
The Prevalence and Comorbidity of Tic Disorders and Obsessive-Compulsive Disorder in Chinese School Students Aged 6–16: A National Survey

Abstract
:
1. Introduction
2. Methods
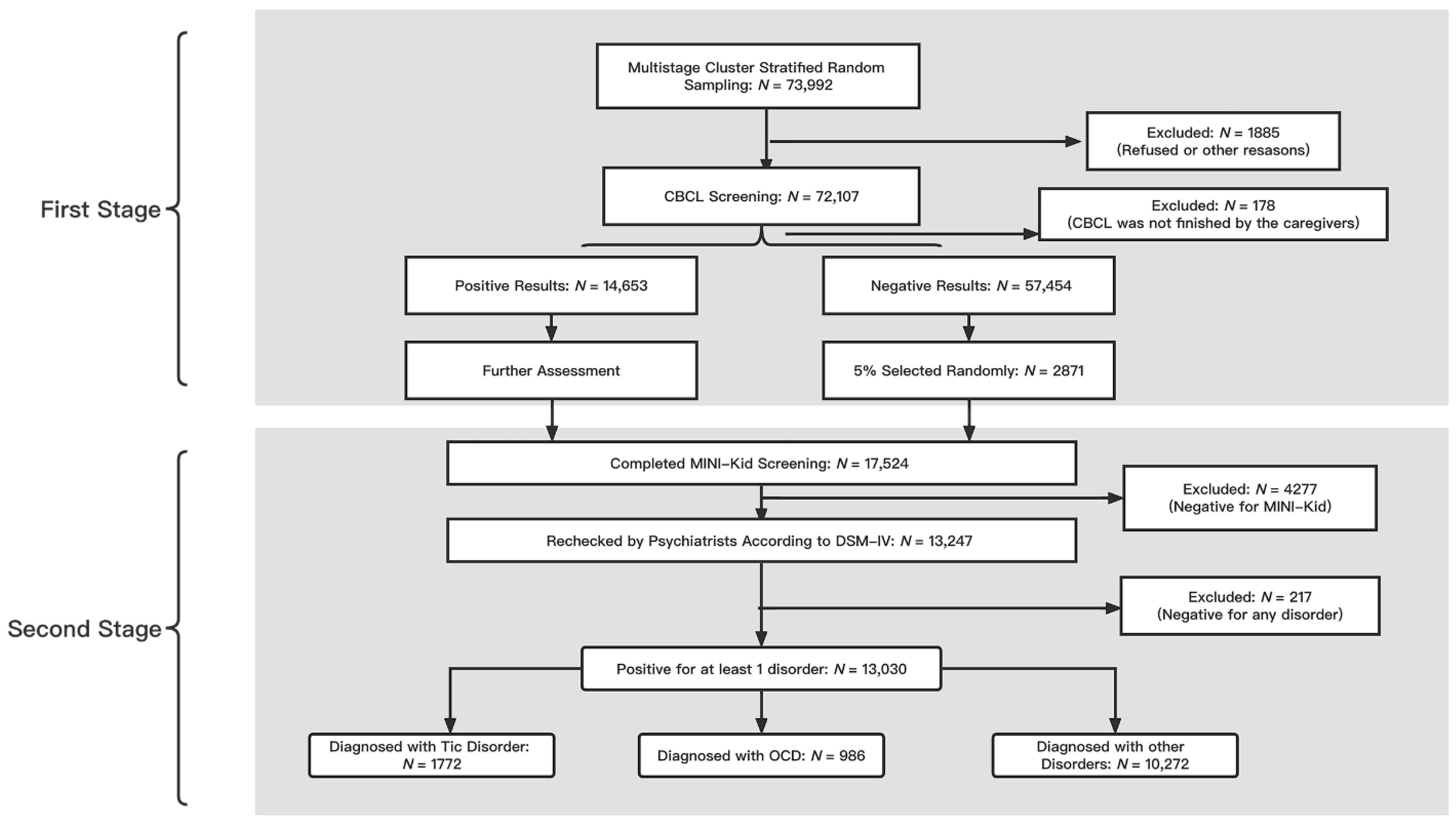
2.1. Participants
2.2. Screening Scales
2.3. Statistical Analysis
2.4. The Introduction of the Study Protocol
3. Results
3.1. Sample Description
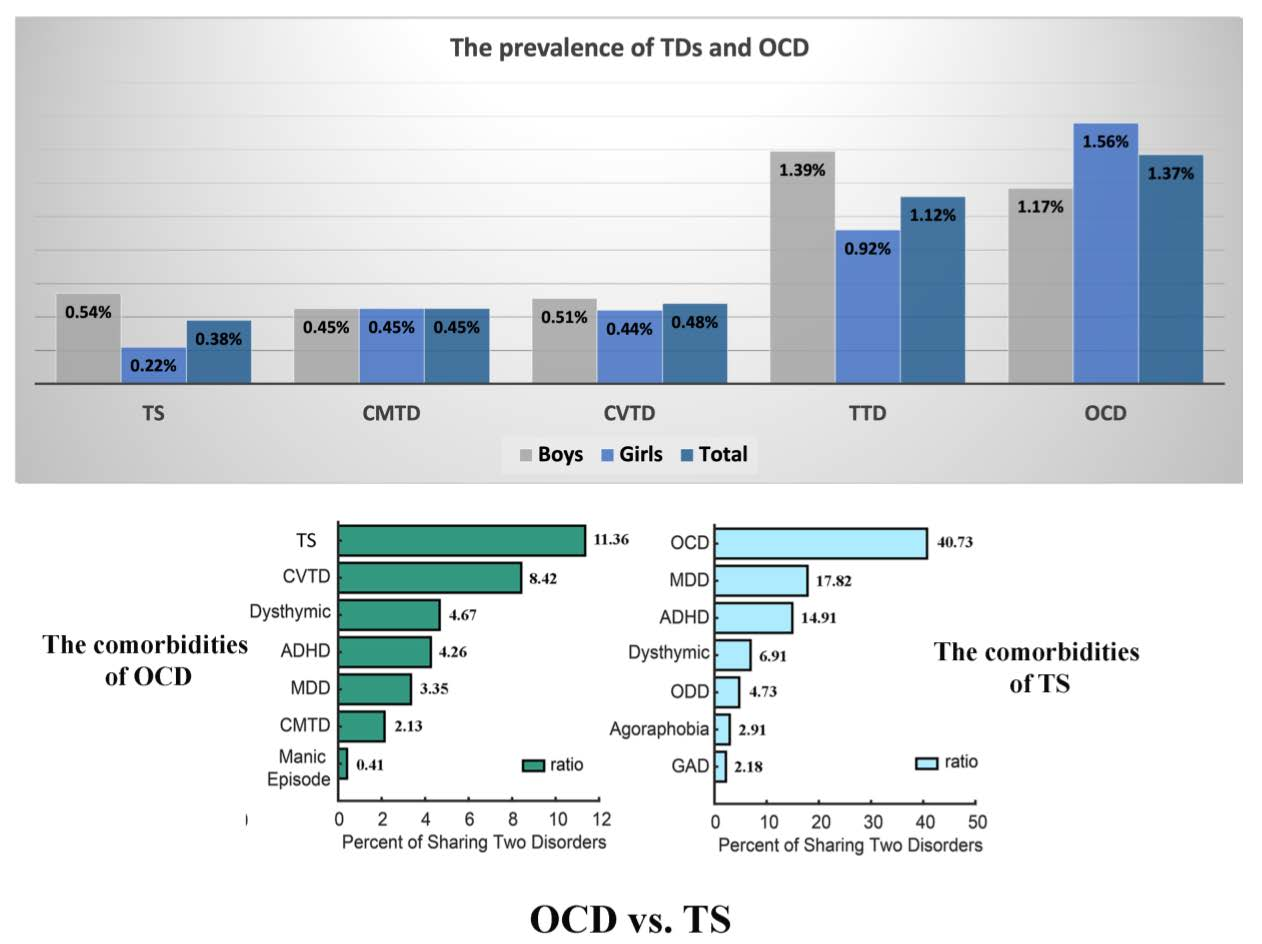
3.2. Point Prevalence of TD and OCD
3.3. Sex Effects on the Prevalence of TD and OCD
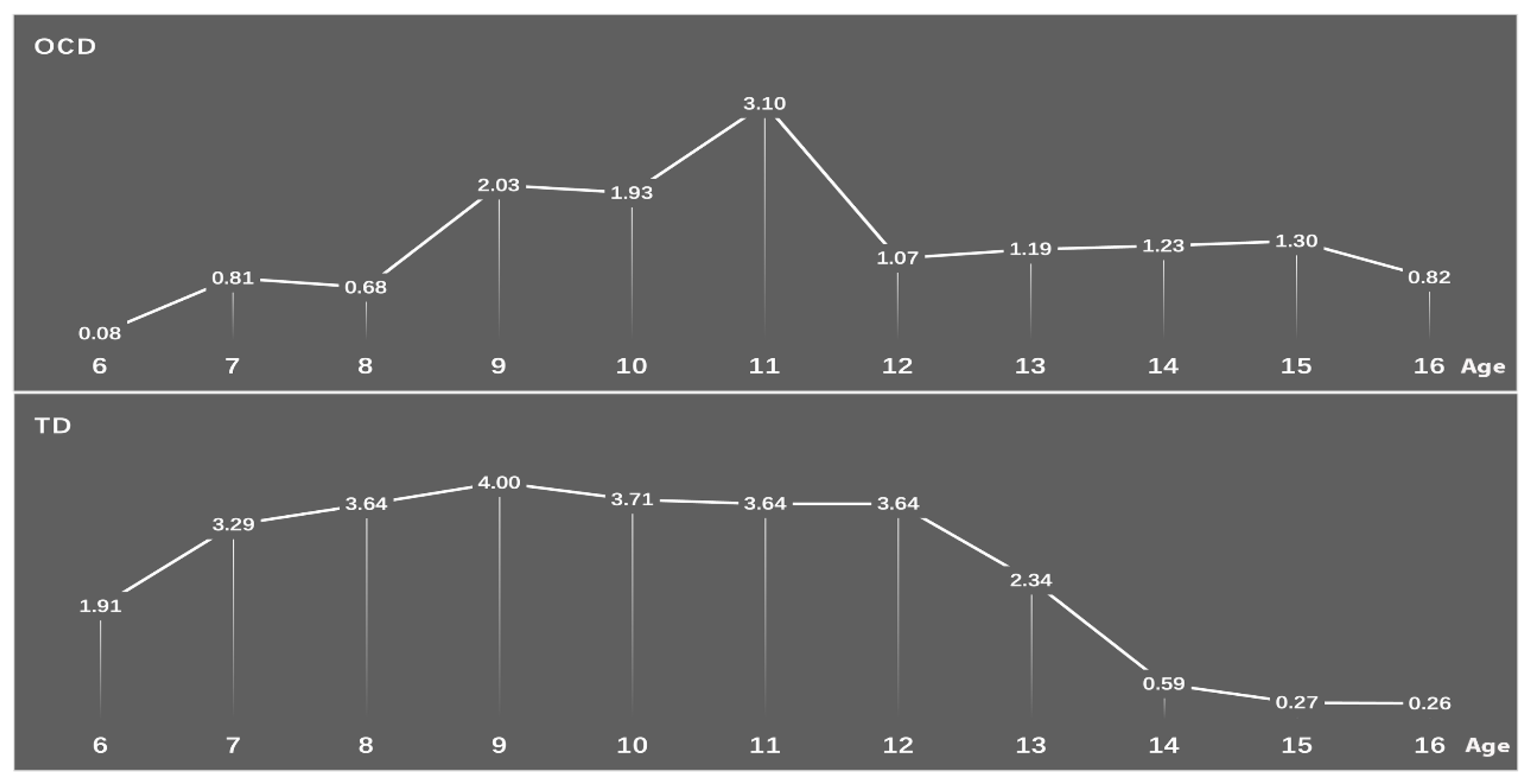
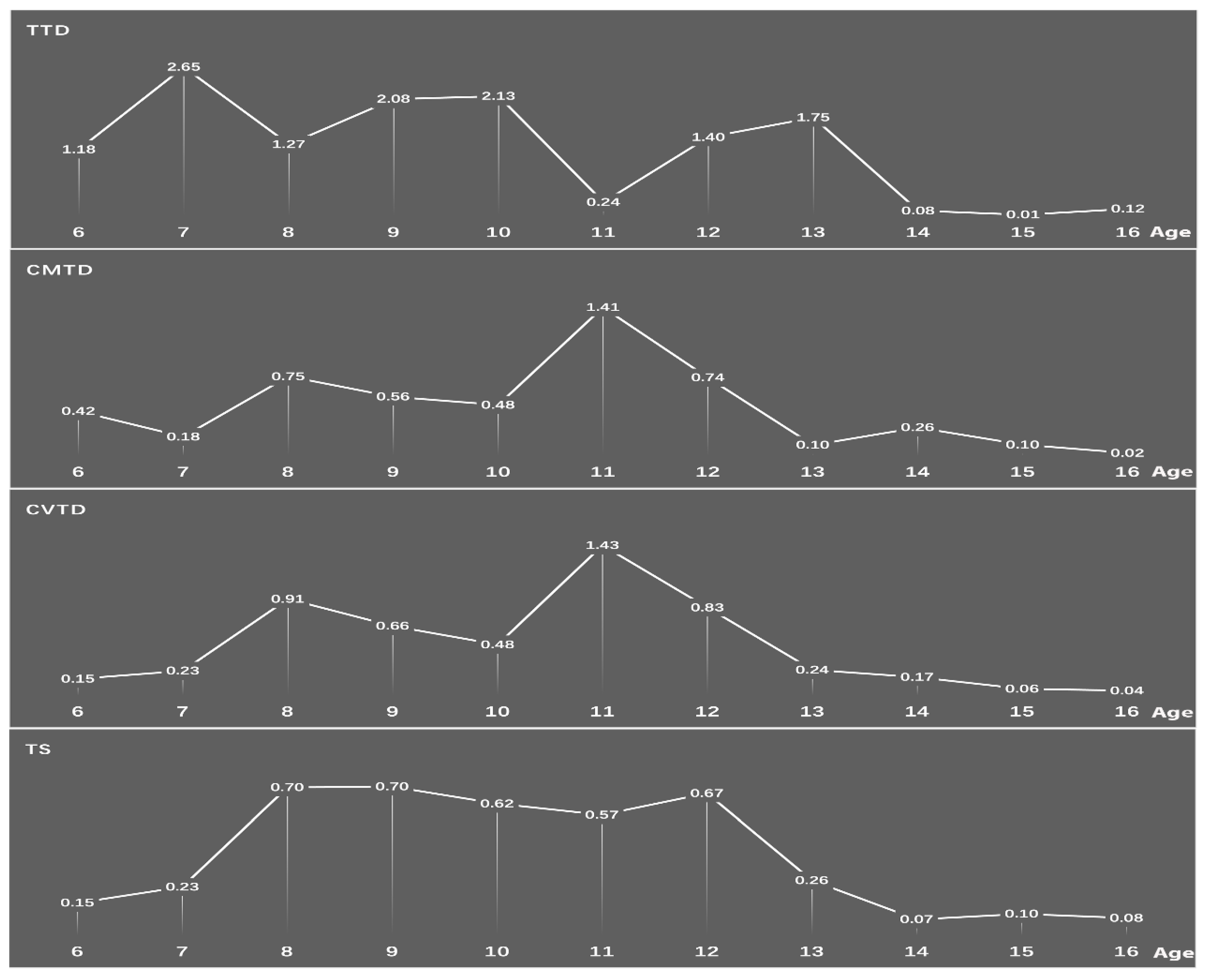
3.4. Age Effects on the Prevalence of TD and OCD
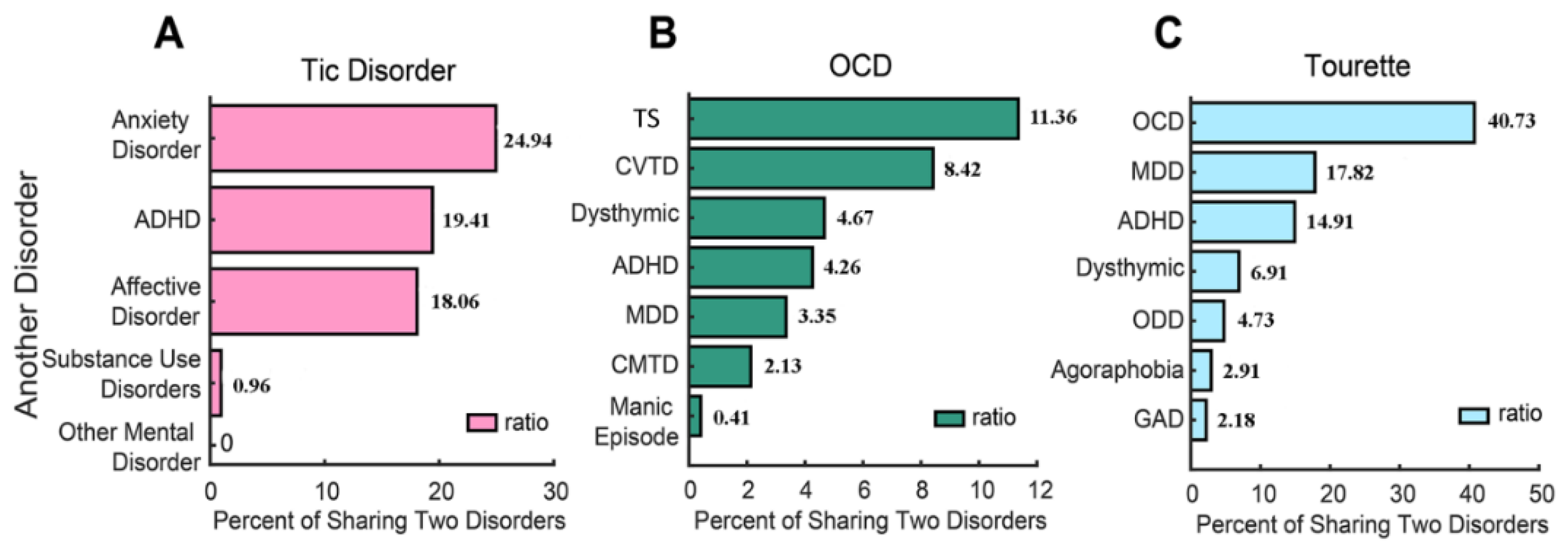
3.5. Comorbidities of TD, TS, and OCD
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- APA. American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; (DSM-5); APA: Washington, DC, USA, 2013. [Google Scholar]
- Hartmann, A.; Millet, B. Repetitive movements and behaviors in neurological and psychiatric practice: Distinctions and similarities between Tourette disorder and obsessive-compulsive disorder. Rev. Neurol. 2018, 174, 199–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirschtritt, M.E.; Lee, P.C.; Pauls, D.L.; Dion, Y.; Grados, M.A.; Illmann, C.; King, R.A.; Sandor, P.; McMahon, W.M.; Lyon, G.J.; et al. Lifetime prevalence, age of risk, and genetic relationships of comorbid psychiatric disorders in Tourette syndrome. JAMA Psychiatry 2015, 72, 325–333. [Google Scholar] [CrossRef] [PubMed]
- Groth, C. Tourette syndrome in a longitudinal perspective. Clinical course of tics and comorbidities, coexisting psychopathologies, phenotypes and predictors. Dan. Med. J. 2018, 65, B5465. [Google Scholar] [PubMed]
- Leckman, J.F. Tourette’s syndrome. Lancet 2002, 360, 1577–1586. [Google Scholar] [CrossRef]
- Martino, D.; Ganos, C.; Pringsheim, T.M. Tourette Syndrome and Chronic Tic Disorders: The Clinical Spectrum Beyond Tics. Int. Rev. Neurobiol. 2017, 134, 1461–1490. [Google Scholar] [CrossRef] [PubMed]
- Gadow, K.D.; Nolan, E.E.; Sprafkin, J.; Schwartz, J. Tics and psychiatric comorbidity in children and adolescents. Dev. Med. Child Neurol. 2002, 44, 330–338. [Google Scholar] [CrossRef]
