
Psychiatric Disorders among the Military in West Africa: A Systematic Narrative Review

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
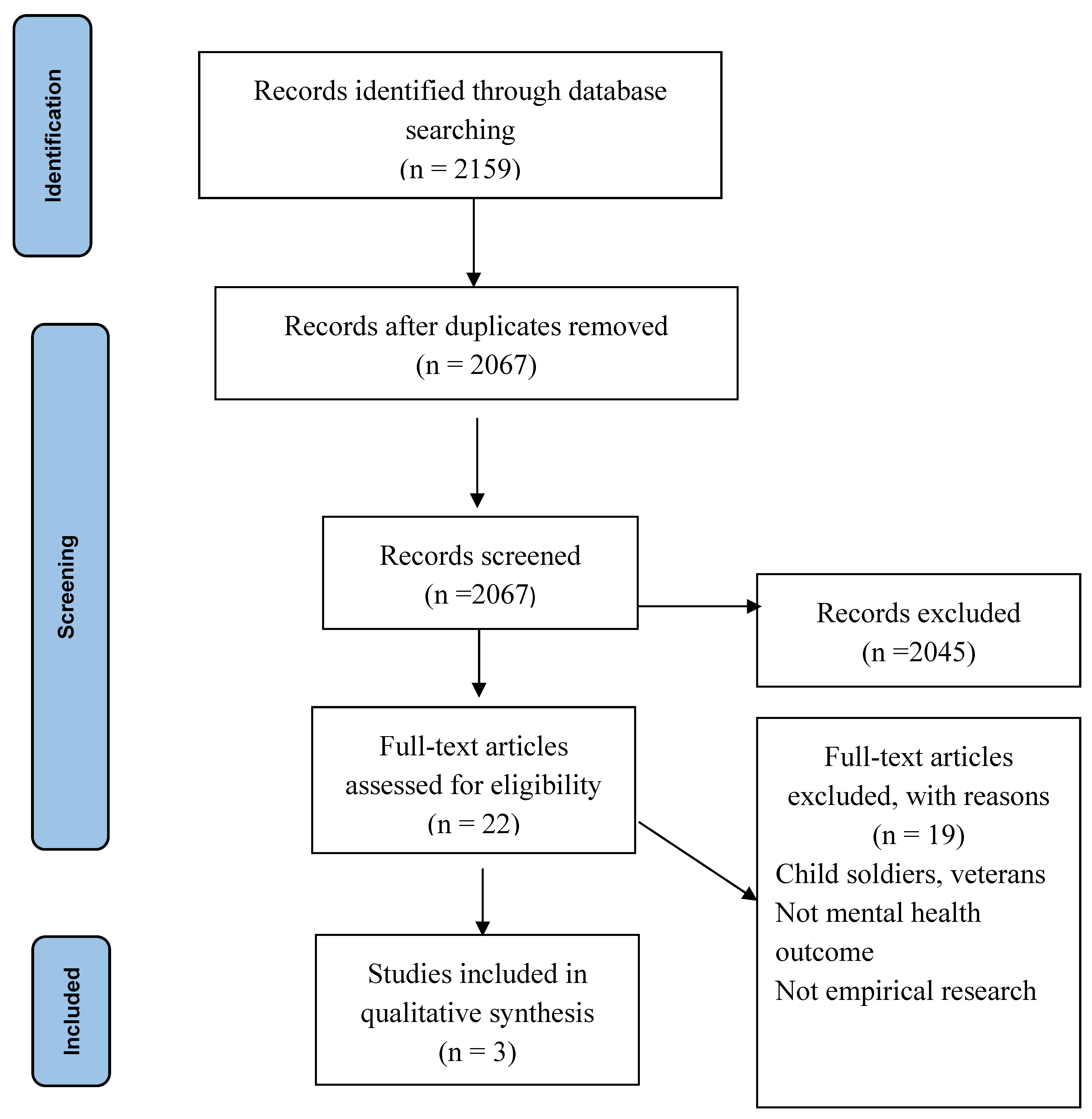
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Risk of Bias
3. Results
3.1. Description of the Included Studies
3.2. Prevalence of Psychiatric Disorders over 12-Month Period
3.3. Prevalence of Lifetime Psychiatric Disorders
4. Discussion
4.1. Limitations and Recommendations
4.2. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McNally, R.J. Psychiatric disorder and suicide in the military, then and now: Commentary on Frueh and Smith. J. Anxiety Disord. 2012, 26, 776–778. [Google Scholar] [CrossRef] [PubMed]
- Ramchand, R.; Rudavsky, R.; Grant, S.; Tanielian, T.; Jaycox, L. Prevalence of, risk factors for, and consequences of posttraumatic stress disorder and other mental health problems in military populations deployed to Iraq and Afghanistan. Curr. Psychiatry Rep. 2015, 17, 37. [Google Scholar] [CrossRef] [PubMed]
- Farmer, C.M.; Vaughan, C.A.; Garnett, J.; Weinick, R.M. Pre-deployment stress, mental health, and help-seeking behaviors among Marines; Rand Corporation: Santa Monica, CA, USA, 2015. [Google Scholar]
- Hoge, C.W.; Terhakopian, A.; Castro, C.A.; Messer, S.C.; Engel, C.C. Association of posttraumatic stress disorder with somatic symptoms, health care visits, and absenteeism among Iraq war veterans. Am. J. Psychiatry 2007, 164, 150–153. [Google Scholar] [CrossRef]
- Ursano, R.J.; Holloway, H.C.; Jones, D.R.; Rodriguez, A.R.; Belenky, G.L. Psychiatric Care in the Military Community: Family and Military Stressors. Psychiatr. Serv. 1989, 40, 1284–1289. [Google Scholar] [CrossRef]
- Beliveau, P.; Boulos, D.; Zamorski, M. Contribution of mental and physical disorders to disability in military personnel. Occup. Med. 2018, 68, 332–339. [Google Scholar] [CrossRef] [Green Version]
- Romero, D.H.; Riggs, S.A.; Raiche, E.; McGuffin, J.; Captari, L.E. Attachment, coping, and psychological symptoms among military veterans and active duty personnel. Anxiety Stress Coping 2020, 33, 326–341. [Google Scholar] [CrossRef] [PubMed]
- Murdoch, M.; Pryor, J.B.; Polusny, M.A.; Gackstetter, G.D. Functioning and Psychiatric Symptoms among Military Men and Women Exposed to Sexual Stressors. Mil. Med. 2007, 172, 718–725. [Google Scholar] [CrossRef] [Green Version]
- Stevelink, S.A.; Malcolm, E.M.; Mason, C.; Jenkins, S.; Sundin, J.; Fear, N.T. The prevalence of mental health disorders in (ex-)military personnel with a physical impairment: A systematic review. Occup. Environ. Med. 2015, 72, 243–251. [Google Scholar] [CrossRef] [Green Version]
