Therapeutic Plasma Exchange in Multiple Sclerosis and Autoimmune Encephalitis: A Comparative Study of Indication, Efficacy, and Safety

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
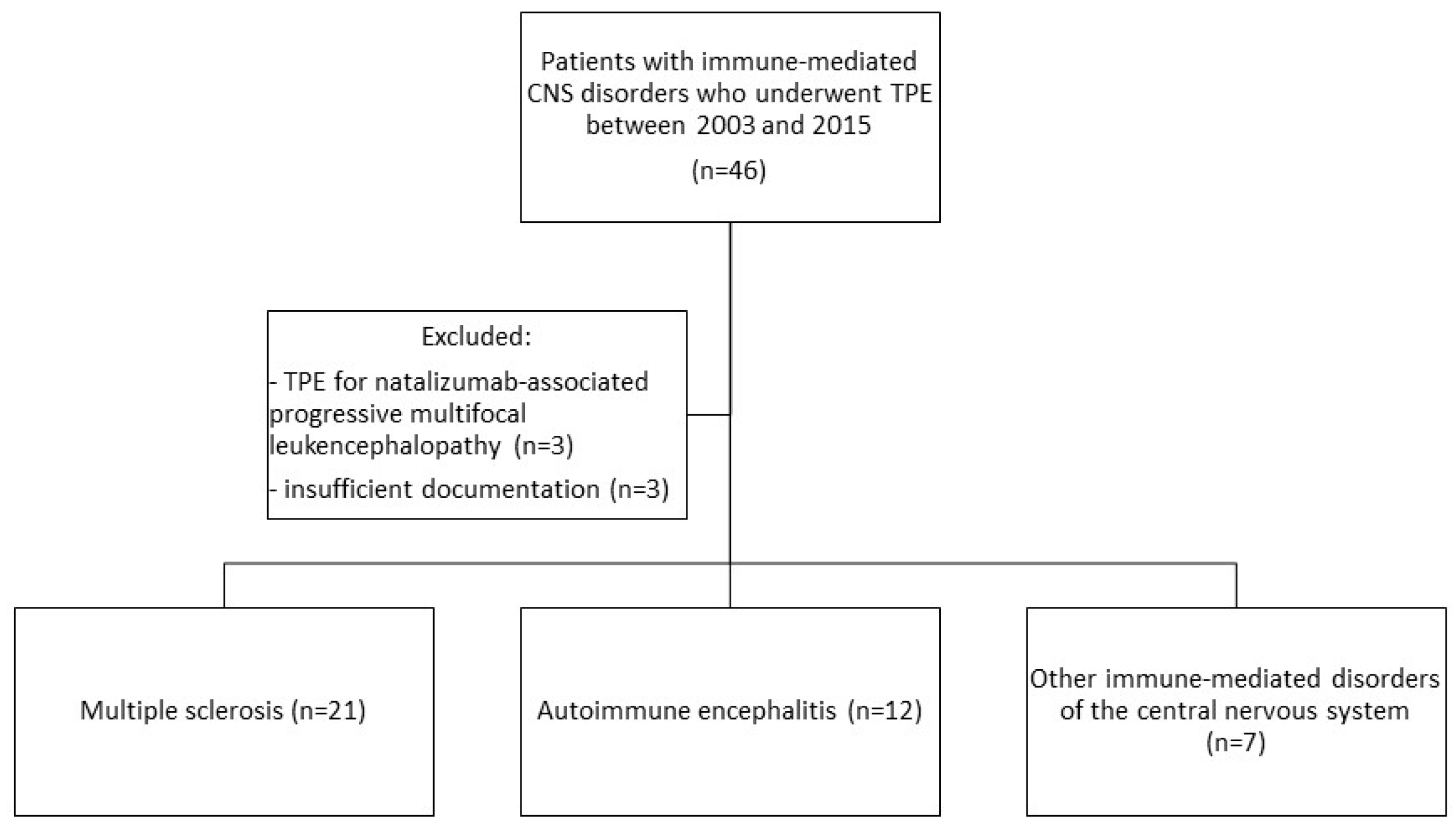
2.2. Study Population and Data Collection
- -
- acute immune-mediated disorder of the CNS
- -
- TPE during the period of January 2003 to December 2015
- -
- sufficient clinical documentation on underlying disease, indication, procedures, and complications
- -
- subacute onset (rapid progression of less than three months) of working memory deficits (short-term memory loss), altered mental status, or psychiatric symptoms
- -
- at least one of the following: new focal CNS findings, seizures not explained by a previously known seizure disorder, CSF pleocytosis (white blood cell count of more than five cells per μL), MRI features suggestive of encephalitis
2.3. Statistical Analysis
3. Results
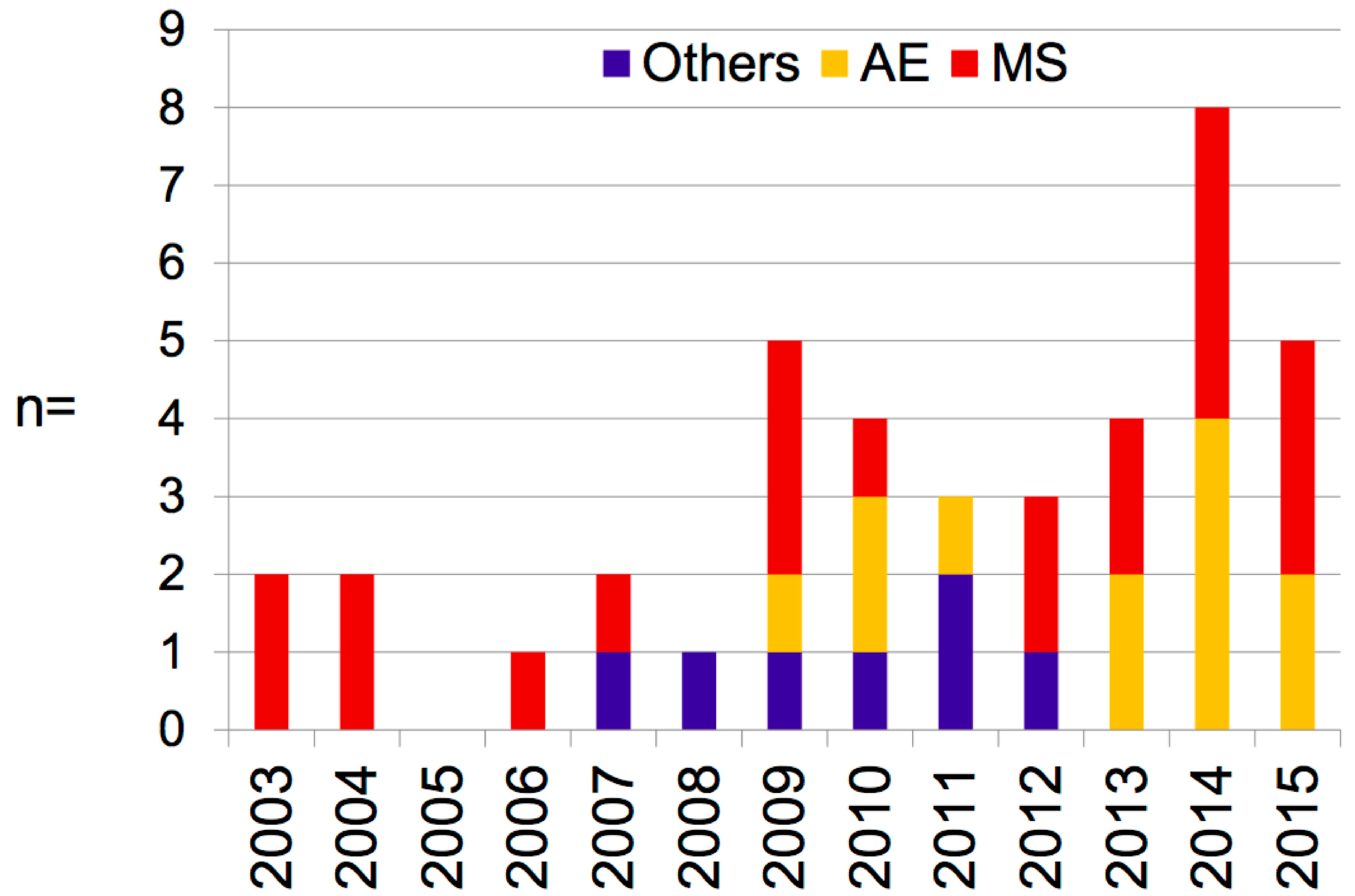
3.1. Clinical and Demographic Characteristics
3.2. Time from Symptom Onset to Start of TPE
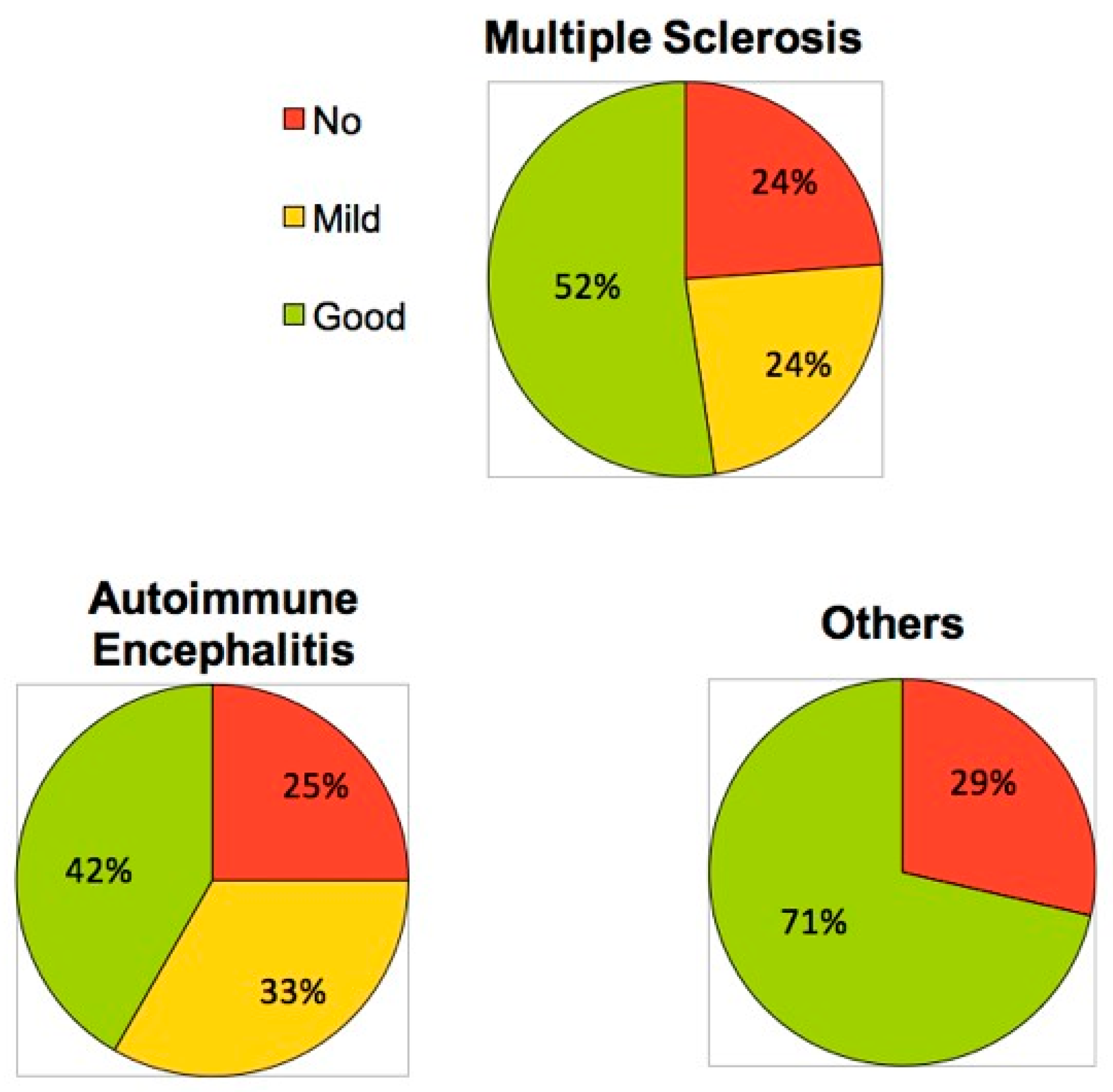
3.3. Outcome
3.4. Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| ADEM | Acute disseminated encephalomyelitis |
| AE | Autoimmune encephalitis |
| CNS-ID | Central nervous system-inflammatory disorders |
| GC | Glucocorticosteroids |
| IVIG | Intravenous immunoglobulins |
| LE | Limbic encephalitis |
| MS | Multiple sclerosis |
| NMDAR | N-methyl-D-aspartate-receptor encephalitis |
| NMOSD | Neuromyelitis optica spectrum disorder |
| NICU | Neurological intensive care unit |
| ON | Optic neuritis |
| TPE | Therapeutic plasma exchange |
References
- Mauch, E.; Zwanzger, J.; Hettich, R.; Fassbender, C.; Klingel, R.; Heigl, F. Immunoadsorption for steroid-unresponsive multiple sclerosis-relapses: clinical data of 14 patients. Nervenarzt 2011, 82, 1590–1595. [Google Scholar] [CrossRef] [PubMed]
