
The Value of Platelet-to-Lymphocyte Ratio as a Prognostic Marker in Cholangiocarcinoma: A Systematic Review and Meta-Analysis

 ,
,  , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Inclusion and Exclusion Criteria
2.3. Statistical Analysis
2.4. Quality Assessment of Studies
3. Results
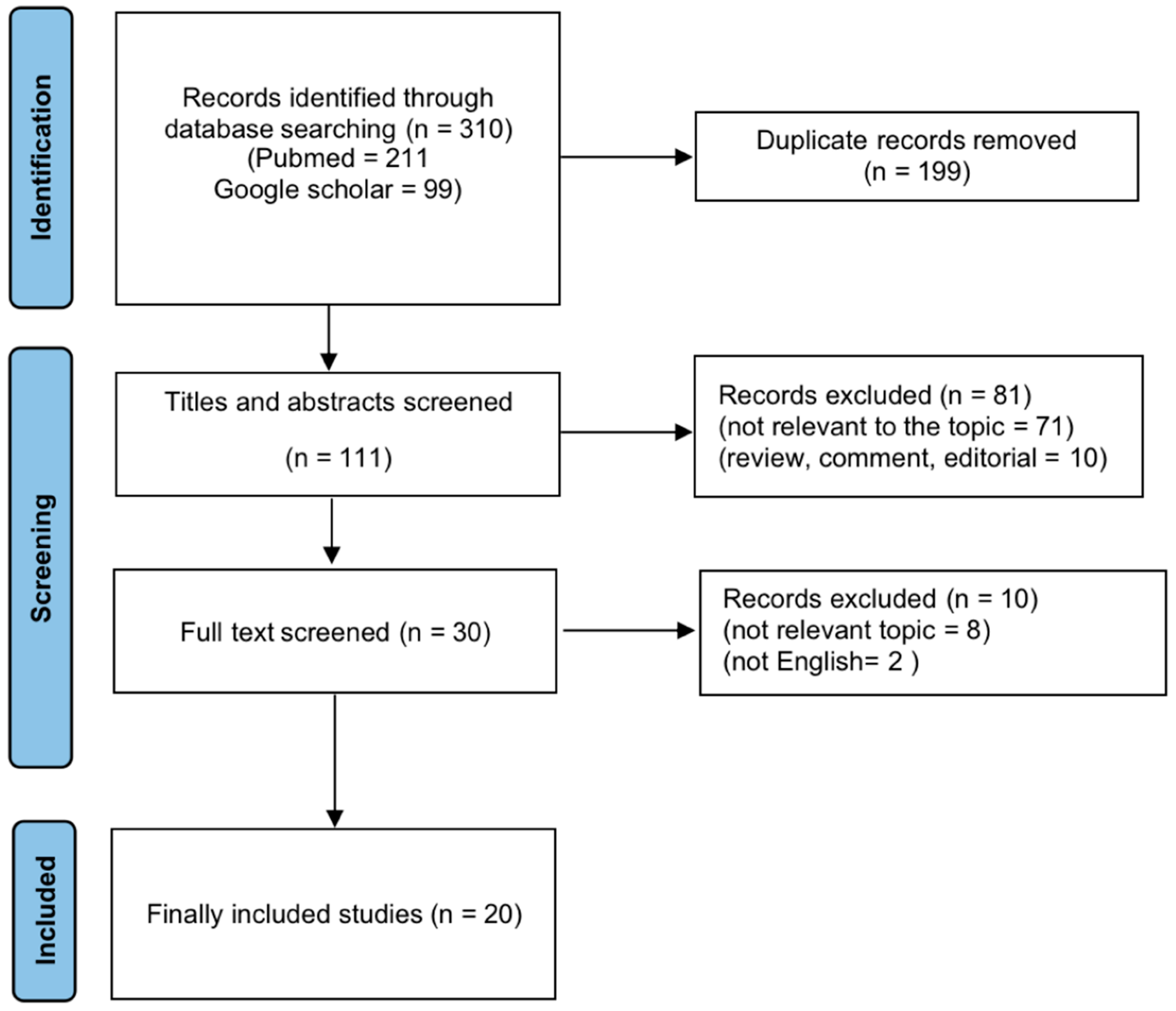
3.1. Literature Search
3.2. Study Characteristics and Quality Assessment
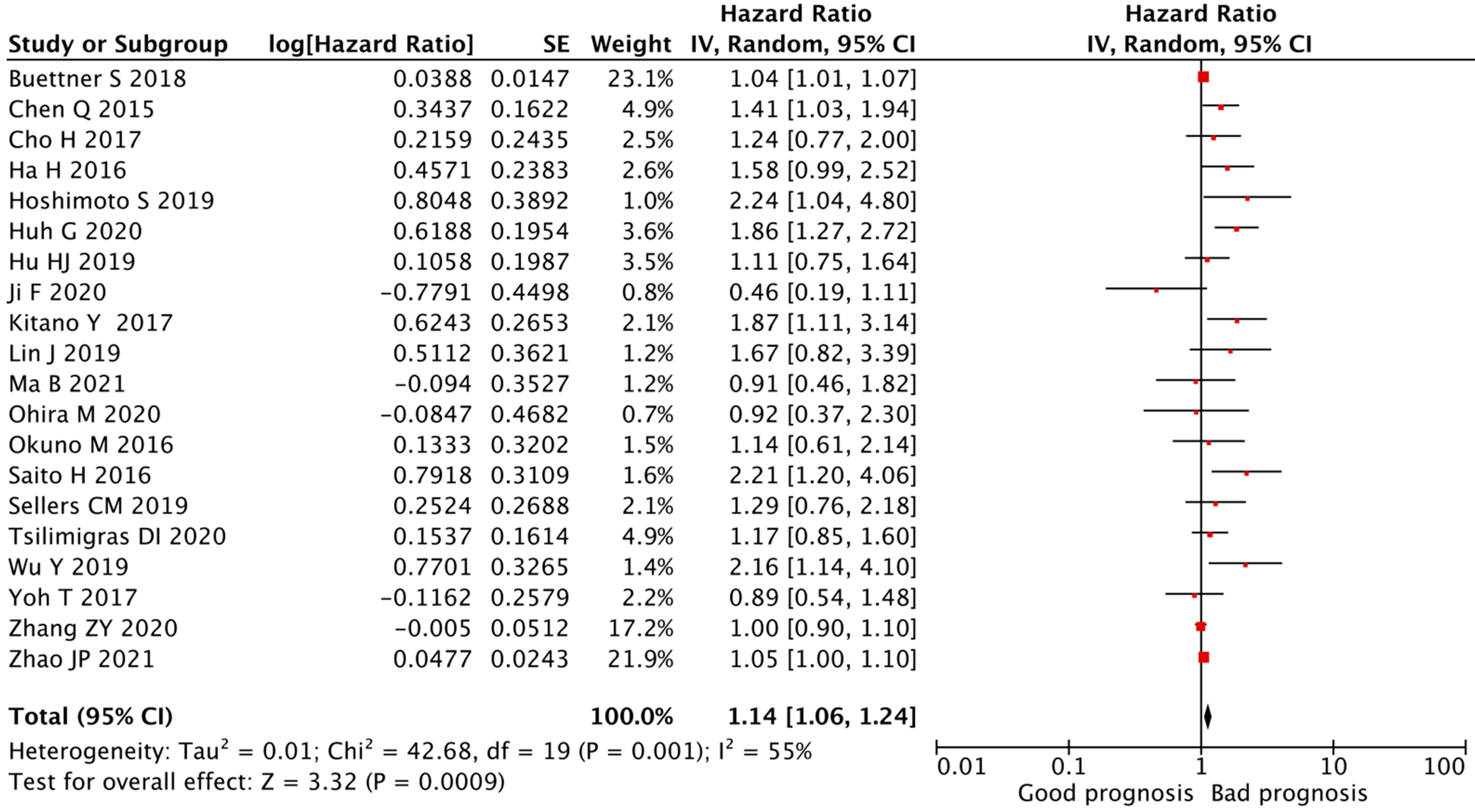
3.3. Correlation between the PLR and OS of CCA Patients
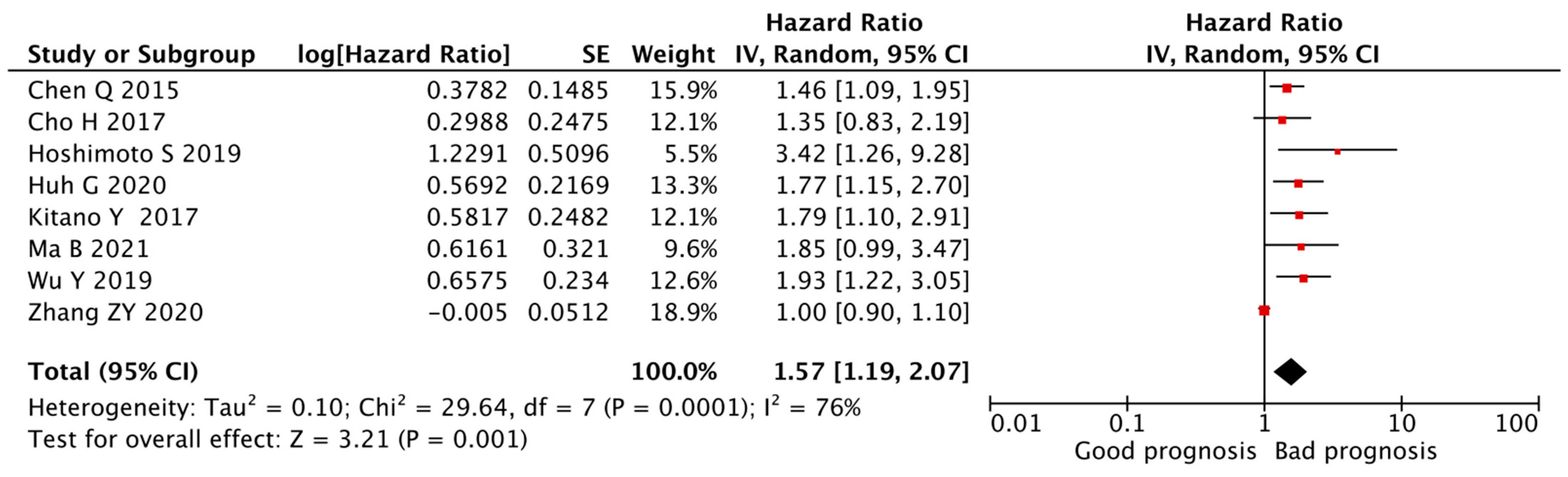
3.4. Correlation between the PLR and DFS of CCA Patients
3.5. Subgroup Analyses of Correlation between the PLR and OS of CCA Patients
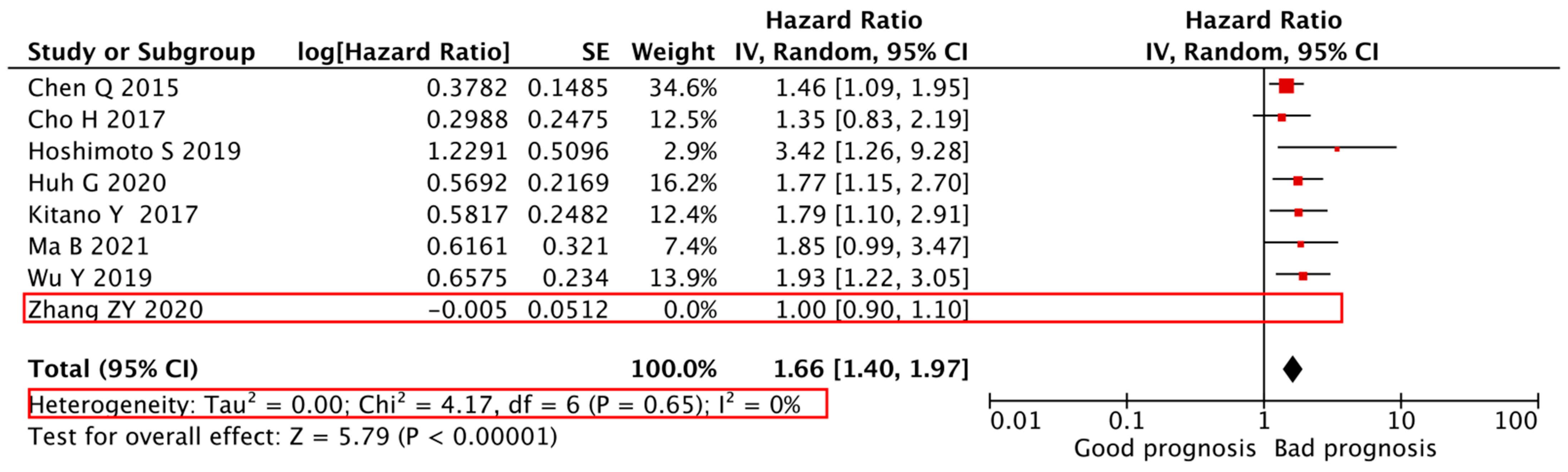
3.6. Sensitivity Analyses of Correlation between the PLR and Prognosis of CCA Patients
3.7. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Oliveira, I.S.; Kilcoyne, A.; Everett, J.M.; Mino-Kenudson, M.; Harisinghani, M.G.; Ganesan, K. Cholangiocarcinoma: Classification, diagnosis, staging, imaging features, and management. Abdom Radiol. 2017, 42, 1637–1649. [Google Scholar] [CrossRef]
- Ghouri, Y.A.; Mian, I.; Blechacz, B. Cancer review: Cholangiocarcinoma. J. Carcinog. 2015, 14, 1. [Google Scholar]
