
Intracranial Mönckeberg’s Atherosclerosis Is Frequently Found in Autopsy Cases of Advanced Stage Malignancy with Cerebral Infarction

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
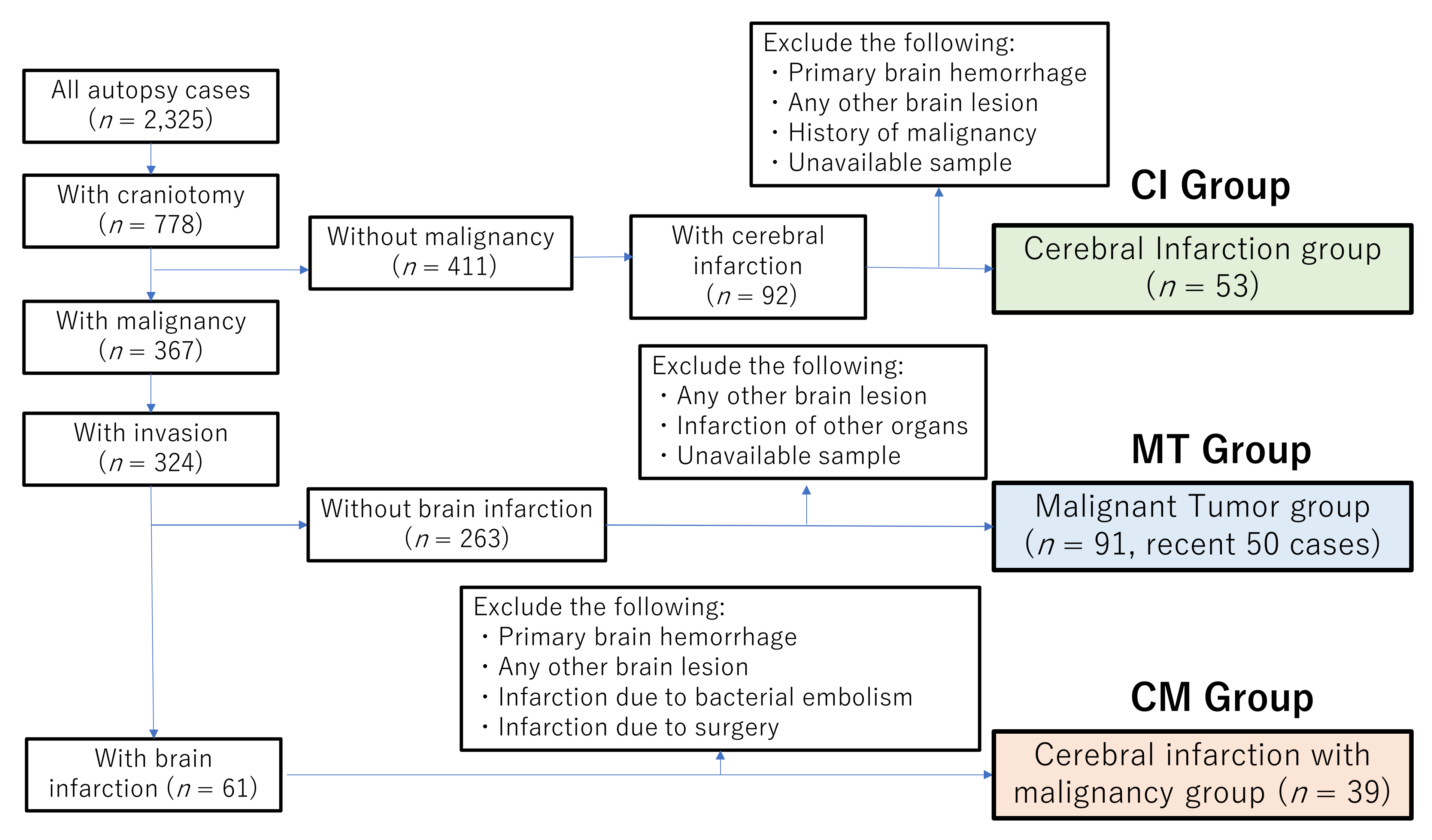
2.1. Patients
2.2. Clinical Data and Pathological Assessments
2.3. Statistical Analysis
3. Results
3.1. Clinicopathological Characteristics of the CM and CI Groups
3.2. Clinicopathological Characteristics of the CM and MT Groups
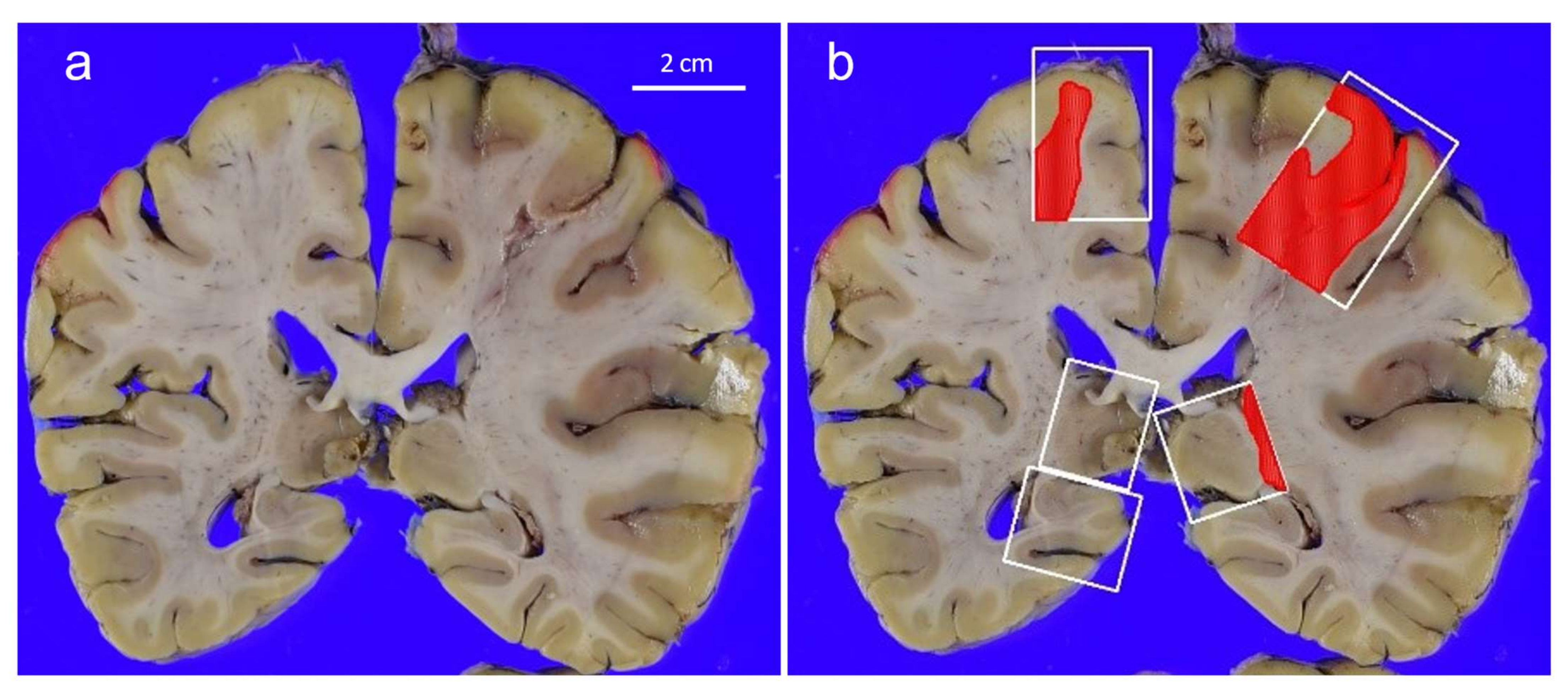
3.3. Pathological Findings in the Brain and Blood Vessels of the CM and CI Groups
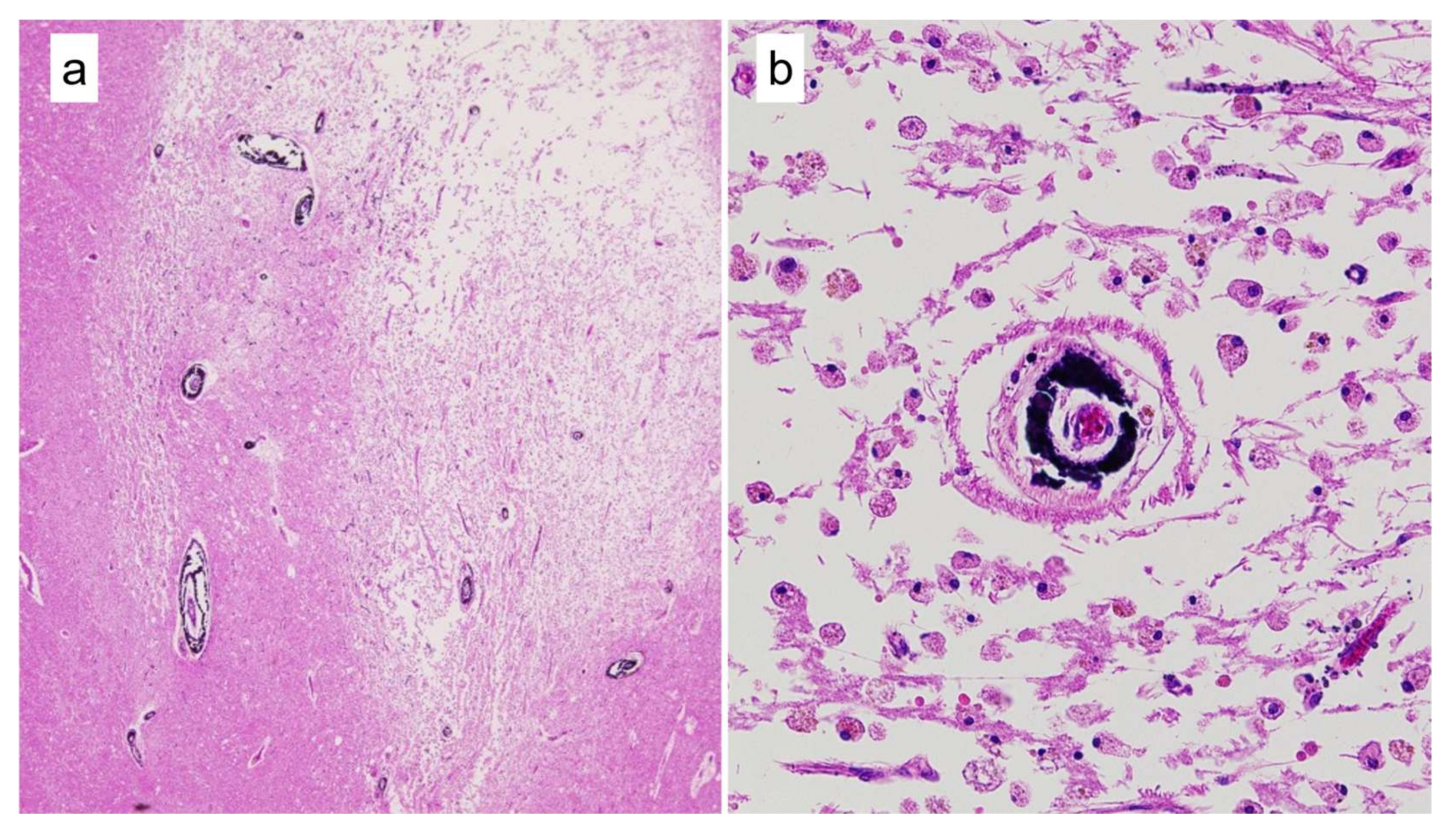
3.4. Mönckeberg’s Atherosclerosis and Amyloid Deposition in Cerebral Vessels
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Grisold, W.; Obernodorfer, S.; Struhal, W. Stroke and cancer: A review. Acta Neurol. Scand. 2009, 119, 1–16. [Google Scholar] [CrossRef]
- Zhang, Y.Y.; Chan, D.K.; Cordato, D.; Shen, Q.; Sheng, A.Z. Stroke risk factor, pattern and outcome in patients with cancer. Acta Neurol. Scand. 2006, 114, 378–383. [Google Scholar] [CrossRef]
- Selvik, H.A.; Thomassen, L.; Bjerkreim, A.T.; Næss, H. Cancer-Associated Stroke: The Bergen NORSTROKE Study. Cerebrovasc. Dis. Extra. 2015, 5, 107–113. [Google Scholar] [CrossRef]
- Zhang, Y.Y.; Cordato, D.; Shen, Q.; Sheng, A.Z.; Hung, W.T.; Chean, D.K. Risk factor, pattern, etiology and outcome in ischemic stroke patients with cancer: A nested case-control study. Cerebrovasc. Dis. 2007, 23, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Trousseau, A. Phlegmasia alba dolens. Clin. Med. Hotel-Dieu Paris 1865, 3, 654–712. [Google Scholar]
- Sack, G.H., Jr.; Levin, J.; Bell, W.R. Trousseau’s syndrome and other manifestations of chronic disseminated coagulopathy in patients with neoplasms: Clinical, pathophysiologic, and therapeutic features. Medicine 1977, 56, 1–37. [Google Scholar] [CrossRef] [PubMed]
- Varki, A. Trousseau’s syndrome: Multiple definitions and multiple mechanisms. Blood 2007, 110, 1723–1729. [Google Scholar] [CrossRef]
