Testis Sparing Surgery in Pediatric Testicular Tumors

 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
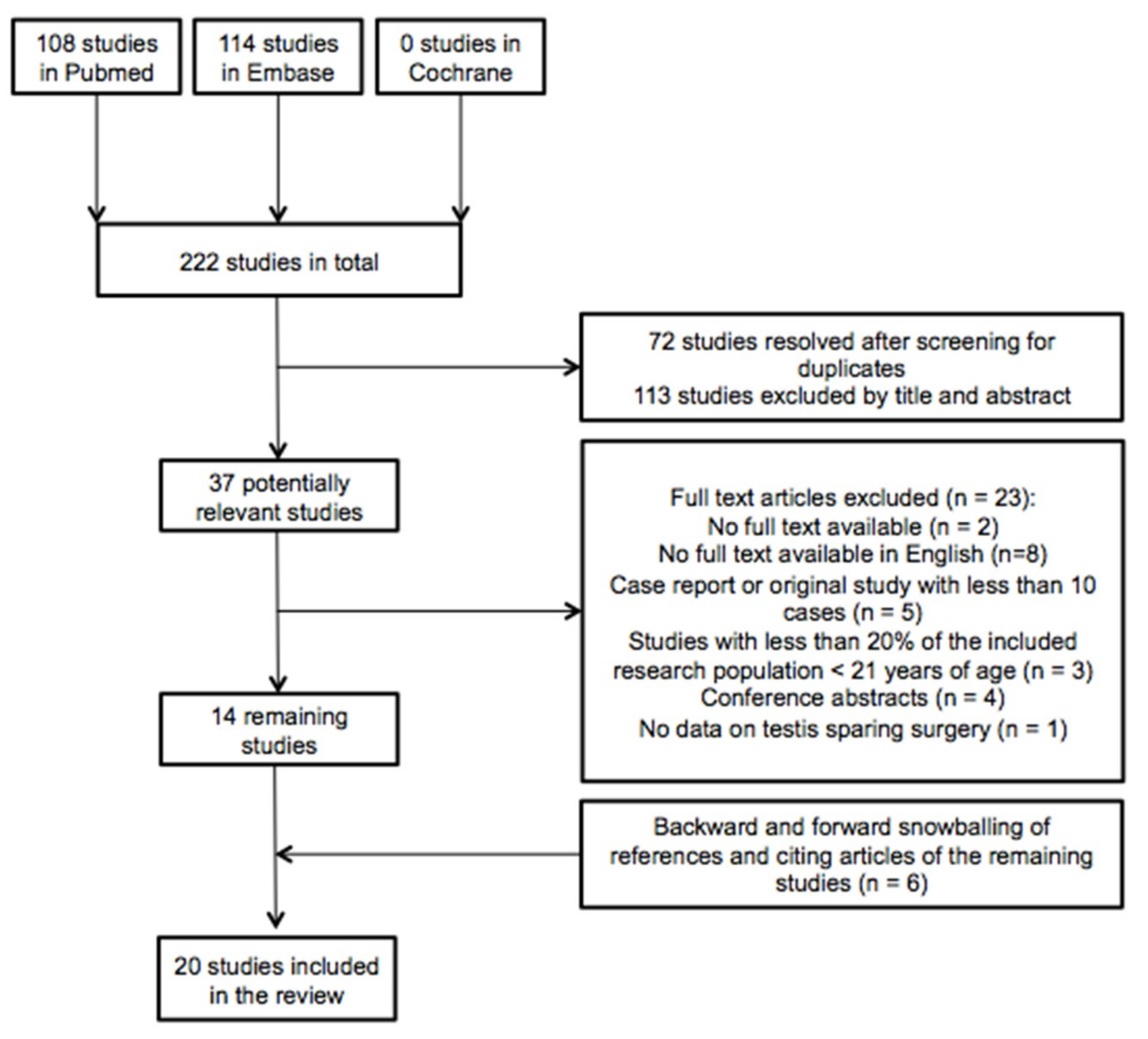
2.1. Search and Selection
2.2. Quality Assessment
2.3. Characteristics of the Included Articles
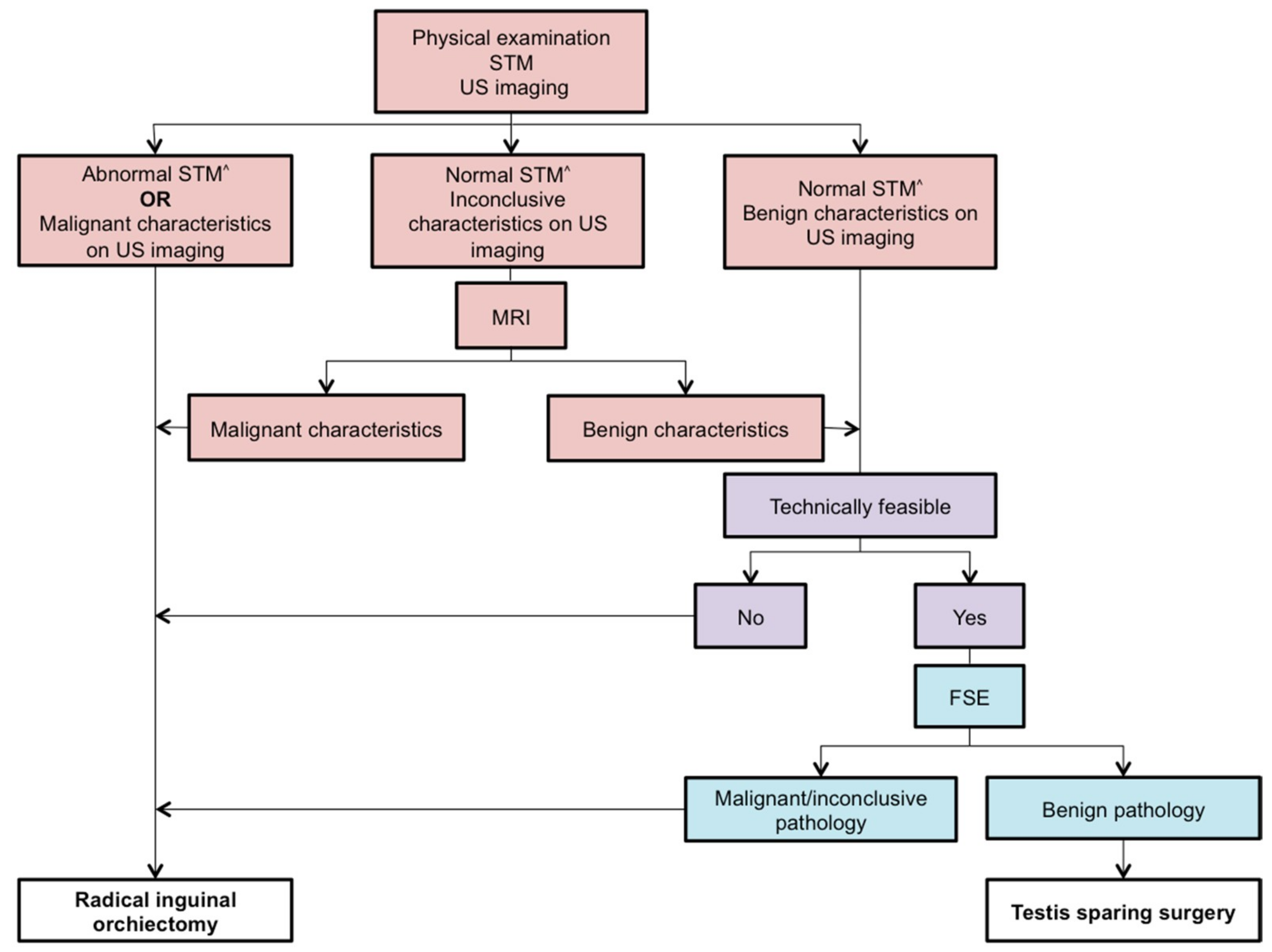
2.4. Criteria for TSS
2.5. TSS in GCTs
2.6. TSS in Non-GCTs
3. Discussion
4. Materials and Methods
4.1. Search Strategy and Study Selection
4.2. Eligibility Criteria
4.3. Quality Assessment
4.4. Data Collection and Data Items
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Kusler, K.A.; Poynter, J.N. International testicular cancer incidence rates in children, adolescents and young adults. Cancer Epidemiology 2018, 56, 106–111. [Google Scholar] [CrossRef]
- Ahmed, H.U.; Arya, M.; Muneer, A.; Mushtaq, I.; Sebire, N.J. Testicular and paratesticular tumours in the prepubertal population. Lancet Oncol. 2010, 11, 476–483. [Google Scholar] [CrossRef]
- Looijenga, L.; Van der Kwast, T.H.; Grignon, D.; Egevad, L.; Kristiansen, G.; Kao, C.S.; Idrees, M.T. Report From the International Society of Urological Pathology (ISUP) Consultation Conference on Molecular Pathology of Urogenital Cancers, IV: Current and Future Utilization of Molecular-Genetic Tests for Testicular Germ Cell Tumors. Am. J. Surg. Pathol. 2020, 44, e66–e79. [Google Scholar] [CrossRef] [PubMed]
- Calaminus, G.; Schneider, D.T.; von Schweinitz, D.; Jürgens, H.; Infed, N.; Schönberger, S.; Olson, T.A.; Albers, P.; Vokuhl, C.; Stein, R.; et al. Age-Dependent Presentation and Clinical Course of 1465 Patients Aged 0 to Less than 18 Years with Ovarian or Testicular Germ Cell Tumors; Data of the MAKEI 96 Protocol Revisited in the Light of Prenatal Germ Cell Biology. Cancers 2020, 12, 611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moch, H.; Cubilla, A.L.; Humphrey, P.A.; Reuter, V.E.; Ulbright, T.M. The 2016 WHO Classification of Tumours of the Urinary System and Male Genital Organs-Part A: Renal, Penile, and Testicular Tumours. Eur. Urol. 2016, 70, 93–105. [Google Scholar] [CrossRef] [PubMed]
- Pohl, H.G.; Shukla, A.R.; Metcalf, P.D.; Cilento, B.G.; Retik, A.B.; Bagli, D.J.; Huff, D.S.; Rushton, H.G. Prepubertal testis tumors: actual prevalence rate of histological types. J. Urol. 2004, 172, 2370–2372. [Google Scholar] [CrossRef]
- Nogueira Neto, F.B.; Petrilli, A.S.; Macedo, C.R.; Caran, E.M. Testicular tumors in children and adolescents. J. Pediatr. (Rio. J.) 2012, 88, 87–92. [Google Scholar] [CrossRef] [Green Version]
- Maizlin, I.I.; Dellinger, M.; Gow, K.W.; Goldin, A.B.; Goldfarb, M.; Nuchtern, J.G.; Langer, M.; Vasudevan, S.A.; Doski, J.J.; Raval, M.V.; et al. Testicular tumors in prepubescent patients. J. Pediatr. Surg. 2018, 53, 1748–1752. [Google Scholar] [CrossRef]
- Ghoreifi, A.; Djaladat, H. Management of Primary Testicular Tumor. Urol. Clin. North Am. 2019, 46, 333–339. [Google Scholar] [CrossRef]
