
Stereotactic Body Radiotherapy for Patients with Lung Oligometastatic Disease: A Five-Year Systematic Review


Abstract
:Simple Summary
Abstract
1. Introduction
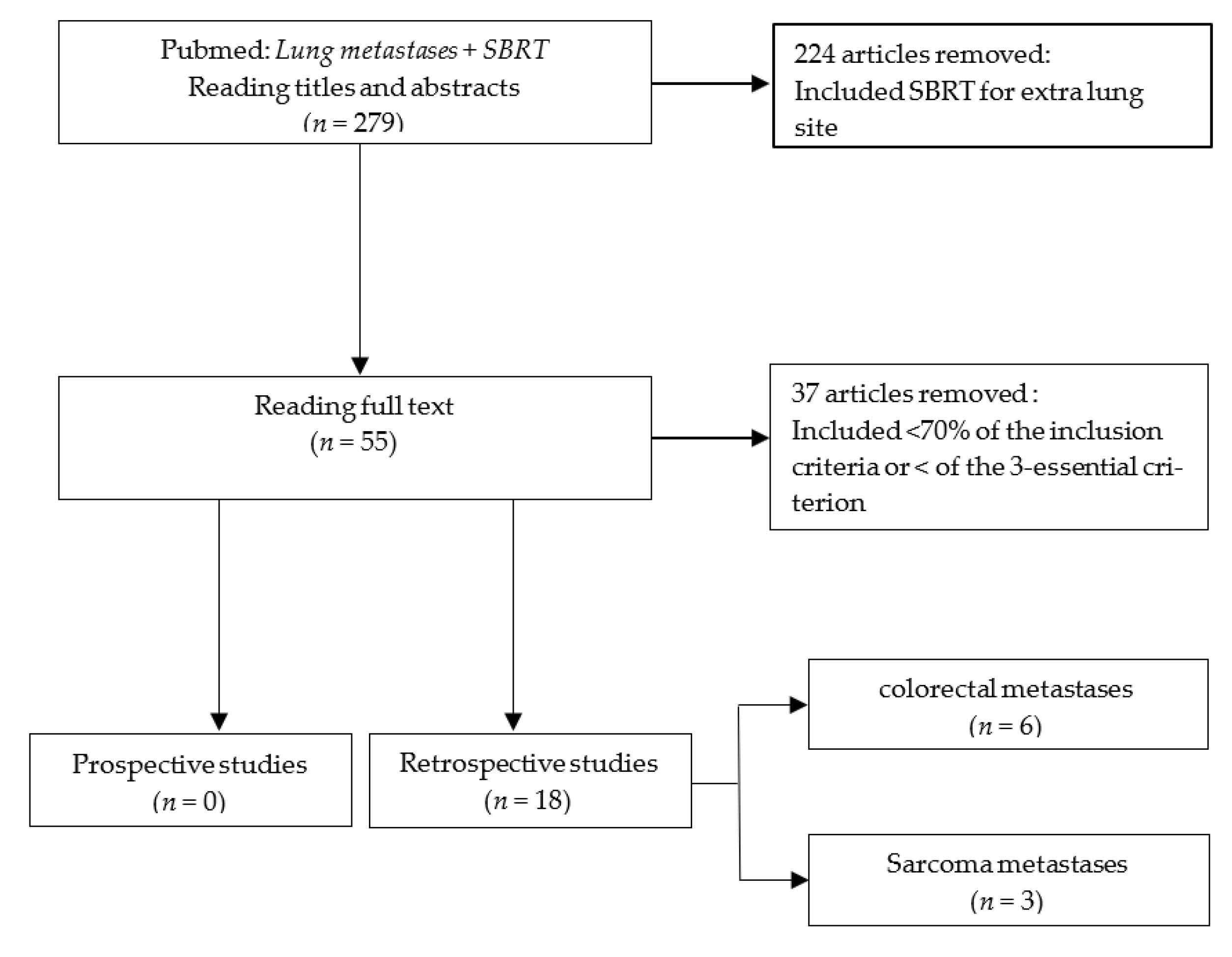
2. Materials and Methods
3. Results
3.1. Patient Population
3.2. Primary Cancer and Time to SBRT
3.3. SBRT Technique
3.3.1. Set-Up
3.3.2. Radiation Therapy Prescription
3.3.3. Technique of Irradiation
3.4. Follow-Up and Evaluation after SBRT
3.4.1. Evaluation
3.4.2. Outcome
3.4.3. Complications
3.5. Prognostic Factors
3.5.1. Demographic Factors
3.5.2. Tumor Size
3.5.3. Number of Thoracic Metastasis Lesions
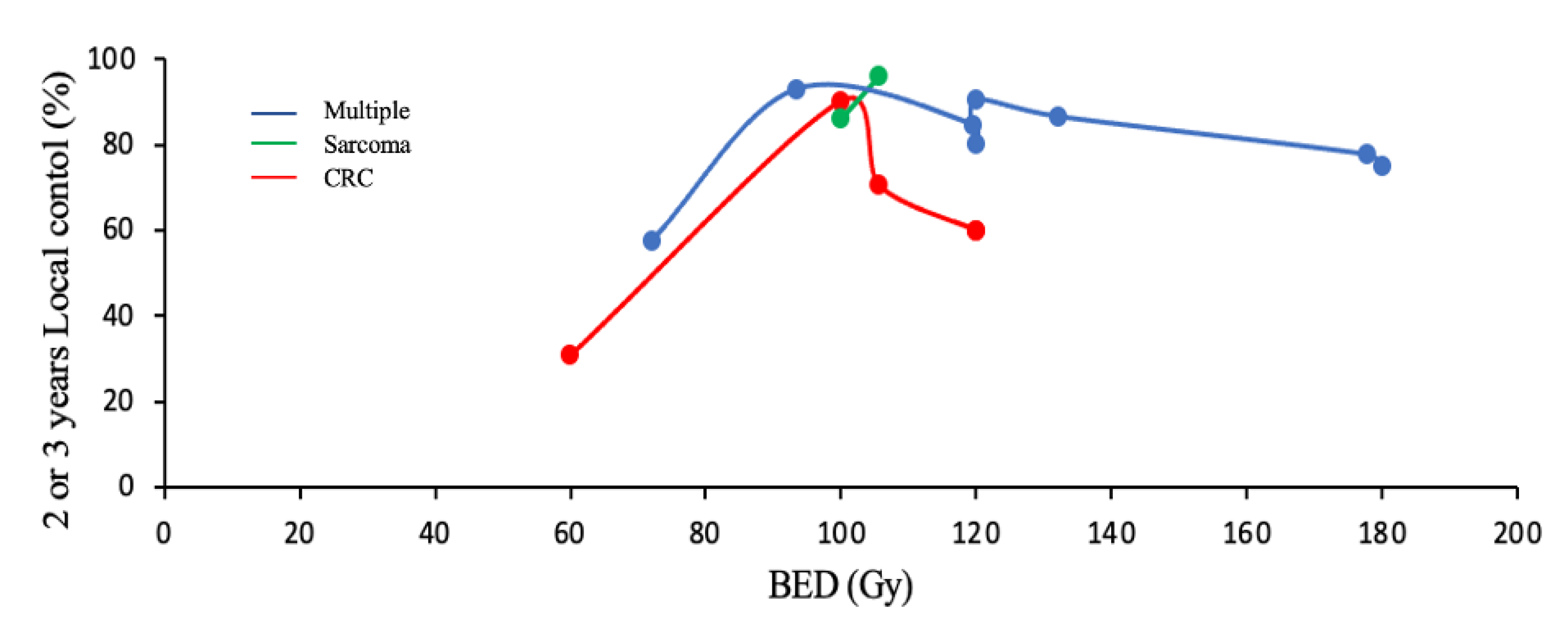
3.5.4. Biological Effective Dose (BED)
3.5.5. Fractionation of SBRT
3.5.6. Time to SBRT
3.5.7. Combination with Chemotherapy
3.5.8. Primary Colorectal Cancer
3.6. Prognostic Factors of Specific Histologies
3.6.1. Colorectal
3.6.2. Sarcomas
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Hellman, S.; Weichselbaum, R.R. Oligometastases. J. Clin. Oncol. 1995, 13, 8–10. [Google Scholar] [CrossRef]
- Palma, D.A.; Olson, R.; Harrow, S.; Gaede, S.; Louie, A.V.; Haasbeek, C.; Mulroy, L.; Lock, M.; Rodrigues, G.B.; Yaremko, B.P.; et al. Stereotactic Ablative Radiotherapy versus Standard of Care Palliative Treatment in Patients with Oligometastatic Cancers (SABR-COMET): A Randomised, Phase 2, Open-Label Trial. Lancet 2019, 393, 2051–2058. [Google Scholar] [CrossRef]
- Ashworth, A.B.; Senan, S.; Palma, D.A.; Riquet, M.; Ahn, Y.C.; Ricardi, U.; Congedo, M.T.; Gomez, D.R.; Wright, G.M.; Melloni, G.; et al. An Individual Patient Data Metaanalysis of Outcomes and Prognostic Factors After Treatment of Oligometastatic Non–Small-Cell Lung Cancer. Clin. Lung Cancer 2014, 15, 346–355. [Google Scholar] [CrossRef]
- Annede, P.; Chargari, C. Oligométastases et oligoprogressions: Concepts et histoire naturelle. Cancer/Radiothérapie 2019, 23, 475–481. [Google Scholar] [CrossRef]
- Fong, Y.; Cohen, A.M.; Fortner, J.G.; Enker, W.E.; Turnbull, A.D.; Coit, D.G.; Marrero, A.M.; Prasad, M.; Blumgart, L.H.; Brennan, M.F. Liver Resection for Colorectal Metastases. J. Clin. Oncol. 1997, 15, 938–946. [Google Scholar] [CrossRef]
- Timmerman, R.D.; Bizekis, C.S.; Pass, H.I.; Fong, Y.; Dupuy, D.E.; Dawson, L.A.; Lu, D. Local Surgical, Ablative, and Radiation Treatment of Metastases. CA Cancer J. Clin. 2009, 59, 145–170. [Google Scholar] [CrossRef]