- Khalifa, N.; Von Knorring, A.L. Psychopathology in a Swedish population of school children with tic disorders. J. Am. Acad. Child Adolesc. Psychiatry 2006, 45, 1346–1353. [Google Scholar] [CrossRef]
- Bloch, M.H.; Leckman, J.F. Clinical course of Tourette syndrome. J. Psychosom. Res. 2009, 67, 497–501. [Google Scholar] [CrossRef] [Green Version]
- Ivarsson, T.; Melin, K.; Wallin, L. Categorical and dimensional aspects of co-morbidity in obsessive-compulsive disorder (OCD). Eur. Child Adolesc. Psychiatry 2008, 17, 20–31. [Google Scholar] [CrossRef] [Green Version]
- Langley, A.K.; Lewin, A.B.; Bergman, R.L.; Lee, J.C.; Piacentini, J. Correlates of comorbid anxiety and externalizing disorders in childhood obsessive compulsive disorder. Eur. Child Adolesc. Psychiatry 2010, 19, 637–645. [Google Scholar] [CrossRef] [Green Version]
- Peris, T.S.; Bergman, R.L.; Asarnow, J.R.; Langley, A.; McCracken, J.T.; Piacentini, J. Clinical and cognitive correlates of depressive symptoms among youth with obsessive compulsive disorder. J. Clin. Child Adolesc. Psychol. 2010, 39, 616–626. [Google Scholar] [CrossRef] [PubMed]
- Piacentini, J.; Bergman, R.L.; Keller, M.; McCracken, J. Functional impairment in children and adolescents with obsessive-compulsive disorder. J. Child Adolesc. Psychopharmacol. 2003, 13 (Suppl. 1), S61–S69. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Li, Z.; Buys, N.; Storch, E.A. Correlates of comorbid depression, anxiety and helplessness with obsessive-compulsive disorder in Chinese adolescents. J. Affect. Disord. 2015, 174, 31–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewin, A.B.; Chang, S.; McCracken, J.; McQueen, M.; Piacentini, J. Comparison of clinical features among youth with tic disorders, obsessive-compulsive disorder (OCD), and both conditions. Psychiatry Res. 2010, 178, 317–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kloft, L.; Steinel, T.; Kathmann, N. Systematic review of co-occurring OCD and TD: Evidence for a tic-related OCD subtype? Neurosci. Biobehav. Rev. 2018, 95, 280–314. [Google Scholar] [CrossRef]