- Capelouto, C.C.; Clark, P.E.; Ransil, B.J.; Loughlin, K.R. A review of scrotal violation in testicular cancer: is adjuvant local therapy necessary? J. Urol. 1995, 153, 981–985. [Google Scholar] [CrossRef]
- Li, J.; Power, N. Scrotal recurrence of germ cell tumour in a non-violated scrotum. Can. Urol. Assoc. J. 2016, 10, E388–E391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, H.D.; Gupta, M.; Cheaib, J.G.; Sharma, R.; Zhang, A.; Bass, E.B.; Pierorazio, P.M. Testis-sparing surgery and scrotal violation for testicular masses suspicious for malignancy: A systematic review and meta-analysis. Urol. Oncol. 2020, 38, 344–353. [Google Scholar] [CrossRef] [PubMed]
- Zuniga, A.; Lawrentschuk, N.; Jewett, M.A. Organ-sparing approaches for testiclar masses. Nat. Rev. Urol. 2010, 7, 454–464. [Google Scholar] [CrossRef] [PubMed]
- Woo, L.L.; Ross, J.H. The role of testis-sparing surgery in children and adolescents with testicular tumors. Urol. Oncol. 2016, 34, 76–83. [Google Scholar] [CrossRef]
- Stoop, H.; Kirkels, W.; Dohle, G.R.; Gillis, A.J.; den Bakker, M.A.; Biermann, K.; Oosterhuis, W.; Looijenga, L.H. Diagnosis of testicular carcinoma in situ’ (intratubular and microinvasive)’ seminoma and embryonal carcinoma using direct enzymatic alkaline phosphatase reactivity on frozen histological sections. Histopathology 2011, 58, 440–446. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, U.; Netto Júnior, N.R.; Esteves, S.C.; Rivero, M.A.; Schirren, C. Comparative study of the fertility potential of men with only one testis. Scand. J. Urol. Nephrol. 1991, 25, 255–259. [Google Scholar] [CrossRef]
- Cheng, L.; Albers, P.; Berney, D.M.; Feldman, D.R.; Daugaard, G.; Gilligan, T.; Looijenga, L. Testicular cancer. Nat. Rev. Dis. Prim. 2018, 4. [Google Scholar] [CrossRef]
- Brunocilla, E.; Gentile, G.; Schiavina, R.; Borghesi, M.; Franceschelli, A.; Pultrone, C.V.; Chessa, F.; Romagnoli, D.; Ghanem, S.M.; Gacci, M.; et al. Testis-sparing surgery for the conservative management of small testicular masses: An update. Anticancer Res. 2013, 33, 5205–5210. [Google Scholar]
- La Rocca, R.; Capece, M.; Spirito, L.; Cumberbatch, M.K.; Creta, M.; Altieri, V.; Franco, G.; Albisinni, S.; Mirone, V.; Esperto, F.; et al. Testis-sparing surgery for testicular masses: Current perspectives. Minerva Urol. e Nefrol. 2019, 71, 359–364. [Google Scholar] [CrossRef]
- Giannarini, G.; Dieckmann, K.P.; Albers, P.; Heidenreich, A.; Pizzocaro, G. Organ-Sparing Surgery for Adult Testicular Tumours: A Systematic Review of the Literature. Eur. Urol. 2010, 57, 780–790. [Google Scholar] [CrossRef]
- Paffenholz, P.; Pfister, D.; Heidenreich, A. Testis-preserving strategies in testicular germ cell tumors and germ cell neoplasia in situ. Transl. Androl. Urol. 2020, 9, S24–S30. [Google Scholar] [CrossRef] [PubMed]