- Stimpson, N.J.; Thomas, H.V.; Weightman, A.L.; Dunstan, F.; Lewis, G. Psychiatric disorder in veterans of the Persian Gulf War of 1991 Systematic review. Br. J. Psychiatry 2003, 182, 391–403. [Google Scholar] [CrossRef] [Green Version]
- Buckman, J.E.J.; Sundin, J.; Greene, T.; Fear, N.T.; Dandeker, C.; Greenberg, N.; Wessely, S. The impact of deployment length on the health and well-being of military personnel: A systematic review of the literature. Occup. Environ. Med. 2011, 68, 69. [Google Scholar] [CrossRef]
- Hoge, C.W.; Castro, C.A.; Messer, S.C.; McGurk, D.; Cotting, D.I.; Koffman, R.L. Combat duty in Iraq and Afghanistan, mental health problems, and barriers to care. N. Engl. J. Med. 2004, 351, 13–22. [Google Scholar] [CrossRef] [Green Version]
- Thomas, J.L.; Wilk, J.E.; Riviere, L.A.; McGurk, D.; Castro, C.A.; Hoge, C.W. Prevalence of mental health problems and functional impairment among active component and National Guard soldiers 3 and 12 months following combat in Iraq. Arch. Gen. psychiatry 2010, 67, 614–623. [Google Scholar] [CrossRef] [PubMed]
- Tanielian, T.L.; Tanielian, T.; Jaycox, L. Invisible wounds of war: Psychological and cognitive injuries, their consequences, and services to assist recovery; Rand Corporation: Santa Monica, CA, USA, 2008; Volume 1. [Google Scholar]
- Ramchand, R.; Schell, T.L.; Karney, B.R.; Osilla, K.C.; Burns, R.M.; Caldarone, L.B. Disparate prevalence estimates of PTSD among service members who served in Iraq and Afghanistan: Possible explanations. J. Trauma. Stress 2010, 23, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Whisman, M.A.; Salinger, J.M.; Gilmour, A.L.; Steele, B.A.; Snyder, D.K.J. Love and war: Prospective associations between relationship distress and incidence of psychiatric disorders in active-duty Army personnel. Abnorm. Psychol. 2020, 130, 3–8. [Google Scholar] [CrossRef]
- Brownlow, J.A.; Klingaman, E.A.; Boland, E.M.; Brewster, G.S.; Gehrman, P.R. Psychiatric disorders moderate the relationship between insomnia and cognitive problems in military soldiers. J. Affect. Disord. 2017, 221, 25–30. [Google Scholar] [CrossRef]
- United Nations. Situation in West Africa, Sahel ‘Extremely Volatile’ as Terrorists Exploit Ethnic Animosities, Special Representative Warns Security Council. Available online: https://www.un.org/press/en/2020/sc14245.doc.htm (accessed on August 2021).
