
Correlation between Mild Traumatic Brain Injury-Induced Inflammatory Cytokines and Emotional Symptom Traits: A Systematic Review


Abstract
:1. Introduction
2. Methods
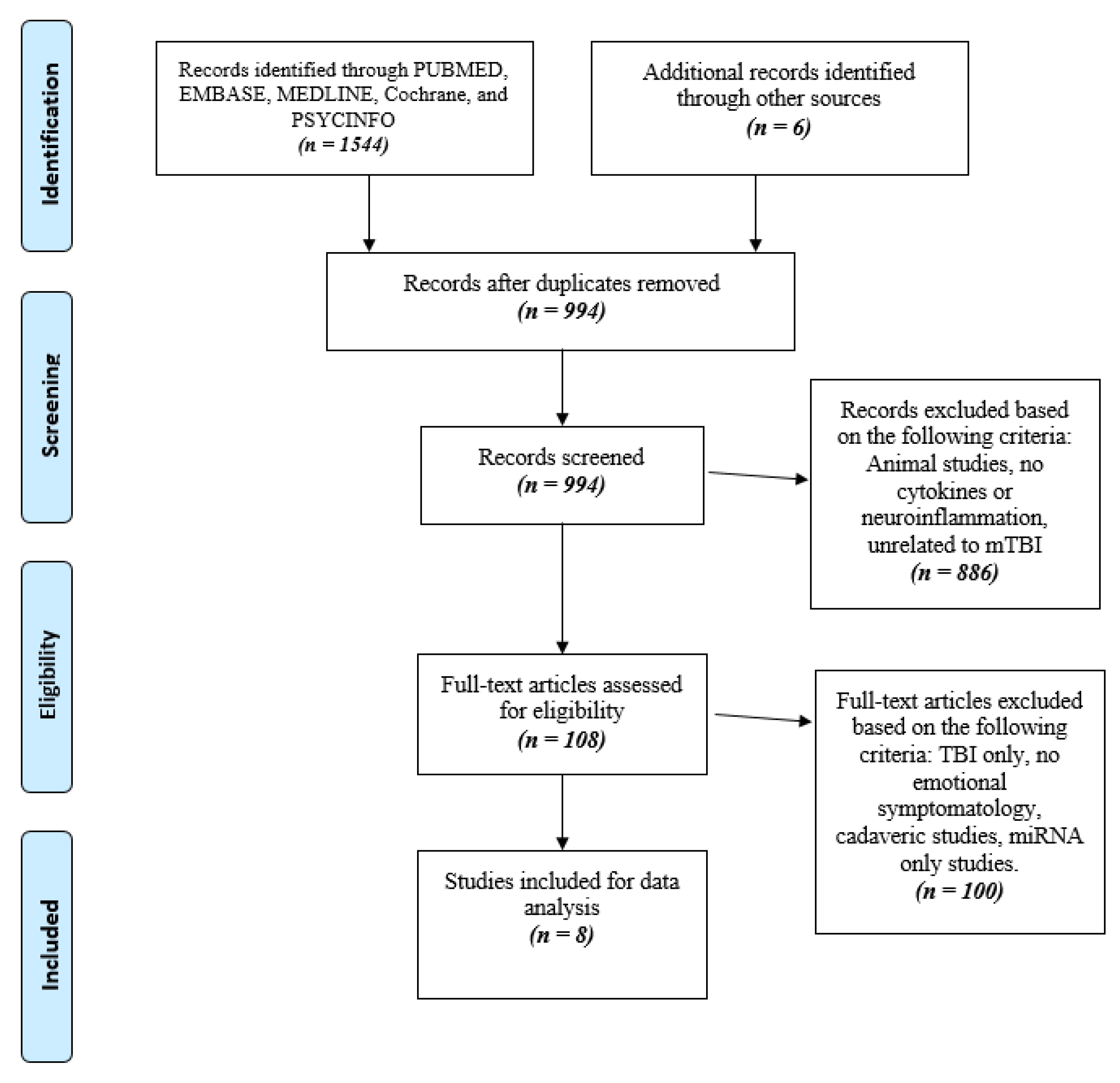
2.1. Search Strategy
2.2. Study Screening
2.3. Data Abstraction
2.4. Quality Assessment
2.5. Statistical Analysis
3. Results
3.1. Study Characteristics
3.2. Study Quality
3.3. Patient Characteristics
3.4. Outcomes
3.4.1. Depression
3.4.2. Post-Traumatic Stress Disorder (PTSD)
3.4.3. Anxiety
3.4.4. Cytokines
IL-6
TNF-α
IL-10
CRP
IL-1β
IL-7
4. Discussion
5. Limitations
6. Conclusions
7. Clinical Significance
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Levin, H.S.; Diaz-Arrastia, R.R. Diagnosis, prognosis, and clinical management of mild traumatic brain injury. Lancet Neurol. 2015, 14, 506–517. [Google Scholar] [CrossRef]
- Cassidy, J.D.; Carroll, L.; Peloso, P.; Borg, J.; von Holst, H.; Holm, L.; Kraus, J.; Coronado, V. Incidence, risk factors and prevention of mild traumatic brain injury: Results of the who collaborating centre task force on mild traumatic brain injury. J. Rehabil. Med. 2004, 36, 28–60. [Google Scholar] [CrossRef] [Green Version]
- McCrory, P.; Meeuwisse, W.; Dvorak, J.; Aubry, M.; Bailes, J.; Broglio, S.; Cantu, R.C.; Cassidy, D.; Echemendia, R.J.; Castellani, R.J.; et al. Consensus statement on concussion in sport—The 5th international conference on concussion in sport held in Berlin, October 2016. Br. J. Sports Med. 2017, 51, 838–847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hiploylee, C.; Dufort, P.A.; Davis, H.S.; Wennberg, R.A.; Tartaglia, M.C.; Mikulis, D.; Hazrati, L.-N.; Tator, C.H. Longitudinal Study of Postconcussion Syndrome: Not Everyone Recovers. J. Neurotrauma 2017, 34, 1511–1523. [Google Scholar] [CrossRef] [Green Version]
- Cnossen, M.C.; Van Der Naalt, J.; Spikman, J.M.; Nieboer, D.; Yue, J.; Winkler, E.A.; Manley, G.T.; Von Steinbuechel, N.; Polinder, S.; Steyerberg, E.W.; et al. Prediction of Persistent Post-Concussion Symptoms after Mild Traumatic Brain Injury. J. Neurotrauma 2018, 35, 2691–2698. [Google Scholar] [CrossRef] [PubMed]
- Langer, L.K.; Alavinia, S.M.; Lawrence, D.W.; Munce, S.E.P.; Kam, A.; Tam, A.; Ruttan, L.; Comper, P.; Bayley, M.T. Prediction of risk of prolonged post-concussion symptoms: Derivation and validation of the TRICORDRR (Toronto Rehabilitation Institute Concussion Outcome Determination and Rehab Recommendations) score. PLoS Med. 2021, 18, e1003652. [Google Scholar] [CrossRef]
- Howell, D.R.; Southard, J. The Molecular Pathophysiology of Concussion. Clin. Sports Med. 2021, 40, 39–51. [Google Scholar] [CrossRef]
- Meares, S.; Shores, E.A.; Taylor, A.J.; Batchelor, J.; Bryant, R.A.; Baguley, I.J.; Chapman, J.; Gurka, J.; Dawson, K.; Capon, L.; et al. Mild traumatic brain injury does not predict acute postconcussion syndrome. J. Neurol. Neurosurg. Psychiatry 2008, 79, 300–306. [Google Scholar] [CrossRef] [Green Version]