- Kim, S.G.; Hong, J.M.; Kim, H.Y.; Lee, J.; Chung, P.W.; Park, K.Y.; Kim, G.M.; Lee, K.H.; Chung, C.S.; Bang, O.Y. Ischemic stroke in cancer patients with and without conventional mechanisms: A multicenter study in Korea. Stroke 2010, 41, 798–801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaturvedi, S.; Ansell, J.; Recht, L. Should cerebral ischemic events in cancer patients be considered a manifestation of hypercoagulability? Stroke 1994, 25, 1215–1218. [Google Scholar] [CrossRef] [Green Version]
- Dearborn, J.L.; Urrutia, V.C.; Zeiler, S.R. Stroke and Cancer- A Complicated Relationship. J. Neurol. Transl. Neurosci. 2014, 2, 1039. [Google Scholar] [PubMed]
- O’Donnell, M.J.; Chin, S.L.; Rangarajan, S.; Xavier, D.; Liu, L.; Zhang, H.; Rao-Melacini, P.; Zhang, X.; Pais, P.; Agapay, S.; et al. Global and regional effects of potentially modifiable risk factors associated with acute stroke in 32 countries (INTERSTROKE): A case-control study. Lancet 2016, 388, 761–775. [Google Scholar] [CrossRef]
- Mönckeberg, J.G. Über die reine Mediaverkalkung der Extremitätenarterien und ihr Verhalten zur Arteriosklerose. Virchows. Arch. Path. Anat. 1903, 171, 141–167. [Google Scholar] [CrossRef] [Green Version]
- Abou-Hassan, N.; Tantisattamo, E.; D’Orsi, E.T.; O’Neill, W.C. The clinical significance of medial arterial calcification in end-stage renal disease in women. Kidney Int. 2015, 87, 195–199. [Google Scholar] [CrossRef]
- Lanzer, P.; Boehm, M.; Sorribas, V.; Thiriet, M.; Janzen, J.; Zeller, T.; St Hilaire, C.; Shanahan, C. Medial vascular calcification revisited: Review and perspectives. Eur. Heart J. 2014, 35, 1515–1525. [Google Scholar] [CrossRef]
- Micheletti, R.G.; Fishbein, G.A.; Currier, J.S.; Fishbein, M.C. Mönckeberg sclerosis revisited: A clarification of the histologic definition of Mönckeberg sclerosis. Arch. Pathol. Lab. Med. 2008, 132, 43–47. [Google Scholar] [CrossRef]
