10, 1206–1212. [Google Scholar] [CrossRef]
- Jeong, H.; Yim, H.W.; Song, Y.J.; Ki, M.; Min, J.A.; Cho, J.; Chae, J.H. Mental health status of people isolated due to Middle East Respiratory Syndrome. Epidemiol. Health 2016, 38, e2016048. [Google Scholar] [CrossRef]
- Lee, S.; Chan, L.Y.Y.; Chau, A.M.Y.; Kwok, K.P.S.; Kleinman, A. The experience of SARS-related stigma at Amoy Gardens. Soc. Sci. Med. 2005, 61, 2038–2046. [Google Scholar] [CrossRef]
- Pellecchia, U.; Crestani, R.; Decroo, T.; Van Den Bergh, R.; Al-Kourdi, Y. Social consequences of ebola containment measures in Liberia. PLoS ONE 2015, 10. [Google Scholar] [CrossRef] [Green Version]
- Wilken, J.A.; Pordell, P.; Goode, B.; Jarteh, R.; Miller, Z.; Saygar, B.G.; Maximore, L.; Borbor, W.M.; Carmue, M.; Walker, G.W.; et al. Knowledge, attitudes, and practices among members of households actively monitored or quarantined to prevent transmission of ebola virus disease-margibi county, liberia: February-march 2015. Prehosp. Disaster Med. 2017, 32, 673–678. [Google Scholar] [CrossRef]
- Yoon, M.K.; Kim, S.Y.; Ko, H.S.; Lee, M.S. System effectiveness of detection, brief intervention and refer to treatment for the people with post-traumatic emotional distress by MERS: A case report of community-based proactive intervention in South Korea. Int. J. Ment. Health Syst. 2016, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bai, Y.M.; Lin, C.C.; Lin, C.Y.; Chen, J.Y.; Chue, C.M.; Chou, P. Survey of stress reactions among health care workers involved with the SARS outbreak. Psychiatr. Serv. 2004, 55, 1055–1057. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Kakade, M.; Fuller, C.J.; Fan, B.; Fang, Y.; Kong, J.; Guan, Z.; Wu, P. Depression after exposure to stressful events: Lessons learned from the severe acute respiratory syndrome epidemic. Compr. Psychiatry 2012, 53, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Marjanovic, Z.; Greenglass, E.R.; Coffey, S. The relevance of psychosocial variables and working conditions in predicting nurses’ coping strategies during the SARS crisis: An online questionnaire survey. Int. J. Nurs. Stud. 2007, 44, 991–998. [Google Scholar] [CrossRef]
- Wu, P.; Liu, X.; Fang, Y.; Fan, B.; Fuller, C.J.; Guan, Z.; Yao, Z.; Kong, J.; Lu, J.; Litvak, I.J. Alcohol abuse/dependence symptoms among hospital employees exposed to a SARS outbreak. Alcohol Alcohol. 2008, 43, 706–712. [Google Scholar] [CrossRef]
- Braunack-Mayer, A.; Tooher, R.; Collins, J.E.; Street, J.M.; Marshall, H. Understanding the school community’s response to school closures during the H1N1 2009 influenza pandemic. BMC Public Health 2013, 13. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Xu, B.; Zhao, G.; Cao, R.; He, X.; Fu, S. Is quarantine related to immediate negative psychological consequences during the 2009 H1N1 epidemic? Gen. Hosp. Psychiatry 2011, 33, 75–77. [Google Scholar] [CrossRef]
- Desclaux, A.; Badji, D.; Ndione, A.G.; Sow, K. Accepted monitoring or endured quarantine? Ebola contacts’ perceptions in Senegal. Soc. Sci. Med. 2017, 178, 38–45. [Google Scholar] [CrossRef]
- Reynolds, D.L.; Garay, J.R.; Deamond, S.L.; Moran, M.K.; Gold, W.; Styra, R. Understanding, compliance and psychological impact of the SARS quarantine experience. Epidemiol. Infect. 2008, 136, 997–1007. [Google Scholar] [CrossRef]
- Mihashi, M.; Otsubo, Y.; Yinjuan, X.; Nagatomi, K.; Hoshiko, M.; Ishitake, T. Predictive Factors of Psychological Disorder Development During Recovery Following SARS Outbreak. Health Psychol. 2009, 28, 91–100. [Google Scholar] [CrossRef]