- Gomez, D.R.; Blumenschein, G.R.; Lee, J.J.; Hernandez, M.; Ye, R.; Camidge, D.R.; Doebele, R.C.; Skoulidis, F.; Gaspar, L.E.; Gibbons, D.L.; et al. Local Consolidative Therapy versus Maintenance Therapy or Observation for Patients with Oligometastatic Non-Small-Cell Lung Cancer without Progression after First-Line Systemic Therapy: A Multicentre, Randomised, Controlled, Phase 2 Study. Lancet Oncol. 2016, 17, 1672–1682. [Google Scholar] [CrossRef] [Green Version]
- Treasure, T.; Milošević, M.; Fiorentino, F.; Macbeth, F. Pulmonary Metastasectomy: What Is the Practice and Where Is the Evidence for Effectiveness? Thorax 2014, 69, 946–949. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brunelli, A.; Charloux, A.; Bolliger, C.T.; Rocco, G.; Sculier, J.-P.; Varela, G.; Licker, M.; Ferguson, M.K.; Faivre-Finn, C.; Huber, R.M.; et al. ERS/ESTS Clinical Guidelines on Fitness for Radical Therapy in Lung Cancer Patients (Surgery and Chemo-Radiotherapy). Eur. Respir. J. 2009, 34, 17–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pastorino, U.; Buyse, M.; Friedel, G.; Ginsberg, R.J.; Girard, P.; Goldstraw, P.; Johnston, M.; McCormack, P.; Pass, H.; Putnam, J.B.; et al. Long-Term Results of Lung Metastasectomy: Prognostic Analyses Based on 5206 Cases. J. Thorac. Cardiovasc. Surg. 1997, 113, 37–49. [Google Scholar] [CrossRef] [Green Version]
- Brunelli, A.; Kim, A.W.; Berger, K.I.; Addrizzo-Harris, D.J. Physiologic Evaluation of the Patient with Lung Cancer Being Considered for Resectional Surgery: Diagnosis and Management of Lung Cancer, 3rd Ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2013, 143, e166S–e190S. [Google Scholar] [CrossRef] [Green Version]
- Chang, J.Y.; Senan, S.; Paul, M.A.; Mehran, R.J.; Louie, A.V.; Balter, P.; Groen, H.J.M.; McRae, S.E.; Widder, J.; Feng, L.; et al. Stereotactic Ablative Radiotherapy versus Lobectomy for Operable Stage I Non-Small-Cell Lung Cancer: A Pooled Analysis of Two Randomised Trials. Lancet Oncol. 2015, 16, 630–637. [Google Scholar] [CrossRef] [Green Version]
- Lagerwaard, F.J.; Haasbeek, C.J.A.; Smit, E.F.; Slotman, B.J.; Senan, S. Outcomes of Risk-Adapted Fractionated Stereotactic Radiotherapy for Stage I Non–Small-Cell Lung Cancer. Int. J. Radiat. Oncol. 2008, 70, 685–692. [Google Scholar] [CrossRef]
