
Late Local Recurrence of Bone Giant Cell Tumors Associated with an Increased Risk for Malignant Transformation

 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract

1. Introduction
2. Patients and Methods
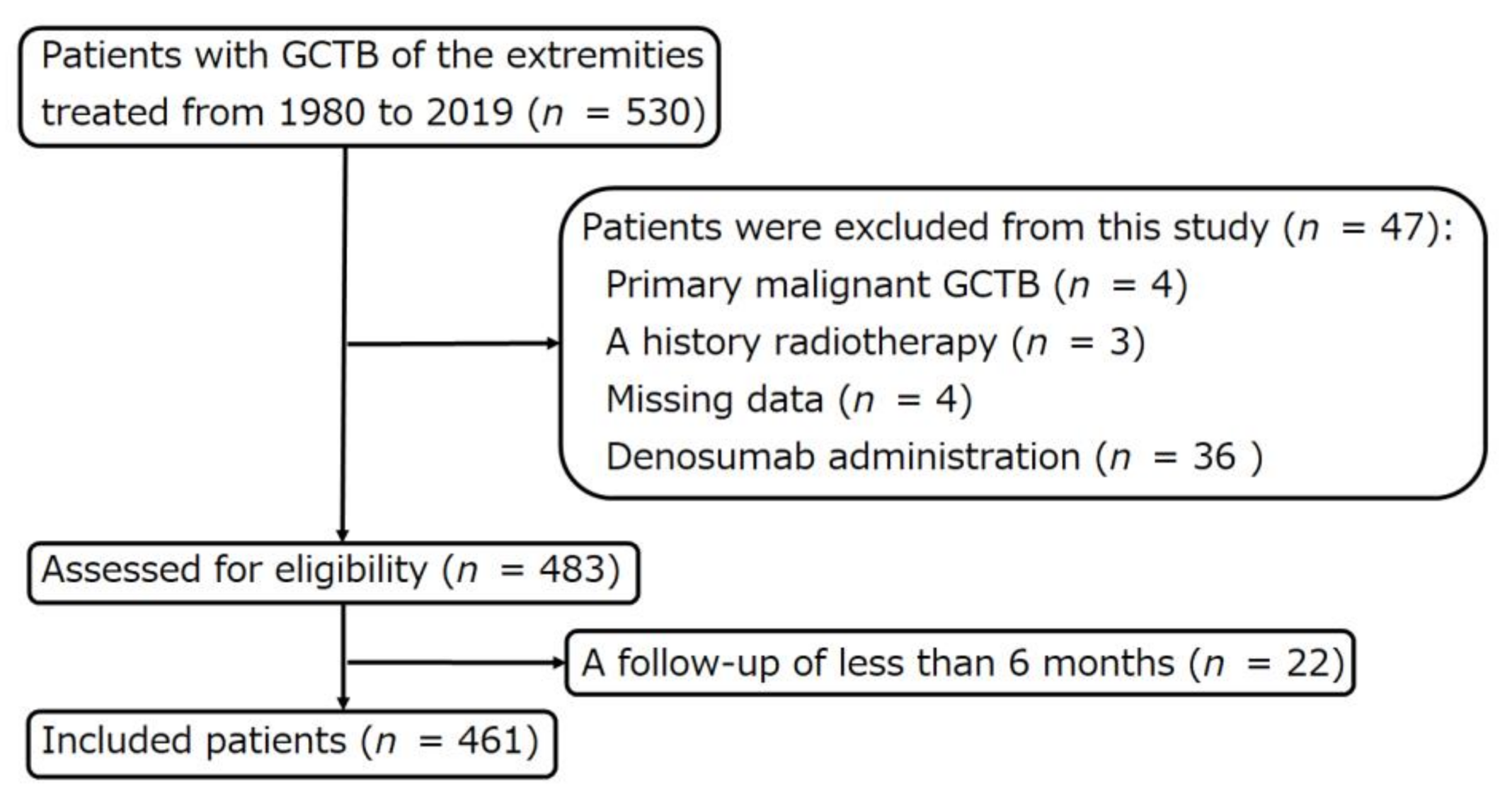
2.1. Patient Selection
2.2. Statistical Analyses
3. Results
3.1. Patient Data and Treatment
3.2. Incidence of Malignant Transformation of GCTB
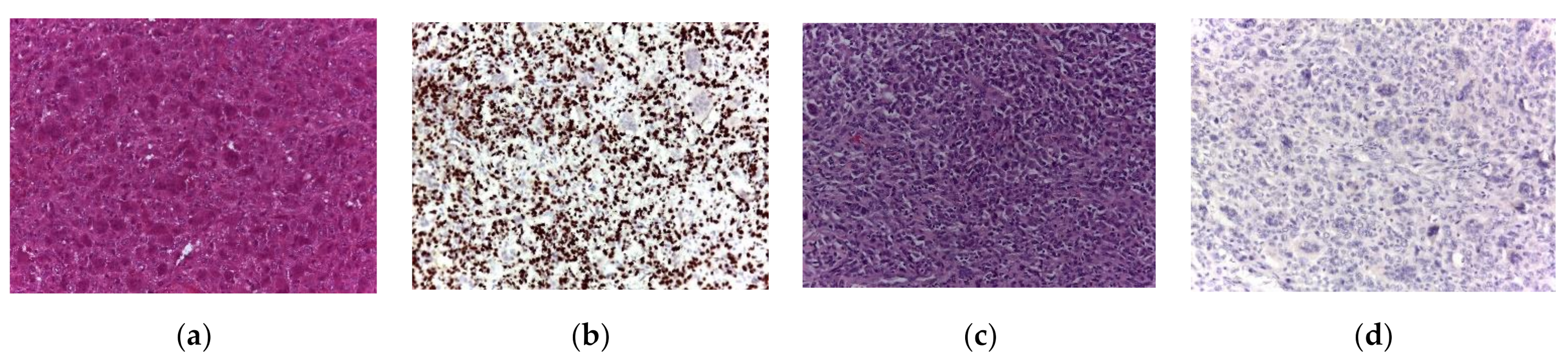
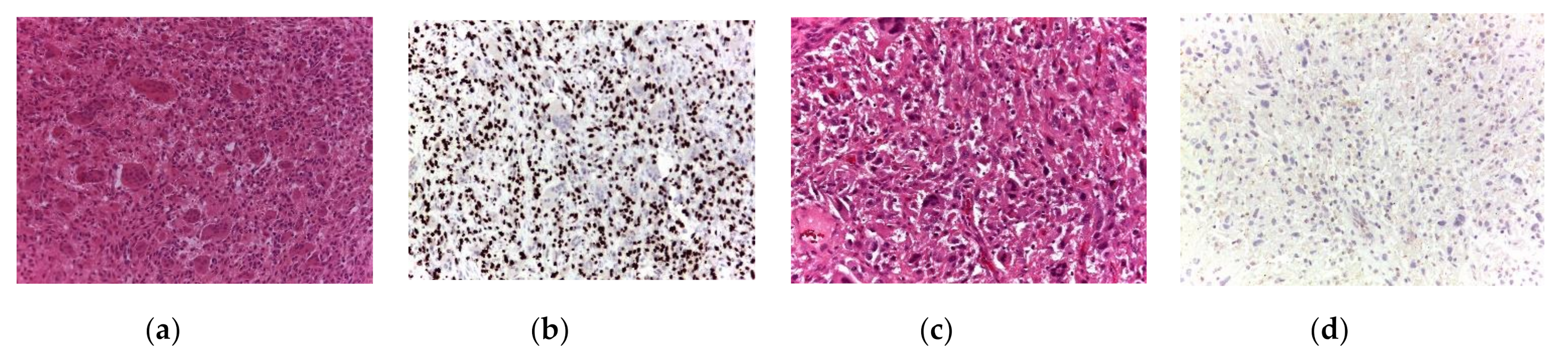
3.3. Histology of Secondary Malignant GCTB
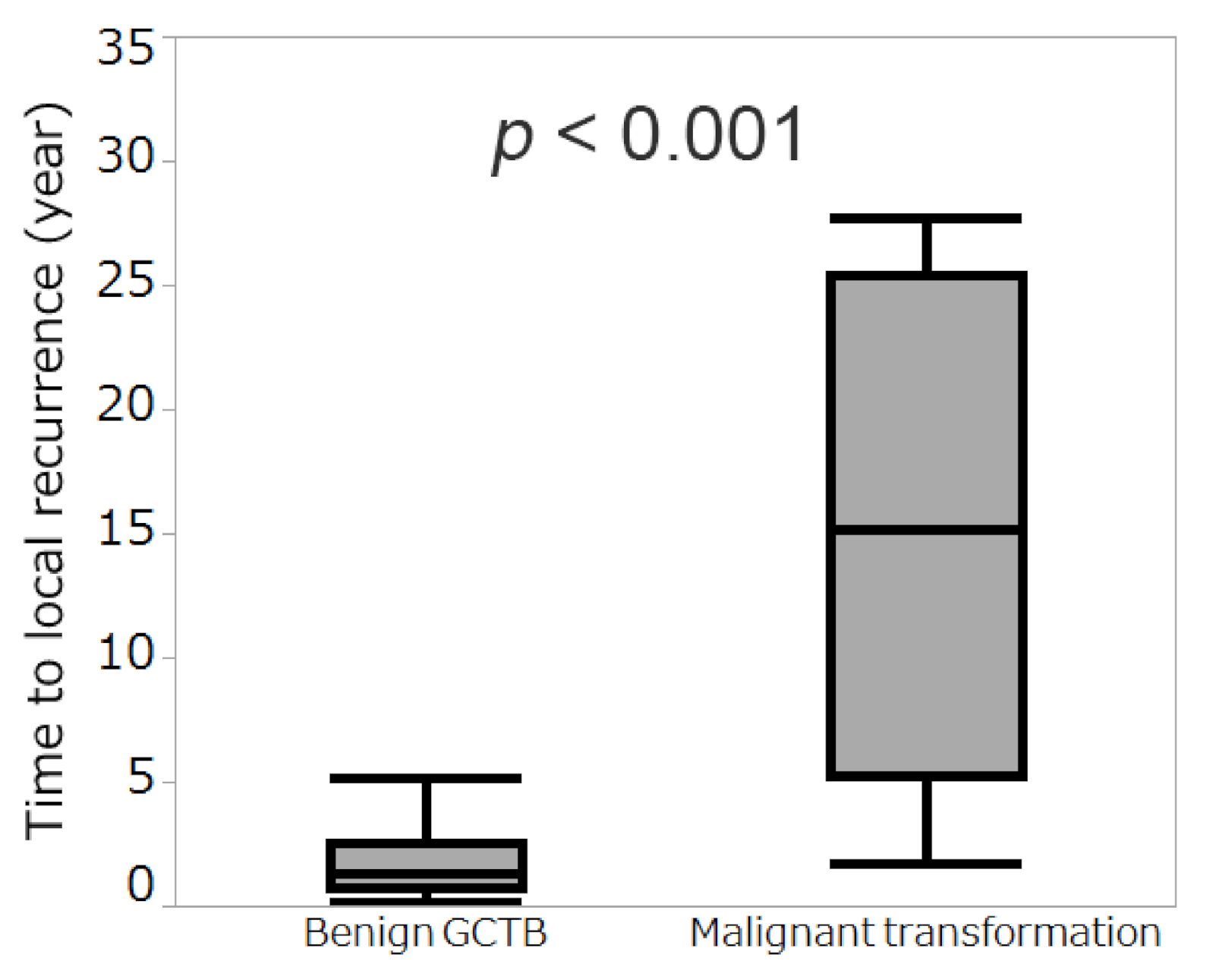
3.4. Comparison of Time to Local Recurrence between Benign GCTB and Secondary Malignant GCTB
3.5. Outcomes in Patients Who Experienced Malignant Transformation
3.6. Risk Factors for Malignant Transformation from GCTB Treated without Radiotherapy
3.7. Details of Excluded Patients Who Received Surgery and Denosumab
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Flanagan, A.M.; Larousserie, F.; O’Donnell, P.G.; Yoshida, A. Giant cell tumour of bone. In Soft Tissue and Bone Tumours. WHO Classification of Tumours, 5th ed.; The WHO Classification of Tumours Editorial Board, Ed.; IARC: Lyon, France, 2020; pp. 440–446. [Google Scholar]
- Yoshida, K.I.; Nakano, Y.; Honda-Kitahara, M.; Wakai, S.; Motoi, T.; Ogura, K.; Sano, N.; Shibata, T.; Okuma, T.; Iwata, S.; et al. Absence of H3F3A mutation in a subset of malignant giant cell tumor of bone. Mod. Pathol. 2019, 32, 1751–1761. [Google Scholar] [CrossRef]
- Deheshi, B.M.; Jaffer, S.N.; Griffin, A.M.; Ferguson, P.C.; Bell, R.S.; Wunder, J.S. Joint salvage for pathologic fracture of giant cell tumor of the lower extremity. Clin. Orthop. Relat. Res. 2007, 459, 96–104. [Google Scholar] [CrossRef] [PubMed]
- Campanacci, M.; Baldini, N.; Boriani, S.; Sudanese, A. Giant-cell tumor of bone. J. Bone Joint Surg. Am. 1987, 69, 106–114. [Google Scholar] [CrossRef] [PubMed]
- Turcotte, R.E.; Wunder, J.S.; Isler, M.H.; Bell, R.S.; Schachar, N.; Masri, B.A.; Moreau, G.; Davis, A.M.; Canadian Sarcoma Group. Giant cell tumor of long bone: A Canadian Sarcoma Group study. Clin. Orthop. Relat. Res. 2002, 397, 248–258. [Google Scholar] [CrossRef] [PubMed]