- Trebst, C.; Bronzlik, P.; Kielstein, J.T.; Schmidt, B.M.; Stangel, M. Immunoadsorption Therapy for Steroid-Unresponsive Relapses in Patients with Multiple Sclerosis. Blood Purif. 2012, 33, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Correia, I.; Sousa, L. Plasma exchange in severe acute relapses of multiple sclerosis—Results from a Portuguese cohort. Mult. Scler. Relat. Disord. 2018, 19, 148–152. [Google Scholar] [CrossRef] [PubMed]
- Graus, F.; Titulaer, M.J.; Balu, R.; Benseler, S.; Bien, C.G.; Cellucci, T.; Cortese, I.; Dale, R.C.; Gelfand, J.M.; Geschwind, M.; et al. A clinical approach to diagnosis of autoimmune encephalitis. Lancet Neurol. 2016, 15, 391–404. [Google Scholar] [CrossRef] [Green Version]
- Ehrlich, S.; Fassbender, C.M.; Blaes, C.; Finke, C.; Gunther, A.; Harms, L.; Hoffmann, F.; Jahner, K.; Klingel, R.; Kraft, A.; et al. Therapeutic apheresis for autoimmune encephalitis: A nationwide data collection. Nervenarzt 2013, 84, 498–507. [Google Scholar] [CrossRef]
- Magana, S.M.; Keegan, B.M.; Weinshenker, B.G.; Erickson, B.J.; Pittock, S.J.; Lennon, V.A.; Rodriguez, M.; Thomsen, K.; Weigand, S.; Mandrekar, J.; et al. Beneficial plasma exchange response in central nervous system inflammatory demyelination. Arch. Neurol. 2011, 68, 870–878. [Google Scholar] [CrossRef]
- Lindner, M.; Klotz, L.; Wiendl, H. Mechanisms underlying lesion development and lesion distribution in CNS autoimmunity. J. Neurochem. 2018, 146, 122–132. [Google Scholar] [CrossRef]
- Rommer, P.S.; Milo, R.; Han, M.H.; Satyanarayan, S.; Sellner, J.; Hauer, L.; Illes, Z.; Warnke, C.; Laurent, S.; Weber, M.S.; et al. Immunological Aspects of Approved MS Therapeutics. Front. Immunol. 2019, 10, 207–220. [Google Scholar] [CrossRef]
- Harutyunyan, G.; Hauer, L.; Dünser, M.W.; Karamyan, A.; Moser, T.; Pikija, S.; Leitinger, M.; Novak, H.F.; Trinka, E.; Sellner, J. Autoimmune Encephalitis at the Neurological Intensive Care Unit: Etiologies, Reasons for Admission and Survival. Neurocrit. Care. 2017, 27, 82–89. [Google Scholar] [CrossRef]
