
Vaccination against PD-L1 with IO103 a Novel Immune Modulatory Vaccine in Basal Cell Carcinoma: A Phase IIa Study

 , ,
, ,  , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
2.1. Patient Characteristics
2.2. Clinical Outcome
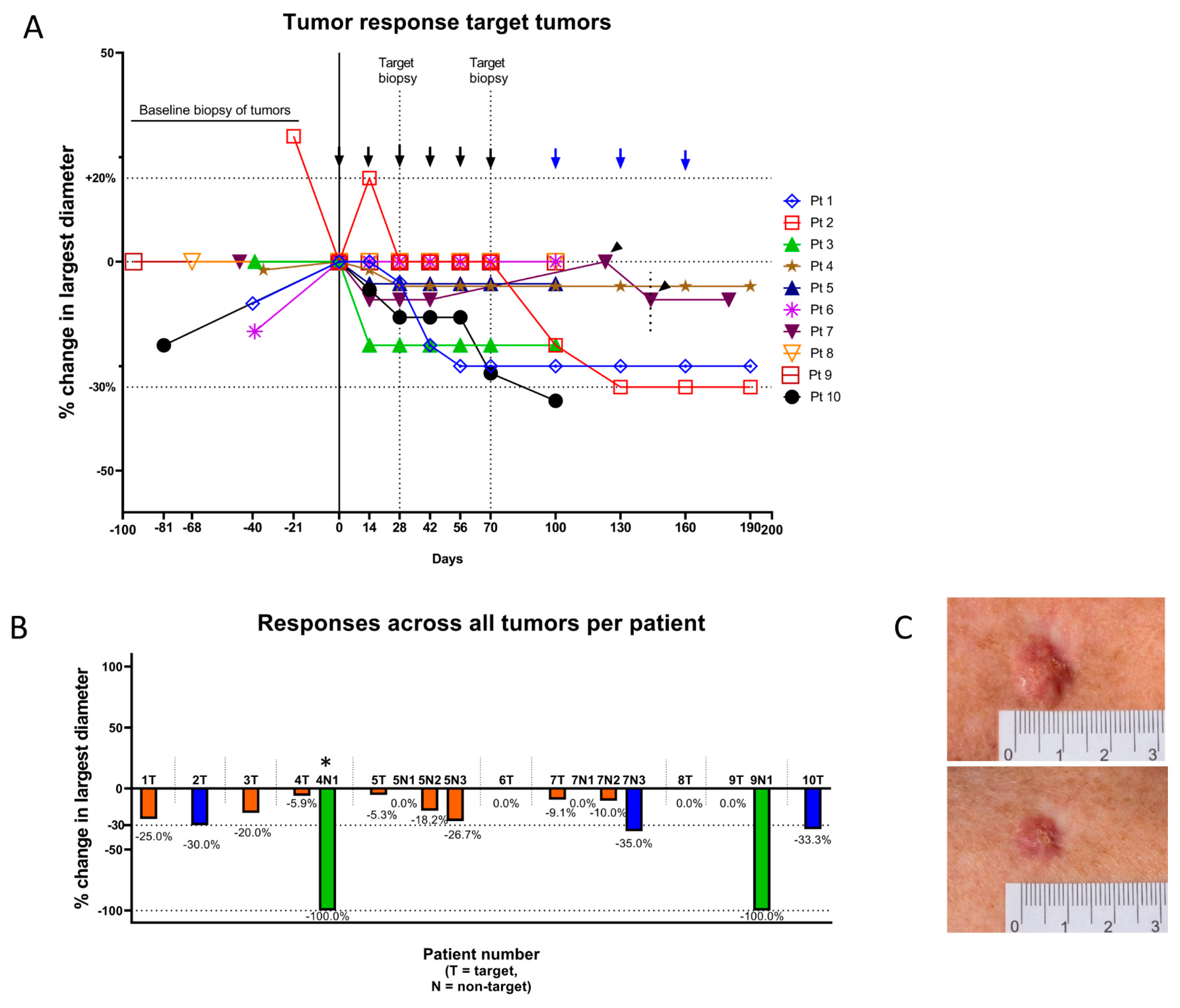
2.2.1. Target Tumors
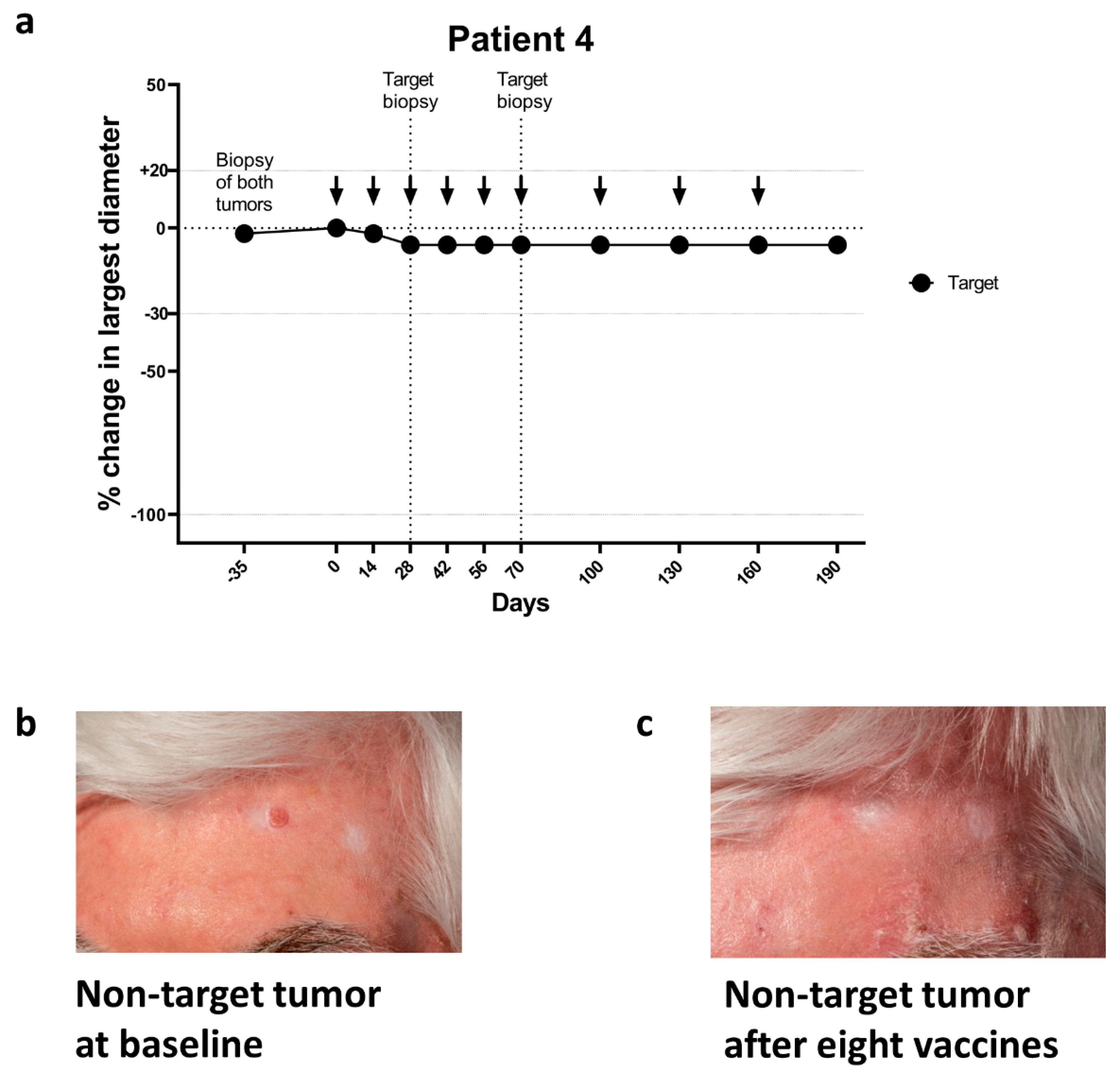
