Exercise Intervention Improves Clinical Outcomes, but the “Time of Session” is Crucial for Better Quality of Life in Breast Cancer Survivors: A Systematic Review and Meta-Analysis


 ,
, 


Abstract
:1. Introduction
2. Results
2.1. Search Results and the Selection of Studies
2.2. Summary of the Included Studies
2.3. Patient-Reported Clinical Outcomes and Scales
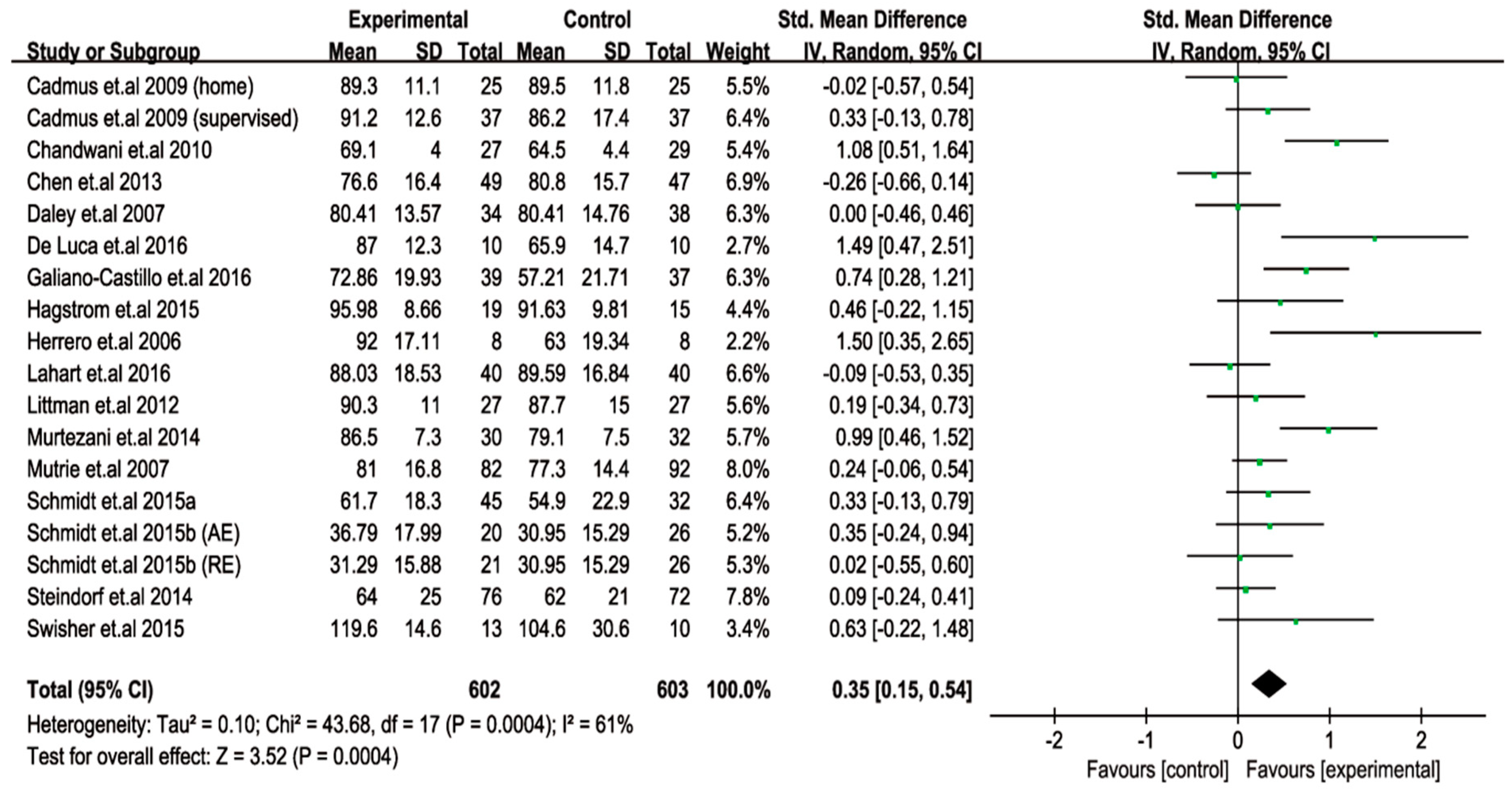
2.4. Exercise Intervention Improves the QoL in Breast Cancer Survivors
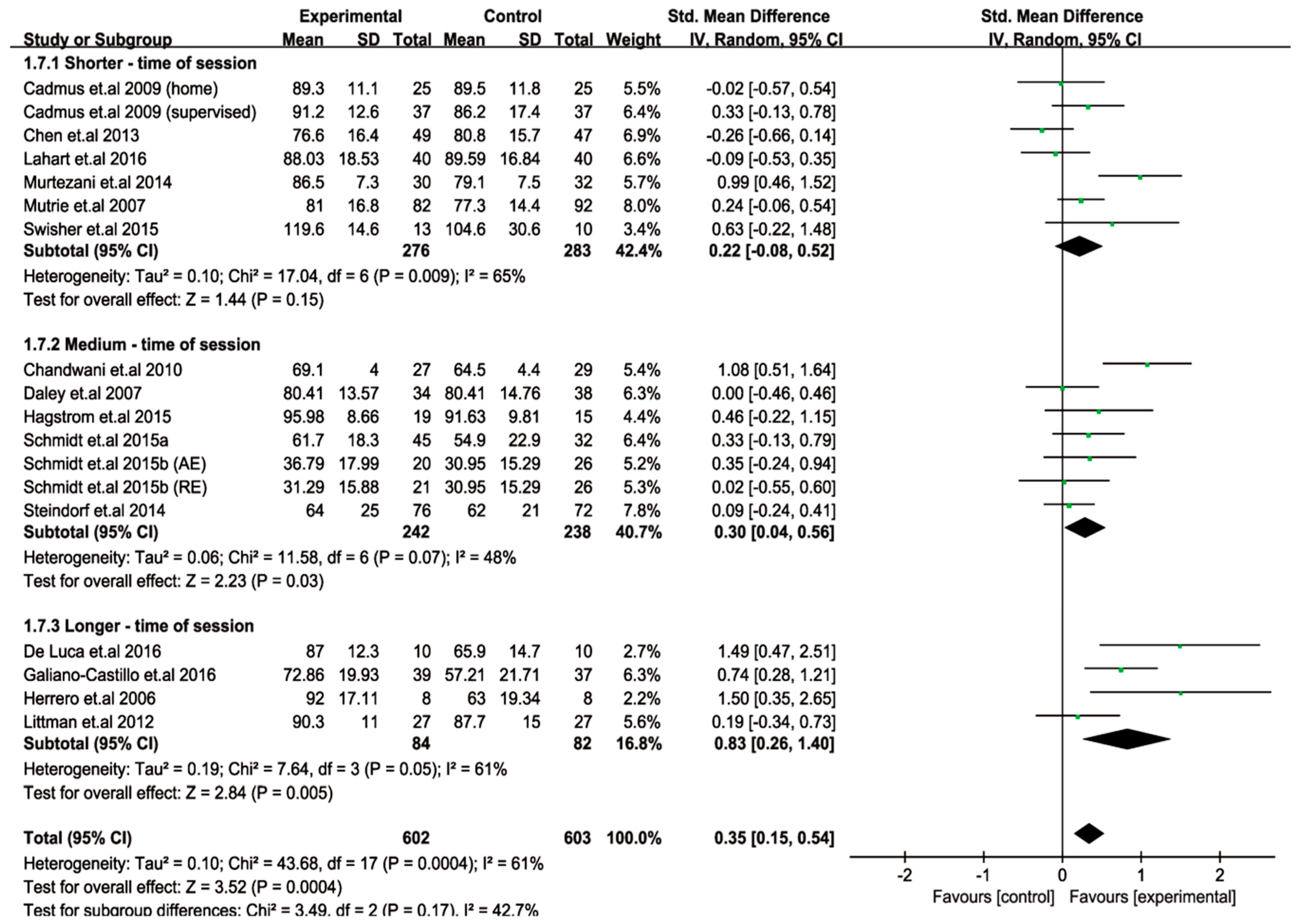
2.5. Longer Time of Session Profoundly Improves the QoL in Women with Breast Cancer
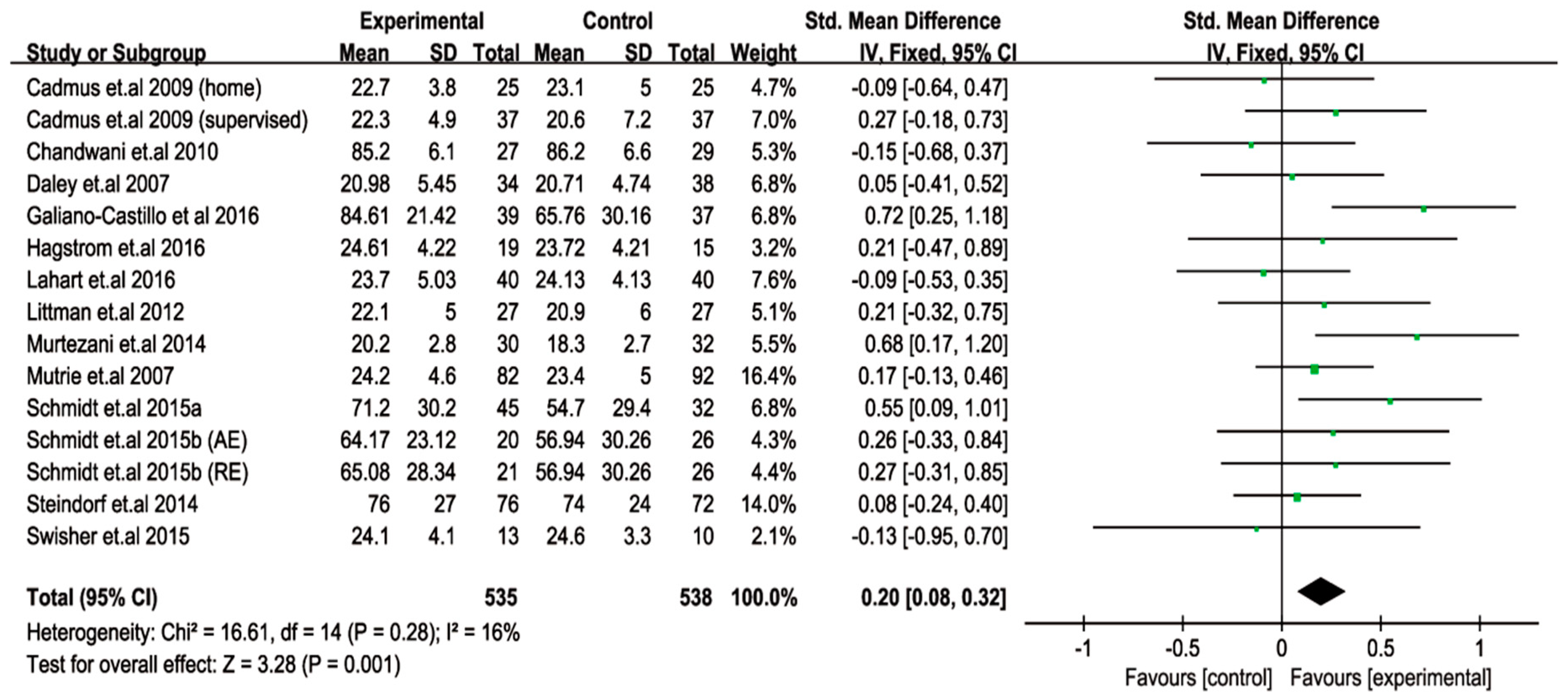
2.6. Beneficial Effects of Exercise on SF amongst Breast Cancer Survivors
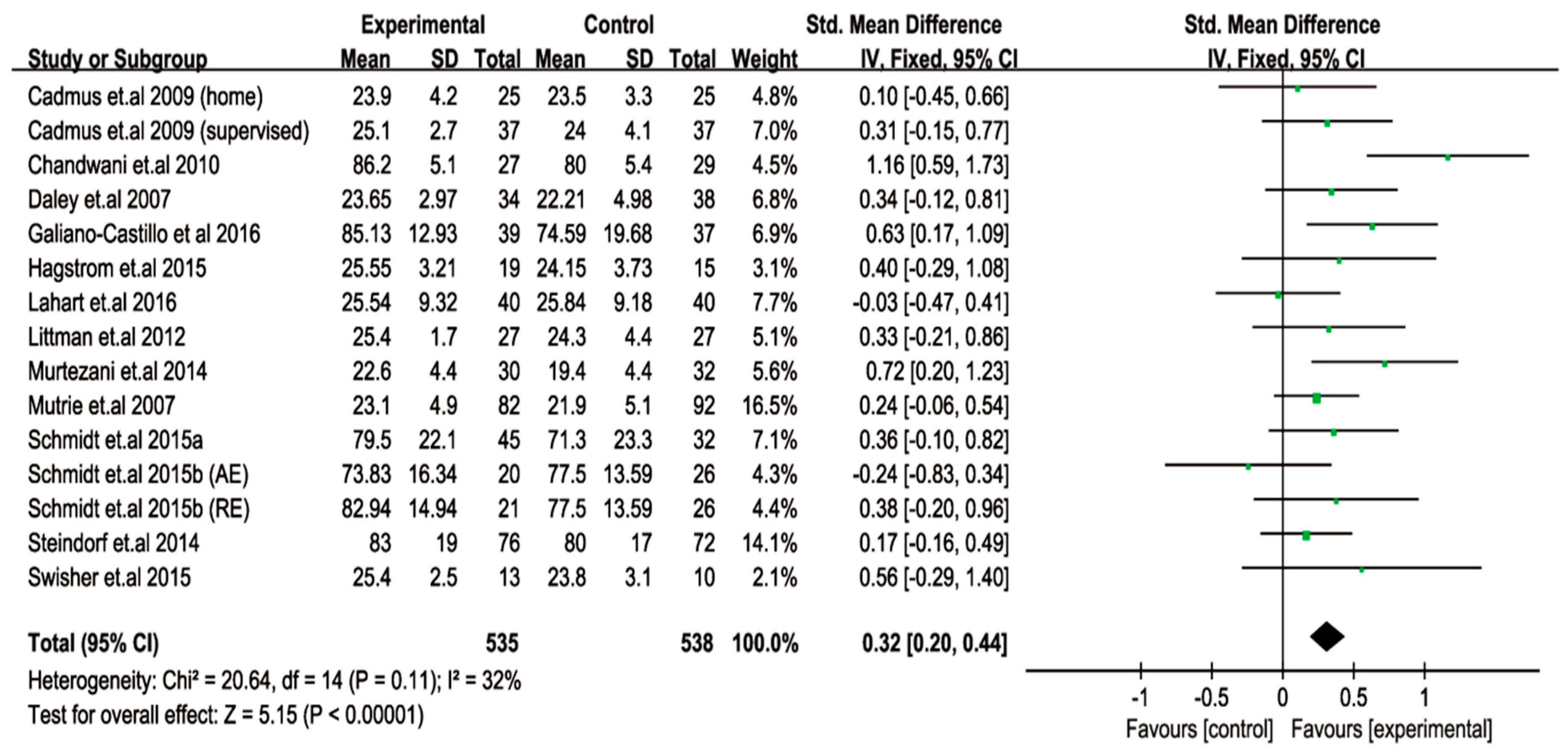
2.7. Beneficial Effects of Exercise on PF amongst Breast Cancer Survivors
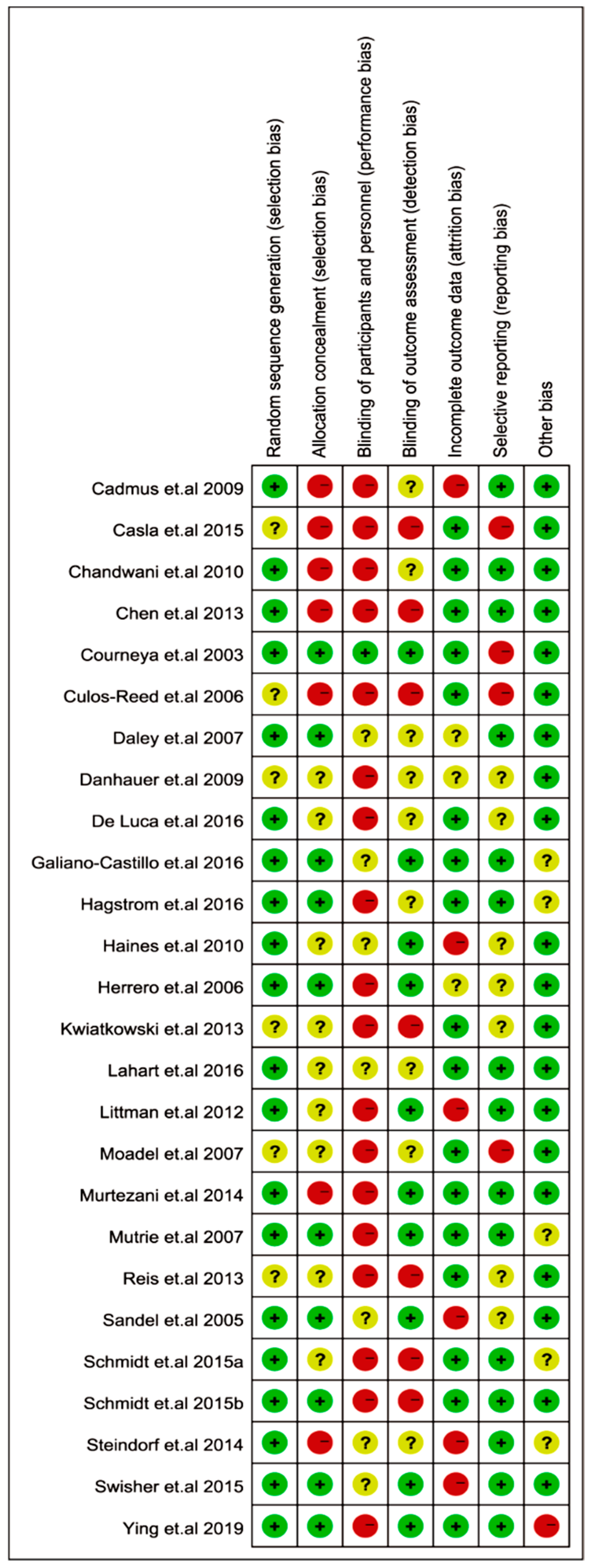
2.8. Risk of Bias of Included Studies
3. Discussion
Significance of Exercise Intervention, Scales, and the Included Trials
4. Materials and Methods
4.1. Search Strategy and the Identification of Studies
4.2. Selection Criteria
4.3. Quality Assessment
4.4. Data Extraction
4.5. Outcome Measures
4.6. Subgroup Division and Analysis
4.7. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hortobagyi, G.N.; de la Garza Salazar, J.; Pritchard, K.; Amadori, D.; Haidinger, R.; Hudis, C.A.; Khaled, H.; Liu, M.C.; Martin, M.; Namer, M.; et al. The global breast cancer burden: Variations in epidemiology and survival. Clin. Breast Cancer 2005, 6, 391–401. [Google Scholar] [CrossRef] [PubMed]
- ACS. American Cancer Society. Breast Cancer Facts & Figures 2017–2018; American Cancer Society, Inc.: Atlanta, GA, USA, 2017. [Google Scholar]
- Allemani, C.; Matsuda, T.; Di Carlo, V.; Harewood, R.; Matz, M.; Nikšić, M.; Bonaventure, A.; Valkov, M.; Johnson, C.J.; Estève, J. Global surveillance of trends in cancer survival 2000–14 (CONCORD-3): Analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet 2018, 391, 1023–1075. [Google Scholar] [CrossRef]
- Sehl, M.; Lu, X.; Silliman, R.; Ganz, P.A. Decline in physical functioning in first 2 years after breast cancer diagnosis predicts 10-year survival in older women. J. Cancer Surviv. 2013, 7, 20–31. [Google Scholar] [CrossRef] [PubMed]
- Noal, S.; Levy, C.; Hardouin, A.; Rieux, C.; Heutte, N.; Segura, C.; Collet, F.; Allouache, D.; Switsers, O.; Delcambre, C.; et al. One-year longitudinal study of fatigue, cognitive functions, and quality of life after adjuvant radiotherapy for breast cancer. Int. J. Radiat. Oncol. Biol. Phys. 2011, 81, 795–803. [Google Scholar] [CrossRef]
- Zhang, X.; Li, Y.; Liu, D. Effects of exercise on the quality of life in breast cancer patients: A systematic review of randomized controlled trials. Support. Care Cancer 2019, 27, 9–21. [Google Scholar] [CrossRef] [PubMed]