- Scharf, J.M.; Miller, L.L.; Gauvin, C.A.; Alabiso, J.; Mathews, C.A.; Ben-Shlomo, Y. Population prevalence of Tourette syndrome: A systematic review and meta-analysis. Mov. Disord. 2015, 30, 221–228. [Google Scholar] [CrossRef]
- Hollander, E.; Doernberg, E.; Shavitt, R.; Waterman, R.J.; Soreni, N.; Veltman, D.J.; Sahakian, B.J.; Fineberg, N.A. The cost and impact of compulsivity: A research perspective. Eur. Neuropsychopharmacol. 2016, 26, 800–809. [Google Scholar] [CrossRef]
- Liu, Y.; Zheng, Y.; Han, S.; Cui, Y. Tic disorders in children aged 6–16 years in Daxing district of Beijing: A cross-sectional study. Chin. J. Psychiatry 2009, 42, 231–234. [Google Scholar]
- Sun, J.; Boschen, M.J.; Farrell, L.J.; Buys, N.; Li, Z.J. Obsessive-compulsive symptoms in a normative Chinese sample of youth: Prevalence, symptom dimensions, and factor structure of the Leyton Obsessional Inventory--Child Version. J. Affect. Disord. 2014, 164, 19–27. [Google Scholar] [CrossRef]
- Qu, Y.; Jiang, H.; Zhang, N.; Wang, D.; Guo, L. Prevalence of mental disorders in 6-16-year-old students in Sichuan province, China. Int. J. Environ. Res. Public Health 2015, 12, 5090–5107. [Google Scholar] [CrossRef] [Green Version]
- Shen, Y.M.; Chan, B.S.M.; Liu, J.B.; Zhou, Y.Y.; Cui, X.L.; He, Y.Q.; Fang, Y.M.; Xiang, Y.T.; Luo, X.R. The prevalence of psychiatric disorders among students aged 6~ 16 years old in central Hunan, China. BMC Psychiatry 2018, 18, 243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, Y.; Zhang, L.; Wang, F.; Zhang, P.; Ye, B.; Liang, Y. The effects of family structure and function on mental health during China’s transition: A cross-sectional analysis. BMC Fam. Pract. 2017, 18, 59. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Cui, Y.; Li, Y.; Guo, L.; Ke, X.; Liu, J.; Luo, X.; Zheng, Y.; Leckman, J.F. Prevalence of mental disorders in school children and adolescents in China: Diagnostic data from detailed clinical assessments of 17,524 individuals. J. Child Psychol. Psychiatry 2022, 63, 34–46. [Google Scholar] [CrossRef] [PubMed]