2.2.2. Non-Target Tumors
2.2.3. Overall Tumor Response
2.3. Adverse Events
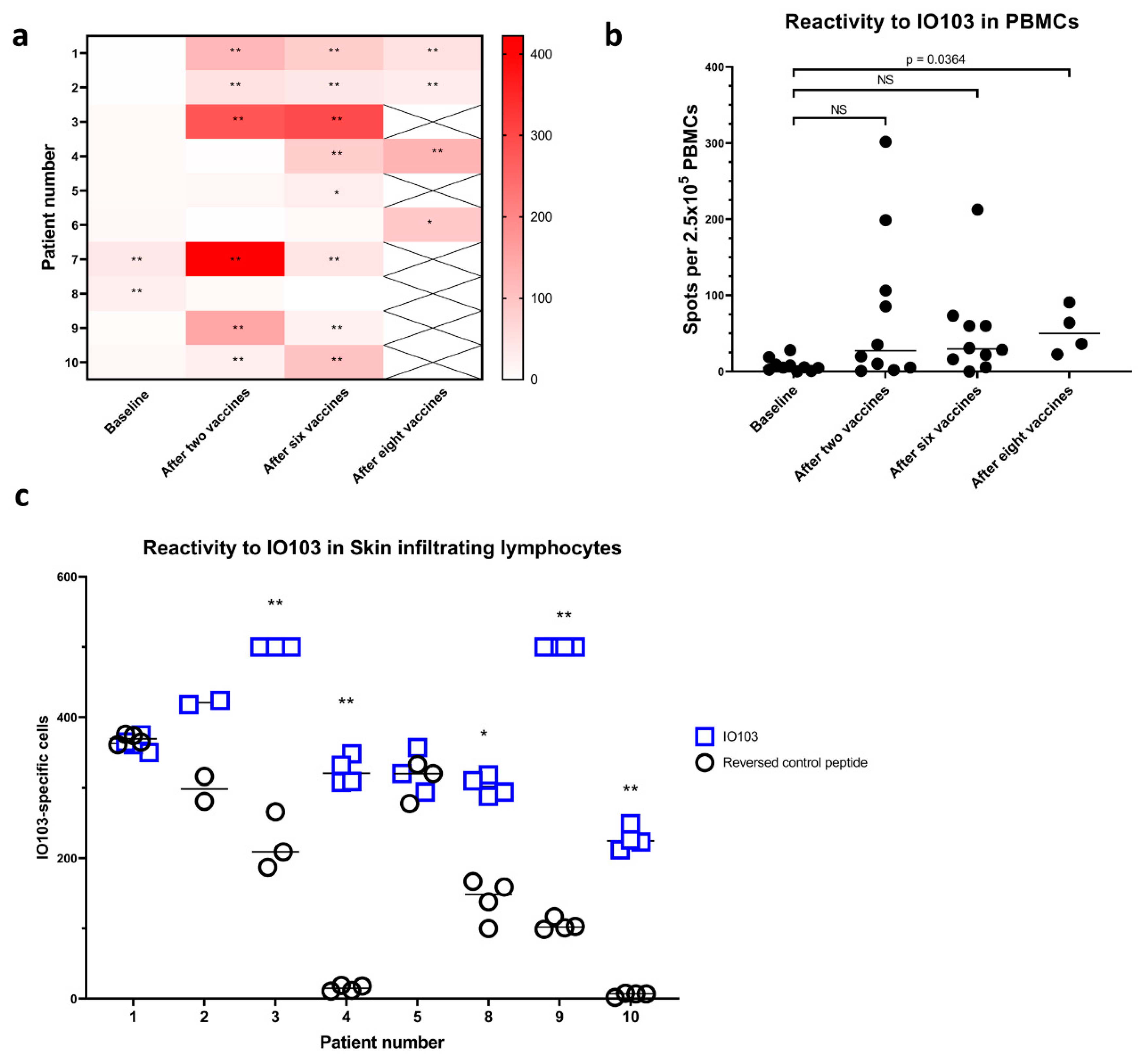
2.4. Vaccine-Specific Immune Responses in Blood
2.5. Immune Responses in Skin-Infiltrating Lymphocytes
2.6. Immune Phenotype in Peripheral Blood
2.7. Immunohistochemistry on BCC Biopsies
3. Discussion
4. Subjects and Methods
4.1. Study Design
4.2. Treatment
4.3. Clinical Evaluation
- Clinical response of the target BCC. Responses were defined as clearance: 100% reduction in tumor; partial response: 30–99% reduction in tumor; worsening: more than 20% increase in tumor; no response: none of the above.
