
Obstructive Apnea and Hypopnea Length in Normal Children and Adolescents

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
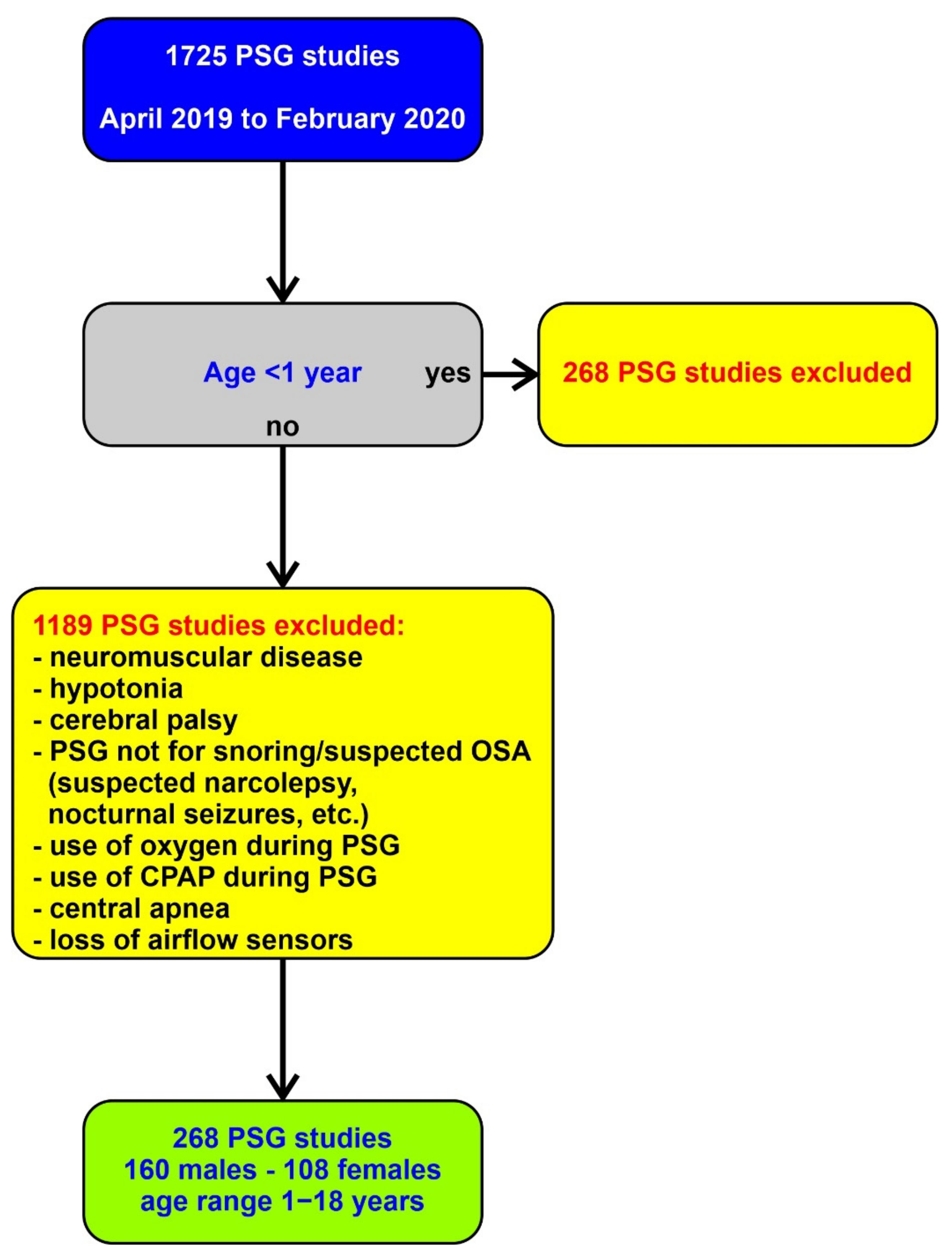
2.1. Subjects
2.2. Polysomnography
2.3. Data, Analysis and Statistics Applied
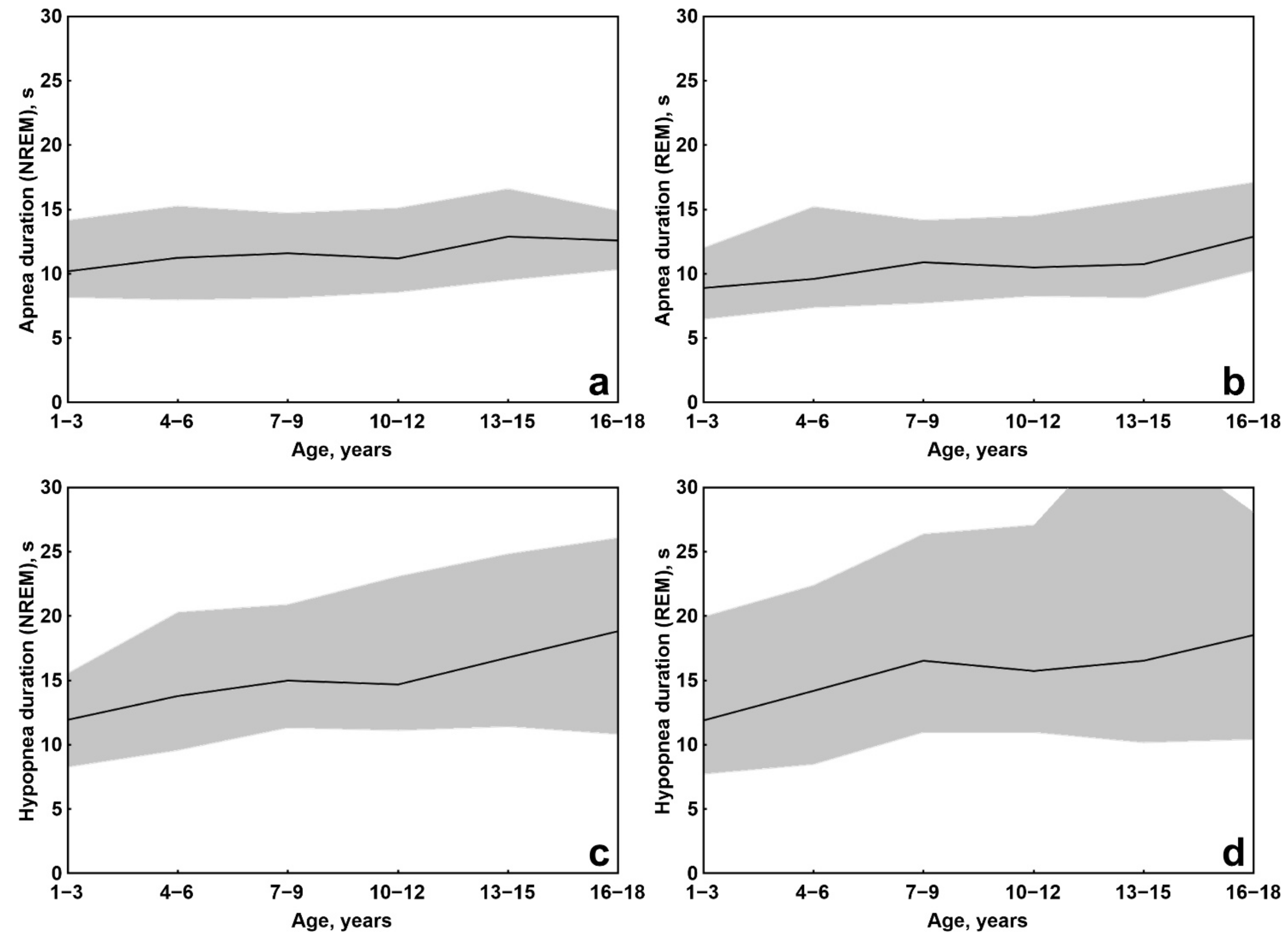
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Waters, T.; Mehra, R. Clinical neurophysiology of apnea. Handb. Clin. Neurol. 2019, 161, 345–352. [Google Scholar] [CrossRef] [PubMed]
- Eckert, D.J.; McEvoy, R.D.; George, K.E.; Thomson, K.J.; Catcheside, P.G. Genioglossus reflex inhibition to upper-airway negative-pressure stimuli during wakefulness and sleep in healthy males. J. Physiol. 2007, 581, 1193–1205. [Google Scholar] [CrossRef] [PubMed]
- Dempsey, J.A.; Smith, C.A. Pathophysiology of human ventilatory control. Eur. Respir. J. 2014, 44, 495–512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simms, T.; Brijbassi, M.; Montemurro, L.T.; Bradley, T.D. Differential timing of arousals in obstructive and central sleep apnea in patients with heart failure. J. Clin. Sleep Med. 2013, 9, 773–779. [Google Scholar] [CrossRef] [PubMed]
- Marcus, C.L.; Brooks, L.J.; Draper, K.A.; Gozal, D.; Halbower, A.C.; Jones, J.; Schechter, M.S.; Ward, S.D.; Sheldon, S.H.; Shiffman, R.N.; et al. Diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics 2012, 130, e714–e755. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maniaci, A.; Iannella, G.; Cocuzza, S.; Vicini, C.; Magliulo, G.; Ferlito, S.; Cammaroto, G.; Meccariello, G.; De Vito, A.; Nicolai, A.; et al. Oxidative stress and inflammation biomarker expression in obstructive sleep apnea patients. J. Clin. Med. 2021, 10, 277. [Google Scholar] [CrossRef] [PubMed]