- Cui, Y.; Li, F.; Leckman, J.F.; Guo, L.; Ke, X.; Liu, J.; Zheng, Y.; Li, Y. The prevalence of behavioral and emotional problems among Chinese school children and adolescents aged 6-16: A national survey. Eur. Child Adolesc. Psychiatry 2021, 30, 233–241. [Google Scholar] [CrossRef] [PubMed]
- Achenback, T.M.; Edelbrock, C. Manual for the Child Behavior Checklist and Revised Child Behavior Profile; University of Vermont, Department of Psychiatry: Burlington, VT, USA, 1983. [Google Scholar]
- Leung, P.W.; Kwong, S.L.; Tang, C.P.; Ho, T.P.; Hung, S.F.; Lee, C.C.; Hong, S.L.; Chiu, C.M.; Liu, W.S. Test-retest reliability and criterion validity of the Chinese version of CBCL, TRF, and YSR. J. Child Psychol. Psychiatry 2006, 47, 970–973. [Google Scholar] [CrossRef] [PubMed]
- Rescorla, L.A.; Jordan, P.; Zhang, S.; Baelen-King, G.; Althoff, R.R.; Ivanova, M.Y.; International ASEBA Consortium. Latent Class Analysis of the CBCL Dysregulation Profile for 6- to 16-Year-Olds in 29 Societies. J. Clin. Child Adolesc. Psychol. 2021, 50, 551–564. [Google Scholar] [CrossRef]
- Xin, R.E.; Zhang, Z.X. National-wide urban only child psychiatric epidemiological survey, mental disorder prevention guidance and Achenbach’s rating scale adjustment: Data of 24013 children in 22 cities and 26 organizations. Shanghai Arch. Psychiatry 1992, 4, 47–55. (In Chinese) [Google Scholar]
- Su, L.; Li, X. Restandardization and Validity Inspection for Revised Chinese Version Achenbach Checklist. Chin. Ment. Health J. 1998, 12, 67–69. [Google Scholar]
- Biederman, J.; DiSalvo, M.; Vaudreuil, C.; Wozniak, J.; Uchida, M.; Yvonne Woodworth, K.; Green, A.; Faraone, S.V. Can the Child Behavior Checklist (CBCL) help characterize the types of psychopathologic conditions driving child psychiatry referrals? Scand J. Child Adolesc. Psychiatr. Psychol 2020, 8, 157–165. [Google Scholar] [CrossRef]
- Sheehan, D.V.; Sheehan, K.H.; Shytle, R.D.; Janavs, J.; Bannon, Y.; Rogers, J.E.; Milo, K.M.; Stock, S.L.; Wilkinson, B. Reliability and validity of the Mini International Neuropsychiatric Interview for Children and Adolescents (MINI-KID). J. Clin. Psychiatry 2010, 71, 313–326. [Google Scholar] [CrossRef]