- Rathbone, A.; Tharmaradinam, S.; Jiang, S.; Rathbone, M.P.; Kumbhare, D. A review of the neuro- and systemic inflammatory responses in post concussion symptoms: Introduction of the “post-inflammatory brain syndrome” PIBS. Brain Behav. Immun. 2015, 46, 1–16. [Google Scholar] [CrossRef]
- Kumar, A.; Loane, D.J. Neuroinflammation after traumatic brain injury: Opportunities for therapeutic intervention. Brain Behav. Immun. 2012, 26, 1191–1201. [Google Scholar] [CrossRef]
- Patterson, Z.R.; Holahan, M.R. Understanding the neuroinflammatory response following concussion to develop treatment strategies. Front. Cell. Neurosci. 2012, 6, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arıkanoglu, A.; Aydın, M.; Demir, C.F.; Bulut, S.; Ilhan, N. Plasma Cytokine Levels in Migraineurs During and Outside of Attacks. Electron. J. Gen. Med. 2015, 12, 307–312. [Google Scholar] [CrossRef] [Green Version]
- Martelletti, P.; Stirparo, G.; Giacovazzo, M. Proinflammatory cytokines in cervicogenic headache. Funct. Neurol. 1999, 14, 159–162. [Google Scholar]
- McAfoose, J.; Baune, B. Evidence for a cytokine model of cognitive function. Neurosci. Biobehav. Rev. 2009, 33, 355–366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krueger, J.M.; Majde, J.A. Cytokines and Sleep. Int. Arch. Allergy Immunol. 1995, 106, 97–100. [Google Scholar] [CrossRef]
- Vgontzas, A.N.; Papanicolaou, D.A.; Bixler, E.O.; Kales, A.; Tyson, K.; Chrousos, G.P. Elevation of Plasma Cytokines in Disorders of Excessive Daytime Sleepiness: Role of Sleep Disturbance and Obesity. J. Clin. Endocrinol. Metab. 1997, 82, 1313–1316. [Google Scholar] [CrossRef]
- Meier, T.B.; Huber, D.L.; Bohorquez-Montoya, L.; Nitta, M.E.; Savitz, J.; Teague, T.K.; Bazarian, J.J.; Hayes, R.L.; Nelson, L.D.; McCrea, M.A. A Prospective Study of Acute Blood-Based Biomarkers for Sport-Related Concussion. Ann. Neurol. 2020, 87, 907–920. [Google Scholar] [CrossRef]
- Goetzl, E.J.; Elahi, F.M.; Mustapic, M.; Kapogiannis, D.; Pryhoda, M.; Gilmore, A.; Gorgens, K.A.; Davidson, B.; Granholm, A.; Ledreux, A. Altered levels of plasma neuron-derived exosomes and their cargo proteins characterize acute and chronic mild traumatic brain injury. FASEB J. 2019, 33, 5082–5088. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Bai, L.; Niu, X.; Wang, Z.; Yin, B.; Bai, G.; Zhang, D.; Gan, S.; Sun, C.; Wang, S.; et al. Elevated Serum Levels of Inflammation-Related Cytokines in Mild Traumatic Brain Injury Are Associated with Cognitive Performance. Front. Neurol. 2019, 10, 1120. [Google Scholar] [CrossRef] [Green Version]
- Thompson, H.J.; Martha, S.R.; Wang, J.; Becker, K.J. Impact of Age on Plasma Inflammatory Biomarkers in the 6 Months Following Mild Traumatic Brain Injury. J. Head Trauma Rehabil. 2020, 35, 324–331. [Google Scholar] [CrossRef]
- Nitta, M.E.; Savitz, J.; Nelson, L.D.; Teague, T.K.; Hoelzle, J.B.; McCrea, M.A.; Meier, T.B. Acute elevation of serum inflammatory markers predicts symptom recovery after concussion. Neurology 2019, 93, e497–e507. [Google Scholar] [CrossRef]