- Banales, J.M.; Cardinale, V.; Carpino, G.; Marzioni, M.; Andersen, J.B.; Invernizzi, P.; Lind, G.E.; Folseraas, T.; Forbes, S.J.; Fouassier, L.; et al. Expert consensus document: Cholangiocarcinoma: Current knowledge and future perspectives consensus statement from the European Network for the Study of Cholangiocarcinoma (ENS-CCA). Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 261–280. [Google Scholar] [CrossRef]
- Bednarsch, J.; Czigany, Z.; Heij, L.R.; Luedde, T.; Loosen, S.H.; Dulk, M.D.; Bruners, P.; Lang, S.A.; Ulmer, T.F.; Neumann, U.P. The prognostic role of in-hospital transfusion of fresh frozen plasma in patients with cholangiocarcinoma undergoing curative-intent liver surgery. Eur. J. Surg. Oncol. 2021. [Google Scholar] [CrossRef]
- Templeton, A.J.; McNamara, M.G.; Seruga, B.; Vera-Badillo, F.E.; Aneja, P.; Ocana, A.; Leibowitz, A.R.; Sonpavde, G.; Knox, J.J.; Tran, B.; et al. Prognostic role of neutrophil-to-lymphocyte ratio in solid tumors: A systematic review and meta-analysis. J. Natl. Cancer Inst. 2014, 106, dju124. [Google Scholar] [CrossRef] [Green Version]
- Templeton, A.J.; Ace, O.; McNamara, M.G.; Al-Mubarak, M.; Vera-Badillo, F.E.; Hermanns, T.; Seruga, B.; Ocana, A.; Tannock, I.F.; Amir, E. Prognostic role of platelet to lymphocyte ratio in solid tumors: A systematic review and meta-analysis. Cancer Epidemiol. Biomarkers Prev. 2014, 23, 1204–1212. [Google Scholar] [CrossRef] [Green Version]