- Liu, X.; Sun, Z.; Neiderhiser, J.M.; Uchiyama, M.; Okawa, M.; Rogan, W. Behavioral and emotional problems in Chinese adolescents: Parent and teacher reports. J. Am. Acad. Child Adolesc. Psychiatry 2001, 40, 828–836. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.-X.; Liu, J.; Wang, Y.-F. Reliability and validity of Chinese version of the Mini International Neuropsychiatric Interview for Children and Adolescents (Parent Version). Chin. Ment. Health J. 2010, 24, 921–925. [Google Scholar]
- Schafer, J.L. Multiple imputation: A primer. Stat. Methods Med. Res. 1999, 8, 3–15. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.; Peng, C.Y. Principled missing data methods for researchers. Springerplus 2013, 2, 222. [Google Scholar] [CrossRef] [Green Version]
- Knight, T.; Steeves, T.; Day, L.; Lowerison, M.; Jette, N.; Pringsheim, T. Prevalence of tic disorders: A systematic review and meta-analysis. Pediatr. Neurol. 2012, 47, 77–90. [Google Scholar] [CrossRef]
- Scahill, L.; Specht, M.; Page, C. The Prevalence of Tic Disorders and Clinical Characteristics in Children. J. Obs. Compuls. Relat. Disord. 2014, 3, 394–400. [Google Scholar] [CrossRef] [Green Version]
- Cubo, E.; Gabriel y Galan, J.M.; Villaverde, V.A.; Velasco, S.S.; Benito, V.D.; Macarron, J.V.; Guevara, J.C.; Louis, E.D.; Benito-Leon, J. Prevalence of tics in schoolchildren in central Spain: A population-based study. Pediatr. Neurol. 2011, 45, 100–108. [Google Scholar] [CrossRef]
- Linazasoro, G.; Van Blercom, N.; de Zarate, C.O. Prevalence of tic disorder in two schools in the Basque country: Results and methodological caveats. Mov. Disord. 2006, 21, 2106–2109. [Google Scholar] [CrossRef]
- Leckman, J.F.; Peterson, B.S.; Pauls, D.L.; Cohen, D.J. Tic disorders. Psychiatr. Clin. N. Am. 1997, 20, 839–861. [Google Scholar] [CrossRef]
- Robertson, M.M. A personal 35 year perspective on Gilles de la Tourette syndrome: Prevalence, phenomenology, comorbidities, and coexistent psychopathologies. Lancet Psychiatry 2015, 2, 68–87. [Google Scholar] [CrossRef]