- Robertson, E.; Hershenfield, K.; Grace, S.L.; Stewart, D.E. The psychosocial effects of being quarantined following exposure to SARS: A qualitative study of Toronto health care workers. Can. J. Psychiatry 2004, 49, 403–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, M.R.; Agho, K.E.; Stevens, G.J.; Raphael, B. Factors influencing psychological distress during a disease epidemic: Data from Australia’s first outbreak of equine influenza. BMC Public Health 2008, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wester, M.; Giesecke, J. Ebola and healthcare worker stigma. Scand. J. Public Health 2019, 47, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Sprang, G.; Silman, M. Posttraumatic stress disorder in parents and youth after health-related disasters. Disaster Med. Public Health Prep. 2013, 7, 105–110. [Google Scholar] [CrossRef]
- Feo, P.; Di Gioia, S.; Carloni, E.; Vitiello, B.; Tozzi, A.E.; Vicari, S. Prevalence of psychiatric symptoms in children and adolescents one year after the 2009 L’Aquila earthquake. BMC Psychiatry 2014, 14. [Google Scholar] [CrossRef] [Green Version]
- Vijayakumar, L.; Kannan, G.K.; Daniel, S.J. Mental health status in children exposed to tsunami. Int. Rev. Psychiatry 2006, 18, 507–513. [Google Scholar] [CrossRef]
- Sourander, A. Behavior problems and traumatic events of unaccompanied refugee minors. Child Abus. Negl. 1998, 22, 719–727. [Google Scholar] [CrossRef]
- Mclaughlin, K.A.; Fairbank, J.A.; Gruber, M.J.; Jones, R.T.; Lakoma, M.D.; Pfefferbaum, B.; Sampson, N.A.; Kessler, R.C. Serious Emotional Disturbance Among Youths Exposed to Hurricane Katrina 2 Years Postdisaster. J. Am. Acad. Child Adolesc. Psychiatry 2009, 48, 1069–1078. [Google Scholar] [CrossRef] [Green Version]
- Qiu, J.; Shen, B.; Zhao, M.; Wang, Z.; Xie, B.; Xu, Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: Implications and policy recommendations. Gen. Psychiatry 2020, 33, e100213. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Zhao, X.; Feng, Q.; Liu, L.; Yao, Y.; Shi, J. Psychological assistance during the coronavirus disease 2019 outbreak in China. J. Health Psychol. 2020, 733–737. [Google Scholar] [CrossRef]
- Flaudias, V.; Iceta, S.; Zerhouni, O.; Rodgers, R.F.; Billieux, J.; Llorca, P.M.; Boudesseul, J.; Chazeron, I.D.E.; Romo, L.; Maurage, P.; et al. COVID-19 pandemic lockdown and problematic eating behaviors in a student population. J. Behav. Addict. 2020, 9, 826–835. [Google Scholar] [CrossRef] [PubMed]
- Achenbach, T.; Rescorla, L. Manual for the ASEBA School-Age Forms and Profiles: An Integrated System of Multi-Informant Assessment; University of Vermont, Research Center for Children, Youth, & Families: Burlington, VT, USA, 2001. [Google Scholar]
- Kaufman, J.; Birmaher, B.; Brent, D.; Rao, U.; Flynn, C.; Moreci, P.; Williamson, D.; Ryan, N. Schedule for affective disorders and schizophrenia for school-age children-present and lifetime version (K-SADS-PL): Initial reliability and validity data. J. Am. Acad. Child Adolesc. Psychiatry 1997, 36, 980–988. [Google Scholar] [CrossRef] [PubMed]
- Lord, C.; Rutter, M.; DiLavore, P.; Risi, S.; Gotham, K.; Bishop, S. Autism Diagnostic Observation Schedule (ADOS-2), 2nd ed.; WWW Document; Los Angeles West. Psychol. Corp: New York, NY, USA, 2012; Available online: https://www.wpspublish.com/ados-2-autism-diagnostic-observation-schedule-second-edition (accessed on 22 February 2020).