- Disease control rate. Defined as the magnitude of reduction of the largest diameter of the target BCC after 6 treatments with IO103.
- Immune responses in biopsies from BCC after treatment with IO103.
- Immune responses in skin after delayed type hypersensitivity injections of IO103.
- Incidence of treatment emergent adverse events (safety and tolerability).
4.4. Tumor Biopsies
4.5. Blood Samples
4.6. Delayed Type Hypersensitivity and Skin Infiltrating Lymphocytes
4.7. IFNγ ELISpot Assay
4.8. Flow Cytometry on PBMCs
4.9. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BCC | Basal cell carcinoma |
| nBCC | Nodular basal cell carcinoma |
| sBCC | Superficial basal cell carcinoma |
| CR | Complete response |
| CTCAE | Common Terminology Criteria for Adverse Events |
| ELISPOT | Enzyme-linked immunospot |
| IFN-γ | Interferon gamma |
| IO103 | 19-amino acid peptide from PD-L1 |
| NC | No chance |
| PD-1 | Programmed death 1 |
| PD-L1 | Programmed death ligand 1 |
| Tregs | Regulatory T cells |
| PBMCs | Peripheral blood mononuclear cells |
| PI | Principal investigator |
| PR | Partial response |
References
- Lomas, A.; Leonardi-Bee, J.; Bath-Hextall, F. A systematic review of worldwide incidence of nonmelanoma skin cancer. Br. J. Dermatol. 2012, 1069–1080. [Google Scholar] [CrossRef]
- Lubeek, S.F.K.; Van Vugt, L.J.; Aben, K.K.H.; Van De Kerkhof, P.C.M.; Gerritsen, M.J.P. The epidemiology and clinicopathological features of basal cell carcinoma in patients 80 years and older a systematic review. JAMA Dermatol. Am. Med. Assoc. 2017, 71–78. [Google Scholar] [CrossRef]
- Peris, K.; Fargnoli, M.C.; Garbe, C.; Kaufmann, R.; Bastholt, L.; Seguin, N.B.; Bataille, V.; Del Marmol, V.; Dummer, R.; Harwood, C.A.; et al. Diagnosis and treatment of basal cell carcinoma: European consensus–based interdisciplinary guidelines. Eur. J. Cancer 2019, 118, 10–34. [Google Scholar] [CrossRef] [Green Version]
- Cannon, J.G.; Russell, J.S.; Kim, J.; Chang, A.L.S. A case of metastatic basal cell carcinoma treated with continuous PD-1 inhibitor exposure even after subsequent initiation of radiotherapy and surgery. JAAD Case Rep. 2018, 4, 248–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, J.; Zhu, G.A.; Cheung, C.; Li, S.; Kim, J.; Chang, A.L.S. Association between programmed death ligand 1 expression in pa-tients with basal cell carcinomas and the number of treatment modalities. JAMA Dermatol. 2017, 153, 285–290. [Google Scholar] [CrossRef]
- Goodman, A.M.; Kato, S.; Cohen, P.R.; Boichard, A.; Frampton, G.; Miller, V.; Stephens, P.J.; Daniels, G.A.; Kurzrock, R. Genomic landscape of advanced basal cell carcinoma: Implications for precision treatment with targeted and immune therapies. OncoImmunology 2018, 7, e1404217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ikeda, S.; Goodman, A.M.; Cohen, P.R.; Jensen, T.J.; Ellison, C.K.; Frampton, G.; Miller, V.; Patel, S.P.; Kurzrock, R. Metastatic basal cell carcinoma with amplifica-tion of PD-L1: Exceptional response to anti-PD1 therapy. NPJ Genom. Med. 2016, 1, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lipson, E.J.; Lilo, M.T.; Ogurtsova, A.; Esandrio, J.; Xu, H.; Brothers, P.; Schollenberger, M.; Sharfman, W.H.; Taube, J.M. Basal cell carcinoma: PD-L1/PD-1 checkpoint expression and tumor regression after PD-1 blockade. J. Immunother. Cancer 2017, 5, 23. [Google Scholar] [CrossRef] [Green Version]