- Reinherz, H.Z.; Giaconia, R.M.; Lefkowitz, E.S.; Pakiz, B.; Frost, A.K. Prevalence of psychiatric disorders in a community population of older adolescents. J. Am. Acad. Child Adolesc. Psychiatry 1993, 32, 369–377. [Google Scholar] [CrossRef] [PubMed]
- Canals, J.; Hernandez-Martinez, C.; Cosi, S.; Voltas, N. The epidemiology of obsessive—Compulsive disorder in Spanish school children. J. Anxiety Disord. 2012, 26, 746–752. [Google Scholar] [CrossRef] [PubMed]
- Douglass, H.M.; Moffitt, T.E.; Dar, R.; McGee, R.; Silva, P. Obsessive-compulsive disorder in a birth cohort of 18-year-olds: Prevalence and predictors. J. Am. Acad. Child Adolesc. Psychiatry 1995, 34, 1424–1431. [Google Scholar] [CrossRef] [PubMed]
- Brynska, A.; Wolanczyk, T. Epidemiology and phenomenology of obsessive-compulsive disorder in non-referred young adolescents: A Polish perspective. Eur. Child Adolesc. Psychiatry 2005, 14, 319–327. [Google Scholar] [CrossRef]
- Heyman, I.; Fombonne, E.; Simmons, H.; Ford, T.; Meltzer, H.; Goodman, R. Prevalence of obsessive-compulsive disorder in the British nationwide survey of child mental health. Br. J. Psychiatry 2001, 179, 324–329. [Google Scholar] [CrossRef]
- Valleni-Basile, L.A.; Garrison, C.Z.; Jackson, K.L.; Waller, J.L.; McKeown, R.E.; Addy, C.L.; Cuffe, S.P. Frequency of obsessive-compulsive disorder in a community sample of young adolescents. J. Am. Acad. Child Adolesc. Psychiatry 1994, 33, 782–791. [Google Scholar] [CrossRef]
- Fontenelle, L.F.; Hasler, G. The analytical epidemiology of obsessive-compulsive disorder: Risk factors and correlates. Prog. Neuropsychopharmacol. Biol. Psychiatry 2008, 32, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Marcks, B.A.; Weisberg, R.B.; Dyck, I.; Keller, M.B. Longitudinal course of obsessive-compulsive disorder in patients with anxiety disorders: A 15-year prospective follow-up study. Compr. Psychiatry 2011, 52, 670–677. [Google Scholar] [CrossRef] [Green Version]