- Radford, A.; Peycelon, M.; Haid, B.; Powis, M.; Lakshminarayanan, B. Testicular-sparing surgery in the pediatric population: Multicenter review of practice with review of the literature. Curr. Opin. Urol. 2019, 29, 481–486. [Google Scholar] [CrossRef] [PubMed]
- Caldwell, B.T.; Saltzman, A.F.; Maccini, M.A.; Cost, N.G. Appropriateness for testis-sparing surgery based on the testicular tumor size in a pediatric and adolescent population. J. Pediatr. Urol. 2019, 15, 70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, P.; Li, W.; Song, H.C.; Jiao, L.L.; Zhang, W.P.; Sun, N. Characteristics, treatment decisions and outcomes of prepubertal testicular germ cell tumor: A descriptive analysis from a large Chinese center. J. Pediatr. Urol. 2018, 14, 443. [Google Scholar] [CrossRef] [PubMed]
- Wu, D.; Shen, N.; Lin, X.; Chen, X. Prepubertal testicular tumors in China: a 10-year experience with 67 cases. Pediatr. Surg. Int. 2018, 34, 1339–1343. [Google Scholar] [CrossRef]
- Ye, Y.L.; He, Q.M.; Zheng, F.F.; Guo, S.J.; Zhou, F.J.; Qin, Z.K. Trends of testis-sparing surgery for pediatric testicular tumors in South China. BMC Surg. 2017, 17, 31. [Google Scholar] [CrossRef] [Green Version]
- Friend, J.; Barker, A.; Khosa, J.; Samnakay, N. Benign scrotal masses in children – some new lessons learned. J. Pediatr. Surg. 2016, 51, 1737–1742. [Google Scholar] [CrossRef]
- Wei, Y.; Wu, S.; Lin, T.; He, D.; Li, X.; Liu, J.; Liu, X.; Hua, Y.; Lu, P.; Wei, G. Testicular yolk sac tumors in children: a review of 61 patients over 19 years. World J. Surg. Oncol. 2014, 12, 400. [Google Scholar] [CrossRef] [Green Version]
- Zahran, M.H.; Helmy, T.E.; Hafez, A.T.; Dawaba, M. Prepubertal testicular tumours: Should testicular-sparing surgery be considered? A single-institution experience and review of the literature. Arab J. Urol. 2014, 12, 130–136. [Google Scholar] [CrossRef]
- Wang, X.; Xu, S.; Tang, D.; Li, M.; Wu, D.; Huang, Y. Prepubertal testicular and paratesticular tumors in China: A single-center experience over a 10-year period. J. Pediatr. Surg. 2012, 47, 1576–1580. [Google Scholar] [CrossRef]
- Bujons, A.; Sfulcini, J.C.; Pascual, M.; Feu, O.A.; Garat, J.M.; Villavicencio, H. Prepubertal testicular tumours and efficacy of testicular preserving surgery. BJU Int. 2011, 107, 1812–1816. [Google Scholar] [CrossRef] [PubMed]
- Cecchetto, G.; Alaggio, R.; Bisogno, G.; Virgone, C.; Dall’Igna, P.; Terenziani, M.; Boldrini, R.; D’Onofrio, V.; Ferrari, A.; Bernini, G. Sex cord-stromal tumors of the testis in children. A clinicopathologic report from the Italian TREP project. J. Pediatr. Surg. 2010, 45, 1868–1873. [Google Scholar] [CrossRef] [PubMed]
- Hisamatsu, E.; Takagi, S.; Nakagawa, Y.; Sugita, Y.; Yoshino, K.; Ueoka, K.; Tanikaze, S. Prepubertal testicular tumors: a 20-year experience with 40 cases. Int. J. Urol. 2010, 17, 956–959. [Google Scholar] [CrossRef] [PubMed]