- Titulaer, M.J.; McCracken, L.; Gabilondo, I.; Armangue, T.; Glaser, C.; Iizuka, T.; Honig, L.S.; Benseler, S.M.; Kawachi, I.; Martinez-Hernandez, E.; et al. Treatment and prognostic factors for long-term outcome in patients with anti-NMDA receptor encephalitis: an observational cohort study. Lancet Neurol. 2013, 12, 157–165. [Google Scholar] [CrossRef] [Green Version]
- Reeves, H.M.; Winters, J.L. The mechanisms of action of plasma exchange. Br. J. Haematol. 2014, 164, 342–351. [Google Scholar] [CrossRef] [PubMed]
- DeSena, A.D.; Noland, D.K.; Matevosyan, K.; King, K.; Phillips, L.; Qureshi, S.S.; Greenberg, B.M.; Graves, D. Intravenous methylprednisolone versus therapeutic plasma exchange for treatment of anti-n-methyl-d-aspartate receptor antibody encephalitis: A retrospective review. J. Clin. Apher. 2015, 30, 212–216. [Google Scholar] [CrossRef] [PubMed]
- Norda, R.; Berséus, O.; Stegmayr, B. Adverse events and problems in therapeutic hemapheresis. A report from the Swedish registry. Transfus. Apher. Sci. 2001, 25, 33–41. [Google Scholar] [CrossRef]
- Kleiter, I.; Gahlen, A.; Borisow, N.; Fischer, K.; Wernecke, K.D.; Hellwig, K.; Florence Pache, K.R.; Pache, F.; Ruprecht, K.; Havla, J.; et al. Apheresis therapies for NMOSD attacks: A retrospective study of 207 therapeutic interventions. Neurol. Neuroimmunol. Neuroinflamm. 2018, 5, e504. [Google Scholar] [CrossRef] [PubMed]
- Lipphardt, M.; Mühlhausen, J.; Kitze, B.; Heigl, F.; Mauch, E.; Helms, H.-J.; Müller, G.A.; Koziolek, M.J. Immunoadsorption or plasma exchange in steroid-refractory multiple sclerosis and neuromyelitis optica. J. Clin. Apher. 2019, 34, 381–391. [Google Scholar] [CrossRef]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S.; et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018, 7, 162–173. [Google Scholar] [CrossRef]
- Weinshenker, B.G.; O’Brien, P.C.; Petterson, T.M.; Noseworthy, J.H.; Lucchinetti, C.F.; Dodick, D.W.; Pineda, A.A.; Stevens, L.N.; Rodriguez, M. A randomized trial of plasma exchange in acute central nervous system inflammatory demyelinating disease. Ann. Neurol. 1999, 46, 878–886. [Google Scholar] [CrossRef]
