Genomic and Transcriptomic Characteristics According to Size of Papillary Thyroid Microcarcinoma

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
2.1. Genomic Characteristics of PTMC Compared to PTC over 1 cm
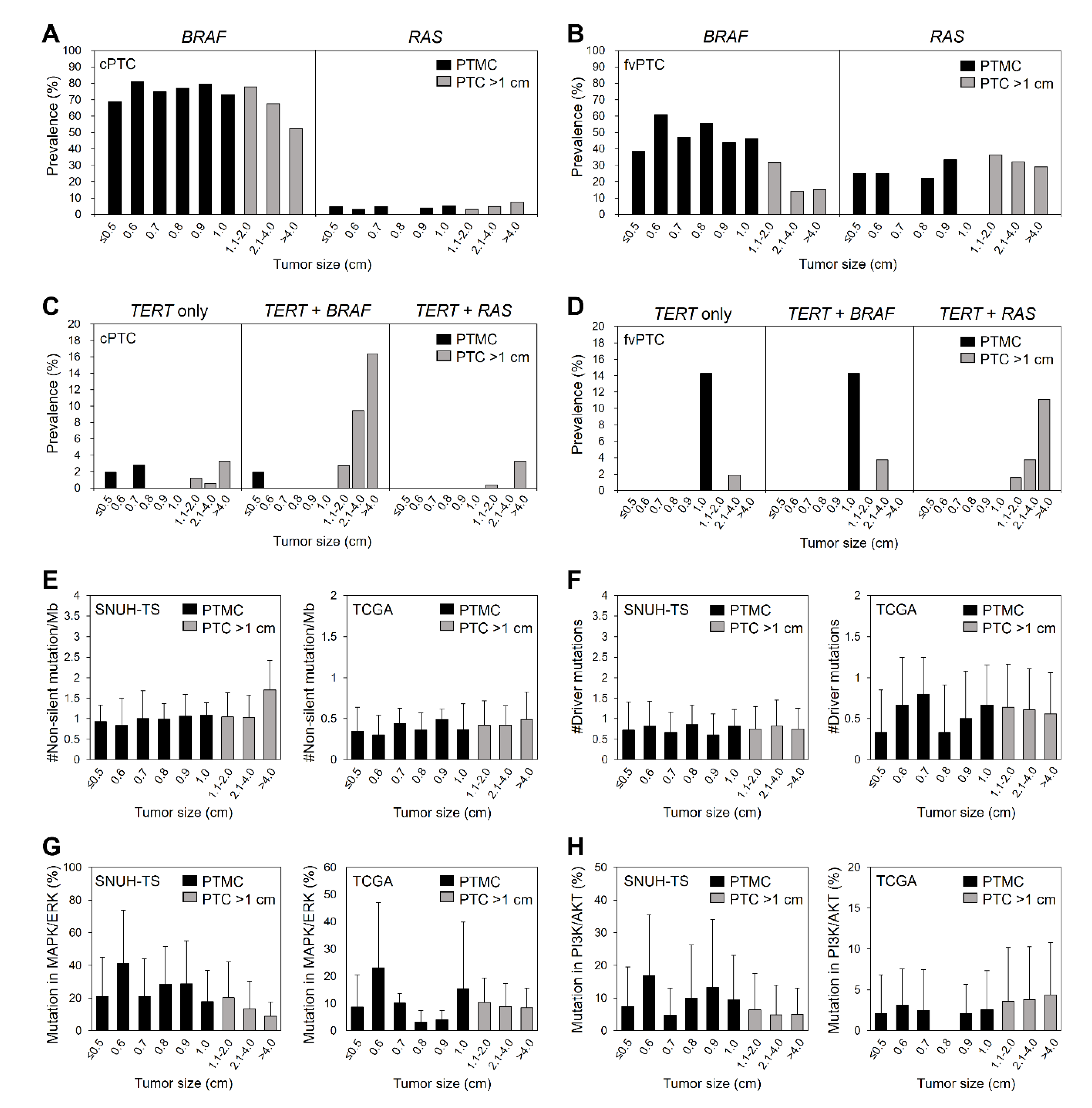
2.2. Genomic Characteristics of PTC According to Tumor Size
2.3. Transcriptomic Characteristics of PTMC
3. Discussion
4. Materials and Methods
4.1. Patients and Tissue Samples
4.2. Library Preparation and Sequencing
4.3. Sequence Data Analysis
4.4. Gene Expression Profiling, Differentially Expressed Gene Analysis, and Gene Scoring
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Mazzaferri, E.L. Management of low-risk differentiated thyroid cancer. Endocr. Pract. 2007, 13, 498–512. [Google Scholar] [CrossRef] [PubMed]
- Ito, Y.; Miyauchi, A.; Kihara, M.; Higashiyama, T.; Kobayashi, K.; Miya, A. Patient age is significantly related to the progression of papillary microcarcinoma of the thyroid under observation. Thyroid 2014, 24, 27–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef] [Green Version]
- Roti, E.; degli Uberti, E.C.; Bondanelli, M.; Braverman, L.E. Thyroid papillary microcarcinoma: A descriptive and meta-analysis study. Eur. J. Endocrinol. 2008, 159, 659–673. [Google Scholar] [CrossRef] [Green Version]
- Mehanna, H.; Al-Maqbili, T.; Carter, B.; Martin, E.; Campain, N.; Watkinson, J.; McCabe, C.; Boelaert, K.; Franklyn, J.A. Differences in the recurrence and mortality outcomes rates of incidental and nonincidental papillary thyroid microcarcinoma: A systematic review and meta-analysis of 21 329 person-years of follow-up. J. Clin. Endocrinol. Metab. 2014, 99, 2834–2843. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.S.; Lim, H.; Chang, H.S.; Park, C.S. Papillary thyroid microcarcinomas are different from latent papillary thyroid carcinomas at autopsy. J. Korean Med. Sci 2014, 29, 676–679. [Google Scholar] [CrossRef] [Green Version]
- Park, Y.J.; Kim, Y.A.; Lee, Y.J.; Kim, S.H.; Park, S.Y.; Kim, K.W.; Chung, J.K.; Youn, Y.K.; Kim, K.H.; Park, D.J.; et al. Papillary microcarcinoma in comparison with larger papillary thyroid carcinoma in BRAF(V600E) mutation, clinicopathological features, and immunohistochemical findings. Head Neck 2010, 32, 38–45. [Google Scholar] [CrossRef]