- McMillan, D.C. The systemic inflammation-based Glasgow Prognostic Score: A decade of experience in patients with cancer. Cancer Treat. Rev. 2013, 39, 534–540. [Google Scholar] [CrossRef] [PubMed]
- Amygdalos, I.; Bednarsch, J.; Meister, F.A.; Erren, D.; Mantas, A.; Strnad, P.; Lang, S.A.; Ulmer, T.F.; Boecke, J.; Liu, W.; et al. Clinical value and limitations of the preoperative C-reactive-protein-to-albumin ratio in predicting post-operative morbidity and mortality after deceased-donor liver transplantation: A retrospective single-centre study. Transpl. Int. 2021, 34, 1468–1480. [Google Scholar] [CrossRef] [PubMed]
- Radulescu, D.; Baleanu, V.D.; Padureanu, V.; Radulescu, P.M.; Bordu, S.; Patrascu, S.; Socea, B.; Bacalbase, N.; Surlin, M.V.; Georgescu, I.; et al. Neutrophil/Lymphocyte ratio as predictor of anastomotic leak after gastric cancer surgery. Diagnostics 2020, 10, 799. [Google Scholar] [CrossRef] [PubMed]
- Hakeem, A.R.; Marangoni, G.; Chapman, S.J.; Young, R.S.; Nair, A.; Hidalgo, E.L.; Toogood, G.J.; Wyatt, J.I.; Lodge, P.A.; Prasad, K.R. Does the extent of lymphadenectomy, number of lymph nodes, positive lymph node ratio and neutrophil–lymphocyte ratio impact surgical outcome of perihilar cholangiocarcinoma? Eur. J. Gastroenterol. Hepatol. 2014, 26, 1047–1054. [Google Scholar] [CrossRef]
- Hamed, M.O.; Roberts, K.J.; Smith, A.M.; Stiff, G.M. Elevated pre-operative neutrophil to lymphocyte ratio predicts disease free survival following pancreatic resection for periampullary carcinomas. Pancreatology 2013, 13, 534–538. [Google Scholar] [CrossRef]
- Tan, D.W.; Fu, Y.; Su, Q.; Guan, M.J.; Kong, P.; Wang, S.Q.; Wang, H.L. Prognostic significance of neutrophil to lymphocyte ratio in oncologic outcomes of cholangiocarcinoma: A meta-analysis. Sci. Rep. UK 2016, 6, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wagner, D.D. New links between inflammation and thrombosis. Arterioscl. Throm. Vas. 2005, 25, 1321–1324. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.; Harris, J.; Ware, J. Platelets linking hemostasis and cancer. Arterioscl. Throm. Vas. 2010, 30, 2362–2367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nieswandt, B.; Hafner, M.; Echtenacher, B.; Mannel, D.N. Lysis of tumor cells by natural killer cells in mice is impeded by platelets. Cancer Res. 1999, 59, 1295–1300. [Google Scholar]
- Buergy, D.; Wenz, F.; Groden, C.; Brockmann, M.A. Tumor-platelet interaction in solid tumors. Int. J. Cancer. 2012, 130, 2747–2760. [Google Scholar] [CrossRef] [PubMed]
- Vigano, A.; Bruera, E.; Jhangri, G.S.; Newman, S.C.; Fields, A.L.; Suarez-Almazor, M.E. Clinical survival predictors in patients with advanced cancer. Arch. Intern. Med. 2000, 160, 861–868. [Google Scholar] [CrossRef] [PubMed]
- Amygdalos, I.; Czigany, Z.; Bednarsch, J.; Boecker, J.; Santana, D.A.M.; Meister, F.A.; Von der Massen, J.; Liu, W.J.; Strnad, P.; Neumann, U.P.; et al. Low postoperative platelet counts are associated with major morbidity and inferior survival in adult recipients of orthotopic liver transplantation. J. Gastrointest. Surg. 2020, 24, 1996–2007. [Google Scholar] [CrossRef] [PubMed]
- Tierney, J.F.; Stewart, L.A.; Ghersi, D.; Burdett, S.; Sydes, M.R. Practical methods for incorporating summary time-to-event data into meta-analysis. Trials 2007, 8, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Galon, J.; Pages, F.; Marincola, F.M.; Angell, H.K.; Thurin, M.; Lugli, A.; Zlobec, C.; Botti, G.; Kreiter, S.; Chouchane, L.; et al. Cancer classification using the Immunoscore: A worldwide task force. J. Trans. Med. 2012, 10, 1–10. [Google Scholar] [CrossRef]
- Wells, G.S.B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M. The Newcastleottawa Scale (NOS) for Assessing the Quality if Non-Randomized Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 14 December 2021).
- Zhao, J.P.; Chen, Y.; Wang, J.J.; Wang, J.; Wang, Y.; Chai, S.S.; Zhang, Y.X.; Chen, X.P.; Zhang, W.U. Preoperative risk grade predicts the long-term prognosis of intrahepatic cholangiocarcinoma: A retrospective cohort analysis. BMC Surg. 2021, 21, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Ma, B.; Meng, H.; Shen, A.; Ma, Y.; Zhao, D.; Liu, G.; Zheng, S.; Tian, Y.; Zhang, W.; Li, Q.; et al. Prognostic value of inflammatory and tumour markers in small-duct subtype intrahepatic cholangiocarcinoma after curative-intent resection. Gastroenterol. Res. Pract. 2021, 2021, 6616062. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.Y.; Zhou, Y.F.; Hu, K.; Huang, Y. Investigating effects of preoperative inflammatory biomarkers on predicting survival outcomes of intrahepatic cholangiocarcinoma after curative resection. World J. Surg. Oncol. 2020, 18, 1–7. [Google Scholar] [CrossRef]
- Tsilimigras, D.I.; Moris, D.; Mehta, R.; Paredes, A.Z.; Sahara, K.; Guglielmi, A.; Aldrighetti, L.; Weiss, M.; Bauer, T.W.; Alexandrescu, S.; et al. The systemic immune-inflammation index predicts prognosis in intrahepatic cholangiocarcinoma: An international multi-institutional analysis. HPB 2020, 22, 1667–1674. [Google Scholar] [CrossRef]
- Ohira, M.; Yoshizumi, T.; Yugawa, K.; Kosai-Fujimoto, Y.; Inokuchi, S.; Motomura, T.; Mano, Y.; Toshima, T.; Itoh, S.; Harada, Y.; et al. Association of inflammatory biomarkers with long-term outcomes after curative surgery for mass-forming intrahepatic cholangiocarcinoma. Surg. Today 2020, 50, 379–388. [Google Scholar] [CrossRef]
- Ji, F.; Kang, Q.; Wang, L.; Liu, L.; Ke, Y.; Zhu, Y.; Zhang, N.; Xiong, S.; Li, Y.; Zou, H. Prognostic significance of the neutrophil-to-lymphocyte ratio with distal cholangiocarcinoma patients. Medicine 2020, 99, e22827. [Google Scholar] [CrossRef]
- Huh, G.; Ryu, J.K.; Chun, J.W.; Kim, J.S.; Park, N.; Cho, I.R.; Paik, W.H.; Lee, S.H.; Kim, Y.T. High platelet-to-lymphocyte ratio is associated with poor prognosis in patients with unresectable intrahepatic cholangiocarcinoma receiving gemcitabine plus cisplatin. BMC Cancer 2020, 20, 1–13. [Google Scholar] [CrossRef]
- Wu, Y.; Zhou, D.Y.; Zhang, G.P.; Yi, F.M.; Feng, L. Preoperative serum platelet-lymphocyte ratio as a prognostic factor in cholangiocarcinoma patients after radical resection: A retrospective analysis of 119 patients. Gastroent. Res. Pract. 2019. [Google Scholar] [CrossRef]
- Sellers, C.M.; Uhlig, J.; Ludwig, J.M.; Stein, S.M.; Kim, H.S. Inflammatory markers in intrahepatic cholangiocarcinoma: Effects of advanced liver disease. Cancer Med. 2019, 8, 5916–5929. [Google Scholar] [CrossRef]
- Lin, J.; Fang, T.; Zhu, M.; Xu, X.; Zhang, J.; Zheng, S.; Jing, C.; Zhang, M.; Liu, B.; Zhang, B. Comparative performance of inflammation-based prognostic scores in patients operated for intrahepatic cholangiocarcinoma. Cancer Manag. Res. 2019, 11, 9107–9119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, H.J.; Jin, Y.W.; Zhou, R.X.; Ma, W.J.; Yang, Q.; Wang, J.K.; Liu, F.; Cheng, N.S.; Li, F.Y. Clinical value of inflammation-based prognostic scores to predict the resectability of hyperbilirubinemia patients with potentially resectable hilar cholangiocarcinoma. J. Gastrointest. Surg. 2019, 23, 510–517. [Google Scholar] [CrossRef]
- Hoshimoto, S.; Hishinuma, S.; Shirakawa, H.; Tomikawa, M.; Ozawa, I.; Ogata, Y. Association of preoperative platelet-to-lymphocyte ratio with poor outcome in patients with distal cholangiocarcinoma. Oncology 2019, 96, 290–298. [Google Scholar] [CrossRef]
- Buettner, S.; Spolverato, G.; Kimbrough, C.W.; Alexandrescu, S.; Marques, H.P.; Lamelas, J.; Aldrighetti, L.; Gamblin, T.C.; Maithel, S.K.; Pulitano, C.; et al. The impact of neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio among patients with intrahepatic cholangiocarcinoma. Surgery 2018, 164, 411–418. [Google Scholar] [CrossRef] [PubMed]
- Yoh, T.; Seo, S.; Hatano, E.; Taura, K.; Fuji, H.; Ikeno, Y.; Okuda, Y.; Yasuchika, K.; Kaido, T.; Okajina, H.; et al. A novel biomarker-based preoperative prognostic grading system for predicting survival after surgery for intrahepatic cholangiocarcinoma. Ann. Surg. Oncol. 2017, 24, 1351–1357. [Google Scholar] [CrossRef]
- Kitano, Y.; Yamashita, Y.I.; Yamamura, K.; Arima, K.; Kaida, T.; Miyata, T.; Nakagawa, S.; Mima, K.; Imai, K.; Hashimoto, D.; et al. Effects of preoperative neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios on survival in patients with extrahepatic cholangiocarcinoma. Anticancer Res. 2017, 37, 3229–3237. [Google Scholar]
- Cho, H.; Yoo, C.; Kim, K.P.; Chang, H.M.; Ryoo, B.Y. Prognostic implication of inflammation-based prognostic scores in patients with intrahepatic cholangiocarcinoma (iCCA) treated with first-line gemcitabine plus cisplatin (GEMCIS). Ann. Oncol. 2017, 28, v244. [Google Scholar] [CrossRef] [Green Version]
- Saito, H.; Noji, T.; Okamura, K.; Tsuchikawa, T.; Shichinohe, T.; Hirano, S. A new prognostic scoring system using factors available preoperatively to predict survival after operative resection of perihilar cholangiocarcinoma. Surgery 2016, 159, 842–851. [Google Scholar] [CrossRef] [Green Version]
- Okuno, M.; Ebata, T.; Yokoyama, Y.; Igami, T.; Sugawara, G.; Mizuno, T.; Yamaguchi, J.; Nagino, M. Evaluation of inflammation-based prognostic scores in patients undergoing hepatobiliary resection for perihilar cholangiocarcinoma. J. Gastroenterol. 2016, 51, 153–161. [Google Scholar] [CrossRef] [PubMed]
- Ha, H.; Nam, A.R.; Bang, J.H.; Park, J.E.; Kim, T.Y.; Lee, K.H.; Han, S.W.; Lm, S.A.; Kim, T.Y.; Bang, Y.J.; et al. Soluble programmed death-ligand 1 (sPDL1) and neutrophil-to-lymphocyte ratio (NLR) predicts survival in advanced biliary tract cancer patients treated with palliative chemotherapy. Oncotarget 2016, 7, 76604–76612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Q.; Dai, Z.; Yin, D.; Yang, L.X.; Wang, Z.; Xiao, Y.S.; Fan, J.; Zhou, J. Negative impact of preoperative platelet-lymphocyte ratio on outcome after hepatic resection for intrahepatic cholangiocarcinoma. Medicine 2015, 94, e574. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Huang, Y.; Zhou, L.; Dai, Y.H.; Hu, G.Y. High pretreatment neutrophil-to-lymphocyte ratio as a predictor of poor survival prognosis in head and neck squamous cell carcinoma: Systematic review and meta-analysis. Head Neck J. Sci. Spec. 2019, 41, 1525–1535. [Google Scholar] [CrossRef]
- Peng, B.; Wang, Y.H.; Liu, Y.M.; Ma, L.X. Prognostic significance of the neutrophil to lymphocyte ratio in patients with non-small cell lung cancer: A systemic review and meta-analysis. Int. J. Clin. Exp. Med. 2015, 8, 3098–3106. [Google Scholar] [PubMed]
- Koh, C.H.; Bhoo-Pathy, N.; Ng, K.L.; Jabir, R.S.; Tan, G.H.; See, M.H.; Jamaris, S.; Taib, N.A. Utility of pre-treatment neutrophil-lymphocyte ratio and platelet-lymphocyte ratio as prognostic factors in breast cancer. Brit. J. Cancer. 2015, 113, 150–158. [Google Scholar] [CrossRef]
- Hu, K.M.; Lou, L.X.; Ye, J.; Zhang, S.Z. Prognostic role of the neutrophil-lymphocyte ratio in renal cell carcinoma: A meta-analysis. BMJ Open 2015, 5, e006404. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Fang, J.; Huang, X.; Liu, Y.; Yuan, Y.; Zhang, X.; Zou, C.; Xiao, K.; Wang, J. Prognostic role of neutrophil to lymphocyte ratio and platelet to lymphocyte ratio in prostate cancer: A meta-analysis of results from multivariate analysis. Int. J. Surg. 2018, 60, 216–223. [Google Scholar] [CrossRef]
- Yodying, H.; Matsuda, A.; Miyashita, M.; Matsumoto, S.; Sakurazawa, N.; Yamada, M.; Uchida, E. Prognostic significance of neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio in oncologic outcomes of esophageal cancer: A systematic review and meta-analysis. Ann. Surg. Oncol. 2016, 23, 646–654. [Google Scholar] [CrossRef] [PubMed]
- Oh, D.; Pyo, J.S.; Son, B.K. Prognostic roles of inflammatory markers in pancreatic cancer: Comparison between the neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio. Gastroent. Res. Pract. 2018, 25, 169–178. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Zhang, H.Y.; Li, J.; Shao, X.Y.; Zhang, C.X. The elevated NLR, PLR and PLT may predict the prognosis of patients with colorectal cancer: A systematic review and meta-analysis. Oncotarget 2017, 8, 68837–68846. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, J.; Cai, J.Y.; Li, H.; Zeng, K.N.; He, L.Y.; Fu, H.Y.; Zhang, J.B.; Chen, L.; Yao, J.; Zhang, Y.C.; et al. Neutrophil to lymphocyte ratio and platelet to lymphocyte ratio as prognostic predictors for hepatocellular carcinoma patients with various treatments: A meta-analysis and systematic review. Cell. Physiol. Biochem. 2017, 44, 967–981. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.S.; Xu, W.; Cheng, H.; Shen, W.; Ying, J.Q.; Cheng, F.; Xu, W.J. The prognostic role of the platelet-lymphocytes ratio in gastric cancer: A meta-analysis. PLoS ONE 2016, 11, e0163719. [Google Scholar] [CrossRef] [PubMed]
- Valle, J.; Wasan, H.; Palmer, D.H.; Cunningham, D.; Anthoney, A.; Maraveyas, A.; Madhusudan, S.; Iveson, T.; Hughes, S.; Pereira, S.P.; et al. Cisplatin plus gemcitabine versus gemcitabine for biliary tract cancer. N. Engl. J. Med. 2010, 362, 1273–1281. [Google Scholar] [CrossRef] [Green Version]
- Bednarsch, J.; Kather, J.; Tan, X.; Sivakumar, S.; Cacchi, C.; Wiltberger, G.; Czigany, Z.; Ulmer, F.; Neumann, U.P.; Heij, L.R. Nerve fibers in the tumor microenvironment as a novel biomarker for oncological outcome in patients undergoing surgery for perihilar cholangiocarcinoma. Liver Cancer 2021, 10, 260–274. [Google Scholar] [CrossRef]
- Bednarsch, J.; Czigany, