
Explicit Training to Improve Affective Prosody Recognition in Adults with Acute Right Hemisphere Stroke

 , , ,
, , ,
Abstract
:1. Introduction
Research Questions and Hypotheses
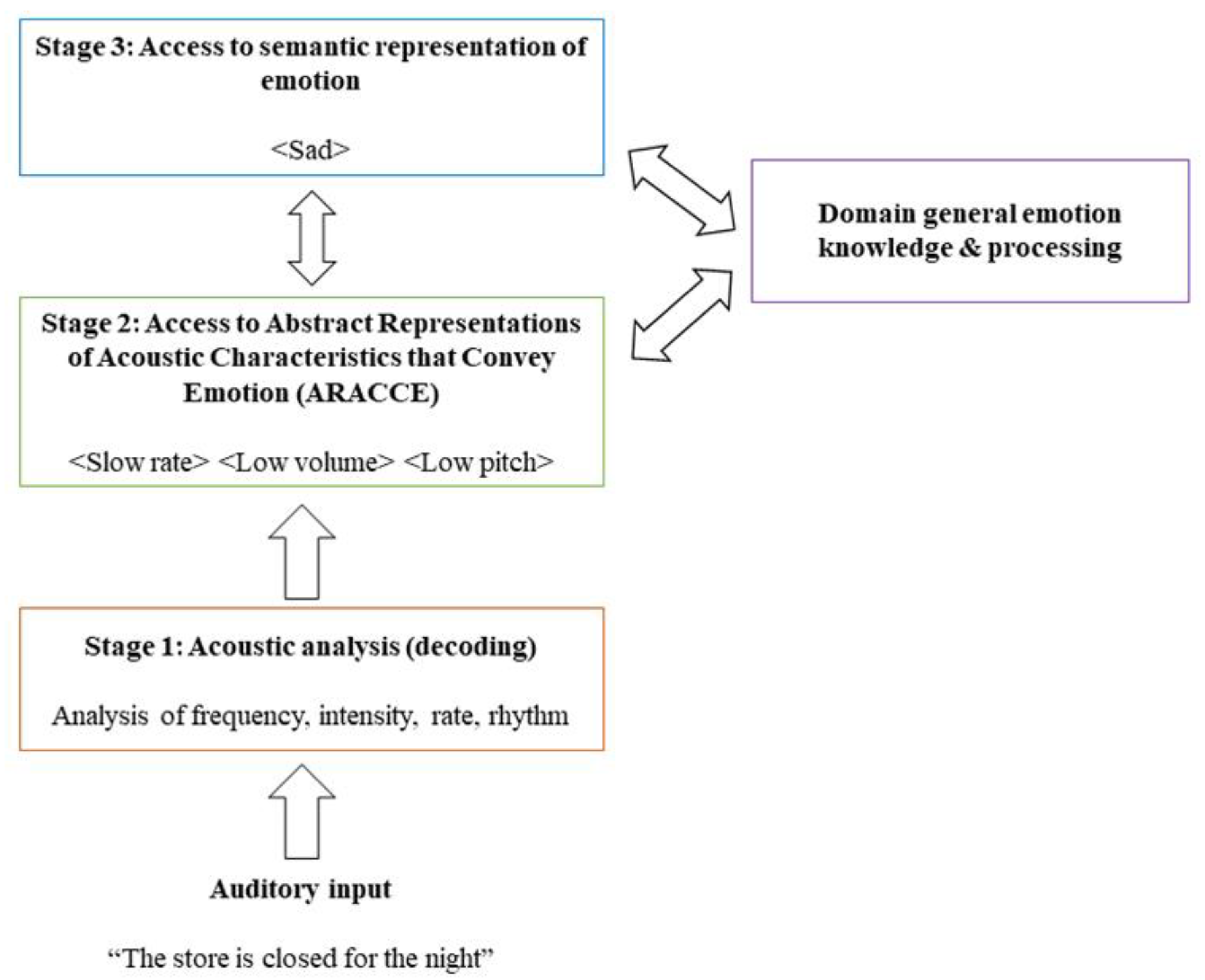
- Does affective prosody recognition improve following acoustic-prosodic-emotion recognition training?Since training tasks target Stages 1 and 2 of affective prosody recognition, it is expected that recognition will improve after training in individuals with deficits at these processing stages.
- Does behavioral impairment locus impact training effectiveness?If Stage 1 (perceptual) deficits are related to more severe prosody recognition impairments, then these individuals are predicted to benefit more from training compared to individuals with Stage 2 (conceptual) deficits that result in less severe affective prosody recognition impairments.