- Rodrigues, A.C.; Penna, G.; Rodrigues, E.; Castro, P.; Sobrinho-Simoes, M.; Soares, P. The Genetics of Papillary Microcarcinomas of the Thyroid: Diagnostic and Prognostic Implications. Curr. Genom. 2017, 18, 244–254. [Google Scholar] [CrossRef] [Green Version]
- Song, Y.S.; Lim, J.A.; Choi, H.; Won, J.K.; Moon, J.H.; Cho, S.W.; Lee, K.E.; Park, Y.J.; Yi, K.H.; Park, D.J.; et al. Prognostic effects of TERT promoter mutations are enhanced by coexistence with BRAF or RAS mutations and strengthen the risk prediction by the ATA or TNM staging system in differentiated thyroid cancer patients. Cancer 2016, 122, 1370–1379. [Google Scholar] [CrossRef]
- Song, Y.S.; Park, Y.J. Genomic Characterization of Differentiated Thyroid Carcinoma. Endocrinol. Metab. (Seoul) 2019, 34, 1–10. [Google Scholar] [CrossRef]
- Perera, D.; Ghossein, R.; Camacho, N.; Senbabaoglu, Y.; Seshan, V.; Li, J.; Bouvier, N.; Boucai, L.; Viale, A.; Socci, N.D.; et al. Genomic and Transcriptomic Characterization of Papillary Microcarcinomas With Lateral Neck Lymph Node Metastases. J. Clin. Endocrinol. Metab. 2019, 104, 4889–4899. [Google Scholar] [CrossRef]
- Bradley, N.L.; Wiseman, S.M. Papillary thyroid microcarcinoma: The significance of high risk features. BMC Cancer 2017, 17, 142. [Google Scholar] [CrossRef] [Green Version]
- Hong, A.R.; Lim, J.A.; Kim, T.H.; Choi, H.S.; Yoo, W.S.; Min, H.S.; Won, J.K.; Lee, K.E.; Jung, K.C.; Park, D.J.; et al. The Frequency and Clinical Implications of the BRAF(V600E) Mutation in Papillary Thyroid Cancer Patients in Korea Over the Past Two Decades. Endocrinol. Metab. (Seoul) 2014, 29, 505–513. [Google Scholar] [CrossRef] [Green Version]
- Yoo, S.K.; Lee, S.; Kim, S.J.; Jee, H.G.; Kim, B.A.; Cho, H.; Song, Y.S.; Cho, S.W.; Won, J.K.; Shin, J.Y.; et al. Comprehensive Analysis of the Transcriptional and Mutational Landscape of Follicular and Papillary Thyroid Cancers. PLoS Genet. 2016, 12, e1006239. [Google Scholar] [CrossRef]
- Cancer Genome Atlas Research Network. Integrated genomic characterization of papillary thyroid carcinoma. Cell 2014, 159, 676–690. [Google Scholar] [CrossRef]
- Yoo, S.K.; Song, Y.S.; Lee, E.K.; Hwang, J.; Kim, H.H.; Jung, G.; Kim, Y.A.; Kim, S.J.; Cho, S.W.; Won, J.K.; et al. Integrative analysis of genomic and transcriptomic characteristics associated with progression of aggressive thyroid cancer. Nat. Commun. 2019, 10, 2764. [Google Scholar] [CrossRef] [Green Version]