- Menoux, I.; Antoni, D.; Truntzer, P.; Keller, A.; Massard, G.; Noël, G. Stereotactic Body Radiation Therapy for Stage I Non-Small Cell Lung Carcinomas: Moderate Hypofractionation Optimizes Outcome. Lung Cancer Amst. Neth. 2018, 126, 201–207. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Healthcare Interventions: Explanation and Elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- Qiu, H.; Katz, A.W.; Chowdhry, A.K.; Usuki, K.Y.; Singh, D.P.; Metcalfe, S.; Cheruvu, P.; Chen, Y.; Okunieff, P.; Milano, M.T. Stereotactic Body Radiotherapy for Lung Metastases from Colorectal Cancer: Prognostic Factors for Disease Control and Survival. Am. J. Clin. Oncol. 2018, 41, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Osti, M.F.; Agolli, L.; Valeriani, M.; Reverberi, C.; Bracci, S.; Marinelli, L.; De Sanctis, V.; Cortesi, E.; Martelli, M.; De Dominicis, C.; et al. 30 Gy Single Dose Stereotactic Body Radiation Therapy (SBRT): Report on Outcome in a Large Series of Patients with Lung Oligometastatic Disease. Lung Cancer Amst. Neth. 2018, 122, 165–170. [Google Scholar] [CrossRef]
- García-Cabezas, S.; Bueno, C.; Rivin, E.; Roldán, J.M.; Palacios-Eito, A. Lung Metastases in Oligometastatic Patients: Outcome with Stereotactic Body Radiation Therapy (SBRT). Clin. Transl. Oncol. 2015, 17, 668–672. [Google Scholar] [CrossRef] [PubMed]
- Helou, J.; Thibault, I.; Poon, I.; Chiang, A.; Jain, S.; Soliman, H.; Erler, D.; Yeung, L.; Cheung, P. Stereotactic Ablative Radiation Therapy for Pulmonary Metastases: Histology, Dose, and Indication Matter. Int. J. Radiat. Oncol. Biol. Phys. 2017, 98, 419–427. [Google Scholar] [CrossRef]
- Filippi, A.R.; Badellino, S.; Ceccarelli, M.; Guarneri, A.; Franco, P.; Monagheddu, C.; Spadi, R.; Ragona, R.; Racca, P.; Ricardi, U. Stereotactic Ablative Radiation Therapy as First Local Therapy for Lung Oligometastases from Colorectal Cancer: A Single-Institution Cohort Study. Int. J. Radiat. Oncol. Biol. Phys. 2015, 91, 524–529. [Google Scholar] [CrossRef] [PubMed]
- Navarria, P.; Ascolese, A.M.; Cozzi, L.; Tomatis, S.; D’Agostino, G.R.; De Rose, F.; De Sanctis, R.; Marrari, A.; Santoro, A.; Fogliata, A.; et al. Stereotactic Body Radiation Therapy for Lung Metastases from Soft Tissue Sarcoma. Eur. J. Cancer 2015, 51, 668–674. [Google Scholar] [CrossRef]
- Li, S.; Dong, D.; Geng, J.; Zhu, X.; Shi, C.; Zhang, Y.; Wang, H.; Zhou, S.; Wu, H.; Cai, Y.; et al. Prognostic Factors and Optimal Response Interval for Stereotactic Body Radiotherapy in Patients with Lung Oligometastases or Oligoprogression from Colorectal Cancer. Front. Oncol. 2019, 9, 1080. [Google Scholar] [CrossRef] [Green Version]