- Sweegers, M.G.; Altenburg, T.M.; Chinapaw, M.J.; Kalter, J.; Verdonck-de Leeuw, I.M.; Courneya, K.S.; Newton, R.U.; Aaronson, N.K.; Jacobsen, P.B.; Brug, J.; et al. Which exercise prescriptions improve quality of life and physical function in patients with cancer during and following treatment? A systematic review and meta-analysis of randomised controlled trials. Br. J. Sports Med. 2018, 52, 505–513. [Google Scholar] [CrossRef] [PubMed]
- Schmitz, K.H.; Courneya, K.S.; Matthews, C.; Demark-Wahnefried, W.; Galvao, D.A.; Pinto, B.M.; Irwin, M.L.; Wolin, K.Y.; Segal, R.J.; Lucia, A.; et al. American College of Sports Medicine roundtable on exercise guidelines for cancer survivors. Med. Sci. Sports Exerc. 2010, 42, 1409–1426. [Google Scholar] [CrossRef]
- Saarto, T.; Penttinen, H.M.; Sievänen, H.; Kellokumpu-Lehtinen, P.L.; Hakamies-Blomqvist, L.; Nikander, R.; Huovinen, R.; Luoto, R.; Kautiainen, H.; Järvenpää, S.; et al. Effectiveness of a 12-month exercise program on physical performance and quality of life of breast cancer survivors. Anticancer Res. 2012, 32, 3875–3884. [Google Scholar]
- Ergun, M.; Eyigor, S.; Karaca, B.; Kisim, A.; Uslu, R. Effects of exercise on angiogenesis and apoptosis-related molecules, quality of life, fatigue and depression in breast cancer patients. Eur. J. Cancer Care (Engl.) 2013, 22, 626–637. [Google Scholar] [CrossRef]
- Adams, S.C.; Segal, R.J.; McKenzie, D.C.; Vallerand, J.R.; Morielli, A.R.; Mackey, J.R.; Gelmon, K.; Friedenreich, C.M.; Reid, R.D.; Courneya, K.S. Impact of resistance and aerobic exercise on sarcopenia and dynapenia in breast cancer patients receiving adjuvant chemotherapy: A multicenter randomized controlled trial. Breast Cancer Res. Treat. 2016, 158, 497–507. [Google Scholar] [CrossRef] [PubMed]
- Kilbreath, S.L.; Refshauge, K.M.; Beith, J.M.; Ward, L.C.; Lee, M.; Simpson, J.M.; Hansen, R. Upper limb progressive resistance training and stretching exercises following surgery for early breast cancer: A randomized controlled trial. Breast Cancer Res. Treat. 2012, 133, 667–676. [Google Scholar] [CrossRef] [PubMed]
- Courneya, K.S.; McKenzie, D.C.; Mackey, J.R.; Gelmon, K.; Friedenreich, C.M.; Yasui, Y.; Reid, R.D.; Cook, D.; Jespersen, D.; Proulx, C.; et al. Effects of exercise dose and type during breast cancer chemotherapy: Multicenter randomized trial. J. Natl. Cancer Inst. 2013, 105, 1821–1832. [Google Scholar] [CrossRef] [PubMed]
- Gerritsen, J.K.W.; Vincent, A.J.P.E. Exercise improves quality of life in patients with cancer: A systematic review and meta-analysis of randomised controlled trials. Br. J. Sports Med. 2016, 50, 796–803. [Google Scholar] [CrossRef] [PubMed]
- Buffart, L.M.; Kalter, J.; Sweegers, M.G.; Courneya, K.S.; Newton, R.U.; Aaronson, N.K.; Jacobsen, P.B.; May, A.M.; Galvao, D.A.; Chinapaw, M.J.; et al. Effects and moderators of exercise on quality of life and physical function in patients with cancer: An individual patient data meta-analysis of 34 RCTs. Cancer Treat. Rev. 2017, 52, 91–104. [Google Scholar] [CrossRef]
- Lipsett, A.; Barrett, S.; Haruna, F.; Mustian, K.; O’Donovan, A. The impact of exercise during adjuvant radiotherapy for breast cancer on fatigue and quality of life: A systematic review and meta-analysis. Breast 2017, 32, 144–155. [Google Scholar] [CrossRef]