- Nicolson, N.G.; Murtha, T.D.; Dong, W.; Paulsson, J.O.; Choi, J.; Barbieri, A.L.; Brown, T.C.; Kunstman, J.W.; Larsson, C.; Prasad, M.L.; et al. Comprehensive Genetic Analysis of Follicular Thyroid Carcinoma Predicts Prognosis Independent of Histology. J. Clin. Endocrinol. Metab. 2018, 103, 2640–2650. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.Y.; Park, W.Y.; Lee, K.E.; Park, W.S.; Chung, Y.S.; Cho, S.J.; Youn, Y.K. Comparative analysis of gene expression profiles of papillary thyroid microcarcinoma and papillary thyroid carcinoma. J. Cancer Res. Ther 2010, 6, 452–457. [Google Scholar] [CrossRef]
- Sugitani, I.; Fujimoto, Y. Symptomatic versus asymptomatic papillary thyroid microcarcinoma: A retrospective analysis of surgical outcome and prognostic factors. Endocr. J. 1999, 46, 209–216. [Google Scholar] [CrossRef] [Green Version]
- Barbaro, D.; Simi, U.; Meucci, G.; Lapi, P.; Orsini, P.; Pasquini, C. Thyroid papillary cancers: Microcarcinoma and carcinoma, incidental cancers and non-incidental cancers-are they different diseases? Clin. Endocrinol. (Oxf) 2005, 63, 577–581. [Google Scholar] [CrossRef]
- Song, Y.S.; Won, J.K.; Yoo, S.K.; Jung, K.C.; Kim, M.J.; Kim, S.J.; Cho, S.W.; Lee, K.E.; Yi, K.H.; Seo, J.S.; et al. Comprehensive Transcriptomic and Genomic Profiling of Subtypes of Follicular Variant of Papillary Thyroid Carcinoma. Thyroid 2018, 28, 1468–1478. [Google Scholar] [CrossRef]
- Moon, J.H.; Kim, J.H.; Lee, E.K.; Lee, K.E.; Kong, S.H.; Kim, Y.K.; Jung, W.J.; Lee, C.Y.; Yoo, R.E.; Hwangbo, Y.; et al. Study Protocol of Multicenter Prospective Cohort Study of Active Surveillance on Papillary Thyroid Microcarcinoma (MAeSTro). Endocrinol. Metab. (Seoul) 2018, 33, 278–286. [Google Scholar] [CrossRef]
- Brito, J.P.; Ito, Y.; Miyauchi, A.; Tuttle, R.M. A Clinical Framework to Facilitate Risk Stratification When Considering an Active Surveillance Alternative to Immediate Biopsy and Surgery in Papillary Microcarcinoma. Thyroid 2016, 26, 144–149. [Google Scholar] [CrossRef] [Green Version]
- Edge, S.; Byrd, D.R.; Compton, C.C.; Fritz, A.G.; Greene, F.; Trotti, A. (Eds.) AJCC Cancer Staging Manual, 7th ed.; Springer: New York, NY, USA, 2010. [Google Scholar]