- Sharma, A.; Duijm, M.; Oomen-de Hoop, E.; Aerts, J.G.; Verhoef, C.; Hoogeman, M.; Nuyttens, J.J. Factors Affecting Local Control of Pulmonary Oligometastases Treated with Stereotactic Body Radiotherapy. Acta Oncol. 2018, 57, 1031–1037. [Google Scholar] [CrossRef] [Green Version]
- Berkovic, P.; Gulyban, A.; Defraene, G.; Swenen, L.; Dechambre, D.; Nguyen, P.V.; Jansen, N.; Mievis, C.; Lovinfosse, P.; Janvary, L.; et al. Stereotactic Robotic Body Radiotherapy for Patients with Oligorecurrent Pulmonary Metastases. BMC Cancer 2020, 20. [Google Scholar] [CrossRef] [PubMed]
- Agolli, L.; Bracci, S.; Nicosia, L.; Valeriani, M.; De Sanctis, V.; Osti, M.F. Lung Metastases Treated With Stereotactic Ablative Radiation Therapy in Oligometastatic Colorectal Cancer Patients: Outcomes and Prognostic Factors After Long-Term Follow-Up. Clin. Colorectal Cancer 2017, 16, 58–64. [Google Scholar] [CrossRef]
- Jung, J.; Song, S.Y.; Kim, J.H.; Yu, C.S.; Kim, J.C.; Kim, T.W.; Jeong, S.-Y.; Kim, S.S.; Choi, E.K. Clinical Efficacy of Stereotactic Ablative Radiotherapy for Lung Metastases Arising from Colorectal Cancer. Radiat. Oncol. 2015, 10, 238. [Google Scholar] [CrossRef] [Green Version]
- Siva, S.; Kirby, K.; Caine, H.; Pham, D.; Kron, T.; Te Marvelde, L.; Whalley, D.; Stevens, M.J.; Foroudi, F.; MacManus, M.; et al. Comparison of Single-Fraction and Multi-Fraction Stereotactic Radiotherapy for Patients with 18F-Fluorodeoxyglucose Positron Emission Tomography-Staged Pulmonary Oligometastases. Clin. Oncol. 2015, 27, 353–361. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.H.; Kang, K.M.; Choi, H.-S.; Ha, I.B.; Jeong, H.; Song, J.H.; Jang, I.-S.; Kim, S.H.; Lee, J.W.; Rhee, D.Y.; et al. Comparison of Stereotactic Body Radiotherapy versus Metastasectomy Outcomes in Patients with Pulmonary Metastases. Thorac. Cancer 2018, 9, 1671–1679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Z.; Kong, Q.-T.; Li, J.; Wu, X.-H.; Li, B.; Shen, Z.-T.; Zhu, X.-X.; Song, Y. Clinical Outcomes of Cyberknife Stereotactic Radiosurgery for Lung Metastases. J. Thorac. Dis. 2015, 7, 407–412. [Google Scholar] [CrossRef]
- Baumann, B.C.; Nagda, S.N.; Kolker, J.D.; Levin, W.P.; Weber, K.L.; Berman, A.T.; Staddon, A.; Hartner, L.; Hahn, S.M.; Glatstein, E.; et al. Efficacy and Safety of Stereotactic Body Radiation Therapy for the Treatment of Pulmonary Metastases from Sarcoma: A Potential Alternative to Resection. J. Surg. Oncol. 2016, 114, 65–69. [Google Scholar] [CrossRef]
