
Stiff-Eye Syndrome—Anti-GAD Ataxia Presenting with Isolated Ophthalmoplegia: A Case Report

 ,
, {kind=link}
Abstract
:1. Introduction
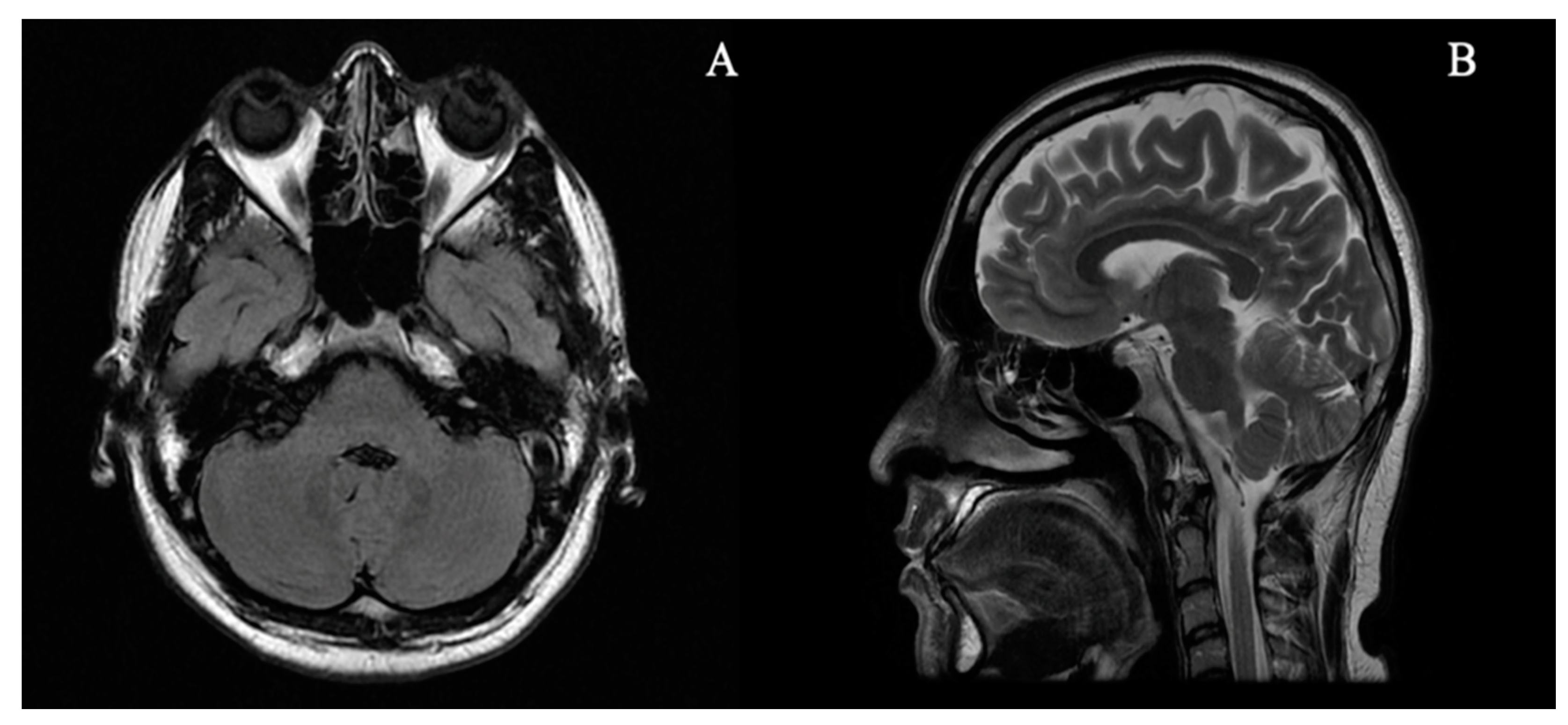
2. Case Report
3. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Mitoma, H.; Manto, M.; Hadjivassiliou, M. Immune-Mediated Cerebellar Ataxias: Clinical Diagnosis and Treatment Based on Immunological and Physiological Mechanisms. J. Mov. Disord. 2021, 14, 10–28. [Google Scholar] [CrossRef] [PubMed]
- Joubert, B.; Rostásy, K.; Honnorat, J. Immune-mediated ataxias. Handb. Clin. Neurol. 2018, 155, 313–332. [Google Scholar] [CrossRef]
- Baizabal-Carvallo, J.F.; Jankovic, J. Stiff-person syndrome: Insights into a complex autoimmune disorder. J. Neurol. Neurosurg. Psychiatry 2015, 86, 840–848. [Google Scholar] [CrossRef] [PubMed]
- Tilikete, C.; Vighetto, A.; Trouillas, P.; Honnorat, J. Potential role of anti-GAD antibodies in abnormal eye movements. Ann. N. Y. Acad. Sci. 2005, 1039, 446–454. [Google Scholar] [CrossRef] [PubMed]
- Economides, J.R.; Horton, J.C. Eye movement abnormalities in stiff person syndrome. Neurology 2005, 65, 1462–1464. [Google Scholar] [CrossRef] [PubMed]
- Markakis, I.; Alexiou, E.; Xifaras, M.; Gekas, G.; Rombos, A. Opsoclonus-myoclonus-ataxia syndrome with autoantibodies to glutamic acid decarboxylase. Clin. Neurol. Neurosurg. 2008, 110, 619–621. [Google Scholar] [CrossRef] [PubMed]
- Dubbioso, R.; Marcelli, V.; Manganelli, F.; Iodice, R.; Esposito, M.; Santoro, L. Anti-GAD antibody ocular flutter: Expanding the spectrum of autoimmune ocular motor disorders. J. Neurol. 2013, 260, 2675–2677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chakravarthi, S.; Goyal, M.K.; Lal, V. Pearls & Oy-sters: Tonic eye deviation in stiff-person syndrome. Neurology 2015, 84, e124–e127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strupp, M.; Kremmyda, O.; Adamczyk, C.; Böttcher, N.; Muth, C.; Yip, C.W.; Bremova, T. Central ocular motor disorders, including gaze palsy and nystagmus. J. Neurol. 2014, 261 (Suppl. 2), S542–S558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feldman, D.; Otero-Millan, J.; Shaikh, A.G. Gravity-Independent Upbeat Nystagmus in Syndrome of Anti-GAD Antibodies. Cerebellum 2019, 18, 287–290. [Google Scholar] [CrossRef] [PubMed]
- Ishida, K . Selective suppression of cerebellar GABAergic transmission by an autoantibody to glutamic acid decarboxylase. Ann. Neurol. 1999, 46, 263–267. [CrossRef]