- Edwards, K.A.; Gill, J.M.; Pattinson, C.L.; Lai, C.; Brière, M.; Rogers, N.J.; Milhorn, D.; Elliot, J.; Carr, W. Interleukin-6 is associated with acute concussion in military combat personnel. BMC Neurol. 2020, 20, 209. [Google Scholar] [CrossRef]
- Brahmajothi, M.V.; Abou-Donia, M.B. Monitoring from Battlefield to Bedside: Serum Repositories Help Identify Biomarkers, Perspectives on Mild Traumatic Brain Injury. Mil. Med. 2020, 185, 197–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feng, G.; Feng, J.; Zhang, S.; Tong, Y.; Zhang, Q.; Yang, X.; Zhang, H. Altered levels of α-melanocyte stimulating hormone in cerebrospinal fluid and plasma of patients with traumatic brain injury. Brain Res. 2018, 1696, 22–30. [Google Scholar] [CrossRef]
- Chaban, V.; Clarke, G.J.; Skandsen, T.; Islam, R.; Einarsen, C.E.; Vik, A.; Damås, J.K.; Mollnes, T.E.; Håberg, A.K.; Pischke, S.E. Systemic Inflammation Persists the First Year after Mild Traumatic Brain Injury: Results from the Prospective Trondheim Mild Traumatic Brain Injury Study. J. Neurotrauma 2020, 37, 2120–2130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gill, J.; Mustapic, M.; Diaz-Arrastia, R.; Lange, R.; Gulyani, S.; Diehl, T.; Motamedi, V.; Osier, N.; Stern, R.A.; Kapogiannis, D. Higher exosomal tau, amyloid-beta 42 and IL-10 are associated with mild TBIs and chronic symptoms in military personnel. Brain Inj. 2018, 32, 1359–1366. [Google Scholar] [CrossRef] [PubMed]
- Bai, L.; Bai, G.; Wang, S.; Yang, X.; Gan, S.; Jia, X.; Yin, B.; Yan, Z. Strategic white matter injury associated with long-term information processing speed deficits in mild traumatic brain injury. Hum. Brain Mapp. 2020, 41, 4431–4441. [Google Scholar] [CrossRef]
- Osimo, E.F.; Pillinger, T.; Rodriguez, I.M.; Khandaker, G.M.; Pariante, C.M.; Howes, O.D. Inflammatory markers in depression: A meta-analysis of mean differences and variability in 5,166 patients and 5,083 controls. Brain Behav. Immun. 2020, 87, 901–909. [Google Scholar] [CrossRef] [PubMed]
- Costello, H.; Gould, R.L.; Abrol, E.; Howard, R. Systematic review and meta-analysis of the association between peripheral inflammatory cytokines and generalised anxiety disorder. BMJ Open 2019, 9, e027925. [Google Scholar] [CrossRef] [Green Version]
- Grubenhoff, J.A.; Currie, D.; Comstock, R.D.; Juarez-Colunga, E.; Bajaj, L.; Kirkwood, M.W. Psychological Factors Associated with Delayed Symptom Resolution in Children with Concussion. J. Pediatr. 2016, 174, 27–32.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kung, J.; Chiappelli, F.; Cajulis, O.O.; Avezova, R.; Kossan, G.; Chew, L.; Maida, C.A. From Systematic Reviews to Clinical Recommendations for Evidence-Based Health Care: Validation of Revised Assessment of Multiple Systematic Reviews (R-AMSTAR) for Grading of Clinical Relevance. Open Dent. J. 2010, 4, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (MINORS ): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef]