- Lischalk, J.W.; Malik, R.M.; Collins, S.P.; Collins, B.T.; Matus, I.A.; Anderson, E.D. Stereotactic Body Radiotherapy (SBRT) for High-Risk Central Pulmonary Metastases. Radiat. Oncol. 2016, 11, 28. [Google Scholar] [CrossRef] [Green Version]
- Pasqualetti, F.; Montrone, S.; Vivaldi, C.; Zani, M.; Fedele, D.; Fornaro, L.; Pasqualetti, G.; Salvatore, L.; Manfredi, B.; Laliscia, C.; et al. Stereotactic Body Radiotherapy in Patients with Lung Oligometastases from Colorectal Cancer. Anticancer Res. 2017, 37, 315–319. [Google Scholar] [CrossRef] [Green Version]
- Lindsay, A.D.; Haupt, E.E.; Chan, C.M.; Spiguel, A.R.; Scarborough, M.T.; Zlotecki, R.A.; Gibbs, P.C. Treatment of Sarcoma Lung Metastases with Stereotactic Body Radiotherapy. Sarcoma 2018, 2018. [Google Scholar] [CrossRef] [Green Version]
- Lewis, S.L.; Porceddu, S.; Nakamura, N.; Palma, D.A.; Lo, S.S.; Hoskin, P.; Moghanaki, D.; Chmura, S.J.; Salama, J.K. Definitive Stereotactic Body Radiotherapy (SBRT) for Extracranial Oligometastases. Am. J. Clin. Oncol. 2017, 40, 418–422. [Google Scholar] [CrossRef]
- Hof, H.; Hoess, A.; Oetzel, D.; Debus, J.; Herfarth, K. Stereotactic Single-Dose Radiotherapy of Lung Metastases. Strahlenther. Onkol. 2007, 183, 673–678. [Google Scholar] [CrossRef]
- Norihisa, Y.; Nagata, Y.; Takayama, K.; Matsuo, Y.; Sakamoto, T.; Sakamoto, M.; Mizowaki, T.; Yano, S.; Hiraoka, M. Stereotactic Body Radiotherapy for Oligometastatic Lung Tumors. Int. J. Radiat. Oncol. 2008, 72, 398–403. [Google Scholar] [CrossRef] [PubMed]
- Alongi, F.; Mazzola, R.; Figlia, V.; Guckenberger, M. Stereotactic Body Radiotherapy for Lung Oligometastases: Literature Review According to PICO Criteria. Tumori J. 2018, 104, 148–156. [Google Scholar] [CrossRef] [PubMed]
- Scher, N.; Bollet, M.; Bouilhol, G.; Tannouri, R.; Khemiri, I.; Vouillaume, A.; Sellami, N.; Von Eyben, R.; Vannetzel, J.-M.; Darmon, I.; et al. Safety and Efficacy of Fiducial Marker Implantation for Robotic Stereotactic Body Radiation Therapy with Fiducial Tracking. Radiat. Oncol. 2019, 14, 167. [Google Scholar] [CrossRef] [PubMed]
- Keall, P.J.; Starkschall, G.; Shukla, H.; Forster, K.M.; Ortiz, V.; Stevens, C.W.; Vedam, S.S.; George, R.; Guerrero, T.; Mohan, R. Acquiring 4D Thoracic CT Scans Using a Multislice Helical Method. Phys. Med. Biol. 2004, 49, 2053–2067. [Google Scholar] [CrossRef]