- Bloch, M.H.; Peterson, B.S.; Scahill, L.; Otka, J.; Katsovich, L.; Zhang, H.; Leckman, J.F. Adulthood outcome of tic and obsessive-compulsive symptom severity in children with Tourette syndrome. Arch. Pediatrics Adolesc. Med. 2006, 160, 65–69. [Google Scholar] [CrossRef] [Green Version]
- Tagwerker Gloor, F.; Walitza, S. Tic Disorders and Tourette Syndrome: Current Concepts of Etiology and Treatment in Children and Adolescents. Neuropediatrics 2016, 47, 84–96. [Google Scholar] [CrossRef]
- Robertson, M.M.; Williamson, F.; Eapen, V. Depressive symptomatology in young people with Gilles de la Tourette Syndrome—A comparison of self-report scales. J. Affect. Disord. 2006, 91, 265–268. [Google Scholar] [CrossRef] [PubMed]
- Debes, N.M.; Hansen, A.; Skov, L.; Larsson, H. A functional magnetic resonance imaging study of a large clinical cohort of children with Tourette syndrome. J. Child Neurol. 2011, 26, 560–569. [Google Scholar] [CrossRef] [PubMed]
- Prado, H.S.; Rosario, M.C.; Lee, J.; Hounie, A.G.; Shavitt, R.G.; Miguel, E.C. Sensory phenomena in obsessive-compulsive disorder and tic disorders: A review of the literature. CNS Spectr. 2008, 13, 425–432. [Google Scholar] [CrossRef] [PubMed]
- Leckman, J.F.; Grice, D.E.; Barr, L.C.; de Vries, A.L.; Martin, C.; Cohen, D.J.; McDougle, C.J.; Goodman, W.K.; Rasmussen, S.A. Tic-related vs. non-tic-related obsessive compulsive disorder. Anxiety 1994, 1, 208–215. [Google Scholar] [PubMed]
- Leckman, J.F.; Walker, D.E.; Cohen, D.J. Premonitory urges in Tourette’s syndrome. Am. J. Psychiatry 1993, 150, 98–102. [Google Scholar] [CrossRef]
- Ferrao, Y.A.; Shavitt, R.G.; Prado, H.; Fontenelle, L.F.; Malavazzi, D.M.; de Mathis, M.A.; Hounie, A.G.; Miguel, E.C.; do Rosario, M.C. Sensory phenomena associated with repetitive behaviors in obsessive-compulsive disorder: An exploratory study of 1001 patients. Psychiatry Res. 2012, 197, 253–258. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC). Prevalence of diagnosed Tourette syndrome in persons aged 6–17 years—United States, 2007. Morb. Mortal. Wkly. Rep. 2009, 58, 581–585. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mental Disorders | Identified Individuals | Unweighted Point Prevalence (%) | Unweighted 95% CI (%) | Adjusted Point Prevalence (%) | Adjusted 95% CI (%) |