- Winkler, J.K.; Schneiderbauer, R.; Bender, C.; Sedlaczek, O.; Fröhling, S.; Penzel, R.; Enk, A.; Hassel, J.C. Anti-programmed cell death-1 therapy in nonmelanoma skin cancer. Br. J. Dermatol. 2017, 176, 498–502. [Google Scholar] [CrossRef] [PubMed]
- Munir, S.; Andersen, G.H.; Met, Ö.; Donia, M.; Frøsig, T.M.; Larsen, S.K.; Klausen, T.W.; Svane, I.M.; Andersen, M.H. HLA-Restricted CTL That Are Specific for the Immune Checkpoint Ligand PD-L1 Occur with High Frequency in Cancer Patients. Cancer Res. 2013, 73, 1764–1776. [Google Scholar] [CrossRef] [Green Version]
- Ahmad, S.M.; Larsen, S.K.; Svane, I.M.; Andersen, M.H. Harnessing PD-L1-specific cytotoxic T cells for anti-leukemia immuno-therapy to defeat mechanisms of immune escape mediated by the PD-1 pathway. Leukemia 2013, 28, 236–238. [Google Scholar] [CrossRef] [PubMed]
- Holmström, M.O.; Riley, C.H.; Skov, V.; Svane, I.M.; Hasselbalch, H.C.; Andersen, M.H. Spontaneous T-cell responses against the immune check point programmed-death-ligand 1 (PD-L1) in patients with chronic myeloproliferative neoplasms correlate with disease stage and clinical response. OncoImmunology 2018, 7, e1433521. [Google Scholar] [CrossRef] [Green Version]
- Munir, S.; Andersen, G.H.; Svane, I.M.; Andersen, M.H. The immune checkpoint regulator PD-L1 is a specific target for naturally occurring CD4+ T cells. OncoImmunology 2013, 2, e23991. [Google Scholar] [CrossRef] [Green Version]
- Munir, S.; Andersen, G.H.; Woetmann, A.; Ødum, N.; Becker, J.C.; Andersen, M.H. Cutaneous T cell lymphoma cells are targets for immune checkpoint ligand PD-L1-specific, cytotoxic T cells. Leukemia 2013, 27, 2251–2253. [Google Scholar] [CrossRef]
- Jørgensen, N.G.; Klausen, U.; Grauslund, J.H.; Helleberg, C.; Aagaard, T.G.; Do, T.H.; Ahmad, S.M.; Olsen, L.R.; Klausen, T.W.; Breinholt, M.F.; et al. Peptide Vaccination Against PD-L1 with IO103 a Novel Immune Modulatory Vaccine in Multiple Myeloma: A Phase I First-in-Human Trial. Front. Immunol. 2020, 11, 2884. [Google Scholar] [CrossRef]
- de Vries, I.J.M.; Bernsen, M.R.; Lesterhuis, W.J.; Scharenborg, N.M.; Strijk, S.P.; Gerritsen, M.-J.P.; Ruiter, D.J.; Figdor, C.G.; Punt, C.J.A.; Adema, G.J. Immunomonitoring tumor-specific T cells in delayed-type hypersensitivity skin biopsies after dendritic cell vaccination correlates with clinical outcome. J. Clin. Oncol. 2005, 23, 5779–5787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aarntzen, E.H.; Bol, K.; Schreibelt, G.; Jacobs, J.F.; Lesterhuis, W.J.; Van Rossum, M.M.; Adema, G.J.; Figdor, C.G.; Punt, C.J.; De Vries, I.J.M.; et al. Skin-Test Infiltrating Lymphocytes Early Predict Clinical Outcome of Dendritic Cell–Based Vaccination in Metastatic Melanoma. Cancer Res. 2012, 72, 6102–6110. [Google Scholar] [CrossRef] [Green Version]
- Fujimura, T.; Kakizaki, A.; Kambayashi, Y.; Aiba, S. Basal cell carcinoma with spontaneous regression: A case report and im-munohistochemical study. Case Rep. Dermatol. 2012, 4, 125–132. [Google Scholar] [CrossRef]