- Dalton, M. The US Should Send More, Not Fewer, Troops to West Africa. 2020. Available online: https://www.defenseone.com/ideas/2020/03/us-should-send-more-not-fewer-troops-west-africa/163479/ (accessed on July 2021).
- The World Bank. Fragile and conflict affected situations: World Bank Group. Available online: https://data.worldbank.org/region/fragile-and-conflict-affected-situations (accessed on 20 September 2021).
- Gardner, F. West Africa’s Islamist Insurgency: Fight at a Critical Stage. Available online: https://www.bbc.com/news/world-africa-57324672 (accessed on July 2021).
- Martinez, L. Pentagon to decide soon on possible troop cut in West Africa. Available online: https://abcnews.go.com/Politics/pentagon-decide-troop-cut-west-africa/story?id=68342094 (accessed on July 2021).
- Adler, A.B.; Kim, P.; Thomas, S.; Sipos, M. Quarantine and the US military response to the Ebola crisis: Soldier health and attitudes. Public Health 2018, 155, 95–98. [Google Scholar] [CrossRef] [PubMed]
- Sipos, M.L.; Kim, P.Y.; Thomas, S.J.; Adler, A.B. US service member deployment in response to the ebola crisis: The psychological perspective. Mil. Med. 2018, 183, 171–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baethge, C.; Goldbeck-Wood, S.; Mertens, S. SANRA—A scale for the quality assessment of narrative review articles. Res. Integr. peer Rev. 2019, 4, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hancock, D.R.; Algozzine, B. Doing Case Study Research: A Practical Guide for Beginning Researchers; Teachers College Press: New York, NY, USA, 2017. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6. [Google Scholar] [CrossRef] [Green Version]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetcu, R.; Currie, M.; Qureshi, R.; Mattis, P.; Lisy, K.; et al. Chapter 7: Systematic reviews of etiology and risk. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Adelaide, South Australia, 2020. [Google Scholar]
- Lasebikan, V.O.; Ijomanta, I.N. Lifetime and 12 months cannabis use and disorders among soldiers residing in a military community in Nigeria. J. Subst. Use 2018, 23, 67–73. [Google Scholar] [CrossRef]
- Ijomanta, I.N.; Lasebikan, V.O. Lifetime and 12 Months Prevalence of Alcohol Use and Alcohol Use Disorders Among Soldiers Residing in a Military Community in Ibadan. Subst. Use Misuse 2016, 51, 722–732. [Google Scholar] [CrossRef]
- Lasebikan, V.O.; Ijomanta, I. Non-medical prescription opioid use and opioid use disorder in the military population in Nigeria. J. Subst. Use 2019, 24, 192–198. [Google Scholar] [CrossRef]
- Kelsall, H.L.; Wijesinghe, M.S.; Creamer, M.C.; McKenzie, D.P.; Forbes, A.B.; Page, M.J.; Sim, M.R. Alcohol use and substance use disorders in Gulf War, Afghanistan, and Iraq War veterans compared with non-deployed military personnel. Epidemiol. Rev. 2015, 37, 38–54. [Google Scholar] [CrossRef] [PubMed]
- Waller, M.; McGuire, A.C.L.; Dobson, A.J. Alcohol use in the military: Associations with health and wellbeing. Subst. Abus. Treat. Prev. Policy 2015, 10, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williamson, V.; Stevelink, S.A.M.; Greenberg, K.; Greenberg, N. Prevalence of Mental Health Disorders in Elderly U.S. Military Veterans: A Meta-Analysis and Systematic Review. Am. J. Geriatr. Psychiatry 2018, 26, 534–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Genevieive, A.; Cunradi, C. Alcohol Use and Preventing Alcohol-Related Problems Among Young Adults in the Military. Available online: https://pubs.niaaa.nih.gov/publications/arh284/252-257.htm (accessed on September 2021).