- Dingli, K.; Fietze, I.; Assimakopoulos, T.; Quispe-Bravo, S.; Witt, C.; Douglas, N.J. Arousability in sleep apnoea/hypopnoea syndrome patients. Eur. Respir. J. 2002, 20, 733–740. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berry, R.B.; Quan, S.F.; Abreu, A.R.; Bibbs, M.L.; DelRosso, L.; Harding, S.M.; Mao, M.-M.; Plante, D.T.; Pressman, M.R.; Troester, M.R.; et al. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications, Ver. 2.6; American Academy of Sleep Medicine: Darien, IL, USA, 2020. [Google Scholar]
- Berry, R.B.; Brooks, R.; Gamaldo, C.; Harding, S.M.; Lloyd, R.M.; Quan, S.F.; Troester, M.T.; Vaughn, B.V. AASM Scoring Manual Version 2.6. In AASM Manual for the Scoring of Sleep and Associated Events; AASM: Darien, IL, USA, 2019. [Google Scholar]
- Marcus, C.L.; Moore, R.H.; Rosen, C.L.; Giordani, B.; Garetz, S.L.; Taylor, H.G.; Mitchell, R.B.; Amin, R.; Katz, E.S.; Arens, R.; et al. A randomized trial of adenotonsillectomy for childhood sleep apnea. N. Engl. J. Med. 2013, 368, 2366–2376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Erlbaum Associates: Hillsdale, NJ, USA, 1988; p. 567. [Google Scholar]
- Brockmann, P.E.; Poets, A.; Poets, C.F. Reference values for respiratory events in overnight polygraphy from infants aged 1 and 3months. Sleep Med. 2013, 14, 1323–1327. [Google Scholar] [CrossRef]
- Ware, J.C.; McBrayer, R.H.; Scott, J.A. Influence of sex and age on duration and frequency of sleep apnea events. Sleep 2000, 23, 165–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oliven, A.; Carmi, N.; Coleman, R.; Odeh, M.; Silbermann, M. Age-related changes in upper airway muscles morphological and oxidative properties. Exp. Gerontol. 2001, 36, 1673–1686. [Google Scholar] [CrossRef]
- Crisalli, J.A.; McConnell, K.; Vandyke, R.D.; Fenchel, M.C.; Somers, V.K.; Shamszumann, A.; Chini, B.; Daniels, S.R.; Amin, R.S. Baroreflex sensitivity after adenotonsillectomy in children with obstructive sleep apnea during wakefulness and sleep. Sleep 2012, 35, 1335–1343. [Google Scholar] [CrossRef] [PubMed]