- Haines, T.P.; Sinnamon, P.; Wetzig, N.G.; Lehman, M.; Walpole, E.; Pratt, T.; Smith, A. Multimodal exercise improves quality of life of women being treated for breast cancer, but at what cost? Randomized trial with economic evaluation. Breast Cancer Res. Treat. 2010, 124, 163–175. [Google Scholar] [CrossRef]
- Danhauer, S.C.; Mihalko, S.L.; Russell, G.B.; Campbell, C.R.; Felder, L.; Daley, K.; Levine, E.A. Restorative yoga for women with breast cancer: Findings from a randomized pilot study. Psychooncology 2009, 18, 360–368. [Google Scholar] [CrossRef]
- Moadel, A.B.; Shah, C.; Wylie-Rosett, J.; Harris, M.S.; Patel, S.R.; Hall, C.B.; Sparano, J.A. Randomized controlled trial of yoga among a multiethnic sample of breast cancer patients: Effects on quality of life. J. Clin. Oncol. 2007, 25, 4387–4395. [Google Scholar] [CrossRef]
- Culos-Reed, S.N.; Carlson, L.E.; Daroux, L.M.; Hately-Aldous, S. A pilot study of yoga for breast cancer survivors: Physical and psychological benefits. Psychooncology 2006, 15, 891–897. [Google Scholar] [CrossRef]
- Casla, S.; Lopez-Tarruella, S.; Jerez, Y.; Marquez-Rodas, I.; Galvao, D.A.; Newton, R.U.; Cubedo, R.; Calvo, I.; Sampedro, J.; Barakat, R.; et al. Supervised physical exercise improves VO2max, quality of life, and health in early stage breast cancer patients: A randomized controlled trial. Breast Cancer Res. Treat. 2015, 153, 371–382. [Google Scholar] [CrossRef] [PubMed]
- Kwiatkowski, F.; Mouret-Reynier, M.A.; Duclos, M.; Leger-Enreille, A.; Bridon, F.; Hahn, T.; Van Praagh-Doreau, I.; Travade, A.; Gironde, M.; Bezy, O.; et al. Long term improved quality of life by a 2-week group physical and educational intervention shortly after breast cancer chemotherapy completion. Results of the ‘Programme of Accompanying women after breast Cancer treatment completion in Thermal resorts’ (PACThe) randomised clinical trial of 251 patients. Eur. J. Cancer 2013, 49, 1530–1538. [Google Scholar] [CrossRef]
- Sandel, S.L.; Judge, J.O.; Landry, N.; Faria, L.; Ouellette, R.; Majczak, M. Dance and movement program improves quality-of-life measures in breast cancer survivors. Cancer Nurs. 2005, 28, 301–309. [Google Scholar] [CrossRef] [PubMed]
- Courneya, K.S.; Mackey, J.R.; Bell, G.J.; Jones, L.W.; Field, C.J.; Fairey, A.S. Randomized controlled trial of exercise training in postmenopausal breast cancer survivors: Cardiopulmonary and quality of life outcomes. J. Clin. Oncol. 2003, 21, 1660–1668. [Google Scholar] [CrossRef]
- Ying, W.; Min, Q.W.; Lei, T.; Na, Z.X.; Li, L.; Jing, L. The health effects of Baduanjin exercise (a type of Qigong exercise) in breast cancer survivors: A randomized, controlled, single-blinded trial. Eur. J. Oncol. Nurs. 2019, 39, 90–97. [Google Scholar] [CrossRef] [PubMed]
- Reis, D.; Walsh, M.E.; Young-McCaughan, S.; Jones, T. Effects of Nia exercise in women receiving radiation therapy for breast cancer. Oncol. Nurs. Forum 2013, 40, E374–381. [Google Scholar] [CrossRef] [PubMed]