- Peskind, E.R.; Petrie, E.C.; Li, G.; Cross, D.; Yarnykh, V.; Richards, T.; Minoshima, S.; Mayer, C.; Pagulayan, K.; Huber, B.R.; et al. P2-078: Neuroimaging and cerebrospinal fluid biomarkers in iraq and afghanistan veterans: Effects of deployment and blast concussion mild traumatic brain injury. Alzheimers Dement. 2015, 11, P513. [Google Scholar] [CrossRef]
- Bellgowan, P.S.F.; Singh, R.; Kuplicki, R.; Taylor, R.; Polanski, A.A.; Allen, D.; Cavanagh, T.W.; Bodurka, L.; Drevets, J.; Teague, W.C.; et al. Global functional connectivity in the visceromotor network is negatively correlated with IL-1 beta serum levels in concussed athletes. J. Neurotrauma 2012, 29, A104–A105. [Google Scholar]
- Su, S.-H.; Xu, W.; Li, M.; Zhang, L.; Wu, Y.-F.; Yu, F.; Hai, J. Elevated C-reactive protein levels may be a predictor of persistent unfavourable symptoms in patients with mild traumatic brain injury: A preliminary study. Brain Behav. Immun. 2014, 38, 111–117. [Google Scholar] [CrossRef]
- Guedes, V.A.; Kenney, K.; Shahim, P.; Qu, B.-X.; Lai, C.; Devoto, C.; Walker, W.C.; Nolen, T.; Diaz-Arrastia, R.; Gill, J.M.; et al. Exosomal neurofilament light. Neurology 2020, 94, e2412–e2423. [Google Scholar] [CrossRef] [PubMed]
- Kanefsky, R.; Motamedi, V.; Mithani, S.; Mysliwiec, V.; Gill, J.M.; Pattinson, C.L. Mild traumatic brain injuries with loss of consciousness are associated with increased inflammation and pain in military personnel. Psychiatry Res. 2019, 279, 34–39. [Google Scholar] [CrossRef]
- Vedantam, A.; Brennan, J.; Levin, H.S.; McCarthy, J.J.; Dash, P.K.; Redell, J.B.; Yamal, J.-M.; Robertson, C.S. Early versus Late Profiles of Inflammatory Cytokines after Mild Traumatic Brain Injury and Their Association with Neuropsychological Outcomes. J. Neurotrauma 2021, 38, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Ghai, V.; Fallen, S.; Baxter, D.; Scherler, M.K.; Kim, T.-K.; Zhou, Y.; Meabon, J.S.; Logsdon, A.F.; Banks, W.A.; Schindler, A.G.; et al. Alterations in Plasma microRNA and Protein Levels in War Veterans with Chronic Mild Traumatic Brain Injury. J. Neurotrauma 2020, 37, 1418–1430. [Google Scholar] [CrossRef]
- Verboon, L.N.; Patel, H.C.; Greenhalgh, A.D. The Immune System’s Role in the Consequences of Mild Traumatic Brain Injury (Concussion). Front. Immunol. 2021, 12, 620698. [Google Scholar] [CrossRef] [PubMed]
- Di Battista, A.P.; Rhind, S.G.; Richards, D.; Hutchison, M.G. An investigation of plasma interleukin-6 in sport-related concussion. PLoS ONE 2020, 15, e0232053. [Google Scholar] [CrossRef] [PubMed]
- Gola, H.; Engler, H.; Sommershof, A.; Adenauer, H.; Kolassa, S.; Schedlowski, M.; Groettrup, M.; Elbert, T.; Kolassa, I.-T. Posttraumatic stress disorder is associated with an enhanced spontaneous production of pro-inflammatory cytokines by peripheral blood mononuclear cells. BMC Psychiatry 2013, 13, 40. [Google Scholar] [CrossRef] [Green Version]
- Frommberger, U.H.; Bauer, J.; Haselbauer, P.; Fräulin, A.; Riemann, D.; Berger, M. Interleukin-6-(IL-6) plasma levels in depression and schizophrenia: Comparison between the acute state and after remission. Eur. Arch. Psychiatry Clin. Neurosci. 1997, 247, 228–233. [Google Scholar] [CrossRef]