- Hunt, M.; Halliday, G.; Weedon, D.; Cooke, B.; Barnetson, R.S. Regression in basal cell carcinoma: An immunohistochemical analysis. Br. J. Dermatol. 1994, 130, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Wong, D.; Bishop, G.; Lowes, M.; Cooke, B.; Barnetson, R.; Halliday, G. Cytokine profiles in spontaneously regressing basal cell carcinomas. Br. J. Dermatol. 2000, 143, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Kelley, R.S.; Wagner, R.F.; Sanchez, R.L.; Duff, R.R. Complete Spontaneous Regression of Multiple Basal Cell Carcinomas in the Basal Cell Nevus Syndrome: The Possible Role of Transepithelial Elimination. J. Dermatol. Surg. Oncol. 1990, 16, 1039–1042. [Google Scholar] [CrossRef]
- Jemec, G.B.; Holm, E.A. Nonmelanoma skin cancer in organ transplant patients. Transplantation 2003, 75, 253–257. [Google Scholar] [CrossRef]
- Goodman, A.M.; Kato, S.; Bazhenova, L.; Patel, S.P.; Frampton, G.M.; Miller, V.; Stephens, P.J.; Daniels, G.A.; Kurzrock, R. Tumor Mutational Burden as an Independent Predictor of Response to Immunotherapy in Diverse Cancers. Mol. Cancer Ther. 2017, 16, 2598–2608. [Google Scholar] [CrossRef] [Green Version]
- Jayaraman, S.S.; Rayhan, D.J.; Hazany, S.; Kolodney, M.S. Mutational landscape of basal cell carcinomas by whole-exome se-quencing. J. Investig. Dermatol. 2014, 134, 213–220. [Google Scholar] [CrossRef] [Green Version]
- Kjeldsen, J.W.; Lorentzen, C.L.; Martinenaite, E.; Andersen, M.H.; Svane, I.M. Clinical efficacy and immunity of combination ther-apy with nivolumab and IDO/PD-L1 peptide vaccine in patients with metastatic melanoma: A phase I/II trial. Ann. Oncol. 2020, 31, S1176. [Google Scholar]
- Zemelman, V.; Silva, P.; Sazunic, I. Basal cell carcinoma: Analysis of regression after incomplete excision. Clin. Exp. Dermatol. 2009, 34, e425. [Google Scholar] [CrossRef] [PubMed]
- Dey, S.; Sutanto-Ward, E.; Kopp, K.L.; Duhadaway, J.; Mondal, A.; Ghaban, D.; Lecoq, I.; Zocca, M.-B.; Merlo, L.M.F.; Mandik-Nayak, L.; et al. Peptide vaccination directed against IDO1-expressing immune cells elicits CD8+ and CD4+ T-cell-mediated antitumor immunity and enhanced anti-PD1 responses. J. Immunother. Cancer 2020, 8, e000605. [Google Scholar] [CrossRef] [PubMed]
- Ascarateil, S.; Puget, A.; Koziol, M.-E. Safety data of Montanide ISA 51 VG and Montanide ISA 720 VG, two adjuvants dedicated to human therapeutic vaccines. J. Immunother. Cancer 2015, 3, P428. [Google Scholar] [CrossRef] [Green Version]
- Dreno, B.; Basset-Seguin, N.; Caro, I.; Yue, H.; Schadendorf, D. Clinical Benefit Assessment of Vismodegib Therapy in Patients with Advanced Basal Cell Carcinoma. Oncologist 2014, 19, 790–796. [Google Scholar] [CrossRef] [Green Version]
- Sekulic, A.; Migden, M.R.; Oro, A.E.; Dirix, L.; Lewis, K.D.; Hainsworth, J.D.; Solomon, J.A.; Yoo, S.; Arron, S.T.; Friedlander, P.A.; et al. Efficacy and Safety of Vismodegib in Advanced Basal-Cell Carcinoma. N. Engl. J. Med. 2012, 366, 2171–2179. [Google Scholar] [CrossRef] [Green Version]
- McCutcheon, M.; Wehner, N.; Wensky, A.; Kushner, M.; Doan, S.; Hsiao, L.; Calabresi, P.; Ha, T.; Tran, T.; Tate, K.; et al. A sensitive ELISPOT assay to detect low-frequency human T lymphocytes. J. Immunol. Methods 1997, 210, 149–166. [Google Scholar] [CrossRef]