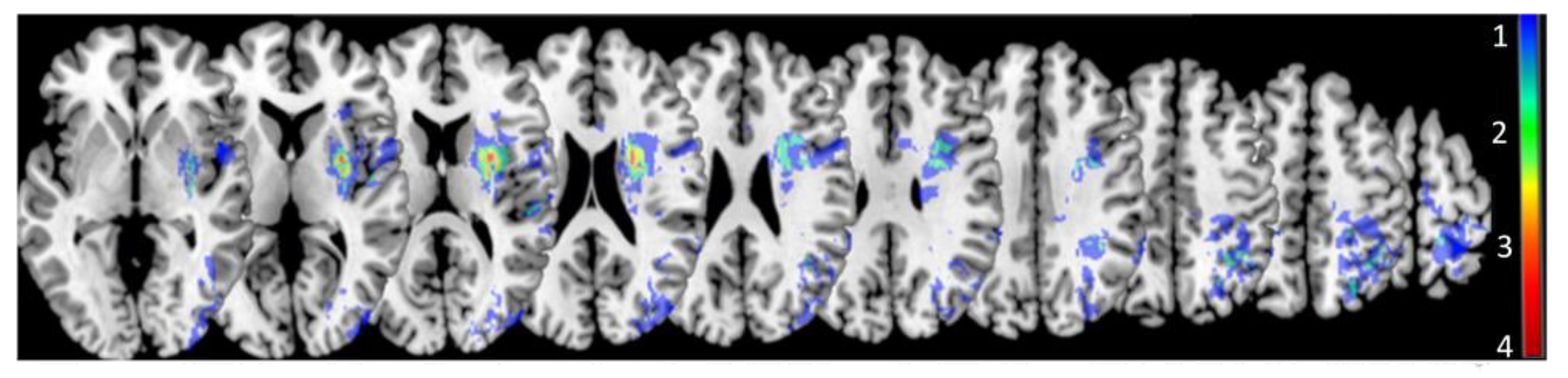
- Are distinct lesion loci observed for different behavioral impairment loci?Based on previous work and models of receptive aprosodia, distinct lesion loci are predicted for Stage 1 and 2 deficits. Maximal lesion overlap is predicted to occur within posterior and subcortical ventral stream regions (e.g., superior posterior temporal gyrus, basal ganglia, thalamus) for Stage 1 deficits and within more frontal ventral stream regions (e.g., inferior frontal lobe) for Stage 2 deficits.
- Does degree of impaired tissue (acute lesion and/or hypoperfusion) predict affective prosody recognition training effectiveness?It is hypothesized that more severe damage and hypoperfusion to right hemisphere ventral stream/subcortical regions will result in worse deficits in prosody recognition, and thus, greater benefit from training.
2. Method
2.1. Participants
Diagnosing Receptive Aprosodia and Determining Locus of Impairment
2.2. Stimuli and Procedures
2.2.1. Affective Prosody Recognition
2.2.2. Acoustic Feature (Stage 1) Training
2.2.3. Prosodic Feature (Stage 1) Training
2.2.4. ARACCE (Stage 2) Training
2.3. Imaging
2.4. Analyses
3. Results
3.1. Participants with RHD and Receptive Aprosodia
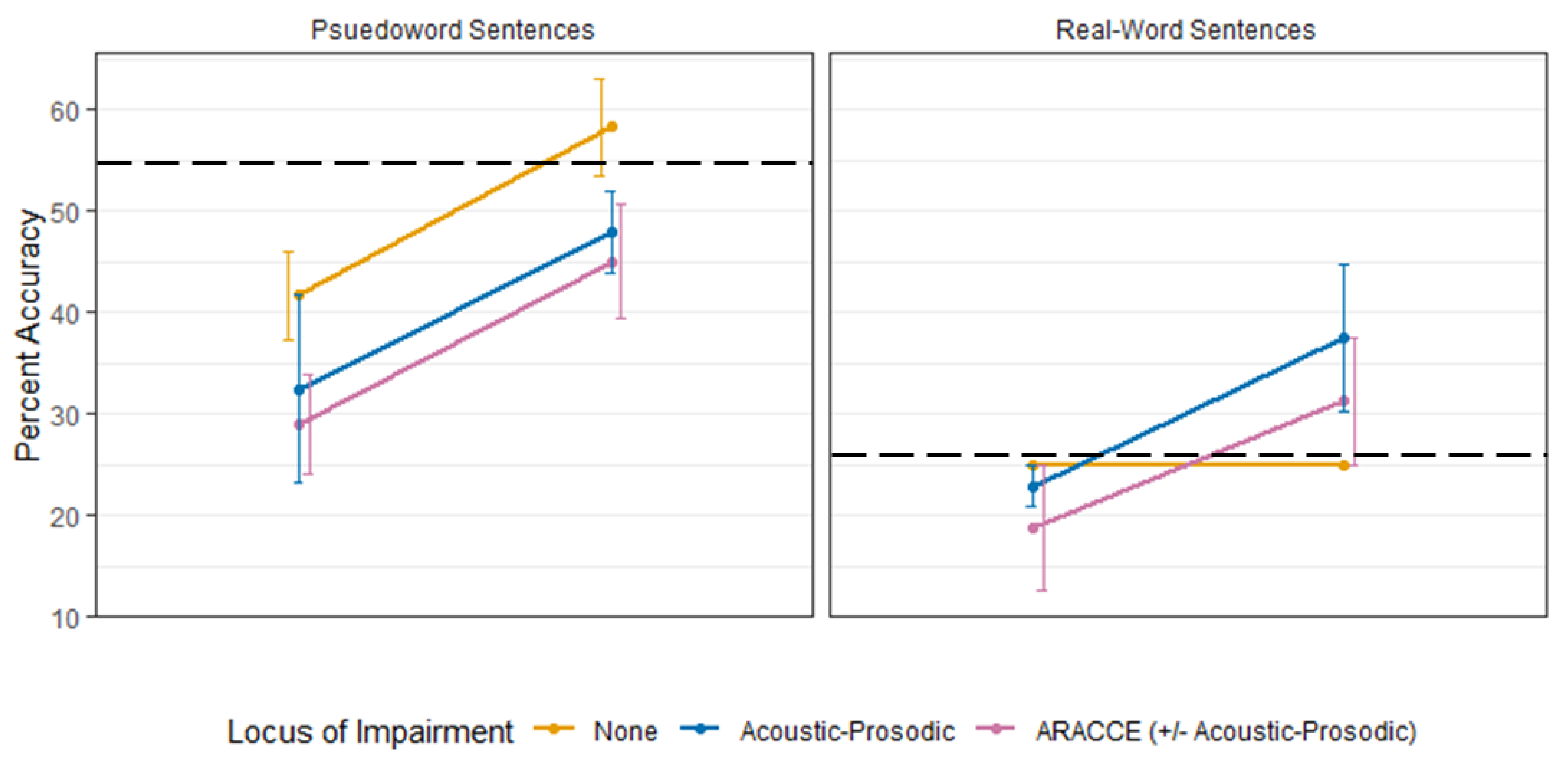
3.2. Affective Prosody Recognition Training Effectiveness (Q1, Q2)
3.3. Lesion Contributions to Affective Prosody Recognition Training (Q3 and Q4)
4. Discussion
4.1. Behavioral Contributions to Affective Prosody Recognition Training (Q1 and Q2)
4.2. Lesion Contributions to Affective Prosody Recognition Training (Q3 and Q4)
4.3. Limitations and Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Patel, S.; Oishi, K.; Wright, A.; Sutherland-Foggio, H.; Saxena, S.; Sheppard, S.M.; Hillis, A.E. Right hemisphere regions critical for expression of emotion through prosody. Front. Neurol. 2018, 9. [Google Scholar] [CrossRef]
- Wright, A.; Saxena, S.; Sheppard, S.M.; Hillis, A.E. Selective impairments in components of affective prosody in neurologically impaired individuals. Brain Cogn. 2018, 124, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Leung, J.H.; Purdy, S.C.; Tippett, L.J.; Leão, S.H.S. Affective speech prosody perception and production in stroke patients with left-hemispheric damage and healthy controls. Brain Lang. 2017, 166, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Martinez, M.; Multani, N.; Anor, C.J.; Misquitta, K.; Tang-Wai, D.F.; Keren, R.; Fox, S.; Lang, A.E.; Marras, C.; Tartaglia, M.C. Emotion detection deficits and decreased empathy in patients with Alzheimer’s disease and Parkinson’s disease affect caregiver mood and burden. Front. Aging Neurosci. 2018, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ilie, G.; Cusimano, M.D.; Li, W. Prosodic processing post traumatic brain injury—A systematic review. Syst. Rev. 2017, 6, 1. [Google Scholar] [CrossRef] [Green Version]
- Knight, M.J.; Baune, B.T. Cognitive dysfunction in Major Depressive Disorder. Curr. Opin. Psychiatry 2018, 31, 26–31. [Google Scholar] [CrossRef]
- Hillis, A.E.; Tippett, D.C. Stroke recovery: Surprising influences and residual consequences. Adv. Med. 2014, 2014. [Google Scholar] [CrossRef] [Green Version]
- Blonder, L.X.; Pettigrew, L.C.; Kryscio, R.J. Emotion recognition and marital satisfaction in stroke. J. Clin. Exp. Neuropsychol. 2012, 34, 634–642. [Google Scholar] [CrossRef]
- Ross, E.D. The aprosodias. Functional-anatomic organization of the affective components of language in the right hemisphere. Arch. Neurol. 1981, 38, 561–569. [Google Scholar] [CrossRef]
- Fridriksson, J.; den Ouden, D.-B.; Hillis, A.E.; Hickok, G.; Rorden, C.; Basilakos, A.; Yourganov, G.; Bonilha, L. Anatomy of aphasia revisited. Brain 2018, 141, 848–862. [Google Scholar] [CrossRef] [PubMed]
- Hickok, G.; Poeppel, D. Dorsal and ventral streams: A framework for understanding aspects of the functional anatomy of language. Cognition 2004, 92, 67–99. [Google Scholar] [CrossRef] [PubMed]
- Hickok, G.; Poeppel, D. The cortical organization of speech processing. Nat. Rev. Neurosci. 2007, 8, 393–402. [Google Scholar] [CrossRef] [PubMed]
- Sammler, D.; Grosbras, M.-H.; Anwander, A.; Bestelmeyer, P.E.G.; Belin, P. Dorsal and ventral pathways for prosody. Curr. Biol. 2015, 25, 3079–3085. [Google Scholar] [CrossRef] [Green Version]
- Schirmer, A.; Kotz, S.A. Beyond the right hemisphere: Brain mechanisms mediating vocal emotional processing. Trends Cogn. Sci. 2006, 10, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Sheppard, S.M.; Keator, L.M.; Breining, B.L.; Wright, A.E.; Saxena, S.; Tippett, D.C.; Hillis, A.E. Right hemisphere ventral stream for emotional prosody identification: Evidence from acute stroke. Neurology 2020, 94, e1013–e1020. [Google Scholar] [CrossRef]
- Baum, S.R.; Pell, M.D. Production of affective and linguistic prosody by brain-damaged patients. Aphasiology 1997, 11, 177–198. [Google Scholar] [CrossRef]
- Darby, D.G. Sensory Aprosodia: A clinical clue to lesions of the inferior division of the right middle cerebral artery? Neurology 1993, 43, 567–572. [Google Scholar] [CrossRef]
- Gorelick, P.B.; Ross, E.D. The aprosodias: Further functional-anatomical evidence for the organisation of affective language in the right hemisphere. J. Neurol. Neurosurg. Psychiatry 1987, 50, 553–560. [Google Scholar] [CrossRef] [Green Version]
- Hughes, C.P.; Chan, J.L.; Su, M.S. Aprosodia in Chinese patients with right cerebral hemisphere lesions. Arch. Neurol. 1983, 40, 732–736. [Google Scholar] [CrossRef]
- Ross, E.D.; Monnot, M. Neurology of affective prosody and its functional-anatomic organization in right hemisphere. Brain Lang. 2008, 104, 51–74. [Google Scholar] [CrossRef]
- Starkstein, S.E.; Federoff, J.P.; Price, T.R.; Leiguarda, R.C.; Robinson, R.G. Neuropsychological and neuroradiologic correlates of emotional prosody comprehension. Neurology 1994, 44, 515–522. [Google Scholar] [CrossRef] [PubMed]
- Witteman, J.; Van Heuven, V.J.P.; Schiller, N.O. Hearing feelings: A quantitative meta-analysis on the neuroimaging literature of emotional prosody perception. Neuropsychologia 2012, 50, 2752–2763. [Google Scholar] [CrossRef] [PubMed]
- Sheppard, S.M.; Meier, E.L.; Zezinka Durfee, A.; Walker, A.; Shea, J.; Hillis, A.E. Characterizing subtypes and neural correlates of receptive aprosodia in acute right hemisphere stroke. Cortex 2021, in press. [Google Scholar] [CrossRef]
- Davis, C.; Oishi, K.; Faria, A.; Hsu, J.; Gomez, Y.; Mori, S.; Hillis, A.E. White matter tracts critical for recognition of sarcasm. Neurocase 2016, 22, 22–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grandjean, D. Brain networks of emotional prosody processing. Emot. Rev. 2021, 13, 34–43. [Google Scholar] [CrossRef] [Green Version]