- Cadmus, L.A.; Salovey, P.; Yu, H.; Chung, G.; Kasl, S.; Irwin, M.L. Exercise and quality of life during and after treatment for breast cancer: Results of two randomized controlled trials. Psychooncology 2009, 18, 343–352. [Google Scholar] [CrossRef] [PubMed]
- Daley, A.J.; Crank, H.; Saxton, J.M.; Mutrie, N.; Coleman, R.; Roalfe, A. Randomized trial of exercise therapy in women treated for breast cancer. J. Clin. Oncol. 2007, 25, 1713–1721. [Google Scholar] [CrossRef] [PubMed]
- Murtezani, A.; Ibraimi, Z.; Bakalli, A.; Krasniqi, S.; Disha, E.D.; Kurtishi, I. The effect of aerobic exercise on quality of life among breast cancer survivors: A randomized controlled trial. J. Cancer Res. Ther. 2014, 10, 658–664. [Google Scholar] [CrossRef]
- Swisher, A.K.; Abraham, J.; Bonner, D.; Gilleland, D.; Hobbs, G.; Kurian, S.; Yanosik, M.A.; Vona-Davis, L. Exercise and dietary advice intervention for survivors of triple-negative breast cancer: Effects on body fat, physical function, quality of life, and adipokine profile. Support. Care Cancer 2015, 23, 2995–3003. [Google Scholar] [CrossRef]
- Lahart, I.M.; Metsios, G.S.; Nevill, A.M.; Kitas, G.D.; Carmichael, A.R. Randomised controlled trial of a home-based physical activity intervention in breast cancer survivors. BMC Cancer 2016, 16. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, T.; Weisser, B.; Duerkop, J.; Jonat, W.; Van Mackelenbergh, M.; Roecken, C.; Mundhenke, C. Comparing endurance and resistance training with standard care during chemotherapy for patients with primary breast cancer. Anticancer Res. 2015, 35, 5623–5629. [Google Scholar]
- Schmidt, M.E.; Wiskemann, J.; Armbrust, P.; Schneeweiss, A.; Ulrich, C.M.; Steindorf, K. Effects of resistance exercise on fatigue and quality of life in breast cancer patients undergoing adjuvant chemotherapy: A randomized controlled trial. Int. J. Cancer 2015, 137, 471–480. [Google Scholar] [CrossRef] [PubMed]
- Steindorf, K.; Schmidt, M.E.; Klassen, O.; Ulrich, C.M.; Oelmann, J.; Habermann, N.; Beckhove, P.; Owen, R.; Debus, J.; Wiskemann, J.; et al. Randomized, controlled trial of resistance training in breast cancer patients receiving adjuvant radiotherapy: Results on cancer-related fatigue and quality of life. Ann. Oncol. 2014, 25, 2237–2243. [Google Scholar] [CrossRef]
- Hagstrom, A.D.; Marshall, P.W.M.; Lonsdale, C.; Cheema, B.S.; Fiatarone Singh, M.A.; Green, S. Resistance training improves fatigue and quality of life in previously sedentary breast cancer survivors: A randomised controlled trial. Eur. J. Cancer Care (Engl.) 2016, 25, 784–794. [Google Scholar] [CrossRef]
- De Luca, V.; Minganti, C.; Borrione, P.; Grazioli, E.; Cerulli, C.; Guerra, E.; Bonifacino, A.; Parisi, A. Effects of concurrent aerobic and strength training on breast cancer survivors: A pilot study. Public Health 2016, 136, 126–132. [Google Scholar] [CrossRef]