- Nerli, R.B.; Ajay, G.; Shivangouda, P.; Pravin, P.; Reddy, M.; Pujar, V.C. Prepubertal testicular tumors: Our 10 years experience. Indian J. Cancer 2010, 47, 292–295. [Google Scholar] [CrossRef] [PubMed]
- Suardi, N.; Strada, E.; Colombo, R.; Freschi, M.; Salonia, A.; Lania, C.; Cestari, A.; Carmignani, L.; Guazzoni, G.; Rigatti, P.; et al. Leydig cell tumour of the testis: presentation, therapy, long-term follow-up and the role of organ-sparing surgery in a single-institution experience. BJU Int. 2009, 103, 197–200. [Google Scholar] [CrossRef] [PubMed]
- Taskinen, S.; Fagerholm, R.; Aronniemi, J.; Rintala, R.; Taskinen, M. Testicular tumors in children and adolescents. J. Pediatr. Urol. 2008, 4, 134–137. [Google Scholar] [CrossRef]
- Treiyer, A.; Blanc, G.; Stark, E.; Haben, B.; Treiyer, E.; Steffens, J. Prepubertal testicular tumors: frequently overlooked. J. Pediatr. Urol. 2007, 3, 480–483. [Google Scholar] [CrossRef]
- Shukla, A.R.; Woodard, C.; Carr, M.C.; Huff, D.S.; Canning, D.A.; Zderic, S.A.; Kolon, T.F.; Snyder, H.M. Experience with testis sparing surgery for testicular teratoma. J. Urol. 2004, 171, 161–163. [Google Scholar] [CrossRef]
- Metcalfe, P.D.; Farivar-Mohseni, H.; Farhat, W.; McLorie, G.; Khoury, A.; Bägli, D.J. Pediatric testicular tumors: Contemporary incidence and efficacy of testicular preserving surgery. J. Urol. 2003, 170, 2412–2416. [Google Scholar] [CrossRef]
- Ciftci, A.O.; Bingöl-Koloğlu, M.; Senocak, M.E.; Tanyel, F.C.; Büyükpamukçu, M.; Büyükpamukçu, N. Testicular tumors in children. J. Pediatr. Surg. 2001, 36, 1796–1801. [Google Scholar] [CrossRef]
- J.S. Valla for the Group D’Etude en Urologie Pédiatrique. Testis-sparing surgery for benign testicular tumors in children. J. Urol. 2001, 165, 2280–2283. [Google Scholar] [CrossRef]
- Sugita, Y.; Clarnette, T.D.; Cooke-Yarborough, C.; Chow, C.W.; Waters, K.; Hutson, J.M. Testicular and paratesticular tumours in children: 30 years’ experience. Aust. N. Z. J. Surg. 1999, 69, 505–508. [Google Scholar] [CrossRef] [PubMed]
- Borghesi, M.; Brunocilla, E.; Schiavina, R.; Gentile, G.; Dababneh, H.; Della Mora, L.; del Prete, C.; Franceschelli, A.; Colombo, F.; Martorana, G. Role of testis-sparing surgery in the conservative management of small testicular masses: Oncological and functional perspectives. Actas Urológicas Españolas 2015, 39, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Del Pozo Jiménez, G.; Castillón Vela, I.; Turo Antona, J.; Gimeno Collado, A.; Carballido Rodríguez, J. Orquiectomía parcial en tumor testicular: técnica quirúrgica y papel de la ecografía intraoperatoria. Arch. Esp. Urol. 2019, 72, 772–785. [Google Scholar]
- Ross, J.H.; Rybicki, L.; Kay, R. Clinical behavior and a contemporary management algorithm for prepubertal testis tumors: A summary of the prepubertal testis tumor registry. J. Urol. 2002, 168, 1675–1679. [Google Scholar] [CrossRef]
- Murray, M. J.; Nicholson, J. C. α-Fetoprotein. Arch. Dis. Child. Educ. Pract. Ed. 2011, 96, 141–147. [Google Scholar] [CrossRef]