- Dell, G.S.; Schwartz, M.F.; Martin, N.; Saffran, E.M.; Gagnon, D.A. Lexical access in aphasic and nonaphasic speakers. Psychol. Rev. 1997, 104, 801–838. [Google Scholar] [CrossRef]
- Indefrey, P.; Levelt, W.J.M. The spatial and temporal signatures of word production components. Cognition 2004, 92, 101–144. [Google Scholar] [CrossRef] [Green Version]
- Hillis, A.E.; Tuffiash, E.; Wityk, R.J.; Barker, P.B. Regions of neural dysfunction associated with impaired naming of actions and objects in acute stroke. Cogn. Neuropsychol. 2002, 19, 523–534. [Google Scholar] [CrossRef]
- Hillis, A.E.; Kleinman, J.T.; Newhart, M.; Heidler-Gary, J.; Gottesman, R.; Barker, P.B.; Aldrich, E.; Llinas, R.; Wityk, R.; Chaudhry, P. Restoring cerebral blood flow reveals neural regions critical for naming. J. Neurosci. 2006, 26, 8069–8073. [Google Scholar] [CrossRef] [PubMed]
- Hillis, A.E.; Wityk, R.J.; Tuffiash, E.; Beauchamp, N.J.; Jacobs, M.A.; Barker, P.B.; Selnes, O.A. Hypoperfusion of Wernicke’s area predicts severity of semantic deficit in acute stroke. Ann. Neurol. 2001, 50, 561–566. [Google Scholar] [CrossRef]
- Hillis, A.E.; Wityk, R.J.; Barker, P.B.; Beauchamp, N.J.; Gailloud, P.; Murphy, K.; Cooper, O.; Metter, E.J. Subcortical aphasia and neglect in acute stroke: The role of cortical hypoperfusion. Brain 2002, 125, 1094–1104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenbek, J.C.; Crucian, G.P.; Leon, S.A.; Hieber, B.; Rodriguez, A.D.; Holiway, B.; Ketterson, T.U.; Ciampitti, M.; Heilman, K.; Gonzalez-Rothi, L. Novel treatments for expressive aprosodia: A Phase I investigation of cognitive linguistic and imitative interventions. J. Int. Neuropsychol. Soc. 2004, 10, 786–793. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenbek, J.C.; Rodriguez, A.D.; Hieber, B.; Leon, S.A.; Crucian, G.P.; Ketterson, T.U.; Ciampitti, M.; Singletary, F.; Heilman, K.M.; Gonzalez Rothi, L.J. Effects of two treatments for aprosodia secondary to acquired brain injury. JRRD 2006, 43, 379. [Google Scholar] [CrossRef] [PubMed]
- Leon, S.A.; Rosenbek, J.C.; Crucian, G.P.; Hieber, B.; Holiway, B.; Rodriguez, A.D.; Ketterson, T.U.; Ciampitti, M.Z.; Freshwater, S.; Heilman, K.; et al. Active treatments for aprosodia secondary to right hemisphere stroke. JRRD 2004, 41, 93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDonald, S.; Togher, L.; Tate, R.; Randall, R.; English, T.; Gowland, A. A randomised controlled trial evaluating a brief intervention for deficits in recognising emotional prosody following severe ABI. Neuropsychol. Rehabil. 2013, 23, 267–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roelofs, R.L.; Wingbermühle, E.; Egger, J.I.M.; Kessels, R.P.C. Social cognitive interventions in neuropsychiatric patients: A meta-analysis. Brain Impair. 2017, 18, 138–173. [Google Scholar] [CrossRef] [Green Version]
- Lado-Codesido, M.; Méndez Pérez, C.; Mateos, R.; Olivares, J.M.; García Caballero, A. Improving emotion recognition in Schizophrenia with “VOICES”: An on-line prosodic self-training. PLoS ONE 2019, 14, e0210816. [Google Scholar] [CrossRef]
- Bornhofen, C.; McDonald, S. Comparing Strategies for treating emotion perception deficits in traumatic brain injury. J. Head Trauma Rehabil. 2008, 23, 103–115. [Google Scholar] [CrossRef]