- Al-Hakeim, H.K.; Al-Rammahi, D.A.; Al-Dujaili, A.H. IL-6, IL-18, sIL-2R, and TNFα proinflammatory markers in depression and schizophrenia patients who are free of overt inflammation. J. Affect. Disord. 2015, 182, 106–114. [Google Scholar] [CrossRef] [PubMed]
- Penninx, B.W.; Kritchevsky, S.B.; Yaffe, K.; Newman, A.B.; Simonsick, E.M.; Rubin, S.; Ferrucci, L.; Harris, T.; Pahor, M. Inflammatory markers and depressed mood in older persons: Results from the health, aging and body composition study. Biol. Psychiatry 2003, 54, 566–572. [Google Scholar] [CrossRef]
- O’Donovan, A.; Hughes, B.M.; Slavich, G.M.; Lynch, L.; Cronin, M.-T.; O’Farrelly, C.; Malone, K.M. Clinical anxiety, cortisol and interleukin-6: Evidence for specificity in emotion–biology relationships. Brain Behav. Immun. 2010, 24, 1074–1077. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parkin, G.M.; Clarke, C.; Takagi, M.; Hearps, S.J.; Babl, F.E.; Davis, G.A.; Anderson, V.; Ignjatovic, V. Plasma Tumor Necrosis Factor Alpha Is a Predictor of Persisting Symptoms Post-Concussion in Children. J. Neurotrauma 2019, 36, 1768–1775. [Google Scholar] [CrossRef]
- Schmidt, F.M.; Lichtblau, N.; Minkwitz, J.; Chittka, T.; Thormann, J.; Kirkby, K.C.; Sander, C.; Mergl, R.; Faßhauer, M.; Stumvoll, M.; et al. Cytokine levels in depressed and non-depressed subjects, and masking effects of obesity. J. Psychiatr. Res. 2014, 55, 29–34. [Google Scholar] [CrossRef]
- Hussein, S.; Dalton, B.; Willmund, G.D.; Ibrahim, M.A.A.; Himmerich, H. A systematic review of tumor necrosis factor-α in post-traumatic stress disorder: Evidence from human and animal studies. Psychiatr. Danub. 2017, 29, 407–420. [Google Scholar] [CrossRef]
- Yang, J.-J.; Jiang, W. Immune biomarkers alterations in post-traumatic stress disorder: A systematic review and meta-analysis. J. Affect. Disord. 2020, 268, 39–46. [Google Scholar] [CrossRef]
- Guo, M.; Liu, T.; Guo, J.-C.; Jiang, X.-L.; Chen, F.; Gao, Y.-S. Study on serum cytokine levels in posttraumatic stress disorder patients. Asian Pac. J. Trop. Med. 2012, 5, 323–325. [Google Scholar] [CrossRef] [Green Version]
- Köhler, C.A.; Freitas, T.H.; Maes, M.; De Andrade, N.Q.; Liu, C.S.; Fernandes, B.S.; Stubbs, B.; Solmi, M.; Veronese, N.; Herrmann, N.; et al. Peripheral cytokine and chemokine alterations in depression: A meta-analysis of 82 studies. Acta Psychiatr. Scand. 2017, 135, 373–387. [Google Scholar] [CrossRef]
- Dowlati, Y.; Herrmann, N.; Swardfager, W.; Liu, H.; Sham, L.; Reim, E.K.; Lanctôt, K.L. A Meta-Analysis of Cytokines in Major Depression. Biol. Psychiatry 2010, 67, 446–457. [Google Scholar] [CrossRef]
- Yao, L.; Pan, L.; Qian, M.; Sun, W.; Gu, C.; Chen, L.; Tang, X.; Hu, Y.; Xu, L.; Wei, Y.; et al. Tumor Necrosis Factor-α Variations in Patients with Major Depressive Disorder Before and After Antidepressant Treatment. Front. Psychiatry 2020, 11, 518837. [Google Scholar] [CrossRef] [PubMed]