- Keegan, M.; Pineda, A.A.; McClelland, R.L.; Darby, C.H.; Rodriguez, M.; Weinshenker, B.G. Plasma exchange for severe attacks of CNS demyelination: predictors of response. Neurology 2002, 58, 143–146. [Google Scholar] [CrossRef]
- De Bruijn, M.A.A.M.; van Sonderen, A.; van Coevorden-Hameete, M.H.; Bastiaansen, A.E.M.; Schreurs, M.W.J.; Rouhl, R.P.W.; van Donselaar, C.A.; Majoie, M.H.J.M.; Neuteboom, V.O.R.C.I.D.P.F.; Smitt, P.A.E.S.; et al. Evaluation of seizure treatment in anti-LGI1, anti-NMDAR, and anti-GABA(B)R encephalitis. Neurology 2019, 92, e2185–e2196. [Google Scholar] [CrossRef]
- Jiao, Y.; Cui, L.; Zhang, W.; Zhang, Y.; Wang, W.; Zhang, L.; Tang, W.; Jiao, J. Plasma Exchange for Neuromyelitis Optica Spectrum Disorders in Chinese Patients and Factors Predictive of Short-term Outcome. Clin. Ther. 2018, 40, 603–612. [Google Scholar] [CrossRef]
- Manguinao, M.; Krysko, K.M.; Maddike, S.; Rutatangwa, A.; Francisco, C.; Hart, J.; Chong, J.; Graves, J.S.; Waubant, E. A retrospective cohort study of plasma exchange in central nervous system demyelinating events in children. Mult. Scler. Relat. Disord. 2019, 35, 50–54. [Google Scholar] [CrossRef] [PubMed]
- Llufriu, S.; Castillo, J.; Blanco, Y.; Ramió-Torrentà, L.; Rio, J.; Valles, M.; Lozano, M.; Castellà, M.D.; Calabia, J.; Horga, A.; et al. Plasma exchange for acute attacks of CNS demyelination: Predictors of improvement at 6 months. Neurology 2009, 73, 949–953. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Li, W.; Zhou, S.; Zhou, Y.; Yang, H.; Yu, L.; Wang, J.; Wang, Y.; Zhang, L. Clinical Features, Treatment, and Outcomes Among Chinese Children with Anti-methyl-D-aspartate Receptor (Anti-NMDAR) Encephalitis. Front. Neurol. 2019, 10, 596. [Google Scholar] [CrossRef] [PubMed]
- Harutyunyan, G.; Hauer, L.; Dünser, M.W.; Moser, T.; Pikija, S.; Leitinger, M.; Novak, H.F.; Trinka, E.; Sellner, J. Risk Factors for Intensive Care Unit Admission in Patients with Autoimmune Encephalitis. Front. Immunol. 2017, 28, 835. [Google Scholar] [CrossRef] [PubMed]