- Bornhofen, C.; McDonald, S. Treating deficits in emotion perception following traumatic brain injury. Neuropsychol. Rehabil. 2008, 18, 22–44. [Google Scholar] [CrossRef]
- McDonald, S.; Tate, R.; Togher, L.; Bornhofen, C.; Long, E.; Gertler, P.; Bowen, R. Social skills treatment for people with severe, chronic acquired brain injuries: A multicenter trial. Arch. Phys. Med. Rehabil. 2008, 89, 1648–1659. [Google Scholar] [CrossRef]
- Vallat-Azouvi, C.; Azouvi, P.; Le-Bornec, G.; Brunet-Gouet, E. Treatment of social cognition impairments in patients with traumatic brain injury: A critical review. Brain Inj. 2019, 33, 87–93. [Google Scholar] [CrossRef]
- Kandalaft, M.R.; Didehbani, N.; Krawczyk, D.C.; Allen, T.T.; Chapman, S.B. Virtual reality social cognition training for young adults with high-functioning Autism. J. Autism Dev. Disord. 2013, 43, 34–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nahum, M.; Fisher, M.; Loewy, R.; Poelke, G.; Ventura, J.; Nuechterlein, K.H.; Hooker, C.I.; Green, M.F.; Merzenich, M.; Vinogradov, S. A novel, online social cognitive training program for young adults with Schizophrenia: A pilot study. Schizophr. Res. Cogn. 2014, 1, e11–e19. [Google Scholar] [CrossRef] [Green Version]
- Dara, C.; Bang, J.; Gottesman, R.F.; Hillis, A.E. Right hemisphere dysfunction is better predicted by emotional prosody impairments as compared to neglect. J. Neurol. Transl. Neurosci. 2014, 2, 1037. [Google Scholar]
- Blake, M.L.; Duffy, J.; Tompkins, C.; Myers, P. Right hemisphere syndrome is in the eye of the beholder. Aphasiology 2003, 17, 423–432. [Google Scholar] [CrossRef]
- Ramsey, A.; Blake, M.L. Speech-language pathology practices for adults with right hemisphere stroke: What are we missing? Am. J. Speech Lang. Pathol. 2020, 29, 741–759. [Google Scholar] [CrossRef] [PubMed]
- Pell, M.D. Evaluation of nonverbal emotion in face and voice: Some preliminary findings on a new battery of tests. Brain Cogn. 2002, 48, 499–504. [Google Scholar]
- Pell, M.D.; Paulmann, S.; Dara, C.; Alasseri, A.; Kotz, S.A. Factors in the recognition of vocally expressed emotions: A comparison of four languages. J. Phon. 2009, 37, 417–435. [Google Scholar] [CrossRef]
- Banse, R.; Scherer, K.R. Acoustic profiles in vocal emotion expression. J. Pers. Soc. Psychol. 1996, 70, 614–636. [Google Scholar] [CrossRef]
- Cirstea, M.C.; Levin, M.F. Improvement of arm movement patterns and endpoint control depends on type of feedback during practice in stroke survivors. Neurorehabil. Neural Repair 2007, 21, 398–411. [Google Scholar] [CrossRef]
- Bakker, M.; Beijer, L.; Rietveld, T. Considerations on effective feedback in computerized speech training for dysarthric speakers. Telemed. J. E-Health 2019, 25, 351–358. [Google Scholar] [CrossRef] [PubMed]
- Reyes, D.; Hitomi, E.; Simpkins, A.; Lynch, J.; Hsia, A.; Benson, R.; Nadareishvili, Z.; Luby, M.; Latour, L.; Leigh, R. Abstract TP63: Detection of perfusion deficits using FLAIR and GRE based vessel signs. Stroke 2017, 48, ATP63. [Google Scholar] [CrossRef]
- Rorden, C.; Karnath, H.-O.; Bonilha, L. Improving lesion-symptom mapping. J. Cogn. Neurosci. 2007, 19, 1081–1088. [Google Scholar] [CrossRef] [PubMed]
- MRIcron. Available online: https://www.nitrc.org/projects/mricron (accessed on 24 March 2021).