- Rutter, M.; LeCouteur, A.; Lord, C. Autism Diagnostic Interview-Revised (ADI-R); WPS: Torrance, CA, USA, 2012. [Google Scholar]
- Racine, N.; Cooke, J.E.; Eirich, R.; Korczak, D.J.; McArthur, B.A.; Madigan, S. Child and adolescent mental illness during COVID-19: A rapid review. Psychiatry Res. 2020, 292. [Google Scholar] [CrossRef] [PubMed]
- Bitsika, V.; Sharpley, C.F.; Andronicos, N.M.; Agnew, L.L. Prevalence, structure and correlates of anxiety-depression in boys with an autism spectrum disorder. Res. Dev. Disabil. 2016, 49–50, 302–311. [Google Scholar] [CrossRef] [PubMed]
- Colizzi, M.; Bortoletto, R.; Silvestri, M.; Mondini, F.; Puttini, E.; Cainelli, C.; Gaudino, R.; Ruggeri, M.; Zoccante, L. Medically unexplained symptoms in the times of Covid-19 pandemic: A case-report. Brain, Behav. Immun. Health 2020, 100073. [Google Scholar] [CrossRef] [PubMed]
- Serra Giacobo, R.; Jané, M.C.; Bonillo, A.; Ballespí, S.; Díaz-Regañon, N. Somatic symptoms, severe mood dysregulation, and aggressiveness in preschool children. Eur. J. Pediatr. 2012, 171, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Xie, X.; Xue, Q.; Zhou, Y.; Zhu, K.; Liu, Q.; Zhang, J.; Song, R. Mental health status among children in home confinement during the coronavirus disease 2019 outbreak in Hubei Province, China. JAMA Pediatr. 2020, 174, 898–900. [Google Scholar] [CrossRef] [Green Version]
- Zhou, S.J.; Zhang, L.G.; Wang, L.L.; Guo, Z.C.; Wang, J.Q.; Chen, J.C.; Liu, M.; Chen, X.; Chen, J.X. Prevalence and socio-demographic correlates of psychological health problems in Chinese adolescents during the outbreak of COVID-19. Eur. Child Adolesc. Psychiatry 2020, 29, 749–758. [Google Scholar] [CrossRef]
- England, M.J.; Sim, L.J. Depression in Parents, Parenting, and Children: Opportunities to Improve Identification, Treatment, and Prevention; National Academies Press: Washingon, DC, USA, 2009; ISBN 0309121787. [Google Scholar]
- Liu, N.; Zhang, F.; Wei, C.; Jia, Y.; Shang, Z.; Sun, L.; Wu, L.; Sun, Z.; Zhou, Y.; Wang, Y.; et al. Prevalence and predictors of PTSS during COVID-19 outbreak in China hardest-hit areas: Gender differences matter. Psychiatry Res. 2020, 287, 112921. [Google Scholar] [CrossRef]
- Willner, P.; Rose, J.; Stenfert Kroese, B.; Murphy, G.H.; Langdon, P.E.; Clifford, C.; Hutchings, H.; Watkins, A.; Hiles, S.; Cooper, V. Effect of the COVID-19 pandemic on the mental health of carers of people with intellectual disabilities. J. Appl. Res. Intellect. Disabil. 2020. [Google Scholar] [CrossRef]
- Sockalingam, S.; Leung, S.E.; Cassin, S.E. The Impact of COVID-19 on Bariatric Surgery: Re-Defining Psychosocial Care. Obesity (Silver Spring) 2020. [Google Scholar] [CrossRef] [Green Version]
- Tanir, Y.; Karayagmurlu, A.; Kaya, İ.; Kaynar, T.B.; Türkmen, G.; Dambasan, B.N.; Meral, Y.; Coşkun, M. Exacerbation of obsessive compulsive disorder symptoms in children and adolescents during COVID-19 pandemic. Psychiatry Res. 2020, 293. [Google Scholar] [CrossRef] [PubMed]