- Armed Forces. Relinquishment of legislative juridiction, minimum drinking age on military institutions. Available online: https://www.law.cornell.edu/uscode/text/10/2683 (accessed on September 2021).
- WHO. World Health Organization’s Composite International Diagnostic Interview. Available online: https://www.hcp.med.harvard.edu/wmhcidi/ (accessed on September 2021).
- Trautmann, S.; Goodwin, L.; Höfler, M.; Jacobi, F.; Strehle, J.; Zimmermann, P.; Wittchen, H.U. Prevalence and severity of mental disorders in military personnel: A standardised comparison with civilians. Epidemiol. Psychiatr. Sci. 2017, 26, 199–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fear, N.T.; Iversen, A.; Meltzer, H.; Workman, L.; Hull, L.; Greenberg, N.; Barker, C.; Browne, T.; Earnshaw, M.; Horn, O.; et al. Patterns of drinking in the UK Armed Forces. Addiction 2007, 102, 1749–1759. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author | Study Aim | Country | Method | Study Design | Sample Size | Risk of Bias | Key Finding |
|---|---|---|---|---|---|---|---|
| Lasebikan, V. O. and Ijomanta, I. N. (2018) | To determine the prevalence of both lifetime and 12 months and cannabis use disorder and their correlates among a military population. | Nigeria | A multi-stage stratified systematic sampling method was used to sample participants. | Descriptive cross-sectional study | 223 | Low | Higher lifetime prevalence of cannabis use; 12-month cannabis use was entirely confined to men; cannabis use was associated with past disciplinary action in the workplace. |
| Lasebikan, V. O. and Ijomanta, I. N. (2019) | To ascertain 12-month prevalence of non-medically prescribed opioid use and non-medically prescribed opioid use disorder among military population. | Nigeria | A multi-stage stratified systematic sampling method was used to sample participants. | Descriptive cross-sectional study | 223 | Low | The 12-month prevalence of non-medical prescription opioid use was 6.7% and non-medical prescription opioid use disorder, 3.6%. Non-medical prescription opioid use was more common among those who ever got injured during combat. Of the participants who had a combat injury, 8% had lifetime use of prescription opioids and developed either abuse or dependence. |
| Ijomanta, I. N. and Lasebikan, V. O. (2016) | To establish the lifetime and 12 months prevalence of alcohol use and alcohol use disorders as well as the profile of problems associated with the diagnoses of alcohol use disorders among a military population. | Nigeria | A multi-stage stratified systematic sampling method was used to sample participants. | Descriptive cross-sectional study | 223 | Low | Prevalence of lifetime alcohol use was 76%, 12 months prevalence was 54%, and frequent binge drinking was reported in 7% of respondents. Alcohol use is more highly prevalent among the military personnel than the general population. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Asare-Doku, W.; Donnir, G.M.; Ayuurebobi Ae-Ngibise, K.; Peprah, J.; Awuviry-Newton, K.; Acquah, F. Psychiatric Disorders among the Military in West Africa: A Systematic Narrative Review. Behav. Sci. 2021, 11, 138. https://0-doi-org.brum.beds.ac.uk/10.3390/bs11100138
Asare-Doku W, Donnir GM, Ayuurebobi Ae-Ngibise K, Peprah J, Awuviry-Newton K, Acquah F. Psychiatric Disorders among the Military in West Africa: A Systematic Narrative Review. Behavioral Sciences. 2021; 11(10):138. https://0-doi-org.brum.beds.ac.uk/10.3390/bs11100138
Chicago/Turabian StyleAsare-Doku, Winifred, Gordon Maanianu Donnir, Kenneth Ayuurebobi Ae-Ngibise, Jennifer Peprah, Kofi Awuviry-Newton, and Francis Acquah. 2021. "Psychiatric Disorders among the Military in West Africa: A Systematic Narrative Review" Behavioral Sciences 11, no. 10: 138. https://0-doi-org.brum.beds.ac.uk/10.3390/bs11100138