- SPM12. Available online: https://www.fil.ion.ucl.ac.uk/spm/software/spm12/ (accessed on 24 March 2021).
- Rorden, C.; Bonilha, L.; Fridriksson, J.; Bender, B.; Karnath, H.-O. Age-specific CT and MRI templates for spatial normalization. Neuroimage 2012, 61, 957–965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tzourio-Mazoyer, N.; Landeau, B.; Papathanassiou, D.; Crivello, F.; Etard, O.; Delcroix, N.; Mazoyer, B.; Joliot, M. Automated anatomical labeling of activations in SPM using a macroscopic anatomical parcellation of the MNI MRI single-subject brain. Neuroimage 2002, 15, 273–289. [Google Scholar] [CrossRef] [PubMed]
- Catani, M.; Thiebaut de Schotten, M. A diffusion tensor imaging tractography atlas for virtual in vivo dissections. Cortex 2008, 44, 1105–1132. [Google Scholar] [CrossRef]
- Bates, D.; Mächler, M.; Bolker, B.; Walker, S. Fitting linear mixed-effects models using Lme4. J. Stat. Softw. 2015, 67, 1–48. [Google Scholar] [CrossRef]
- Kuznetsova, A.; Brockhoff, P.B.; Christensen, R.H.B. LmerTest package: Tests in linear mixed effects models. J. Stat. Softw. 2017, 82, 1–26. [Google Scholar] [CrossRef] [Green Version]
- Tibshirani, R. Regression shrinkage and selection via the Lasso. J. R. Stat. Soc. Ser. B (Methodol.) 1996, 58, 267–288. [Google Scholar] [CrossRef]
- Cancelliere, A.E.; Kertesz, A. Lesion localization in acquired deficits of emotional expression and comprehension. Brain Cogn. 1990, 13, 133–147. [Google Scholar] [CrossRef]
- Burnham, K.P.; Anderson, D.R. Multimodel inference: Understanding AIC and BIC in model selection. Sociol. Methods Res. 2004, 33, 261–304. [Google Scholar] [CrossRef]
- Tompkins, C.A. Rehabilitation for cognitive-communication disorders in right hemisphere brain damage. Arch. Phys. Med. Rehabil. 2012, 93, S61–S69. [Google Scholar] [CrossRef] [PubMed]
- Brownell, H.; Lundgren, K.; Cayer-Meade, C.; Milione, J.; Katz, D.I.; Kearns, K. Treatment of metaphor interpretation deficits subsequent to traumatic brain injury. J. Head Trauma Rehabil. 2013, 28, 446–452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lundgren, K.; Brownell, H.; Cayer-Meade, C.; Milione, J.; Kearns, K. Treating metaphor interpretation deficits subsequent to right hemisphere brain damage: Preliminary results. Aphasiology 2011, 25, 456–474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blake, M.L. Inferencing processes after right hemisphere brain damage: Effects of contextual bias. J. Speech Lang. Hear. Res. 2009, 52, 373–384. [Google Scholar] [CrossRef]
- Blake, M.L.; Tompkins, C.A.; Scharp, V.L.; Meigh, K.M.; Wambaugh, J. Contextual Constraint Treatment for coarse coding deficit in adults with right hemisphere brain damage: Generalization to narrative discourse comprehension. Neuropsychol. Rehabil. 2015, 25, 15–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tompkins, C.A. Redundancy enhances emotional inferencing by right- and left-hemisphere-damaged adults. J. Speech Hear. Res. 1991, 34, 1142–1149. [Google Scholar] [CrossRef]
- Tompkins, C.A.; Flowers, C.R. Contextual mood priming following left and right hemisphere damage. Brain Cogn. 1987, 6, 361–376. [Google Scholar] [CrossRef]
- Zezinka, A.; Tompkins, C.A. Negative word production in adults with right hemisphere grain damage: Effects of implicit assessment and contextual bias. Am. J. Speech Lang. Pathol. 2015, 24, S815–S827. [Google Scholar] [CrossRef]