- Onishi, H.; Shirato, H.; Nagata, Y.; Hiraoka, M.; Fujino, M.; Gomi, K.; Niibe, Y.; Karasawa, K.; Hayakawa, K.; Takai, Y.; et al. Hypofractionated Stereotactic Radiotherapy (HypoFXSRT) for Stage I Non-Small Cell Lung Cancer: Updated Results of 257 Patients in a Japanese Multi-Institutional Study. J. Thorac. Oncol. 2007, 2, S94–S100. [Google Scholar] [CrossRef] [Green Version]
- Mazzola, R.; Tebano, U.; Aiello, D.; Paola, G.D.; Giaj-Levra, N.; Ricchetti, F.; Fersino, S.; Fiorentino, A.; Ruggieri, R.; Alongi, F. Increased Efficacy of Stereotactic Ablative Radiation Therapy after Bevacizumab in Lung Oligometastases from Colon Cancer. Tumori J. 2018, 104, 423–428. [Google Scholar] [CrossRef]
- Rusthoven, K.E.; Kavanagh, B.D.; Burri, S.H.; Chen, C.; Cardenes, H.; Chidel, M.A.; Pugh, T.J.; Kane, M.; Gaspar, L.E.; Schefter, T.E. Multi-Institutional Phase I/II Trial of Stereotactic Body Radiation Therapy for Lung Metastases. J. Clin. Oncol. 2009, 27, 1579–1584. [Google Scholar] [CrossRef]
- Chen, H.; Laba, J.M.; Zayed, S.; Boldt, R.G.; Palma, D.A.; Louie, A.V. Safety and Effectiveness of Stereotactic Ablative Radiotherapy for Ultra-Central Lung Lesions: A Systematic Review. J. Thorac. Oncol. 2019, 14, 1332–1342. [Google Scholar] [CrossRef] [PubMed]
- Bezjak, A.; Paulus, R.; Gaspar, L.E.; Timmerman, R.D.; Straube, W.L.; Ryan, W.F.; Garces, Y.I.; Pu, A.T.; Singh, A.K.; Videtic, G.M.; et al. Safety and Efficacy of a Five-Fraction Stereotactic Body Radiotherapy Schedule for Centrally Located Non–Small-Cell Lung Cancer: NRG Oncology/RTOG 0813 Trial. J. Clin. Oncol. 2019, 37, 1316–1325. [Google Scholar] [CrossRef] [PubMed]
- Mazzola, R.; Ruggieri, R.; Figlia, V.; Rigo, M.; Giaj Levra, N.; Ricchetti, F.; Nicosia, L.; Corradini, S.; Alongi, F. Stereotactic Body Radiotherapy of Central Lung Malignancies Using a Simultaneous Integrated Protection Approach: A Prospective Observational Study. Strahlenther. Onkol. 2019, 195, 719–724. [Google Scholar] [CrossRef] [PubMed]
- Lo, S.S.; Moffatt-Bruce, S.D.; Dawson, L.A.; Schwarz, R.E.; Teh, B.S.; Mayr, N.A.; Lu, J.J.; Grecula, J.C.; Olencki, T.E.; Timmerman, R.D. The Role of Local Therapy in the Management of Lung and Liver Oligometastases | Nature Reviews Clinical Oncology. Available online: https://0-www-nature-com.brum.beds.ac.uk/articles/nrclinonc.2011.75?proof=trueJul (accessed on 19 July 2020).
- Weichselbaum, R.R.; Hellman, S. Oligometastases Revisited. Nat. Rev. Clin. Oncol. 2011, 8, 378–382. [Google Scholar] [CrossRef] [PubMed]
- Guckenberger, M.; Lievens, Y.; Bouma, A.B.; Collette, L.; Dekker, A.; deSouza, N.M.; Dingemans, A.-M.C.; Fournier, B.; Hurkmans, C.; Lecouvet, F.E.; et al. Characterisation and Classification of Oligometastatic Disease: A European Society for Radiotherapy and Oncology and European Organisation for Research and Treatment of Cancer Consensus Recommendation. Lancet Oncol. 2020, 21, e18–e28. [Google Scholar] [CrossRef] [Green Version]
- Basler, L.; Kroeze, S.G.C.; Guckenberger, M. SBRT for Oligoprogressive Oncogene Addicted NSCLC. Lung Cancer 2017, 106, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Uppal, A.; Ferguson, M.K.; Posner, M.C.; Hellman, S.; Khodarev, N.N.; Weichselbaum, R.R. Towards a Molecular Basis of Oligometastatic Disease: Potential Role of Micro-RNAs. Clin. Exp. Metastasis 2014, 31, 735–748. [Google Scholar] [CrossRef] [Green Version]
- Lussier, Y.A.; Xing, H.R.; Salama, J.K.; Khodarev, N.N.; Huang, Y.; Zhang, Q.; Khan, S.A.; Yang, X.; Hasselle, M.D.; Darga, T.E.; et al. MicroRNA Expression Characterizes Oligometastasis(Es). PLoS ONE 2011, 6, e28650. [Google Scholar] [CrossRef]
- Sun, R.; Deutsch, E. Imagerie médicale computationnelle (radiomique): Principes et potentiel en onco-pneumologie: Computational medical imaging (radiomics): Principles and potential in onco-pneumology. Rev. Mal. Respir. Actual. 2020, 12, 2S307–2S313. [Google Scholar] [CrossRef]
- Menoux, I.; Le Fèvre, C.; Noël, G.; Antoni, D. Facteurs prédictifs de toxicité pulmonaire après irradiation en conditions stéréotaxiques des carcinomes bronchopulmonaires non à petites cellules de stade I. Cancer/Radiothérapie 2018, 22, 826–838. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.; He, W.; Wen, S.; Feng, X.; Fu, X.; Liu, Y.; Pu, K. Is IMRT Superior or Inferior to 3DCRT in Radiotherapy for NSCLC? A Meta-Analysis. PLoS ONE 2016, 11, e0151988. [Google Scholar] [CrossRef] [PubMed]
- Nyman, J.; Hallqvist, A.; Lund, J.-Å.; Brustugun, O.-T.; Bergman, B.; Bergström, P.; Friesland, S.; Lewensohn, R.; Holmberg, E.; Lax, I. SPACE—A Randomized Study of SBRT vs. Conventional Fractionated Radiotherapy in Medically Inoperable Stage I NSCLC. Radiother. Oncol. 2016, 121, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Vogelius, I.R.; Bentzen, S.M. A Literature-Based Meta-Analysis of Clinical Risk Factors for Development of Radiation Induced Pneumonitis. Acta Oncol. 2012, 51, 975–983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johansson, S.; Bjermer, L.; Franzen, L.; Henriksson, R. Effects of Ongoing Smoking on the Development of Radiation-Induced Pneumonitis in Breast Cancer and Oesophagus Cancer Patients. Radiother. Oncol. 1998, 49, 41–47. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author | Number of Irradiated Metastases Per Patient | Treated Patient | Irradiated Metastases | Size of Lesions | Primitive Cancer | Dose | Local Control | PFS | Evaluation Imaging |
|---|---|---|---|---|---|---|---|---|---|
| Jung et al. 2015 [26] | 1–3 | 50 | 79 | 1.5 cc (med) | CRC | 40 to 60 Gy (med 48 Gy); 3 or 4 frct | 70.6% (3 years) | 24% (3 years) | PET/CT or CT |
| Garcia-Cabezas et al. 2015 [18] | - | 44 | 53 | 2.0 cm (med) | multiple | 50 to 60 Gy; 5 to 8 frct | 86.7% (2 years) | ns | PET/CT |
| Filippi et al. 2015 [20] | 1–4 | 40 | 59 | 1.5 cm | CRC | 26 to 60 Gy; 1 to 8 fract | ns | 27% (2 years) | PET/CT or CT |
| Navarria et al. 2015 [21] | 1–4 | 28 | 51 | 6.5 cc (med) | sarcoma | 30 to 60 Gy; 1 to 8 frct | 96% (2 years) | ns | PET/CT or CT |
| Wang et al. 2015 [29] | 1–4 | 95 | 134 | 14.6 cc (med) | multiple | 30 to 60 Gy; 1 to 5 frct | 90.6% (2 years) | 29% (2 years) | PET/CT |
| Siva et al. 2015 [27] | 1–3 | 65 | 85 | ns | multiple | 18 to 50 Gy; 1 to 5 frct | 93% (2 years) | 38% (2 years) | PET/CT |