- Goldenberg, R.R.; Campbell, C.J.; Bonfiglio, M. Giant-cell tumor of bone. An analysis of two hundred and eighteen cases. J. Bone Joint Surg. Am. 1970, 52, 619–664. [Google Scholar] [CrossRef]
- Liu, W.; Chan, C.M.; Gong, L.; Bui, M.M.; Han, G.; Letson, G.D.; Yang, Y.; Niu, X. Malignancy in giant cell tumor of bone in the extremities. J. Bone Oncol. 2021, 26, 100334. [Google Scholar] [CrossRef]
- Palmerini, E.; Picci, P.; Reichardt, P.; Downey, G. Malignancy in giant cell tumor of bone: A review of the literature. Technol. Cancer Res. Treat. 2019, 18, 1533033819840000. [Google Scholar] [CrossRef] [Green Version]
- Chakravarti, A.; Spiro, I.J.; Hug, E.B.; Mankin, H.J.; Efird, J.T.; Suit, H.D. Megavoltage radiation therapy for axial and inoperable giant-cell tumor of bone. J. Bone Joint Surg. Am. 1999, 81, 1566–1573. [Google Scholar] [CrossRef]
- Malone, S.; O’Sullivan, B.; Catton, C.; Bell, R.; Fornasier, V.; Davis, A. Long-term follow-up of efficacy and safety of megavoltage radiotherapy in high-risk giant cell tumors of bone. Int. J. Radiat. Oncol. Biol. Phys. 1995, 33, 689–694. [Google Scholar] [CrossRef]
- Nair, M.K.; Jyothirmayi, R. Radiation therapy in the treatment of giant cell tumor of bone. Int. J. Radiat. Oncol. Biol. Phys. 1999, 43, 1065–1069. [Google Scholar] [CrossRef]
- Ruka, W.; Rutkowski, P.; Morysiński, T.; Nowecki, Z.; Zdzienicki, M.; Makula, D.; Ptaszyński, K.; Bylina, E.; Grzesiakowska, U. The megavoltage radiation therapy in treatment of patients with advanced or difficult giant cell tumors of bone. Int. J. Radiat. Oncol. Biol. Phys. 2010, 78, 494–498. [Google Scholar] [CrossRef]
- Shi, W.; Indelicato, D.J.; Reith, J.; Smith, K.B.; Morris, C.G.; Scarborough, M.T.; Gibbs, C.P.; Mendenhall, W.M.; Zlotecki, R.A. Radiotherapy in the management of giant cell tumor of bone. Am. J. Clin. Oncol. 2013, 36, 505–508. [Google Scholar] [CrossRef]