- Heider, F.; Simmel, M. An experimental study of apparent behavior. Am. J. Psychol. 1944, 57, 243–259. [Google Scholar] [CrossRef]
- Belyk, M.; Brown, S. Perception of affective and linguistic prosody: An ALE meta-analysis of neuroimaging studies. Soc. Cogn. Affect. Neurosci. 2014, 9, 1395–1403. [Google Scholar] [CrossRef] [Green Version]
- Lima, C.F.; Krishnan, S.; Scott, S.K. Roles of supplementary motor areas in auditory processing and auditory imagery. Trends Neurosci. 2016, 39, 527–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kotz, S.A.; Paulmann, S. Emotion, language, and the brain. Lang. Linguist. Compass 2011, 5, 108–125. [Google Scholar] [CrossRef]
- Paulmann, S.; Ott, D.V.M.; Kotz, S.A. Emotional speech perception unfolding in time: The role of the basal ganglia. PLoS ONE 2011, 6, e17694. [Google Scholar] [CrossRef] [Green Version]
- Lim, S.-J.; Fiez, J.A.; Holt, L.L. How may the basal ganglia contribute to auditory categorization and speech perception? Front. Neurosci. 2014, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shohamy, D.; Myers, C.E.; Kalanithi, J.; Gluck, M.A. Basal banglia and dopamine contributions to probabilistic category learning. Neurosci. Biobehav. Rev. 2008, 32, 219–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant | Sex | Race | Age | Education (years) | Handedness, Pre-Stroke | Admitting NIHSSs | Affective Prosody Recognition, Pre-Training | Affective Prosody Recognition, Post-Training | Emotion Synonym Matching | Emotional Facial Expression Recognition |
|---|---|---|---|---|---|---|---|---|---|---|
| STAGE 1 DEFICIST (ACOUSTIC-PROSODIC) | ||||||||||
| 101 | female | white | 64 | 12 | right | 1 | 10 | 58.33 | 87.50 | 67.50 |
| 102 | female | black | 85 | 20 | right | 1 | 18.75 | 37.50 | 87.50 | 67.50 |
| 105 | female | white | 75 | na | na | 15 | 35 | 50 | 70.83 | na |
| 107 | male | black | 56 | 12 | right | 4 | 25 | 25 | 79.17 | 60 |
| 108 | female | white | 76 | 16 | right | 8 | 25 | 50 | 91.67 | 67.50 |
| 114 | male | white | 73 | 16 | left | 1 | 55 | 41.67 | 79.17 | 57.50 |
| 117 | male | black | 70 | 13 | right | 6 | 30 | 41.67 | 91.67 | 52.50 |
| STAGE 2 DEFICITS (ARACCE ACCESS) | ||||||||||
| 106 | male | black | 64 | 18 | right | 3 | 45 | 41.67 | 91.67 | 85 |
| STAGE 1 and 2 DEFICITS | ||||||||||
| 100 | female | white | 71 | 10 | right | 7 | 20 | 50 | 95.83 | 65 |
| 103 | female | black | 75 | 12 | right | 17 | 20 | 25 | 45.83 | na |
| 104 | male | white | 74 | 10 | right | 0 | 25 | 25 | 95.83 | 82.50 |
| 110 | male | white | 63 | 8 | left | 3 | 12.50 | 37.50 | 87.50 | na |
| 112 | male | white | 57 | na | na | 3 | 35 | 50 | 75 | 82.50 |
| 115 | male | black | 62 | 10 | right | 15 | 25 | 58.33 | 54.17 | 62.50 |
| NO IMPAIRMENT LOCUS | ||||||||||
| 109 | male | white | 60 | 13 | right | 5 | 25 | 25 | 91.67 | 65 |
| 111 | male | black | 87 | 16 | right | 17 | 50 | 66.67 | 95.83 | na |
| 113 | male | white | 72 | 16 | right | 13 | 40 | 58.33 | 95.83 | 90 |
| 116 | male | black | 63 | na | right | 10 | 35 | 50 | 70.83 | 65 |
| Model Specification | Model Name | Nested Model | Fixed Effects Added | Random Effects | Model Fit | LRT against Nested | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Subjects | AIC | BIC | LL | df.resid | df | X2 | ||||