- Galiano-Castillo, N.; Cantarero-Villanueva, I.; Fernandez-Lao, C.; Ariza-Garcia, A.; Diaz-Rodriguez, L.; Del-Moral-Avila, R.; Arroyo-Morales, M. Telehealth system: A randomized controlled trial evaluating the impact of an internet-based exercise intervention on quality of life, pain, muscle strength, and fatigue in breast cancer survivors. Cancer 2016, 122, 3166–3174. [Google Scholar] [CrossRef]
- Herrero, F.; San Juan, A.F.; Fleck, S.J.; Balmer, J.; Perez, M.; Canete, S.; Earnest, C.P.; Foster, C.; Lucia, A. Combined aerobic and resistance training in breast cancer survivors: A randomized, controlled pilot trial. Int. J. Sports Med. 2006, 27, 573–580. [Google Scholar] [CrossRef]
- Mutrie, N.; Campbell, A.M.; Whyte, F.; McConnachie, A.; Emslie, C.; Lee, L.; Kearney, N.; Walker, A.; Ritchie, D. Benefits of supervised group exercise programme for women being treated for early stage breast cancer: Pragmatic randomised controlled trial. BMJ 2007, 334, 517. [Google Scholar] [CrossRef] [PubMed]
- Chandwani, K.D.; Thornton, B.; Perkins, G.H.; Arun, B.; Raghuram, N.V.; Nagendra, H.R.; Wei, Q.; Cohen, L. Yoga improves quality of life and benefit finding in women undergoing radiotherapy for breast cancer. J. Soc. Integr. Oncol. 2010, 8, 43–55. [Google Scholar] [PubMed]
- Littman, A.J.; Bertram, L.C.; Ceballos, R.; Ulrich, C.M.; Ramaprasad, J.; McGregor, B.; McTiernan, A. Randomized controlled pilot trial of yoga in overweight and obese breast cancer survivors: Effects on quality of life and anthropometric measures. Support. Care Cancer 2012, 20, 267–277. [Google Scholar] [CrossRef]
- Chen, Z.; Meng, Z.; Milbury, K.; Bei, W.; Zhang, Y.; Thornton, B.; Liao, Z.; Wei, Q.; Chen, J.; Guo, X.; et al. Qigong improves quality of life in women undergoing radiotherapy for breast cancer: Results of a randomized controlled trial. Cancer. 2013, 119, 1690–1698. [Google Scholar] [CrossRef]
- Liu, Y.; Ye, W.; Chen, Q.; Zhang, Y.; Kuo, C.H.; Korivi, M. Resistance exercise intensity is correlated with attenuation of HbA1c and insulin in patients with type 2 diabetes: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health. 2019, 16, 140. [Google Scholar] [CrossRef]
- Yousuf Zafar, S. Financial toxicity of cancer care: It’s time to intervene. J. Natl. Cancer Inst. 2015, 108. [Google Scholar] [CrossRef]
- Silva, D.A.S.; Tremblay, M.S.; Souza, M.d.F.M.d.; Guerra, M.R.; Mooney, M.; Naghavi, M.; Malta, D.C. Mortality and years of life lost due to breast cancer attributable to physical inactivity in the Brazilian female population (1990–2015). Sci. Rep. 2018, 8, 11141. [Google Scholar] [CrossRef]
- Wen, C.P.; Wai, J.P.M.; Tsai, M.K.; Yang, Y.C.; Cheng, T.Y.D.; Lee, M.-C.; Chan, H.T.; Tsao, C.K.; Tsai, S.P.; Wu, X. Minimum amount of physical activity for reduced mortality and extended life expectancy: A prospective cohort study. Lancet 2011, 378, 1244–1253. [Google Scholar] [CrossRef]
- Cramer, H.; Rabsilber, S.; Lauche, R.; Kümmel, S.; Dobos, G. Yoga and meditation for menopausal symptoms in breast cancer survivors—A randomized controlled trial. Cancer 2015, 121, 2175–2184. [Google Scholar] [CrossRef]