- Sangüesa, C.; Veiga, D.; Llavador, M.; Serrano, A. Testicular tumours in children: an approach to diagnosis and management with pathologic correlation. Insights Imaging 2020, 11, 74. [Google Scholar] [CrossRef]
- Mittal, P.K.; Abdalla, A.S.; Chatterjee, A.; Baumgarten, D.A.; Harri, P.A.; Patel, J.; Moreno, C.C.; Gabriel, H.; Miller, F.H. Spectrum of extratesticular and testicular pathologic conditions at scrotal MR imaging. Radiographics 2018, 38, 806–830. [Google Scholar] [CrossRef] [Green Version]
- Albers, P.; Albrecht, W.; Algaba, F.; Bokemeyer, C.; Cohn-Cedermark, G.; Fizazi, K.; Horwich, A.; Laguna, M.P.; Nicolai, N.; Oldenburg, J.; et al. Guidelines on Testicular Cancer: 2015 Update. Eur. Urol. 2015, 68, 1054–1068. [Google Scholar] [CrossRef]
- Elert, A.; Olbert, P.; Hegele, A.; Barth, P.; Hofmann, R.; Heidenreich, A. Accuracy of frozen section examination of testicular tumors of uncertain origin. Eur. Urol. 2002, 41, 290–293. [Google Scholar] [CrossRef]
- Matei, D.V.; Vartolomei, M.D.; Renne, G.; Tringali, V.; Russo, A.; Bianchi, R.; Cozzi, G.; Bottero, D.; Musi, G.; Mazzarol, G.; et al. Reliability of Frozen Section Examination in a Large Cohort of Testicular Masses: What Did We Learn? Clin. Genitourin. Cancer 2017, 15, e689–e696. [Google Scholar] [CrossRef] [PubMed]
- Steiner, H.; Höltl, L.; Maneschg, C.; Berger, A.P.; Rogatsch, H.; Bartsch, G.; Hobisch, A. Frozen section analysis-guided organ-sparing approach in testicular tumors: Technique, feasibility, and long-term results. Urology 2003, 62, 508–513. [Google Scholar] [CrossRef]
- Nord, C.; Bjøro, T.; Ellingsen, D.; Mykletun, A.; Dahl, O.; Klepp, O.; Bremnes, R.M.; Wist, E.; Fosså, S.D. Gonadal hormones in long-term survivors 10 years after treatment for unilateral testicular cancer. Eur. Urol. 2003, 44, 322–328. [Google Scholar] [CrossRef]
- Zu’bi, F.; Koyle, M.A.; Rickard, M.; Beaiti, M.; Kahn, N.; Blais, A.S.; Hannick, J.H.; Lopes, R.I.; Lorenzo, A.J. Testis-sparing Surgery for Pediatric Leydig Cell Tumors: Evidence of Favorable Outcomes Irrespective of Surgical Margins. Urology 2019, 134, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Ross, J.H.; Kay, R. Prepubertal testis tumors. Rev. Urol. 2004, 6, 11–18. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6. [Google Scholar] [CrossRef] [Green Version]
- Claes, W. Guidelines for snowballing in systematic literature studies and a replication in software engineering. ACM Int. Conf. Proceeding Ser. 2014, 38, 1–10. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [Green Version]
- Howick, J.; Chalmers, I.; Howick, P.; Greenhalgh, T.; Heneghan, C.; Liberati, A.; Moschetti, I.; Phillips, B.; Thornton, H.; Hodgkinson, M.; et al. The Oxford Levels of Evidence 2. Oxford Cent. Evidence-Based Med. 2011. Available online: https:www.cebm.ox.ac.uk/resources/levels-of-evidence/ocebm-levels-of-evidence (accessed on 28 May 2020).