- Manto, M.-U.; Laute, M.-A.; Aguera, M.; Rogemond, V.; Pandolfo, M.; Honnorat, J. Effects of anti-glutamic acid decarboxylase antibodies associated with neurological diseases: GAD-Ab and Cerebellar Function. Ann. Neurol. 2007, 61, 544–551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Das, V.E.; Leigh, R.J.; Swann, M.; Thurtell, M.J. Muscimol inactivation caudal to the interstitial nucleus of Cajal induces hemi-seesaw nystagmus. Exp. Brain Res. 2010, 205, 405–413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kodama, S.; Tokushige, S.I.; Sugiyama, Y.; Sato, K.; Otsuka, J.; Shirota, Y.; Hamada, M.; Iwata, A.; Toda, T.; Tsuji, S.; et al. Rituximab improves not only back stiffness but also “stiff eyes” in stiff person syndrome: Implications for immune-mediated treatment. J. Neurol. Sci. 2020, 408, 116506. [Google Scholar] [CrossRef] [PubMed]
- Nakajima, H.; Nakamura, Y.; Inaba, Y.; Tsutsumi, C.; Unoda, K.; Hosokawa, T.; Kimura, F.; Hanafusa, T.; Date, M.; Kitaoka, H. Neurologic disorders associated with anti-glutamic acid decarboxylase antibodies: A comparison of anti-GAD antibody titers and time-dependent changes between neurologic disease and type I diabetes mellitus. J. Neuroimmunol. 2018, 317, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Namchuk, M.; Bugawan, T.; Fu, Q.; Jaffe, M.; Shi, Y.; Aanstoot, H.J.; Turck, C.W.; Erlich, H.; Lennon, V.; et al. Higher autoantibody levels and recognition of a linear NH2-terminal epitope in the autoantigen GAD65, distinguish stiff-man syndrome from insulin-dependent diabetes mellitus. J. Exp. Med. 1994, 180, 595–606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manto, M.; Honnorat, J.; Hampe, C.S.; Guerra-Narbona, R.; López-Ramos, J.C.; Delgado-García, J.M.; Saitow, F.; Suzuki, H.; Yanagawa, Y.; Mizusawa, H.; et al. Disease-specific monoclonal antibodies targeting glutamate decarboxylase impair GABAergic neurotransmission and affect motor learning and behavioral functions. Front. Behav. Neurosci. 2015, 9, 78. [Google Scholar] [CrossRef] [PubMed] [Green Version]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Belém, A.D.; Vasconcelos, T.d.M.F.; Paula, R.C.d.A.d.; Costa, F.B.S.d.; Rodrigues, P.G.B.; Pereira, I.d.S.; Tavares, P.R.d.A.; Galdino, G.S.; Dias, D.A.; Santos, C.d.F.; et al. Stiff-Eye Syndrome—Anti-GAD Ataxia Presenting with Isolated Ophthalmoplegia: A Case Report. Brain Sci. 2021, 11, 932. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11070932
Belém AD, Vasconcelos TdMF, Paula RCdAd, Costa FBSd, Rodrigues PGB, Pereira IdS, Tavares PRdA, Galdino GS, Dias DA, Santos CdF, et al. Stiff-Eye Syndrome—Anti-GAD Ataxia Presenting with Isolated Ophthalmoplegia: A Case Report. Brain Sciences. 2021; 11(7):932. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11070932
Chicago/Turabian StyleBelém, Abel Dantas, Thaís de Maria Frota Vasconcelos, Rafael César dos Anjos de Paula, Francisco Bruno Santana da Costa, Pedro Gustavo Barros Rodrigues, Isabelle de Sousa Pereira, Paulo Roberto de Arruda Tavares, Gabriela Studart Galdino, Daniel Aguiar Dias, Carolina de Figueiredo Santos, and et al. 2021. "Stiff-Eye Syndrome—Anti-GAD Ataxia Presenting with Isolated Ophthalmoplegia: A Case Report" Brain Sciences 11, no. 7: 932. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11070932