- Ohayon, M.M.; Carskadon, M.A.; Guilleminault, C.; Vitiello, M.V. Meta-analysis of quantitative sleep parameters from childhood to old age in healthy individuals: Developing normative sleep values across the human lifespan. Sleep 2004, 27, 1255–1273. [Google Scholar] [CrossRef] [PubMed]
- Efken, C.; Bitter, T.; Prib, N.; Horstkotte, D.; Oldenburg, O. Obstructive sleep apnoea: Longer respiratory event lengths in patients with heart failure. Eur. Respir. J. 2013, 41, 1340–1346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, H.; Zhan, X.; Zhao, M.; Wei, Y. Mean apnea-hypopnea duration (but not apnea-hypopnea index) is associated with worse hypertension in patients with obstructive sleep apnea. Medicine 2016, 95, e5493. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Age | oAHI | Sex | ||
|---|---|---|---|---|
| Apnea, NREM | Correlation | 0.287 | −0.015 | 0.067 |
| F | 13.410 | 0.036 | 0.664 | |
| p< | 0.00035 | NS | NS | |
| Apnea, REM | Correlation | 0.304 | −0.032 | −0.035 |
| F | 15.168 | 0.155 | 0.187 | |
| p< | 0.00015 | NS | NS | |
| Hypopnea, NREM | Correlation | 0.442 | 0.007 | 0.003 |
| F | 36.165 | 0.007 | 0.001 | |
| p< | 0.000001 | NS | NS | |
| Hypopnea, REM | Correlation | 0.390 | −0.035 | −0.119 |
| F | 26.710 | 0.188 | 2.122 | |
| p< | 0.000001 | NS | NS | |
| oAHI = obstructive apnea/hypopnea index; NS = not significant. | ||||
| Apnea, NREM | Apnea, REM | Hypopnea, NREM | Hypopnea, REM | |||||
|---|---|---|---|---|---|---|---|---|
| Age, Years | N | Mean ± SD | N | Mean ± SD | N | Mean ± SD | N | Mean ± SD |
| 1 | 5 | 9.4 ± 1.9 | 6 | 7.1 ± 0.7 | 6 | 10.7 ± 2.8 | 6 | 9.2 ± 1.8 |
| 2 | 19 | 9.8 ± 1.8 | 19 | 9.2 ± 1.7 | 18 | 11.3 ± 2.3 | 19 | 12.5 ± 3.8 |
| 3 | 20 | 11.3 ± 1.6 | 19 | 9.3 ± 1.7 | 20 | 12.8 ± 2.7 | 19 | 13.6 ± 3.2 |
| 4 | 17 | 11.4 ± 1.7 | 17 | 10.0 ± 2.8 | 18 | 13.1 ± 3.2 | 18 | 12.7 ± 3.2 |
| 5 | 19 | 11.4 ± 1.4 | 17 | 10.8 ± 2.8 | 18 | 14.1 ± 2.6 | 17 | 15.5 ± 4.5 |
| 6 | 18 | 11.1 ± 3.1 | 13 | 11.1 ± 2.7 | 18 | 15.0 ± 4.3 | 16 | 15.4 ± 6.7 |