- Ho, C.Y.; Shanahan, C.M. Medial Arterial Calcification: An Overlooked Player in Peripheral Arterial Disease. Arterioscler. Thromb. Vasc. Biol. 2016, 36, 1475–1482. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, S.; Ishibashi-Ueda, H.; Niizuma, S.; Yoshihara, F.; Horio, T.; Kawano, Y. Coronary calcification in patients with chronic kidney disease and coronary artery disease. Clin. J. Am. Soc. Nephrol. 2009, 4, 1892–1900. [Google Scholar] [CrossRef]
- Castillo, B.V., Jr.; Torczynski, E.; Edward, D.P. Monckeberg’s sclerosis in temporal artery biopsy specimens. Br. J. Ophthalmol. 1999, 83, 1091–1092. [Google Scholar] [CrossRef] [Green Version]
- Tahmasbi-Arashlow, M.; Barghan, S.; Kashtwari, D.; Nair, M.K. Radiographic manifestations of Mönckeberg arteriosclerosis in the head and neck region. Imaging Sci. Dent. 2016, 46, 53–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lucksom, P.; Kharka, L.; Sebastian, N.; Gupta, A. Monckeberg’s Arteriosclerosis in Uterine Vessels: An Unusual Presentation. J. Obstet. Gynaecol. India 2014, 64, 436–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saxena, A.; Waddell, I.C.; Friesen, R.W.; Michalski, R.T. Monckeberg medial calcific sclerosis mimicking malignant calcification pattern at mammography. J. Clin. Pathol. 2005, 58, 447–448. [Google Scholar]
- Kim, H.; Greenberg, J.S.; Javitt, M.C. Breast calcifications due to Mönckeberg medial calcific sclerosis. Radiographics 1999, 19, 1401–1403. [Google Scholar] [CrossRef] [Green Version]
- Trimboli, R.M.; Capra, D.; Codari, M.; Cozzi, A.; Di Leo, G.; Sardanelli, F. Breast arterial calcifications as a biomarker of cardiovascular risk: Radiologists’ awareness, reporting, and action. A survey among the EUSOBI members. Eur. Radiol. 2021, 31, 958–966. [Google Scholar] [CrossRef] [PubMed]
- Pisani, I.; De Troia, A.; Allegri, L.; Corradi, D.; Vaglio, A. Malignant Mönckeberg medial calcific sclerosis. Intern. Emerg. Med. 2018, 13, 615–617. [Google Scholar] [CrossRef] [Green Version]