- Moodie, Z.; Price, L.; Janetzki, S.; Britten, C.M. Response Determination Criteria for ELISPOT: Toward a Standard that Can Be Applied Across Laboratories. Methods Mol. Biol. 2012, 185–196. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ID | Sex | Age | Previous Skin Cancer | Co-Morbidity | Immuno-Suppressive Medications |
|---|---|---|---|---|---|
| 1 | Male | 50 | BCC × 33. Superficial MM × 1 | BRCA-1 and BRCA-2 mutatet, Apoplexia cerebri, Retinal detachment, Malignant melanoma, Thyroiditis, Diabetes type II, Folliculitis decalvans, Hypercholesterolemia, Hypertension | None |
| 2 | Female | 47 | None | None | None |
| 3 | Female | 56 | None | Hypertension | None |
| 4 | Male | 73 | BCC × 5 | Age-related macular degeneration (AMD), Allergic hand eczema | Methotrexate 15 mg weekly |
| 5 | Female | 69 | None | Psoriasis | None |
| 6 | Male | 76 | None | Porokeratosis | None |
| 7 | Female | 56 | None | Slipped disk | None |
| 8 | Male | 59 | None | Hypertension, Psoriasis, C. prostatea operata | Methotrexate 15 mg weekly |
| 9 | Male | 73 | BCC × 29 | Hypertension | None |
| 10 | Male | 72 | BCC × 2 | Hypertension | None |
| ID | Target Tumor Location | Target Tumor Type (Longest Diameter, mm) | Target, Clinical Response | Target, Change (%) | ELISPOT Response to IO103 in PBMCs | ELISPOT Response to IO103 in SKILs |
|---|---|---|---|---|---|---|
| 1 | Shoulder | sBCC (20) | NC | −25 | ** | High Background |
| 2 | Chest | sBCC (10) | PR | −30 | ** | 0 |
| 3 | Upper arm | nBCC (25) | NC | −20 | ** | ** |
| 4 | Lower leg | sBCC (51) | NC | −5.9 | ** | ** |
| 5 | Back | sBCC (19) | NC | −5.3 | * | High Background |
| 6 | Chest | nBCC (18) | NC | 0 | * | NA |
| 7 | Back | sBCC (22) | NC | −9.1 | ** | NA |
| 8 | Shoulder | nBCC (14) | NC | 0 | 0 | * |
| 9 | Back | sBCC (20) | NC | 0 | ** | ** |
| 10 | Shoulder | nBCC (15) | PR | −33 | ** | ** |
| ID | Non-Target BCCs n (Longest Diameter, mm) | Non-Target, Clinical Response | Non-Target, Change (%) |
|---|---|---|---|
| 4 | 1 (not measured) | CR | −100 |
| 5 | 3 (15, 13, 11) | NC | 0 |
| NC | −18.2 | ||
| NC | −26.7 | ||
| 7 | 3 (20, 12, 10) | NC | 0 |
| NC | −10 | ||
| PR | −35 | ||
| 9 | 1 (6) | CR | −100 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jørgensen, N.G.; Kaae, J.; Grauslund, J.H.; Met, Ö.; Nielsen, S.L.; Pedersen, A.W.; Svane, I.M.; Ehrnrooth, E.; Andersen, M.H.; Zachariae, C.; et al. Vaccination against PD-L1 with IO103 a Novel Immune Modulatory Vaccine in Basal Cell Carcinoma: A Phase IIa Study. Cancers 2021, 13, 911. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13040911
Jørgensen NG, Kaae J, Grauslund JH, Met Ö, Nielsen SL, Pedersen AW, Svane IM, Ehrnrooth E, Andersen MH, Zachariae C, et al. Vaccination against PD-L1 with IO103 a Novel Immune Modulatory Vaccine in Basal Cell Carcinoma: A Phase IIa Study. Cancers. 2021; 13(4):911. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13040911
Chicago/Turabian StyleJørgensen, Nicolai Grønne, Jeanette Kaae, Jacob Handlos Grauslund, Özcan Met, Signe Ledou Nielsen, Ayako Wakatsuki Pedersen, Inge Marie Svane, Eva Ehrnrooth, Mads Hald Andersen, Claus Zachariae, and et al. 2021. "Vaccination against PD-L1 with IO103 a Novel Immune Modulatory Vaccine in Basal Cell Carcinoma: A Phase IIa Study" Cancers 13, no. 4: 911. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13040911