- DeLellis, R.A.; Lloyd, R.V.; Heitz, P.U.; Eng, C. World Health Organization Classification of Tumours. Pathology And Genetics Of Tumors Of Endocrine Organs, 3rd ed.; IARC Press: Lyon, France, 2004. [Google Scholar]
- Li, H.; Durbin, R. Fast and accurate long-read alignment with Burrows-Wheeler transform. Bioinformatics 2010, 26, 589–595. [Google Scholar] [CrossRef] [Green Version]
- McKenna, A.; Hanna, M.; Banks, E.; Sivachenko, A.; Cibulskis, K.; Kernytsky, A.; Garimella, K.; Altshuler, D.; Gabriel, S.; Daly, M.; et al. The Genome Analysis Toolkit: A MapReduce framework for analyzing next-generation DNA sequencing data. Genome Res. 2010, 20, 1297–1303. [Google Scholar] [CrossRef] [Green Version]
- Cibulskis, K.; Lawrence, M.S.; Carter, S.L.; Sivachenko, A.; Jaffe, D.; Sougnez, C.; Gabriel, S.; Meyerson, M.; Lander, E.S.; Getz, G. Sensitive detection of somatic point mutations in impure and heterogeneous cancer samples. Nat. Biotechnol. 2013, 31, 213–219. [Google Scholar] [CrossRef]
- Kumar, P.; Henikoff, S.; Ng, P.C. Predicting the effects of coding non-synonymous variants on protein function using the SIFT algorithm. Nat. Protoc. 2009, 4, 1073–1081. [Google Scholar] [CrossRef]
- Adzhubei, I.A.; Schmidt, S.; Peshkin, L.; Ramensky, V.E.; Gerasimova, A.; Bork, P.; Kondrashov, A.S.; Sunyaev, S.R. A method and server for predicting damaging missense mutations. Nat. Methods 2010, 7, 248–249. [Google Scholar] [CrossRef] [Green Version]
- Tate, J.G.; Bamford, S.; Jubb, H.C.; Sondka, Z.; Beare, D.M.; Bindal, N.; Boutselakis, H.; Cole, C.G.; Creatore, C.; Dawson, E.; et al. COSMIC: The Catalogue Of Somatic Mutations In Cancer. Nucleic Acids Res. 2019, 47, D941–D947. [Google Scholar] [CrossRef] [Green Version]
- Love, M.I.; Huber, W.; Anders, S. Moderated estimation of fold change and dispersion for RNA-seq data with DESeq2. Genome Biol. 2014, 15, 550. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | PTMC | PTC > 1 cm | p |
|---|---|---|---|
| No. of patients | 1985 | 1450 | |
| Age, mean ± SD | 47.6 ± 11.5 | 47.6 ± 14.6 | 0.994 |
| Male sex, n (%) | 332/1985 (16.7) | 314/1450 (21.7) | <0.001 |
| Tumor size, cm, median | 0.6 (0.5–0.8) | 1.7 (1.3–2.5) | <0.001 |
| PTC subtype, n (%) | <0.001 | ||
| Classical | 1828/1964 (93.1) | 1126/1417 (79.5) | |