- Miranda, D.O.; De Lima, T.A.S.; Azevedo, L.R.; Féres, O.; Da Rocha, J.J.R.; Pereira-Da-Silva, G. Proinflammatory Cytokines Correlate with Depression and Anxiety in Colorectal Cancer Patients. BioMed Res. Int. 2014, 2014, 1–5. [Google Scholar] [CrossRef]
- Hori, H.; Kim, Y. Inflammation and post-traumatic stress disorder. Psychiatry Clin. Neurosci. 2019, 73, 143–153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tavakoli-Ardakani, M.; Mehrpooya, M.; Mehdizadeh, M.; Hajifathali, A.; Abdolahi, A. Association between Interlukin-6 (IL-6), Interlukin-10 (IL-10) and depression in patients undergoing Hematopoietic stem cell transplantation. Int. J. Hematol. Stem Cell Res. 2015, 9, 80–87. [Google Scholar]
- Dhabhar, F.S.; Burke, H.M.; Epel, E.S.; Mellon, S.H.; Rosser, R.; Reus, V.; Wolkowitz, O.M. Low serum IL-10 concentrations and loss of regulatory association between IL-6 and IL-10 in adults with major depression. J. Psychiatr. Res. 2009, 43, 962–969. [Google Scholar] [CrossRef]
- Zou, W.; Feng, R.; Yang, Y. Changes in the serum levels of inflammatory cytokines in antidepressant drug-naïve patients with major depression. PLoS ONE 2018, 13, e0197267. [Google Scholar] [CrossRef] [PubMed]
- Gazal, M.; Jansen, K.; Souza, L.D.; Oses, J.P.; Magalhães, P.V.; Pinheiro, R.; Ghisleni, G.; Quevedo, L.; Kaster, M.P.; Kapczinski, F.; et al. Association of interleukin-10 levels with age of onset and duration of illness in patients with major depressive disorder. Rev. Bras. Psiquiatr. 2015, 37, 296–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teche, S.P.; Rovaris, D.L.; Aguiar, B.W.; Hauck, S.; Vitola, E.S.; Bau, C.H.; Freitas, L.H.; Grevet, E.H. Resilience to traumatic events related to urban violence and increased IL10 serum levels. Psychiatry Res. 2017, 250, 136–140. [Google Scholar] [CrossRef]
- De Oliveira, J.F.; Wiener, C.D.; Jansen, K.; Portela, L.V.; Lara, D.R.; Souza, L.D.D.M.; da Silva, R.A.; Moreira, F.P.; Oses, J.P. Serum levels of interleukins IL-6 and IL-10 in individuals with posttraumatic stress disorder in a population-based sample. Psychiatry Res. 2018, 260, 111–115. [Google Scholar] [CrossRef]
- Hou, R.; Garner, M.; Holmes, C.; Osmond, C.; Teeling, J.; Lau, L.; Baldwin, D.S. Peripheral inflammatory cytokines and immune balance in Generalised Anxiety Disorder: Case-controlled study. Brain Behav. Immun. 2017, 62, 212–218. [Google Scholar] [CrossRef] [Green Version]
- Xu, M.L.; Yue, J.K.; Korley, F.K.; Puccio, A.M.; Yuh, E.L.; Sun, M.X.; Rabinowitz, M.; Vassar, M.M.; Taylor, S.R.; Winkler, E.A.; et al. High-Sensitivity C-Reactive Protein is a Prognostic Biomarker of Six-Month Disability after Traumatic Brain Injury: Results from the TRACK-TBI Study. J. Neurotrauma 2021, 38, 918–927. [Google Scholar] [CrossRef] [PubMed]
- Sogut, O.; Guloglu, C.; Orak, M.; Sayhan, M.; Gokdemir, M.; Ustundag, M.; Akkus, Z. Trauma Scores and Neuron-Specific Enolase, Cytokine and C-Reactive Protein Levels as Predictors of Mortality in Patients with Blunt Head Trauma. J. Int. Med. Res. 2010, 38, 1708–1720. [Google Scholar] [CrossRef]