- Scahill, L.; Riddle, M.A.; McSwiggin-Hardin, M.; Ort, S.I.; King, R.A.; Goodman, W.K.; Cicchetti, D.; Leckman, J.F. Children’s Yale-Brown Obsessive Compulsive Scale: Reliability and validity. J. Am. Acad. Child Adolesc. Psychiatry 1997, 36, 844–852. [Google Scholar] [CrossRef] [PubMed]
- Liang, L.; Ren, H.; Cao, R.; Hu, Y.; Qin, Z.; Li, C.; Mei, S. The Effect of COVID-19 on Youth Mental Health. Psychiatr. Q. 2020. [Google Scholar] [CrossRef] [PubMed]
- Bobo, E.; Lin, L.; Acquaviva, E.; Caci, H.; Franc, N.; Gamon, L.; Picot, M.C.; Pupier, F.; Speranza, M.; Falissard, B.; et al. How do children and adolescents with Attention Deficit Hyperactivity Disorder (ADHD) experience lockdown during the COVID-19 outbreak? Encephale 2020, 46, S85–S92. [Google Scholar] [CrossRef]
- Reising, M.M.; Watson, K.H.; Hardcastle, E.J.; Merchant, M.J.; Roberts, L.; Forehand, R.; Compas, B.E. Parental Depression and Economic Disadvantage: The Role of Parenting in Associations with Internalizing and Externalizing Symptoms in Children and Adolescents. J. Child Fam. Stud. 2013, 22, 335–343. [Google Scholar] [CrossRef] [Green Version]
- Fegert, J.M.; Vitiello, B.; Plener, P.L.; Clemens, V. Challenges and burden of the Coronavirus 2019 (COVID-19) pandemic for child and adolescent mental health: A narrative review to highlight clinical and research needs in the acute phase and the long return to normality. Child Adolesc. Psychiatry Ment. Health 2020, 14. [Google Scholar] [CrossRef]
- Joel, D.; McCarthy, M.M. Incorporating Sex As a Biological Variable in Neuropsychiatric Research: Where Are We Now and Where Should We Be? Neuropsychopharmacology 2017, 42, 1–7. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| INT Problems | EXT Problems | Total Problems | Stress Problems | Affective Problems | Anxiety Problems | PDD | ADHP | ODP | Emotionally Reactive | Anxious/Depressed | Somatic Complaints | Withdrawn | Sleep Problems | Attention Problems | Aggressive Behaviour | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Intercept | 8.041 | 10.732 | 12.767 | 12.789 | 4.245 | 6.929 | 10.376 | 9.272 | 5.908 | 3.063 | 7.007 | 8.454 | 10.186 | 1.637 | 5.022 | 5.345 |
| Neurological Disorders | −1.355 | 2.157 | −0.996 | −6.332 | 2.749 | −8.143 ** | 2.009 | −0.358 | 1.058 | −1.502 | −4.056 | 1.224 | −3.306 | 3.130 | 2.673 | 2.579 |
| Emotional and Behavioural Disorders | −3.353 | −0.014 | −1.655 | −4.599 ** | 0.047 | −2.462 | −5.19 ** | −0.875 | 1.153 | −1.816 | −1.017 | 0.363 | −2.180 | 1.747 | 0.795 | −0.037 |
| Neuro-Developmental Disorders | −3.591 | −7.699 | −6.472 | −7.410 | 1.368 | −4.880 | 3.960 | −4.781 | −5.66 | −1.073 | −7.497 | −5.359 | −6.836 | 4.557 | 1.246 | −5.045 |
| Treatment pre-lockdown (hrs/week) | 0.143 | 0.178 | 0.256 | −0.257 | 0.346 | −0.262 | −0.162 | 0.529 | −.0.21 | 0.440 | −0.002 | −0.245 | 0.217 | 0.187 | 0.066 | −0.379 |
| Age | −1.289 | −1.245 | −1.976 ** | −0.903 | −1.525 | −0.566 | −1.133 | −1.88 ** | −0.45 | −1.046 | −0.290 | −1.264 | −1.108 | −2.071 * | −2.079 * | 0.041 |