| Follicular-variant | 113/1964 (5.8) | 229/1417 (16.2) | |
| Extrathyroidal extension, n (%) | 1003/1964 (51.1) | 882/1445 (61.0) | <0.001 |
| Minimal | 951/1964 (48.4) | 656/1445 (45.4) | <0.001 |
| Gross | 52/1964 (2.6) | 226/1445 (15.6) | |
| LN metastasis, n (%) | 514/1980 (26.0) | 690/1391 (49.6) | <0.001 |
| Major mutation, n (%) | |||
| BRAFV600E | 1438/1985 (72.4) | 941/1450 (64.9) | <0.001 |
| RAS | 16/309 (5.2) | 84/844 (10.0) | 0.011 |
| TERT | 5/266 (1.9) | 61/712 (8.6) | <0.001 |
| Other drivers, n (%) 1 | 6/93 (6.5) 2; 14/39 (35.9) 3 | 8/128 (6.3) 2; 127/457 (27.8) 3 | 0.952 2; 0.281 3 |
| No driver, n (%) | 28/93 (30.1) 2; 4/39 (10.3) 3 | 39/128 (30.5) 2; 60/457 (13.1) 3 | 0.954 2; 0.607 3 |
| TMB, mean ± SD | 0.97 ± 0.48 2; 0.38 ± 0.26 3 | 1.06 ± 0.59 2; 0.44 ± 0.28 3 | 0.262 2; 0.272 3 |
| No. of driver mutations, mean ± SD | 0.75 ± 0.54 2; 0.59 ± 0.50 3 | 0.77 ± 0.57 2; 0.61 ± 0.51 3 | 0.865 2; 0.846 3 |
| Characteristics | ≤0.5 cm | 0.6–0.7 cm | 0.8–1.0 cm | 1.1–2.0 cm | 2.1–4.0 cm | >4.0 cm | p1 | p2 |
|---|---|---|---|---|---|---|---|---|
| No. of patients | 752 | 580 | 653 | 906 | 410 | 134 | ||
| Age, mean ± SD | 47.3 ± 11.4 | 47.8 ± 11.6 | 47.7 ± 11.6 | 48.3 ± 13.5 | 44.9 ± 15.8 | 50.4 ± 17.0 | 0.401 | 0.983 |
| Male sex, n (%) | 117 (15.6) | 94 (16.2) | 121 (18.5) | 172 (19.0) | 93 (22.7) | 49 (36.6) | 0.282 | <0.001 |
| PTC subtype, n (%) | <0.001 | <0.001 | ||||||
| Classical | 712/748 (95.6) | 535/577 (92.7) | 581/642 (90.5) | 737/887 (83.1) | 301/398 (75.6) | 88/132 (66.7) | ||
| Follicular variant | 26/748 (3.5) | 40/577 (6.9) | 47/642 (7.3) | 118/887 (13.3) | 78/398 (19.6) | 33/132 (25.0) | ||
| Extrathyroidal extension, n (%) | 247/735 (33.6) | 319/578 (55.2) | 437/651 (67.1) | 612/903 (67.8) | 207/409 (50.6) | 63/133 (47.4) | <0.001 | <0.001 |
| Minimal | 239/735 (32.5) | 306/578 (52.9) | 406/651 (62.4) | 464/903 (51.4) | 147/409 (35.9) | 45/133 (33.8) | <0.001 | <0.001 |
| Gross | 8/735 (1.1) | 13/578 (2.2) | 31/651 (4.8) | 148/903 (16.4) | 60/409 (14.7) | 18/133 (13.5) | ||
| LN metastasis, n (%) | 126/750 (16.8) | 175/578 (30.3) | 213/652 (32.7) | 424/890 (47.6) | 198/378 (52.4) | 68/123 (55.3) | <0.001 | <0.001 |
| Major mutation, n (%) | ||||||||