- Wium-Andersen, M.K.; Ørsted, D.D.; Nielsen, S.F.; Nordestgaard, B.G. Elevated C-Reactive Protein Levels, Psychological Distress, and Depression in 73 131 Individuals. JAMA Psychiatry 2013, 70, 176–184. [Google Scholar] [CrossRef] [Green Version]
- Heath, N.M.; Chesney, S.A.; Gerhart, J.I.; Goldsmith, R.E.; Luborsky, J.L.; Stevens, N.R.; Hobfoll, S.E. Interpersonal violence, PTSD, and inflammation: Potential psychogenic pathways to higher C-reactive protein levels. Cytokine 2013, 63, 172–178. [Google Scholar] [CrossRef] [Green Version]
- Powers, A.; Dixon, H.D.; Conneely, K.; Gluck, R.; Munoz, A.; Rochat, C.; Mendoza, H.; Hartzell, G.; Ressler, K.J.; Bradley, B.; et al. The differential effects of PTSD, MDD, and dissociation on CRP in trauma-exposed women. Compr. Psychiatry 2019, 93, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Felger, J.C.; Haroon, E.; Patel, T.A.; Goldsmith, D.R.; Wommack, E.C.; Woolwine, B.J.; Le, N.-A.; Feinberg, R.; Tansey, M.G.; Miller, A.H. What does plasma CRP tell us about peripheral and central inflammation in depression? Mol. Psychiatry 2020, 25, 1301–1311. [Google Scholar] [CrossRef] [PubMed]
- Liukkonen, T.; Räsänen, P.; Jokelainen, J.; Leinonen, M.; Järvelin, M.-R.; Meyer-Rochow, V.; Timonen, M. The association between anxiety and C-reactive protein (CRP) levels: Results from the Northern Finland 1966 Birth Cohort Study. Eur. Psychiatry 2011, 26, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Passos, I.C.; Vasconcelos-Moreno, M.P.; Costa, L.G.; Kunz, M.; Brietzke, E.; Quevedo, J.; Salum, G.; Magalhães, P.V.; Kapczinski, F.; Kauer-Sant’Anna, M. Inflammatory markers in post-traumatic stress disorder: A systematic review, meta-analysis, and meta-regression. Lancet Psychiatry 2015, 2, 1002–1012. [Google Scholar] [CrossRef]
- Owen, B.M.; Eccleston, D.; Ferrier, I.N.; Young, H. Raised levels of plasma interleukin-1β in major and postviral depression. Acta Psychiatr. Scand. 2001, 103, 226–228. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author and Year | Population | mTBI Setting | Cytokine(s) | Biospecimen | Outcome of Interest | Acute/Chronic (Average Time) |
|---|---|---|---|---|---|---|
| Bellgowan et al. (2012) | n = 9 (Cases = 9, Controls = 0) | Sports | IL-1β | Blood—venous plasma | IL-1β levels were significantly elevated at 24–48 h compared to either 1 week or 1 month post-concussion. Depression and anxiety ratings significantly higher at 24–48 h and 1 week, but not 1 month after concussion. | Acute (24 h, 1 week–4 weeks) |
| Ghai et al. (2020) | n = 69 (Cases = 27, Non-mTBI Veterans (DC) = 11, Community Controls (CC) = 31) | Military | CRP | Blood—venous plasma | Elevated CRP levels in chronic mTBI patients compared to CC and DC controls. Chronic mTBI group had significantly greater comorbid PTSD and depressive symptoms, compared to CC and DC. | Chronic (4.6 years) |
| Gill et al. (2018) | n = 64 (Cases = 42, Controls = 22) | Military | IL-6, IL-10, TNFα | Blood exosomal plasma | Chronic mTBI patients had elevated exosomal IL-10 levels compared to controls. PTSD was significantly related, and depression tended to be related to exosomal IL-10. | Chronic (3–36 months) |