{kind=link}
{kind=link}
| Study | Oxford Level | n | TSS (n) | Median Age in Years | Median Follow-Up in Months | n of Benign Histopathology | n of Malignant Histopathology |
|---|---|---|---|---|---|---|---|
| Caldwell 2019 [23] | 4 | 24 | 9 | 10.7 | 7.15 # | 22 | 2 |
| Liu 2018 [24] | 4 | 171 | 113 | 1.66 | 54 | 120 | 51 |
| Wu 2018 [25] | 4 | 67 | 30 | 1.5 | 34 | 44 | 23 |
| Ye 2017 [26] | 4 | 47 | 16 | 3.17 | 56 | 47 | 0 |
| Friend 2016 [27] | 4 | 21 | 8 | 4 | ND | 12 | 9 |
| Wei 2014 [28] | 4 | 61 | 1 | 1.5 | 48^ | 0 | 61 |
| Zahran 2014 [29] | 4 | 13 | 3 | 8.7 | ND | 7 | 6 |
| Wang 2012 [30] | 4 | 63 | 15 | 0.92 | 50 | 40 | 23 |
| Bujons 2011 [31] | 4 | 15 | 11 | 8 | 65 | 12 | 3 |
| Cecchetto 2010 [32] | 4 | 11 | 4 | 1.92 | 59 ^ | ND | ND |
| Hisamatsu 2010 [33] | 4 | 40 | 8 | 1.17 | 68 | 25 | 15 |
| Nerli 2010 [34] | 4 | 22 | 9 | 4.6 ^ | 47 | 16** | 4 ** |
| Suardi 2009 [35] | 4 | 37 | 28 | 33 | 4.6 years | 37 | 0 |
| Taskinen 2008 [36] | 4 | 34 | 10 | 3.2 | 3.5 years # | 23 | 11 |
| Treiyer 2007 [37] | 4 | 15 | 3 | 4 | 48.2 ^ | 13 | 2 |
| Shukla 2004 [38] | 4 | 77 | 13 | 2.88 ^ | 72 | 37 | 40 |
| Metcalfe 2003 [39] | 4 | 48 | 13 | 1.5 | 3 years | 27 ** | 17 ** |
| Ciftci 2001 [40] | 4 | 51 | 5 | 3.8^ | 89 ^ | 15 | 36 |
| Valla 2001 [41] | 4 | 83 | 56 | ND | 4.8 years ^ | 83 | 0 |
| Sugita 1999 [42] | 4 | 68 | 21 | 3.6^ | 9 years ^ | 34 | 22 |
| Study | n | n TSS (%) | Median Age in Years (Range) | Median Follow-Up in Months (Range) | STM | Recurrence | Testicular Atrophy |
|---|---|---|---|---|---|---|---|
| Teratoma | |||||||
| Liu 2018 [24] | 87 | ||||||
| MT (70) | 70 (100%) | 1.7 (0.4–11.6) | 52.2 (20–125) | AFP < 1 years abnormal ^^ AFP > 1 year normal, hCG normal | None | ND | |
| IT (17) | 10 (58.8%) | 0.4 (0–1) | 44.0 (20–115) | None | |||
| Wu 2018 [25] | 32 | 19 (59.4%) | 1.6 (0.3–14) | 23 | AFP normal, hCG normal | None | None |
| Ye 2017 [26] | 37 | ||||||
| MT (37) | 8 (21.6%) | ND | ND | AFP normal, hCG normal | None | None | |
| Friend 2016 [27] | 4 | 1 (25%) | 1.5 (0.4–4) | ND | ND | None | ND |
| Wang 2012 [30] | 32 | ||||||
| MT (27) | 9 (33.3%) | 0.8 | 60 | AFP > 6 months normal | None | None | |
| IT (5) | 1 (20%) | 0.3 | 26 | AFP < 6 months abnormal (2) | None | None | |
| Bujons 2011 [31] | 2 | 2 (100%) | 0.3 | 56.5 (48–65) | AFP normal, hCG normal | None | None |
| Hisamatsu 2010 [33] | 18 | 5 (27.8%) | ND | ND | AFP < 6 months abnormal ^^ (2) AFP > 6 months normal, hCG normal | Recurrence (1) | None |
| Nerli 2010 [34] | 13 | ||||||
| MT (11) | 7 (63.6%) | ND | 47 # | AFP normal | None | None | |
| IT (2) | 0 (0%) | ND | ND | AFP normal | None | NA | |
| Taskinen 2008 [36] | 16 | ||||||
| MT (15) | 4 (25%) | 2.6 (0.2–15.2) | 3.5 years (0.5–6.7) # | AFP normal, hCG normal | Recurrence (2) | ND | |
| IT (1) | |||||||
| Treiyer 2007 [37] | 3 | ||||||
| MT (2) | 0 (0%) | 6.5 (4–9) | ND | AFP normal, hCG normal | None | NA | |