| BRAFV600E | 507/752 (67.4) | 443/580 (76.4) | 488/653 (74.7) | 647/906 (71.4) | 235/410 (57.3) | 59/134 (44.0) | 0.032 | <0.001 |
| RAS | 4/71 (5.6) | 5/95 (5.3) | 7/143 (4.9) | 37/406 (9.1) | 32/315 (10.2) | 15/123 (12.2) | 0.827 | 0.011 |
| TERT | 2/59 (3.4) | 1/84 (1.2) | 2/123 (1.6) | 14/353 (4.0) | 29/260 (11.2) | 18/99 (18.2) | 1.000 | <0.001 |
| Subject | SNUH-RS Dataset 1 | TCGA Dataset 2 | ||||
|---|---|---|---|---|---|---|
| Gene | q-Value | Log2(FC) | Gene | q-Value | Log2(FC) | |
| All PTC | ||||||
| ≤1.0 vs. >1.0 cm | SFTPA1 | 1.67 × 10−5 | 1.33 | |||
| (No. 1 = 43 vs. 81 No. 2 = 39 vs. 457) | ECM1 | 2.67 × 10−5 | 1.25 | |||
| KCNK17 | 9.92 × 10−5 | 1.18 | ||||
| FGF12 | 1.58 × 10−4 | 1.09 | ||||
| HIST1H1C | 1.84 × 10−4 | 1.06 | ||||
| PIWIL1 | 2.02 × 10−4 | 1.13 | ||||
| ESM1 | 2.40 × 10−4 | 1.02 | ||||
| CNTFR | 4.45 × 10−4 | 1.12 | ||||
| HSPB7 | 4.45 × 10−4 | 1.05 | ||||
| TRIM36 | 1.01 × 10−3 | 1.03 | ||||
| PYGM | 1.03 × 10−3 | 1.00 | ||||
| CSMD1 | 1.45 × 10−3 | 1.02 | ||||
| RAS mutant PTC | ||||||
| ≤1.0 vs. >1.0 cm | CXCL9 | 1.03 × 10−3 | −2.02 | DLG2 | 5.55 × 10−3 | −1.70 |
| (No. 1 = 4 vs. 20 No. 2 = 3 vs. 49) | DGKI | 1.46 × 10−2 | −1.61 | |||
| FAP | 1.75 × 10−2 | −1.71 | ||||
| HTRA3 | 1.75 × 10−2 | −1.68 | ||||
| FRAS1 | 1.83 × 10−2 | −1.60 | ||||
| TTN | 1.83 × 10−2 | −1.52 | ||||
| IL7R | 1.83 × 10−2 | −1.62 | ||||
| CTSE | 2.08 × 10−2 | −1.59 | ||||
| ITGAL | 2.33 × 10−2 | −1.34 | ||||
| NEK6 | 3.44 × 10−2 | −1.21 | ||||
| PTPRC | 3.77 × 10−2 | −1.39 | ||||
| KIAA1324 | 3.84 × 10−2 | −1.51 | ||||
| HNMT | 4.15 × 10−2 | −1.15 | ||||
| AKR1C2 | 4.15 × 10−2 | −1.48 | ||||
| SCN3B | 4.15 × 10−2 | −1.46 | ||||
| MFAP5 | 4.15 × 10−2 | −1.23 | ||||
| COL3A1 | 4.77 × 10−2 | −1.45 | ||||
| H2AFX | 1.83 × 10−2 | 1.16 | ||||
| CEBPD | 2.50 × 10−2 | 1.27 | ||||
| C4orf48 | 4.15 × 10−2 | 1.41 | ||||
| All PTMC | ||||||
| ≤0.6 vs. >0.6 cm | SFTPA2 | 1.21 × 10−6 | −2.16 | |||
| (No. 1 = 13 vs. 30 No. 2 = 9 vs. 30) | JSRP1 | 5.94 × 10−4 | −1.74 | |||
| COL9A3 | 1.85 × 10−2 | −1.50 | ||||
| FLJ40330 | 1.85 × 10−2 | −1.53 | ||||
| DERL3 | 2.68 × 10−2 | −1.44 | ||||
| SIDT1 | 2.68 × 10−2 | −1.43 | ||||
| FKBP11 | 4.72 × 10−2 | −1.26 | ||||
| TXNDC5 | 4.72 × 10−2 | −1.05 | ||||
| SPAG17 | 2.67 × 10−2 | 1.35 | ||||
| ≤0.7 vs. >0.7 cm | TRIB3 | 6.96 × 10−6 | −1.19 | VGF | 1.14 × 10−4 | −1.19 |