- Watson, T.; Mock, V. Exercise as an intervention for cancer-related fatigue. Phys. Ther. 2004, 84, 736–743. [Google Scholar] [CrossRef]
- Felce, D.; Perry, J. Quality of life: Its definition and measurement. Res. Dev. Disabil. 1995, 16, 51–74. [Google Scholar] [CrossRef]
- Zhu, G.; Zhang, X.; Wang, Y.; Xiong, H.; Zhao, Y.; Sun, F. Effects of exercise intervention in breast cancer survivors: A meta-analysis of 33 randomized controlled trails. Onco. Targets Ther. 2016, 9, 2153–2168. [Google Scholar] [CrossRef]
- Arends, J.; Bachmann, P.; Baracos, V.; Barthelemy, N.; Bertz, H.; Bozzetti, F.; Fearon, K.; Hutterer, E.; Isenring, E.; Kaasa, S.; et al. ESPEN guidelines on nutrition in cancer patients. Clin. Nutr. 2017, 36, 11–48. [Google Scholar] [CrossRef]
- Cheville, A.L.; Troxel, A.B.; Basford, J.R.; Kornblith, A.B. Prevalence and treatment patterns of physical impairments in patients with metastatic breast cancer. J. Clin. Oncol. 2008, 26, 2621–2629. [Google Scholar] [CrossRef]
- Costa, D.S.; Mercieca-Bebber, R.; Rutherford, C.; Gabb, L.; King, M.T. The Impact of cancer on psychological and social outcomes. Aust. Psychol. 2016, 51, 89–99. [Google Scholar] [CrossRef]
- Floyd, A.; Moyer, A. Group versus individual exercise interventions for women with breast cancer: A meta-analysis. Health Psychol. Rev. 2010, 4, 22–41. [Google Scholar] [CrossRef] [PubMed]
- Duijts, S.F.; Faber, M.M.; Oldenburg, H.S.; van Beurden, M.; Aaronson, N.K. Effectiveness of behavioral techniques and physical exercise on psychosocial functioning and health-related quality of life in breast cancer patients and survivors-a meta-analysis. Psychooncology 2011, 20, 115–126. [Google Scholar] [CrossRef]
- Juvet, L.; Thune, I.; Elvsaas, I.Ø.; Fors, E.; Lundgren, S.; Bertheussen, G.; Leivseth, G.; Oldervoll, L. The effect of exercise on fatigue and physical functioning in breast cancer patients during and after treatment and at 6 months follow-up: A meta-analysis. Breast 2017, 33, 166–177. [Google Scholar] [CrossRef]
- White, S.M.; Wójcicki, T.R.; Mcauley, E. Physical activity and quality of life in community dwelling older adults. Health Qual. Life Outcomes 2009, 7. [Google Scholar] [CrossRef]
- Hamilton, D.; Giesinger, J.; Giesinger, K. It is merely subjective opinion that patient-reported outcome measures are not objective tools. Bone Jt. Res. 2017, 6, 665–666. [Google Scholar] [CrossRef]
- Atkinson, T.M.; Stover, A.M.; Storfer, D.F.; Saracino, R.M.; D’Agostino, T.A.; Pergolizzi, D.; Matsoukas, K.; Li, Y.; Basch, E. Patient-reported physical function measures in cancer clinical trials. Epidemiol. Rev. 2017, 39, 59–70. [Google Scholar] [CrossRef] [PubMed]
- Brazier, J.E.; Harper, R.; Jones, N.; O’cathain, A.; Thomas, K.; Usherwood, T.; Westlake, L. Validating the SF-36 health survey questionnaire: New outcome measure for primary care. BMJ 1992, 305, 160–164. [Google Scholar] [CrossRef] [PubMed]