- Chawla, S.; Henshaw, R.; Seeger, L.; Choy, E.; Blay, J.-Y.; Ferrari, S.; Kroep, J.; Grimer, R.; Reichardt, P.; Rutkowski, P.; et al. Safety and Efficacy of denosumab for adults and skeletally mature adolescents with giant cell tumour of bone: Interim analysis of an open-label, parallel-group, phase 2 study. Lancet Oncol. 2013, 14, 901–908. [Google Scholar] [CrossRef]
- Rutkowski, P.; Ferrari, S.; Grimer, R.J.; Stalley, P.D.; Dijkstra, S.P.D.; Pienkowski, A.; Vaz, G.; Wunder, J.S.; Seeger, L.L.; Feng, A.; et al. Surgical downstaging in an open-label phase II trial of denosumab in patients with giant cell tumor of bone. Ann. Surg. Oncol. 2015, 22, 2860–2868. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agarwal, M.G.; Gundavda, M.K.; Gupta, R.; Reddy, R. Does denosumab change the giant cell tumor treatment strategy? Lessons learned from early experience. Clin. Orthop. Relat. Res. 2018, 476, 1773–1782. [Google Scholar] [CrossRef] [PubMed]
- Alaqaili, S.I.; Abduljabbar, A.M.; Altaho, A.J.; Khan, A.A.; Alherabi, J.A. Malignant sarcomatous transformation of benign giant cell tumor of bone after treatment with denosumab therapy: A literature review of reported cases. Cureus 2018, 10, e3792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aponte-Tinao, L.A.; Piuzzi, N.S.; Roitman, P.; Farfalli, G.L. A high-grade sarcoma arising in a patient with recurrent benign giant cell tumor of the proximal tibia while receiving treatment with denosumab. Clin. Orthop. Relat. Res. 2015, 473, 3050–3055. [Google Scholar] [CrossRef]
- Broehm, C.J.; Garbrecht, E.L.; Wood, J.; Bocklage, T. Two cases of sarcoma arising in giant cell tumor of bone treated with denosumab. Case Rep. Med. 2015, 2015, 767198. [Google Scholar] [CrossRef] [Green Version]
- Park, A.; Cipriano, C.A.; Hill, K.; Kyriakos, M.; McDonald, D.J. Malignant Transformation of a giant cell tumor of bone treated with denosumab: A case report. JBJS Case Connect. 2016, 6, e78. [Google Scholar] [CrossRef]
- Perrin, D.L.; Visgauss, J.D.; Wilson, D.A.; Griffin, A.M.; Abdul Razak, A.R.; Ferguson, P.C.; Wunder, J.S. The role of denosumab in joint preservation for patients with giant cell tumour of bone. Bone Joint J. 2021, 103-B, 184–191. [Google Scholar] [CrossRef] [PubMed]