| Financial hardship during Covid | 1.884 | 0.857 | 1.329 | 0.561 | −0.826 | 2.009 | 3.607 * | 2.212 | 2.202 | 1.550 | 2.275 | 0.882 | 2.668 | 0.791 | 2.224 | 0.792 |
| INT P | EXT P | Total P | SCT | OCP | PTSP | Aff P | Anx P | Som P | ADHP | ODP | CP | AD | WD | SC | SP | TP | AT | RBB | AB | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Intercept | −7.924 | −1.836 | −6.020 | −0.650 | −3.631 | −4.046 | −7.937 | −5.329 | −2.819 | −6.012 | 2.747 | −0.948 | −6.748 | −9.159 | −1.503 | −4.412 | −3.357 | −4.826 | −3.017 | −3.404 |
| Neuolog Disorders | 0.693 | 0.017 | −0.435 | −3.552 | 2.375 | −0.299 | −2.299 | 0.643 | −1.555 | 1.593 | −1.282 | −0.856 | 0.452 | 0.187 | −1.236 | −1.097 | −1.483 | −1.276 | 1.278 | −2.170 |
| Emotional BehaviourDisorders | 4.091 * | 4.020 * | 4.658 * | 1.387 | 2.364 | 1.821 | 3.843 * | 1.408 | 1.608 | 3.784 * | 1.206 | 0.078 | 2.219 | 2.888 | 2.964 | 1.753 | 0.958 | 4.756 ** | 0.555 | 3.232 |
| Neuro-DevelopmDisorders | 0.725 | −0.405 | 0.299 | −1.982 | −1.525 | 0.223 | 0.221 | −0.376 | 2.182 | 2.651 | −3.203 ** | 0.494 | −0.262 | 2.956 | 0.135 | 0.511 | 1.110 | −1.582 | 1.281 | −1.168 |
| Treatment pre-LD (hrs/week) | 0.571 | −0.040 | 0.298 | 0.008 | 1.125 | 0.481 | 0.322 | 0.760 * | 0.290 | 0.049 | 0.396 | 0.054 | 0.681 | 0.319 | 0.219 | 0.470 | −0.346 | 0.143 | 0.128 | 0.463 |
| Age | 0.445 * | −0.024 | 0.263 | 0.204 | 0.111 | 0.145 | 0.539 ** | 0.156 | −0.015 | 0.040 | −0.155 | 0.062 | 0.344 | 0.619 ** | −0.058 | 0.184 | 0.249 | 0.193 | 0.103 | 0.066 |
| Financial Hardship | −3.808 ** | −1.203 | −2.959 ** | −1.186 | −3.248 * | −2.540 * | −1.288 | 0.409 | −1.615 | −1.497 | −0.743 | −0.239 | −1.706 | −4.523 ** | −3.340 ** | 1.149 | −2.644 | −1.866 | −0.038 | 0.527 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Conti, E.; Sgandurra, G.; De Nicola, G.; Biagioni, T.; Boldrini, S.; Bonaventura, E.; Buchignani, B.; Della Vecchia, S.; Falcone, F.; Fedi, C.; et al. Behavioural and Emotional Changes during COVID-19 Lockdown in an Italian Paediatric Population with Neurologic and Psychiatric Disorders. Brain Sci. 2020, 10, 918. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10120918
Conti E, Sgandurra G, De Nicola G, Biagioni T, Boldrini S, Bonaventura E, Buchignani B, Della Vecchia S, Falcone F, Fedi C, et al. Behavioural and Emotional Changes during COVID-19 Lockdown in an Italian Paediatric Population with Neurologic and Psychiatric Disorders. Brain Sciences. 2020; 10(12):918. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10120918
Chicago/Turabian StyleConti, Eugenia, Giuseppina Sgandurra, Giacomo De Nicola, Tommaso Biagioni, Silvia Boldrini, Eleonora Bonaventura, Bianca Buchignani, Stefania Della Vecchia, Francesca Falcone, Caterina Fedi, and et al. 2020. "Behavioural and Emotional Changes during COVID-19 Lockdown in an Italian Paediatric Population with Neurologic and Psychiatric Disorders" Brain Sciences 10, no. 12: 918. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10120918