- Fujita, D.; Terada, S.; Ishizu, H.; Yokota, O.; Nakashima, H.; Ishihara, T.; Kuroda, S. Immunohistochemical examination on intracranial calcification in neurodegenerative diseases. Acta Neuropathol. 2003, 105, 259–264. [Google Scholar] [CrossRef] [Green Version]
- Slager, U.T.; Wagner, J.A. The incidence, composition, and pathological significance of intracerebral vascular deposits in the basal ganglia. J. Neuropathol. Exp. Neurol. 1956, 15, 417–431. [Google Scholar] [CrossRef] [PubMed]
- Fahr, I. Idiopathipathische verkalking der hirume fasse. Zbl. Allf. Path. 1930, 50, 129–133. [Google Scholar]
- Savino, E.; Soavi, C.; Capatti, E.; Borrelli, M.; Vigna, G.B.; Passaro, A.; Zuliani, G. Bilateral strio-pallido-dentate calcinosis (Fahr’s disease): Report of seven cases and revision of literature. BMC Neurol. 2016, 16, 165. [Google Scholar] [CrossRef] [Green Version]
- de Oliveira, J.; de Oliveira, M.F. Basal ganglia calcification as a putative cause for cognitive decline. Dement. Neuropsychol. 2013, 7, 151–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mann D., M. Calcification of the basal ganglia in Down’s syndrome and Alzheimer’s disease. Acta Neuropathol. 1988, 76, 595–598. [Google Scholar] [CrossRef]
- Lorente-Poch, L.; Rifà-Terricabras, S.; Sancho, J.J.; Torselli-Valladares, D.; González-Ortiz, S.; Sitges-Serra, A. Prevalence of basal ganglia and carotid artery calcifications in patients with permanent hypoparathyroidism after total thyroidectomy. Endocr. Connect. 2020, 9, 955–962. [Google Scholar] [CrossRef] [PubMed]
- de Brouwer, E.; Kockelkoren, R.; De Vis, J.B.; Dankbaar, J.W.; Velthuis, B.K.; Takx, R.A.; De Jonghe, A.; Emmelot-Vonk, M.H.; Koek, H.L.; de Jong, P.A.; et al. Prevalence and vascular risk factors of basal ganglia calcifications in patients at risk for cerebrovascular disease. J. Neuroradiol. 2020, 47, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Moe, S.M.; Chen, N.X. Pathophysiology of vascular calcification in chronic kidney disease. Circ. Res. 2004, 95, 560–567. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variable | CM Group n = 39 | CI Group n = 53 | p-Value |