- Thomas, D.; Carriere, P.; Jacobs, I. Safety of denosumab in giant-cell tumour of bone. Lancet Oncol. 2010, 11, 815. [Google Scholar] [CrossRef]
- Treffel, M.; Lardenois, E.; Larousserie, F.; Karanian, M.; Gomez-Brouchet, A.; Bouvier, C.; Le Loarer, F.; Aubert, S.; de Pinieux, G.; Audard, V.; et al. Denosumab-treated giant cell tumors of bone: A clinicopathologic analysis of 35 cases from the French Group of Bone Pathology. Am. J. Surg. Pathol. 2020, 44, 1–10. [Google Scholar] [CrossRef]
- Tsukamoto, S.; Righi, A.; Vanel, D.; Honoki, K.; Donati, D.M.; Errani, C. Development of high-grade osteosarcoma in a patient with recurrent giant cell tumor of the ischium while receiving treatment with denosumab. Jpn. J. Clin. Oncol. 2017, 47, 1090–1096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Errani, C.; Tsukamoto, S.; Mavrogenis, A.F. How safe and effective is denosumab for bone giant cell tumour? Int. Orthop. 2017, 41, 2397–2400. [Google Scholar] [CrossRef] [PubMed]
- Errani, C.; Ruggieri, P.; Asenzio, M.A.N.; Toscano, A.; Colangeli, S.; Rimondi, E.; Rossi, G.; Longhi, A.; Mercuri, M. Giant cell tumor of the extremity: A review of 349 cases from a single institution. Cancer Treat. Rev. 2010, 36, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Tsukamoto, S.; Mavrogenis, A.F.; Leone, G.; Righi, A.; Akahane, M.; Tanzi, P.; Kido, A.; Honoki, K.; Tanaka, Y.; Donati, D.M.; et al. Denosumab does not decrease the risk of lung metastases from bone giant cell tumour. Int. Orthop. 2019, 43, 483–489. [Google Scholar] [CrossRef]
- O’Donnell, R.J.; Springfield, D.S.; Motwani, H.K.; Ready, J.E.; Gebhardt, M.C.; Mankin, H.J. Recurrence of giant-cell tumors of the long bones after curettage and packing with cement. J. Bone Joint Surg. Am. 1994, 76, 1827–1833. [Google Scholar] [CrossRef] [PubMed]
- Tsukamoto, S.; Mavrogenis, A.F.; Tanzi, P.; Leone, G.; Ciani, G.; Righi, A.; Akahane, M.; Honoki, K.; Tanaka, Y.; Donati, D.M.; et al. Denosumab for bone giant cell tumor of the distal radius. Orthopedics 2020, 43, 284–291. [Google Scholar] [CrossRef] [PubMed]
- Palmerini, E.; Chawla, N.S.; Ferrari, S.; Sudan, M.; Picci, P.; Marchesi, E.; Leopardi, M.P.; Syed, I.; Sankhala, K.K.; Parthasarathy, P.; et al. Denosumab in advanced/unresectable giant-cell tumour of bone (GCTB): For how long? Eur. J. Cancer 2017, 76, 118–124. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.-L.; Wu, Y.-H.; Shi, Y.-F.; Lin, H.; Nisar, M.; Meftah, Z.; Xu, C.; Chen, J.-X.; Wang, X.-Y. Survival and prognosis in malignant giant cell tumor of bone: A population-based analysis from 1984 to 2013. J. Bone Oncol. 2019, 19, 100260. [Google Scholar] [CrossRef]
- Anract, P.; De Pinieux, G.; Cottias, P.; Pouillart, P.; Forest, M.; Tomeno, B. Malignant giant-cell tumours of bone. clinico-pathological types and prognosis: A review of 29 cases. Int. Orthop. 1998, 22, 19–26. [Google Scholar] [CrossRef] [Green Version]
- Chawla, S.; Blay, J.-Y.; Rutkowski, P.; Le Cesne, A.; Reichardt, P.; Gelderblom, H.; Grimer, R.J.; Choy, E.; Skubitz, K.; Seeger, L.; et al. Denosumab in patients with giant-cell tumour of bone: A multicentre, open-label, phase 2 study. Lancet Oncol. 2019, 20, 1719–1729. [Google Scholar] [CrossRef]
- Palmerini, E.; Seeger, L.L.; Gambarotti, M.; Righi, A.; Reichardt, P.; Bukata, S.; Blay, J.-Y.; Dai, T.; Jandial, D.; Picci, P. Malignancy in giant cell tumor of bone: Analysis of an open-label phase 2 study of denosumab. BMC Cancer 2021, 21, 89. [Google Scholar] [CrossRef] [PubMed]
- Righi, A.; Mancini, I.; Gambarotti, M.; Picci, P.; Gamberi, G.; Marraccini, C.; Dei Tos, A.P.; Simi, L.; Pinzani, P.; Franchi, A. Histone 3.3 Mutations in Giant Cell Tumor and Giant Cell-Rich Sarcomas of Bone. Hum. Pathol. 2017, 68, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Mancini, I.; Righi, A.; Gambarotti, M.; Picci, P.; Dei Tos, A.P.; Billings, S.D.; Simi, L.; Franchi, A. Phenotypic and Molecular Differences between Giant-Cell Tumour of Soft Tissue and Its Bone Counterpart. Histopathology 2017, 71, 453–460. [Google Scholar] [CrossRef] [PubMed]
- Gamberi, G.; Morandi, L.; Benini, S.; Resca, A.; Cocchi, S.; Magagnoli, G.; Donati, D.M.; Righi, A.; Gambarotti, M. Detection of H3F3A p.G35W and p.G35R in Giant Cell Tumor of Bone by Allele Specific Locked Nucleic Acid Quantitative PCR (ASLNAqPCR). Pathol. Res. Pract. 2018, 214, 89–94. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable (n = 461) | Number of Patients |
|---|---|
| Age (Years) | |
| Median | 30.0 |
| Interquartile Range | 23.3–41.6 |
| Sex | |
| Male | 225 (48.8%) |
| Female | 236 (51.2%) |
| Site | |
| Distal Radius | 54 (11.7%) |
| Proximal Femur | 25 (5.4%) |
| Distal Femur | 153 (33.2%) |
| Proximal Tibia | 120 (26.0%) |
| Distal Tibia | 17 (3.7%) |
| Proximal Humerus | 23 (5.0%) |
| Others | 69 (15.0%) |
| Campanacci Classification | |
| Stage I | 9 (2.0%) |
| Stage II | 269 (58.4%) |
| Stage III | 183 (39.7%) |
| Previous Surgery | |
| None | 383 (83.1%) |
| 1 | 78 (16.9%) |
| Surgery | |
| Curettage | 270 (58.6%) |
| Resection or Amputation | 191 (41.4%) |
| Local Recurrence | |
| None | 378 (82.0%) |
| 1 | 63 (13.7%) |
| ≥2 | 20 (4.3%) |
| Lung Metastasis | |
| None | 431 (93.5%) |
| Synchronous | 9 (2.0%) |
| Metachronous | 21 (4.6%) |
| Malignant Transformation | |
| None | 446 (96.7%) |
| 1 | 15 (3.3%) |
| Follow-Up (Months) | |
| Median | 89.4 |
| Interquartile Range | 54.8–134.0 |
| Case | Sex | Age | Site | Campanacci Stage | Lung Metastasis at Presentation | Previous Surgery | Surgery | Total Number of Local Recurrence |
|---|---|---|---|---|---|---|---|---|
| 1 | M | 63 | Proximal femur | Stage 3 | No | No | Resection | 1 |
| 2 | F | 21 | Distal femur | Stage 2 | Yes | No | Resection | 0 |
| 3 | F | 27 | Proximal tibia | Stage 2 | No | No | Curettage | 1 |
| 4 | M | 31 | Proximal tibia | Stage 2 | No | No | Curettage | 0 |
| 5 | M | 34 | Proximal tibia | Stage 2 | No | No | Curettage | 6 |
| 6 | F | 36 | Distal ulna | Stage 2 | No | No | Curettage | 1 |
| 7 | M | 31 | Distal femur | Stage 2 | Yes | No | Curettage | 0 |
| 8 | M | 24 | Proximal tibia | Stage 2 | No | No | Curettage | 1 |
| 9 | M | 26 | Proximal tibia | Stage 2 | No | No | Curettage | 1 |
| 10 | M | 37 | Distal femur | Stage 2 | No | No | Curettage | 2 |
| 11 | M | 77 | Distal femur | Stage 2 | No | No | Curettage | 1 |
| 12 | M | 42 | Proximal tibia | Stage 2 | No | No | Curettage | 1 |
| 13 | M | 47 | Proximal femur | Stage 2 | No | No | Curettage | 1 |
| 14 | M | 72 | Proximal tibia | Stage 3 | No | No | Curettage | 1 |
| 15 | F | 62 | Distal radius | Stage 3 | No | No | Curettage | 1 |
| Case | Histology of Malignant GCTB | H3F3A G34W Mutation on Sarcomatous Component | Interval between Initial Surgery of Benign GCTB and Malignant Transformation (Years) | Interval between Last Surgery for Benign GCTB and Local Recurrence with Malignant Transformation (Years) | Distant Metastases at Diagnosis of Malignant GCTB | Treatment for Malignant GCTB | Status | Follow-Up Period from Diagnosis of Malignant GCTB (Months) |
|---|---|---|---|---|---|---|---|---|
| 1 | UPS | Negative | 6.5 | 6.5 | No | External hemipelvectomy | DOD | 19 |
| 2 | Osteosarcoma | Negative | 11.4 | NA | Yes | Palliative CHT | AWD | 9 |
| 3 | Osteosarcoma | Negative | 22.8 | 22.8 | No | Neo- and adjuvant CHT, resection | NED | 46 |
| 4 | UPS | Negative | 13.7 | NA | No | Neo- and adjuvant CHT, amputation | NED | 33 |
| 5 | Osteosarcoma | Negative | 32 | 26.3 | No | Neo- and adjuvant CHT, resection | NED | 97 |
| 6 | Osteosarcoma | Negative | 1.7 | 1.7 | No | Neo- and adjuvant CHT, resection | NED | 86 |
| 7 | Osteosarcoma | Negative | 26.3 | NA | Yes | Palliative CHT | AWD | 9 |
| 8 | UPS | Positive | 4.8 | 4.8 | No | Amputation and adjuvant CHT | NED | 10 |
| 9 | UPS | Positive | 4.1 | 4.1 | No | Resection | NED | 66 |
| 10 | UPS | Negative | 16 | 14 | No | Disarticulation, adjuvant CHT | NED | 123 |
| 11 | Osteosarcoma | Negative | 27 | 27 | Yes | Palliative RT | DOD | 3 |
| 12 | Osteosarcoma | Negative | 16.3 | 16.3 | No | RT, amputation | DOOD | 122 |
| 13 | Osteosarcoma | Negative | 22 | 22 | Yes | Palliative RT, CHT | DOD | 2 |
| 14 | Osteosarcoma | Negative | 27.7 | 27.7 | No | Amputation | NED | 113 |
| 15 | Osteosarcoma | Negative | 7.3 | 7.3 | No | Resection, adjuvant CHT | NED | 32 |
| Variable | No. of Patients (n = 461) | 10-Year Malignant Transformation-Free Survival (95% CI) (%) | p-Value |
|---|---|---|---|
| Age (Years) | 0.806 | ||
| <30 | 225 | 98.9 (95.5–99.7) | |
| 30≤ | 236 | 97.9 (93.6–99.4) | |
| Sex | 0.398 | ||
| Male | 225 | 98.0 (94.0–99.4) | |
| Female | 236 | 98.7 (94.8–99.7) | |
| Site | 0.967 | ||
| Distal Radius/Proximal Femur | 79 | 96.1 (85.8–99.0) | |
| The Others | 382 | 99.0 (97.0–99.7) | |
| Campanacci Classification | 0.575 | ||
| Stage I, II | 278 | 98.6 (95.8–99.6) | |
| Stage III | 183 | 98.0 (92.2–99.5) | |
| Previous Surgery | 0.117 | ||
| None | 383 | 98.1 (95.3–99.2) | |
| 1 | 78 | 100.0 | |
| Surgery | 0.042 * | ||
| Curettage | 270 | 97.8 (94.2–99.2) | |
| Resection or Amputation | 191 | 99.2 (94.3–99.9) | |
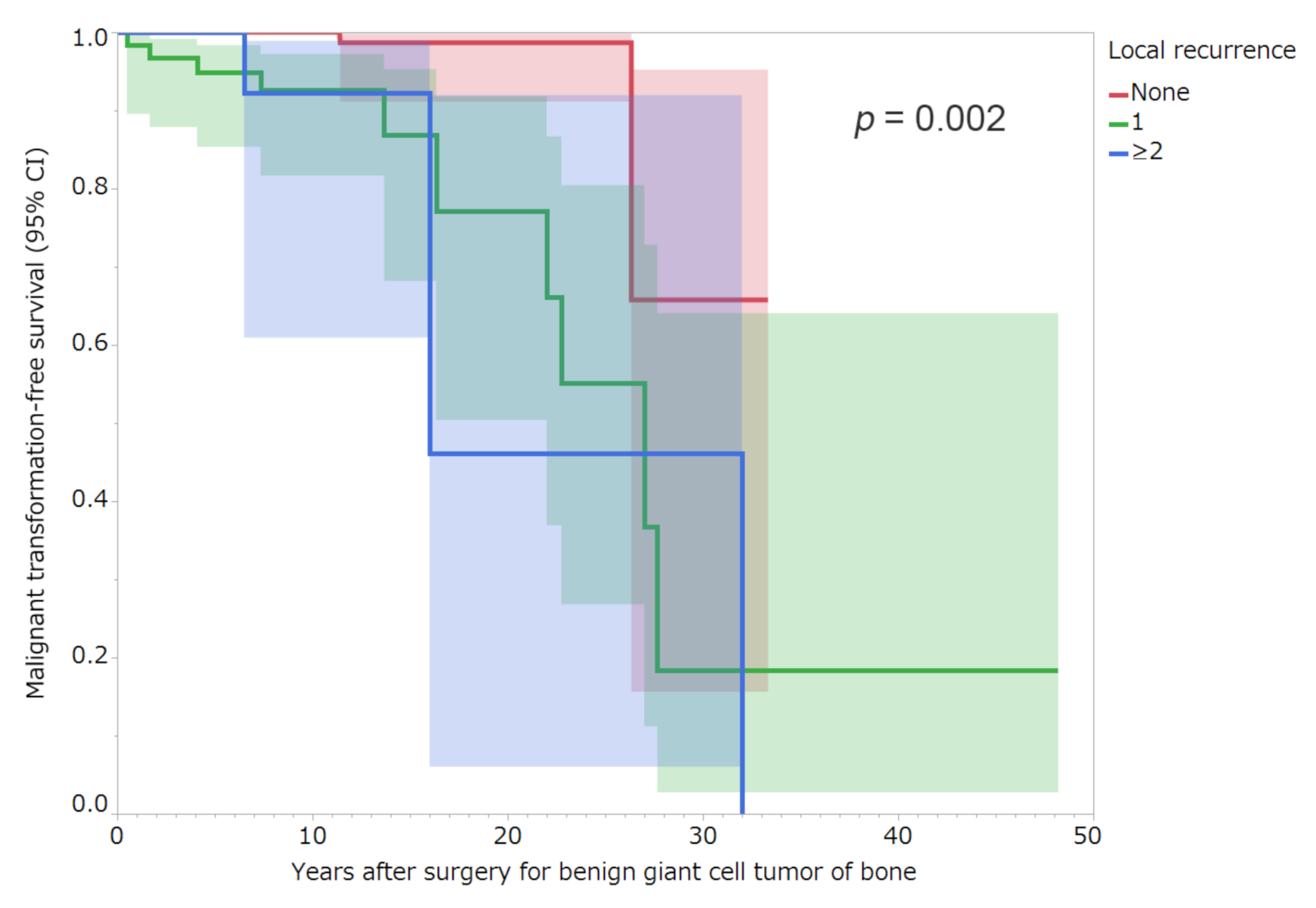
| Local Recurrence | 0.002 * | ||
| None | 378 | 100.0 | |
| 1 | 63 | 92.4 (81.2–97.1) | |
| ≥2 | 20 | 92.3 (60.9–98.9) | |
| Lung Metastasis | 0.751 | ||
| None | 431 | 98.3 (95.8–99.3) | |
| Synchronous or Metachronous | 30 | 100.0 |
| Variable | Hazard Ratio (95% CI) | p-Value |
|---|---|---|
| Local Recurrence | ||
| 1 Versus None | 11.33 (2.33–55.13) | 0.003 * |
| ≥2 Versus None | 11.24 (1.76–71.96) | 0.011 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsukamoto, S.; Righi, A.; Mavrogenis, A.F.; Akahane, M.; Honoki, K.; Tanaka, Y.; Donati, D.M.; Errani, C. Late Local Recurrence of Bone Giant Cell Tumors Associated with an Increased Risk for Malignant Transformation. Cancers 2021, 13, 3644. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13143644
Tsukamoto S, Righi A, Mavrogenis AF, Akahane M, Honoki K, Tanaka Y, Donati DM, Errani C. Late Local Recurrence of Bone Giant Cell Tumors Associated with an Increased Risk for Malignant Transformation. Cancers. 2021; 13(14):3644. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13143644
Chicago/Turabian StyleTsukamoto, Shinji, Alberto Righi, Andreas F. Mavrogenis, Manabu Akahane, Kanya Honoki, Yasuhito Tanaka, Davide Maria Donati, and Costantino Errani. 2021. "Late Local Recurrence of Bone Giant Cell Tumors Associated with an Increased Risk for Malignant Transformation" Cancers 13, no. 14: 3644. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13143644