- Huda, S.; Whittam, D.; Bhojak, M.; Chamberlain, J.; Noonan, C.; Jacob, A. Neuromyelitis optica spectrum disorders. Clin. Med. 2019, 19, 169–176. [Google Scholar] [CrossRef]
- Kivity, S.; Agmon-Levin, N.; Zandman-Goddard, G.; Chapman, J.; Shoenfeld, Y. Neuropsychiatric lupus: a mosaic of clinical presentations. BMC Med. 2015, 13, 43. [Google Scholar] [CrossRef]
- Chessa, E.; Piga, M.; Floris, A.; Mathieu, A.; Cauli, A. Demyelinating syndrome in SLE: review of different disease subtypes and report of a case series. Reumatismo 2017, 69, 175–183. [Google Scholar] [CrossRef] [Green Version]
- Aguirre-Valencia, D.; Naranjo-Escobar, J.; Posso-Osorio, I.; Macía-Mejía, M.C.; Nieto-Aristizábal, I.; Barrera, T.; Obando, M.A.; Tobón, G.J. Therapeutic Plasma Exchange as Management of Complicated Systemic Lupus Erythematosus and Other Autoimmune Diseases. Autoimmune Dis. 2019, 2019. [Google Scholar] [CrossRef]
- Pons-Estel, G.J.; Salerni, G.E.; Serrano, R.M.; Gómez-Puerta, J.A.; Plasín, M.A.; Aldasoro, E.; Lozano, M.; Cid, J.; Cervera, R.; Espinosa, G. Therapeutic plasma exchange for the management of refractory systemic autoimmune diseases: Report of 31 cases and review of the literature. Autoimmun. Rev. 2011, 10, 679–684. [Google Scholar] [CrossRef]
- Ehler, J.; Blechinger, S.; Rommer, P.S.; Koball, S.; Mitzner, S.; Hartung, H.-P.; Leutmezer, F.; Sauer, M.; Zettl, U.K. Treatment of the First Acute Relapse Following Therapeutic Plasma Exchange in Formerly Glucocorticosteroid-Unresponsive Multiple Sclerosis Patients—A Multicenter Study to Evaluate Glucocorticosteroid Responsiveness. Int. J. Mol. Sci. 2017, 18, 1749. [Google Scholar] [CrossRef]
- Cortese, I.; Cornblath, D.R. Therapeutic plasma exchange in neurology: 2012. J. Clin. Apher. 2013, 28, 16–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faissner, S.; Nikolayczik, J.; Chan, A.; Hellwig, K.; Gold, R.; Yoon, M.-S.; Haghikia, A. Plasmapheresis and immunoadsorption in patients with steroid refractory multiple sclerosis relapses. J. Neurol. 2016, 263, 1092–1098. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| No. | Age | Gender | Indication | GC Refractory | Courses of TPE | Clinical Response |
|---|---|---|---|---|---|---|
| 1 | 42 | M | GC contraindicated | 5 | good | |
| 2 | 37 | F | optic neuritis | X | 5 | good |
| 3 | 39 | F | optic neuritis | X | 5 | good |
| 4 | 44 | F | optic neuritis | X | 5 | good |
| 5 | 25 | F | optic neuritis | X | 5 | mild |
| 6 | 40 | F | optic neuritis | X | 5 | mild |
| 7 | 28 | F | optic neuritis | X | 5 | mild |
| 8 | 28 | M | optic neuritis | X | 5 | mild |
| 9 | 47 | M | optic neuritis | X | 5 | no |
| 10 | 33 | F | optic neuritis | X | 5 | no |
| 11 | 43 | F | tetraparesis | X | 2 | good |
| 12 | 23 | M | tetraplegia | X | 5 | good |
| 13 | 33 | M | hemiparesis, dysarthria | X | 5 | good |
| 14 | 17 | M | hemiparesis | X | 5 | good |
| 15 | 34 | F | tetraparesis | X | 5 | mild |
| 16 | 44 | F | tetraplegia | X | 8 | no |
| 17 | 50 | M | tetrapresis, dysarthia, dysphagia | X | 5 | no |
| 18 | 43 | F | hemiparesis, ataxia | X | 3 | no |
| 19 | 25 | F | fulminant MRI, aphasia | X | 5 | good |
| 20 | 29 | F | fulminant MRI, natalizumab rebound | X | 5 | good |
| 21 | 21 | F | fulminant radiological findings | X | 9 | good |
| n | Age | Gender | Details | Antibody | Memo | Epil | Psych | Move | Auto | Sleep | Pons | Detection of Lesion on MRI | CSF | Treatment | TPE Courses | Clinical Response |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 42 | M | Paraneopl.AE | Ma1/Ma2 | + | + | + | + | temporomesial | neg. | TPE/OP/Ritux | 3 | no | |||
| 2 | 29 | W | NMDAR-E | NMDAR | + | + | + | diffuse | IgG ↑ | TPE/IVIG | 10 | good | ||||
| 3 | 26 | W | NMDAR-E | NMDAR | + | + | none | 33 cells | TPE/IVIG/OP | 5 | good | |||||
| 4 | 30 | W | NMDAR-E | NMDAR | + | + | none | neg. | TPE/IVIG/OP | 5 | good | |||||
| 5 | 25 | F | NMDAR-E | NMDAR | + | + | + | none | 10 cells | TPE/IVIG/GC/OP | 13 | no | ||||
| 6 | 64 | M | LE | LGI-1/VGKC | + | + | + | temporomesial | 9 cells | TPE/IVIG/GC | 5 | mild | ||||