| Lischalk et al. 2016 [31] | ns | 20 | 20 | 85.8 cc (med) | multiple | 35 to 40 Gy; 5 fract | 57.4% (2 years) | ns | PET/CT or CT |
| Baumann et al. 2016 [30] | ns | 30 | 39 | 2.4 cm (med) | sarcoma | 50 Gy (med); 4 or 5 frct | 86% (2 years) | ns | PET/CT or CT |
| Pasqualetti et al. 2017 [32] | 1–3 | 33 | 56 | 2.3 cc (med) | CRC | 24 to 42 Gy; 3 frct | 62% (1 year) | 10% (2 years) | PET/CT or CT |
| Agolli et al. 2017 [25] | 1–4 | 44 | 69 | 1.4 cm (med) | CRC | 23 to 45 Gy; 1 to 3 frct | 60.2% (2 years) | 16% (3 years) | PET/CT |
| Lindsay et al. 2018 [33] | 1–7 | 44 | 117 | 2.1 cm (med) | sarcoma | 50 Gy; 10 frct | ns | ns | CT |
| Qiu et al. 2016 [16] | ns | 65 | ns | ns | CRC | 50 Gy; 5 or 10 frct | 30.9% (2 years) | 23.5% (1 year) | ns |
| Osti et al. 2018 [17] | 1–5 | 129 | 166 | 1.3 cm (ave) | multiple | 30 Gy; 1 frct | 80.1% (3 years) | 34% (3 years) | PET/CT or CT |
| Lee et al. 2018 [28] | 1–3 | 21 | 29 | 2.5 cm (med) | multiple | 60 Gy; 3 frct or 48 Gy; 4 frct | 75.2% (2 years) | 12 (2 years) | ns |
| Sharma et al. 2018 [23] | 1–5 | 206 | 327 | ns | multiple | 30 to 60 Gy; 1 to 8 frct | 85% (2 years) | 36% (2 years) | PET/CT or CT |
| Li et al. 2019 [22] | 1–4 | 53 | 105 | 1.1 cm/1.6 cc (med) | CRC | 48 to 75 Gy; 4 to 10 frct | 90.4% (1 year) | ns | PET/CT |
| Helou et al. 2017 [19] | ns | 120 | 184 | 1.5 cm (med) | multiple | 48 to 60 Gy; 4 to 5 frct | 84.8% (2 years) | ns | CT |
| Berkovic et al. 2020 [24] | 1–4 | 104 | 132 | 7.9 cc (ave) | multiple | 20 to 60 Gy; 3 or 5 | 77.8% (3 years) | ns | PET/CT or CT |
| Author | Tumor Size | Number of Thoracic Metastasis Lesions | Biological Effective Dose | Time to SBRT | Combination with Chemotherapy | Primary Colorectal Cancer |
|---|---|---|---|---|---|---|
| Jung et al. 2015 [26] | 2.5 cm (LC) | - | - | - | - | - |
| Garcia-Cabezas et al. 2015 [18] | - | - | - | - | - | - |
| Filippi et al. 2015 [20] | - | - | - | - | - | - |
| Navarria et al. 2015 [21] | - | - | - | - | - | - |
| Wang et al. 2015 [29] | - | 1 (PFS) | 100 Gy (LC) | - | - | - |
| Siva et al. 2015 [27] | - | - | - | - | - | - |
| Lischalk et al. 2016 [31] | - | - | - | - | - | - |
| Baumann et al. 2016 [30] | - | - | - | - | - | - |
| Pasqualetti et al. 2017 [32] | - | - | - | - | - | - |
| Agolli et al. 2017 [25] | - | - | - | - | - | - |
| Lindsay et al. 2018 [33] | - | - | - | - | - | - |
| Qiu et al. 2018 [16] | - | - | - | - | - | - |
| Osti et al. 2018 [17] | 1.8 cm (LC) | - | - | - | - | CLRM < no CLRM (LC and PFS) |
| Lee et al. 2018 [28] | - | - | - | Synchronous < metachronous (OS) | - | - |
| Sharma et al. 2018 [23] | - | - | 100 Gy (LC) | Synchronous < metachronous (OS) | pre-SBRT CT < no pre-SBRT CT (LC) | - |
| Li et al. 2019 [22] | - | - | - | Oligoprogression < oligometatic (regional metastases) | - | - |
| Helou et al. 2017 [19] | largest lesions (LC) | - | 100 Gy (LC) | - | - | CLRM < no CLRM (LC) |
| Berkovic et al. 2020 [24] | - | - | 120 Gy (LC) | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Virbel, G.; Le Fèvre, C.; Noël, G.; Antoni, D. Stereotactic Body Radiotherapy for Patients with Lung Oligometastatic Disease: A Five-Year Systematic Review. Cancers 2021, 13, 3623. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13143623
Virbel G, Le Fèvre C, Noël G, Antoni D. Stereotactic Body Radiotherapy for Patients with Lung Oligometastatic Disease: A Five-Year Systematic Review. Cancers. 2021; 13(14):3623. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13143623
Chicago/Turabian StyleVirbel, Guillaume, Clara Le Fèvre, Georges Noël, and Delphine Antoni. 2021. "Stereotactic Body Radiotherapy for Patients with Lung Oligometastatic Disease: A Five-Year Systematic Review" Cancers 13, no. 14: 3623. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13143623