- Overcash, J.; Extermann, M.; Parr, J.; Perry, J.; Balducci, L. Validity and reliability of the FACT-G scale for use in the older person with cancer. Am. J. Clin. Oncol. 2001, 24, 591–596. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions; Version 5.1.0 [updated March 2011]; The Cochrane Collaboration, 2011; Available online: http://handbook-5-1.cochrane.org/ (accessed on 3 December 2018).
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; Filiberti, A.; Flechtner, H.; Fleishman, S.B.; de Haes, J.C. The European Organization for Research and Treatment of Cancer QLQ-C30: A quality-of-life instrument for use in international clinical trials in oncology. J. Natl. Cancer Inst. 1993, 85, 365–376. [Google Scholar] [CrossRef] [PubMed]
- Schag, A.C.; Ganz, P.A.; Heinrich, R.L. Cancer rehabilitation evaluation system-short form (CARES-SF). A cancer specific rehabilitation and quality of life instrument. Cancer 1991, 68, 1406–1413. [Google Scholar] [CrossRef]
- Hahn, E.A.; Segawa, E.; Kaiser, K.; Cella, D.; Smith, B.D. Validation of the functional assessment of cancer therapy-breast (FACT-B) quality of life instrument. J. Clin. Concol. 2015, 33. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Country | Age (Years) | Sample (n) | Cancer Stage | Exercise Type | Time of Session (min) | Frequency (t/wk) | Duration (Weeks) | Outcome | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Exercise | Control | Exercise | Control | ||||||||
| Ying et al. 2019 [26] | China | 1n: <40 36n: 40–60 9n >60 | 2n:< 40 28n: 40–60 10n: >60 | 46 | 40 | Ⅰ–Ⅲ | Qigong | S:60, H:20 | 7 | 26 | QoL, PWB, S/FWB |
| De Luca et al. 2016 [37] | Italy | 50.2 ± 9.7 | 46.0 ± 2.8 | 10 | 10 | Ⅰ–Ⅲ | AE + RE | 90 | 2 | 24 | QoL |
| Galiano-Castillo et al. 2016 [38] | Spain | 47.4 ± 9.6 | 49.2 ± 7.9 | 39 | 37 | Ⅰ–Ⅲ | AE + RE | 90 | 3 | 8 | QoL, PF, SF |
| Hagstrom et al. 2016 [36] | Australia | 51.2 ± 8.5 | 52.7 ± 9.4 | 19 | 15 | Ⅰ–Ⅲ | RE | 60 | 3 | 16 | QoL, PWB, S/FWB |
| Lahart et al. 2016 [32] | England | 52.4 ± 10.3 | 54.7 ± 8.3 | 40 | 40 | Ⅰ–Ⅲ | AE | 30 | 3–7 | 26 | QoL, PWB, S/FWB |
| Casla et al. 2015 [22] | Spain | 45.91 ± 8.21 | 51.87 ± 8.21 | 44 | 45 | Ⅰ–Ⅲ | AE + RE | (nr) | 2 | 12 | QoL |
| Schmidt et al. 2015a [34] | Germany | 52.2 ± 9.9 | 53.3 ± 10.2 | 45 | 32 | Ⅰ–Ⅲ | RE | 60 | 2 | 12 | QoL, PF, SF |
| Schmidt et al. 2015b [33] | Germany | AE:56 ± 10.15 RE:53 ± 12.55 | 54 ± 11.19 | AE:20 RE:21 | 26 | (nr) | AE RE | 60 | 2 | 12 | QoL, PF, SF |
| Swisher et al. 2015 [31] | United States | 43–65 | 36–71 | 13 | 10 | Ⅰ–Ⅲ | AE | 30 | 5 | 12 | QoL, PWB, S/FWB |
| Murtezani et al. 2014 [30] | Kosovo | 53 ± 11 | 51 ± 11 | 30 | 32 | Ⅰ–Ⅲ | AE | 25–45 | 3 | 10 | QoL, PWB, S/FWB |
| Steindorf et al. 2014 [35] | Germany | 55.2 ± 9.5 | 56.4 ± 8.7 | 76 | 72 | 0–Ⅲ | RE | 60 | 2 | 12 | QoL, PF, SF |
| Chen et al. 2013 [43] | China | 45.3 ± 6.3 | 44.7 ± 9.7 | 49 | 47 | 0–Ⅲ | Qigong | 40 | 5 | 6 | QoL |
| Kwiatkowski et al. 2013 [23] | France | 51.8 ± 8.7 | 52.3 ± 10.1 | 113 | 107 | (nr) | AE + RE | (nr) | 7 | 2 | QoL, PF, SF |
| Reis et al. 2013 [27] | United States | 54 ± 11.1 | 59 ± 10.7 | 12 | 17 | (nr) | AE | 20–60 | 3 | 12 | QoL, PWB, S/FWB |