| IT (1) | 0.17 | AFP normal, hCG normal | |||||
| Shukla 2004 [38] | 11 | ||||||
| MT (11) | 8 (72.7%) | 2.9 (0.3–10) * | 88 (5–22) * | AFP normal | None | None | |
| Metcalfe 2003 [39] | 22 | ||||||
| MT (19) | 7 (31.8%) | 2.3^ | 3 years^ (11 months–14 years) # | AFP abnormal (2), hCG normal AFP normal, hCG normal | None | None | |
| IT (3) | None | None | |||||
| Ciftci 2001 [40] | 9 | 2 (22%) | 2.5 ^ (± 0.6) | ND | ND | None | ND |
| Valla 2001 [41] | 33 | 16 (48.5%) | ND | ND | ND | None | None |
| Sugita 1999 [42] | 27 | 17 (63.0%) | 2.3 ^ (0.2–14) | 10 years ^ (4 months–26) | ND | None | None |
| Epidermoid cyst | 186 + 89 | ||||||
| Liu 2018 [24] | 33 | 33 (100%) | 7.1 (0.7–11.8) | 50 (18–101) | hCG normal | None | ND |
| Wu 2018 [25] | 9 | 8 (88.8%) | 2 (0.3–13.9) | 27 | AFP normal | None | None |
| Ye 2017 [26] | 3 | 3 (100%) | ND | ND | AFP abnormal (1), hCG normal | None | None |
| Friend 2016 [27] | 3 | 3 (100%) | 9 (8–15) | ND | ND | Recurrence (1) | ND |
| Wang 2012 [30] | 4 | 3 (75%) | 10 | 60.5 | AFP normal | None | None |
| Bujons 2011 [31] | 4 | 4 (100%) | 11.5 (10–13) | 65 (48–100) | AFP normal, hCG normal | None | None |
| Hisamatsu 2010 [33] | 5 | 3 (60%) | ND | ND | ND | None | None |
| Nerli 2010 [34] | 3 | 2 (66.6%) | ND | 47 # | AFP normal | None | None |
| Taskinen 2008 [36] | 2 | 2 (100%) | 8.0 (1.2–14.7) | 3.5 years (0.5–6.7) # | AFP normal, hCG normal | None | ND |
| Treiyer 2007 [37] | 4 | 2 (50%) | 3.5 (0.1–9) | ND | AFP normal, hCG normal | None | ND |
| Shukla 2004 [38] | 5 | 5 (100%) | 2.9 (0.3–10) ** | 88 (5–22) ** | AFP normal | None | None |
| Metcalfe 2003 [39] | 5 | 5 (100%) | 5.5 ^ | 3 years ^ (11 months–14 years) # | AFP < 6 months abnormal (1), hCG normal | None | None |
| Ciftci 2001 [40] | 3 | 3 (100%) | 3.6 ^ (± 1.2) | ND | ND | None | ND |
| Valla 2001 [41] | 15 | 13 (86.7%) | ND | ND | ND | None | ND |
| Total | 444 | 275 (61.9%) | 3.7 + | Recurrence (4) | None |
| (a) | |||||||
| Study | n | n TSS (%) | Median Age in Years (Range) | Median Follow-Up in Months (Range) | STM | Recurrence | Testicular Atrophy |
| LCT | |||||||
| Wu 2018 [25] | 1 | 1 (100%) | 6.8 | 26 | AFP normal, hCG normal | None | None |
| Zahran 2014 [29] | 2 | 1 (50%) | 11 | 24 | AFP normal, hCG normal | None | None |
| Wang 2012 [30] | 2 | 2 (100%) | 6 | 67 | AFP normal | None | None |
| Cecchetto 2010 [32] | 4 | 3 * (75%) | 9.8 (6.8–11.6) | 59 ^ (8–94) ** | AFP normal, hCG normal | None | ND |
| Suardi 2009 [35] | 37 | 28 (75.7%) | 33 (5–67) | 4.6 years (0.6–16.2) | AFP normal, hCG normal | None | ND |
| Taskinen 2008 [36] | 2 | 2 (100%) | 7 (5.1–8.9) | 3.5 years (0.5–6.7) # | AFP normal, hCG normal | None | ND |
| Treiyer 2007 [37] | 1 | 1 (100%) | 6 | ND | AFP normal, hCG normal | None | ND |
| Ciftci 2001 [40] | 3 | 0 (0%) | 6 ^ (± 0.5) | ND | ND | ND | NA |
| Valla 2001 [41] | 4 | 4 (100%) | ND | ND | ND | None | None |