| Random effect + all covariates | Covariate 1 | - | age + education + admitNIHSS | intercepts | 298.6 | 308.1 | −143.3 | 30 | - | - |
| † Random effect + covariate subset 1 | Covariate 2 | Covariate 1 | education + admitNIHSS | intercepts | 296.7 | 304.6 | −143.3 | 31 | 1 | 0.129 |
| Random effect + covariate subset 2 | Covariate 3 | Covariate 2 | Education | intercepts | 297.8 | 304.1 | −144.9 | 32 | 1 | 3.076 |
| Fixed effects, 2-way interaction | Main effects + Interaction | Main effects | education + admitNIHSS + impairment locus × time + context | intercepts | 285.2 | 302.6 | −131.6 | 25 | 2 | 0.113 |
| † Fixed effects, main effects only | Main effects only | Covariate 2 | education + admitNIHSS + impairment locus + time + context | intercepts | 281.3 | 295.6 | −131.7 | 27 | 4 | 23.343 * |
| Fixed effects | |||||
| Estimates (Β) | SE | 95% CI | t | p | |
| Intercept | 22.911 | 11.215 | −17.883, 34.769 | 2.043 | 0.048 |
| Impairment locus: Acoustic-prosodic | −5.191 | 4.546 | −15.118, 4.736 | −1.142 | 0.261 |
| Impairment locus: ARACCE ± acoustic-prosodic | −6.168 | 4.836 | −16.727, 4.392 | −1.275 | 0.210 |
| Testing (post-training) | 14.468 | 3.126 | 7.640, 21.294 | 4.628 | <0.001 |
| Context (real-word sentences) | −12.384 | 3.821 | −20.729, −4.039 | −3.241 | 0.003 |
| Education | 1.084 | 0.610 | −0.247, 2.415 | 1.778 | 0.084 |
| admitNIHSS | 0.063 | 0.335 | −0.668, 0.795 | 0.189 | 0.851 |
| Random effects | |||||
| Variance | SD | ||||
| Participant (intercept) | 0 | 0 | |||
| Model fit | |||||
| Marginal | Conditional | ||||
| R2 | na | 0.521 | |||
| Variable | Adjusted Coefficient | Coefficient | z-Score | p-Value | 95% CI |
|---|---|---|---|---|---|
| Intercept | 7.066 × 10−17 | - | - | - | - |
| Age | −4.933 × 10−2 | −0.305 | −0.903 | 0.814 | −0.832, 8.222 |
| Education | −1.247 × 10−1 | −0.510 | −1.253 | 0.668 | −1.216, 5.600 |
| Hypoperfusion: ACA | −1.664 × 10−1 | −0.215 | −0.757 | 0.369 | −2.319, 1.605 |
| Hypoperfusion: MCA-parietal | −3.695 × 10−1 | −0.664 | −1.979 | 0.251 | −1.298, 1.243 |
| Angular gyrus | −3.073 × 10−1 | −0.412 | −1.299 | 0.262 | −1.033, 0.871 |
| Thalamus | −3.597 × 10−1 | −0.538 | −1.908 | 0.291 | −1.068, 1.217 |
| ILF | −5.827 × 10−1 | −0.847 | −2.306 | 0.379 | −1.563, 2.642 |
| IFOF | −5.120 × 10−1 | −0.852 | −2.403 | 0.210 | −1.515, 1.255 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Durfee, A.Z.; Sheppard, S.M.; Meier, E.L.; Bunker, L.; Cui, E.; Crainiceanu, C.; Hillis, A.E. Explicit Training to Improve Affective Prosody Recognition in Adults with Acute Right Hemisphere Stroke. Brain Sci. 2021, 11, 667. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11050667
Durfee AZ, Sheppard SM, Meier EL, Bunker L, Cui E, Crainiceanu C, Hillis AE. Explicit Training to Improve Affective Prosody Recognition in Adults with Acute Right Hemisphere Stroke. Brain Sciences. 2021; 11(5):667. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11050667
Chicago/Turabian StyleDurfee, Alexandra Zezinka, Shannon M. Sheppard, Erin L. Meier, Lisa Bunker, Erjia Cui, Ciprian Crainiceanu, and Argye E. Hillis. 2021. "Explicit Training to Improve Affective Prosody Recognition in Adults with Acute Right Hemisphere Stroke" Brain Sciences 11, no. 5: 667. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11050667