| (No. 1 = 22 vs. 21 No. 2 = 14 vs. 25) | CR2 | 6.96 × 10−6 | −1.26 | SLC25A15 | 3.45 × 10−2 | −1.02 |
| IGFN1 | 7.21 × 10−6 | −1.23 | ||||
| PAX9 | 6.67 × 10−5 | 1.58 | ||||
| LAMA3 | 3.59 × 10−3 | 1.34 | ||||
| PLN | 6.88 × 10−3 | 1.15 | ||||
| SFRP1 | 6.96 × 10−3 | 1.26 | ||||
| COL7A1 | 6.96 × 10−3 | 1.24 | ||||
| CNN1 | 7.21 × 10−3 | 1.21 | ||||
| ADAMTS12 | 1.92 × 10−2 | 1.03 | ||||
| HS6ST2 | 1.92 × 10−2 | 1.16 | ||||
| BNC2 | 3.23 × 10−2 | 1.02 | ||||
| GPC6 | 4.07 × 10−2 | 1.02 | ||||
| ≤0.8 vs. >0.8 cm | FGFR3 | 2.45 × 10−7 | 1.87 | SPAG17 | 3.69 × 10−2 | 1.07 |
| (No. 1 = 32 vs. 11 No. 2 = 17 vs. 22) | SAMD11 | 1.47 × 10−3 | 1.51 | |||
| LGR6 | 2.83 × 10−3 | 1.46 | ||||
| PASK | 4.95 × 10−2 | 1.16 | ||||
| BRAF mutant PTMC | ||||||
| ≤0.6 vs. >0.6 cm | TMEM132D | 1.04 × 10−5 | −1.81 | |||
| (No. 1 = 11 vs. 18 No. 2 = 3 vs. 15) | FOXA2 | 4.54 × 10−3 | −1.06 | |||
| DDO | 3.62 × 10−2 | 1.18 | ||||
| ≤0.7 vs. >0.7 cm | LAMA3 | 3.44 × 10−3 | 1.17 | KIAA1199 | 6.96 × 10−3 | −1.07 |
| (No. 1 = 18 vs. 11 No. 2 = 6 vs. 12) | PHEX | 3.44 × 10−3 | 1.22 | |||
| GLDN | 4.65 × 10−3 | 1.08 | ||||
| HS6ST2 | 1.79 × 10−2 | 1.04 | ||||
| PLN | 2.83 × 10−2 | 1.02 | ||||
| ≤0.8 vs. >0.8 cm | MKX | 1.52 × 10−2 | −1.24 | |||
| (No. 1 = 22 vs. 7 No. 2 = 7 vs. 11) | KIAA1199 | 1.58 × 10−2 | −1.12 | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, Y.S.; Kang, B.-H.; Lee, S.; Yoo, S.-K.; Choi, Y.S.; Park, J.; Park, D.Y.; Lee, K.E.; Seo, J.-S.; Park, Y.J. Genomic and Transcriptomic Characteristics According to Size of Papillary Thyroid Microcarcinoma. Cancers 2020, 12, 1345. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12051345
Song YS, Kang B-H, Lee S, Yoo S-K, Choi YS, Park J, Park DY, Lee KE, Seo J-S, Park YJ. Genomic and Transcriptomic Characteristics According to Size of Papillary Thyroid Microcarcinoma. Cancers. 2020; 12(5):1345. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12051345
Chicago/Turabian StyleSong, Young Shin, Byung-Hee Kang, Seungbok Lee, Seong-Keun Yoo, Young Sik Choi, Jungsun Park, Dong Yoon Park, Kyu Eun Lee, Jeong-Sun Seo, and Young Joo Park. 2020. "Genomic and Transcriptomic Characteristics According to Size of Papillary Thyroid Microcarcinoma" Cancers 12, no. 5: 1345. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12051345