| 7 | 55 | M | LE | none | + | temporomesial | 21 cells | TPE/IVIG | 5 | mild | ||||||
| 8 | 62 | M | LE | AMPA-R1 | + | + | temporomesial | 16 cells | TPE/IVIG/Ritux | 7 | no | |||||
| 9 | 66 | M | LE | LGI-1 | + | + | none | neg. | TPE/ IVIG/ GC | 4 | good | |||||
| 10 | 24 | F | probable LE | none | + | + | + | temperomesial | neg. | TPE/IVIG/GC | 5 | mild | ||||
| 11 | 71 | M | Brainstem E | none | + | pons | neg. | TPE/IVIG | 7 | good | ||||||
| 12 | 47 | M | Brainstem E | none | + | pons | neg. | TPE/IVIG/GC | 6 | mild |
| No. | Age | Gender | Condition | TPE Courses (n) | Outcome |
|---|---|---|---|---|---|
| 1 | 60 | W | CNS-lupus | 4 | no |
| 2 | 55 | W | CNS-lupus | 4 | good |
| 3 | 59 | W | CNS-lupus | 7 | good |
| 4 | 27 | W | optic neuritis | 5 | good |
| 5 | 47 | W | optic neuritis | 10 | mild |
| 6 | 78 | W | NMOSD | 5 | no |
| 7 | 29 | W | ADEM | 5 | good |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moser, T.; Harutyunyan, G.; Karamyan, A.; Otto, F.; Bacher, C.; Chroust, V.; Leitinger, M.; Novak, H.F.; Trinka, E.; Sellner, J. Therapeutic Plasma Exchange in Multiple Sclerosis and Autoimmune Encephalitis: A Comparative Study of Indication, Efficacy, and Safety. Brain Sci. 2019, 9, 267. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci9100267
Moser T, Harutyunyan G, Karamyan A, Otto F, Bacher C, Chroust V, Leitinger M, Novak HF, Trinka E, Sellner J. Therapeutic Plasma Exchange in Multiple Sclerosis and Autoimmune Encephalitis: A Comparative Study of Indication, Efficacy, and Safety. Brain Sciences. 2019; 9(10):267. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci9100267
Chicago/Turabian StyleMoser, Tobias, Gayane Harutyunyan, Anush Karamyan, Ferdinand Otto, Carola Bacher, Vaclav Chroust, Markus Leitinger, Helmut F. Novak, Eugen Trinka, and Johann Sellner. 2019. "Therapeutic Plasma Exchange in Multiple Sclerosis and Autoimmune Encephalitis: A Comparative Study of Indication, Efficacy, and Safety" Brain Sciences 9, no. 10: 267. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci9100267