| Guedes et al. (2020) | n = 195 (Cases = 150, Controls = 45) | Military | IL-6, TNF-α, IL-10 | Blood venous plasma | mTBI group had increased PTSD and depression symptoms compared to controls. Plasma TNF-α (p = 0.02) and exosomal IL-6 (p = 0.08) levels correlated with PTSD. | Chronic (NR) |
| Kanefsky et al. (2019) | n = 143 mTBI+LOC (n = 25), mTBI without LOC (n = 36), Controls = 82) | Military | TNF-a, IL-6, IL-10 | Blood venous plasma | Both mTBI groups (+/− LOC) reported significantly greater depression and PTSD symptoms compared to controls. IL-6 was elevated in the mTBI with LOC group compared to both the mTBI w/out LOC and control groups. Within the mTBI groups, increased TNF-α concentrations were associated with greater PTSD symptoms (r = 0.36, p = 0.005). | Chronic (NR) |
| Peskind et al. (2015) | n = 105 (Cases = 35, Non-mTBI Veterans (DC) = 16 Community Controls (CC) = 55 | Military | IL-7, IL-6 | CSF | mTBI veterans had greater PTSD and depression and elevated CSF IL-7 levels compared to the DC. CSF IL-6 levels did not differ between mTBI Veterans and DC but was significantly higher in both Veteran groups than in CCs. | Chronic (NR) |
| Su et al. (2014) | n = 213 (Cases = 213, Controls = 0) | Trauma | CRP | Blood venous plasma | CRP levels were significantly correlated with PCS, persistent psychological problems and persistent cognitive impairments. | Chronic (1–3 months) |
| Vedantam et al. (2021) | n = 77 (Cases = 53, OI Controls = 24) | Trauma | IL-1β, IL-2, IL-4, IL-6, IL-10, IL-17, IFN-γ, TNFα, IL-12p70 | Blood exosomal plasma | Within 24 h, IL-2 and IL-6 levels were significantly elevated in the mTBI population vs. OI controls. At 6 months post-injury, mTBI group had elevated IL-6 (p = 0.044) levels vs. OI controls. Elevated IL-10 levels at 6-month post-mTBI was significantly associated with severe PTSD (p = 0.004) symptoms and worse mood (p = 0.001). | Acute (24 h)/ Chronic (6 months) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malik, S.; Alnaji, O.; Malik, M.; Gambale, T.; Rathbone, M.P. Correlation between Mild Traumatic Brain Injury-Induced Inflammatory Cytokines and Emotional Symptom Traits: A Systematic Review. Brain Sci. 2022, 12, 102. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci12010102
Malik S, Alnaji O, Malik M, Gambale T, Rathbone MP. Correlation between Mild Traumatic Brain Injury-Induced Inflammatory Cytokines and Emotional Symptom Traits: A Systematic Review. Brain Sciences. 2022; 12(1):102. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci12010102
Chicago/Turabian StyleMalik, Shazia, Omar Alnaji, Mahnoor Malik, Teresa Gambale, and Michel Piers Rathbone. 2022. "Correlation between Mild Traumatic Brain Injury-Induced Inflammatory Cytokines and Emotional Symptom Traits: A Systematic Review" Brain Sciences 12, no. 1: 102. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci12010102