| Littman et al. 2012 [42] | United States | 60.6 ± 7.1 | 58.2 ± 8.8 | 27 | 27 | 0–Ⅲ | Yoga | 75 | 5 | 26 | QoL, PWB, S/FWB |
| Chandwani et al. 2010 [41] | United States | 51.39 ± 7.97 | 40.2 ± 9.96 | 27 | 29 | 0–Ⅲ | Yoga | 60 | 3 | 12 | QoL, PF, SF |
| Haines et al. 2010 [18] | Australia | 55.9 ± 10.5 | 59.5 ± 13.3 | 33 | 32 | (nr) | AE + RE | (nr) | (nr) | 24 | QoL, PF, SF |
| Cadmus et al. 2009 [28] | United States | H:54.5 ± 8.2 S:56.5 ± 9.5 | H:54 ± 10.9 S:55 ± 7.7 | H:25 S:37 | H:25 S:37 | 0–Ⅲ | AE | 30 | 5 | 26 | QoL, PWB, S/FWB |
| Danhauer et al. 2009 [19] | United States | 54.3 ± 9.6 | 57.2 ± 10.2 | 13 | 14 | Ⅰ–Ⅳ | Yoga | 70 | (nr) | 10 | QoL, PWB, S/FWB |
| Daley et al. 2007 [29] | England | 51.6 ± 8.8 | 51.1 ± 8.6 | 34 | 38 | (nr) | AE | 50 | 3 | 8 | QoL, PWB, S/FWB |
| Moadel et al. 2007 [20] | United States | 55.11 ± 10.07 | 54.23 ± 9.8 | 45 | 26 | Ⅰ–Ⅲ | Yoga | (nr) | (nr) | 12 | QoL, PWB, S/FWB |
| Mutrie et al. 2007 [40] | England | 51.3 ± 10.3 | 51.8 ± 8.7 | 82 | 92 | (nr) | AE + RE | 45 | 3 | 12 | QoL, PWB, S/FWB |
| Culos-Reed et al. 2006 [21] | Canada | 51.18 ± 10.33 | 18 | 18 | (nr) | Yoga | 75 | (nr) | 7 | QoL | |
| Herrero et al. 2006 [39] | Spain | 50 ± 5 | 51 ± 10 | 8 | 8 | Ⅰ–Ⅱ | AE + RE | 90 | 3 | 8 | QoL |
| Sandel et al. 2005 [24] | United States | 59.7 ± 9.8 | 59.5 ± 13.3 | 19 | 19 | (nr) | AE | (nr) | 1–2 | 12 | QoL |
| Courneya et al. 2003 [25] | Canada | 59 ± 5 | 58 ± 6 | 24 | 28 | Ⅰ–Ⅲ | AE | (nr) | 3 | 12 | QoL, PWB, S/FWB |
| Exercise Characteristics | Coefficient | Standard Error | T Value | p-Value |
|---|---|---|---|---|
| Type of exercise | −0.3471926 | 0.3498219 | −0.99 | 0.339 |
| Time of session | 0.0121459 | 0.0054789 | 2.22 | 0.041 * |
| Frequency | −0.1384031 | 0.0839449 | −1.65 | 0.119 |
| Duration | −0.006877 | 0.0171193 | −0.40 | 0.693 |
| Total time of exercise | −0.0000111 | 0.0000583 | −0.19 | 0.851 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hong, F.; Ye, W.; Kuo, C.-H.; Zhang, Y.; Qian, Y.; Korivi, M. Exercise Intervention Improves Clinical Outcomes, but the “Time of Session” is Crucial for Better Quality of Life in Breast Cancer Survivors: A Systematic Review and Meta-Analysis. Cancers 2019, 11, 706. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11050706
Hong F, Ye W, Kuo C-H, Zhang Y, Qian Y, Korivi M. Exercise Intervention Improves Clinical Outcomes, but the “Time of Session” is Crucial for Better Quality of Life in Breast Cancer Survivors: A Systematic Review and Meta-Analysis. Cancers. 2019; 11(5):706. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11050706
Chicago/Turabian StyleHong, Feng, Weibing Ye, Chia-Hua Kuo, Yong Zhang, Yongdong Qian, and Mallikarjuna Korivi. 2019. "Exercise Intervention Improves Clinical Outcomes, but the “Time of Session” is Crucial for Better Quality of Life in Breast Cancer Survivors: A Systematic Review and Meta-Analysis" Cancers 11, no. 5: 706. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11050706