| 7 | 18 | 11.3 ± 1.6 | 17 | 10.9 ± 2.4 | 20 | 14.9 ± 3.7 | 17 | 16.4 ± 4.9 |
| 8 | 12 | 10.7 ± 1.2 | 10 | 11.3 ± 1.6 | 12 | 14.5 ± 4.3 | 8 | 16.0 ± 3.7 |
| 9 | 15 | 12.2 ± 2.5 | 14 | 10.7 ± 2.2 | 18 | 16.3 ± 2.9 | 18 | 17.8 ± 5.1 |
| 10 | 7 | 12.5 ± 2.3 | 6 | 12.6 ± 1.6 | 9 | 18.8 ± 4.8 | 8 | 19.0 ± 7.4 |
| 11 | 16 | 11.7 ± 2.8 | 12 | 11.2 ± 2.3 | 19 | 15.4 ± 3.5 | 17 | 17.1 ± 4.8 |
| 12 | 10 | 10.5 ± 1.7 | 9 | 9.1 ± 1.2 | 12 | 13.5 ± 2.6 | 9 | 15.7 ± 3.1 |
| 13 | 11 | 13.0 ± 2.8 | 7 | 10.1 ± 2.1 | 13 | 16.1 ± 3.6 | 11 | 18.0 ± 9.6 |
| 14 | 13 | 12.4 ± 2.2 | 10 | 12.4 ± 2.4 | 16 | 16.2 ± 3.6 | 12 | 16.1 ± 4.4 |
| 15 | 11 | 13.3 ± 2.2 | 7 | 10.5 ± 2.8 | 17 | 19.4 ± 4.8 | 15 | 22.6 ± 11.9 |
| 16 | 9 | 13.2 ± 1.9 | 1 | 18.0 | 9 | 20.2 ± 5.4 | 6 | 21.2 ± 7.5 |
| 17 | 5 | 11.6 ± 0.7 | 4 | 12.8 ± 1.6 | 8 | 16.8 ± 4.0 | 7 | 18.4 ± 3.4 |
| 18 | 1 | 14.1 | 1 | 9.9 | 4 | 18.9 ± 10.5 | 4 | 13.3 ± 4.4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
DelRosso, L.M.; Panek, D.; Redding, G.; Mogavero, M.P.; Ruth, C.; Sheldon, N.; Blazier, H.; Strong, C.; Samson, M.; Fickenscher, A.; et al. Obstructive Apnea and Hypopnea Length in Normal Children and Adolescents. Brain Sci. 2021, 11, 1343. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11101343
DelRosso LM, Panek D, Redding G, Mogavero MP, Ruth C, Sheldon N, Blazier H, Strong C, Samson M, Fickenscher A, et al. Obstructive Apnea and Hypopnea Length in Normal Children and Adolescents. Brain Sciences. 2021; 11(10):1343. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11101343
Chicago/Turabian StyleDelRosso, Lourdes M., David Panek, Greg Redding, Maria Paola Mogavero, Chris Ruth, Nicole Sheldon, Holly Blazier, Candace Strong, Maria Samson, Amy Fickenscher, and et al. 2021. "Obstructive Apnea and Hypopnea Length in Normal Children and Adolescents" Brain Sciences 11, no. 10: 1343. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11101343