| Sugita 1999 [42] | 3 | 2 (66,6%) | 4.8 ^ (0.7–6) | 15 years ^ (12–21) | ND | None | ND |
| SCT | |||||||
| Zahran 2014 [29] | 2 | 0 (0%) | 3.5 | ND | AFP normal, hCG normal | None | NA |
| Cecchetto 2010 [32] | 1 | 0 (0%) | 0.3 | 59 ^ (8–94) * | AFP normal, hCG normal | None | NA |
| Taskinen 2008 [36] | 1 | 0 (0%) | 0.4 | 3.5 years (0.5–6.7) # | AFP normal, hCG normal | None | NA |
| Treiyer 2007 [37] | 1 | 0 (0%) | 14 | ND | AFP normal, hCG normal | None | NA |
| Metcalfe 2003 [39] | 2 | 0 (0%) | 3.1 (0.4–5.8) | ND | AFP normal, hCG normal | None | NA |
| Valla 2001 [41] | 7 | 5 (71.4%) | ND | ND | ND | None | None |
| Sugita 1999 [42] | 2 | 1 (50%) | 1.2 (0.2–2) | 11 years (5–13) | ND | None | ND |
| JGCT | |||||||
| Bujons 2011 [31] | 1 | 1 (100%) | 10 | 60 | AFP normal, hCG normal | None | None |
| Cecchetto 2010 [32] | 4 | 1 (25%) | 0.3 (0.2–1.9) | 59^ (8–94) * | AFP normal, hCG normal | None | ND |
| Valla 2001 [41] | 1 | 0 (0%) | ND | ND | ND | None | NA |
| Sugita 1999 [42] | 1 | 0 (0%) | 2.0 | 12 | ND | None | NA |
| Undifferentiated | |||||||
| Cecchetto 2010 [32] | 2 | 0 (0%) | 7.2 (0.1–14.3) | 59 ^ (8–94) * | AFP normal, hCG normal | None | NA |
| Valla 2001 [41] | 1 | 0 (0%) | ND | ND | ND | None | NA |
| Total | 85 | 52 (61.2%) | 6.6 + | None | |||
| (b) | |||||||
| Study | n | n TSS (%) | Median Age in Years (Range) | Median Follow-Up in Months (Range) | STM | Recurrence | Testicular Atrophy |
| Hemangioma | |||||||
| Wu 2018 [25] | 1 | 1 (100%) | 1.3 | 14 | AFP normal, hCG normal | None | None |
| Zahran 2014 [29] | 1 | 0 (0%) | 1.3 | ND | AFP normal, hCG normal | None | NA |
| Bujons 2011 [31] | 1 | 1 (100%) | 3 | 24 | AFP normal, hCG normal | None | None |
| Valla 2001 [41] | 1 | 1 (100%) | ND | ND | ND | None | None |
| Adenomatoid tumor | |||||||
| Ye 2017 [26] | 1 | 1 (100%) | ND | ND | AFP normal, hCG normal | None | None |
| Total | 5 | 4 (80%) | 1.9 + | None | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kooij, C.D.; Hulsker, C.C.C.; Kranendonk, M.E.G.; Zsiros, J.; Littooij, A.S.; Looijenga, L.H.J.; Klijn, A.J.; Mavinkurve-Groothuis, A.M.C. Testis Sparing Surgery in Pediatric Testicular Tumors. Cancers 2020, 12, 2867. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12102867
Kooij CD, Hulsker CCC, Kranendonk MEG, Zsiros J, Littooij AS, Looijenga LHJ, Klijn AJ, Mavinkurve-Groothuis AMC. Testis Sparing Surgery in Pediatric Testicular Tumors. Cancers. 2020; 12(10):2867. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12102867
Chicago/Turabian StyleKooij, Cezanne D., Caroline C.C. Hulsker, Mariëtte E.G. Kranendonk, József Zsiros, Annemieke S. Littooij, Leendert H.J. Looijenga, Aart J. Klijn, and Annelies M.C. Mavinkurve-Groothuis. 2020. "Testis Sparing Surgery in Pediatric Testicular Tumors" Cancers 12, no. 10: 2867. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12102867