|---|---|---|---|
| Age, years (mean ± SD) | 69.4 ± 9.5 | 75.0 ± 10.4 | 0.009 |
| Gender (%) | 1.000 | ||
| Male | 22 (56.4%) | 31 (58.5%) | |
| Female | 17 (43.6%) | 22 (41.5%) | |
| Body mass index (mean ± SD) a | 18.9 ± 0.6 | 21.0 ± 0.6 | 0.019 |
| General risk factors for CI | |||
| Hypertension | 8 (20.5%) | 23 (43.4%) | 0.027 |
| Diabetes | 5 (12.8%) | 9 (17.0%) | 0.771 |
| Atrial fibrillation | 2 (5.1%) | 12 (22.6%) | 0.037 |
| Chronic kidney disease | 1 (2.6%) | 11 (20.8%) | 0.012 |
| Infarction of other organs (%) b | 16 (41.0%) | 28 (52.8%) | 0.296 |
| Heart | 10 (25.6%) | 22 (41.5%) | 0.128 |
| Spleen | 6 (15.4%) | 1 (1.9%) | 0.039 |
| Kidney | 4 (10.3%) | 5 (9.4%) | 1.000 |
| Lung | 1 (2.6%) | 3 (5.7%) | 0.635 |
| Variable | CM Group n = 39 | MT Group n = 50 | p-Value |
|---|---|---|---|
| Age, years (mean ± SD) | 69.4 ± 9.5 | 64.0 ± 14.7 | 0.052 |
| Gender (%) | |||
| Male | 22 (56.4%) | 28 (56.0%) | 1.000 |
| Female | 17 (43.6%) | 22 (44.0%) | |
| Body mass index (mean ± SD) a | 18.9 ± 3.8 | 19.6 ± 3.2 | 0.398 |
| General risk factors for CI | |||
| Hypertension | 8 (20.5%) | 7 (14.0%) | 0.569 |
| Diabetes | 5 (12.8%) | 5 (10.0%) | 0.743 |
| Atrial fibrillation | 2 (5.1%) | 2 (4.0%) | 1.000 |
| Chronic kidney disease | 1 (2.6%) | 1 (2.0%) | 1.000 |
| Variable | CM Group n = 39 | CI Group n = 53 | p-Value |
|---|---|---|---|
| Number of brain sections (mean, range) | 8.6 (2–22) | 10.9 (4–25) | 0.045 * |
| Number of brain infarctions | 0.803 | ||
| Multiple | 30 (76.9%) | 42 (79.3%) | |
| Single | 9 (23.1%) | 11 (20.8%) | |
| Site of cerebral infarction (%) | |||
| Cortex/Subcortex | 28 (71.8%) | 35 (66.4%) | 0.652 |
| Thalamus/Basal ganglia | 30/36 (83.3%), NA = 3 | 42/51 (82.4%), NA = 2 | 1.000 |
| Cerebellum | 8/33 (24.2%), NA = 6 | 13/46 (28.3%), NA = 7 | 0.799 |
| Brain stem | 9/29 (31.0%), NA = 10 | 27/51 (52.9%), NA = 2 | 0.066 |
| Lacunar infarction (<1.5 cm) only (%) | 0.675 | ||
| Yes | 22 (56.4%) | 27 (50.9%) | |
| No | 17 (43.6%) | 26 (49.1%) | |
| With hemorrhage | 9 (23.1%) | 19 (35.9%) | 0.253 |
| Micro hemorrhage (<1.5 cm) | 4 (10.3%) | 7 (13.2%) | 0.754 |
| Massive hemorrhage | 5 (12.8%) | 12 (22.6%) | 0.284 |
| Variable | CM n = 39 | CI n = 53 | MT n = 50 | p-Value (CM vs. CI) | p-Value (CM vs. MT) | p-Value (CI vs. MT) |
|---|---|---|---|---|---|---|
| Mönckeberg’s atherosclerosis | 15 (38.5%) | 10 (18.9%) | 6 (12.0%) | 0.057 | 0.005 | 0.419 |
| Cortex/Subcortex | 1 | 0 | 0 | 0.424 | 0.438 | - |
| Thalamus/Basal ganglia | 14 | 10 | 6 | 0.056 | 0.009 | 0.416 |
| Cerebellum | 2 | 0 | 1 | 0.171 | 0.586 | 0.465 |
| Brain stem | 1 | 0 | 0 | 0.363 | 0.387 | - |
| Amyloid deposition at vessels | 2 (5.1%) | 4 (7.6%) | 2 (4.0%) | 1.000 | 1.000 | 0.679 |
| Chronic kidney disease | 1 (2.6%) | 11 (20.8%) | 1 (2.0%) | 0.012 | 1.000 | 0.004 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shichijo, C.; Kai, K.; Jinnouchi, K.; Nishihara, M.; Hara, H.; Aishima, S. Intracranial Mönckeberg’s Atherosclerosis Is Frequently Found in Autopsy Cases of Advanced Stage Malignancy with Cerebral Infarction. Cancers 2021, 13, 5234. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13205234
Shichijo C, Kai K, Jinnouchi K, Nishihara M, Hara H, Aishima S. Intracranial Mönckeberg’s Atherosclerosis Is Frequently Found in Autopsy Cases of Advanced Stage Malignancy with Cerebral Infarction. Cancers. 2021; 13(20):5234. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13205234
Chicago/Turabian StyleShichijo, Chika, Keita Kai, Kazuki Jinnouchi, Masashi Nishihara, Hideo Hara, and Shinichi Aishima. 2021. "Intracranial Mönckeberg’s Atherosclerosis Is Frequently Found in Autopsy Cases of Advanced Stage Malignancy with Cerebral Infarction" Cancers 13, no. 20: 5234. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13205234