|---|---|---|---|---|---|
| OCD | 986 | 1.4 | 1.3–1.5 | 1.3 | 1.2–1.4 |
| TDs | 1772 | 2.5 | 2.4–2.6 | 2.5 | 2.3–3.0 |
| TS | 275 | 0.4 | 0.3–0.4 | 0.4 | 0.3–0.4 |
| CMTD/CVTD | 664 | 0.9 | 0.8–1.0 | 0.9 | 0.8–1.0 |
| TTD | 833 | 1.2 | 1.1–1.2 | 1.2 | 1.1–1.2 |
| Disorders | Boys | Girls | χ2 | p |
|---|---|---|---|---|
| (N = 35,953) | (N = 36,154) | |||
| OCD | 1.17% | 1.56% | 19.94 | <0.001 |
| Tic Disorder | 2.56% | 2.35% | 3.43 | >0.05 |
| TS | 0.54% | 0.22% | 47.27 | <0.001 |
| CMTD | 0.45% | 0.45% | <0.001 | >0.05 |
| CVTD | 0.51% | 0.44% | 1.68 | >0.05 |
| TTD | 1.39% | 0.92% | 34.00 | <0.001 |
| Disorders | Children | Adolescents | χ2 | p |
|---|---|---|---|---|
| (N = 41,332) | (N = 30,775) | |||
| OCD | 1.51% | 1.17% | 15.45 | <0.001 |
| Tic Disorder | 3.55% | 0.99% | 480.98 | <0.001 |
| TS | 0.56% | 0.14% | 84.76 | <0.001 |
| CMTD | 0.68% | 0.14% | 115.44 | <0.001 |
| CVTD | 0.72% | 0.14% | 125.54 | <0.001 |
| TTD | 1.59% | 0.58% | 157.65 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yan, J.; Deng, H.; Wang, Y.; Wang, X.; Fan, T.; Li, S.; Wen, F.; Yu, L.; Wang, F.; Liu, J.; et al. The Prevalence and Comorbidity of Tic Disorders and Obsessive-Compulsive Disorder in Chinese School Students Aged 6–16: A National Survey. Brain Sci. 2022, 12, 650. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci12050650
Yan J, Deng H, Wang Y, Wang X, Fan T, Li S, Wen F, Yu L, Wang F, Liu J, et al. The Prevalence and Comorbidity of Tic Disorders and Obsessive-Compulsive Disorder in Chinese School Students Aged 6–16: A National Survey. Brain Sciences. 2022; 12(5):650. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci12050650
Chicago/Turabian StyleYan, Junjuan, Hu Deng, Yongming Wang, Xiaolin Wang, Tengteng Fan, Shijie Li, Fang Wen, Liping Yu, Fang Wang, Jingran Liu, and et al. 2022. "The Prevalence and Comorbidity of Tic Disorders and Obsessive-Compulsive Disorder in Chinese School Students Aged 6–16: A National Survey" Brain Sciences 12, no. 5: 650. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci12050650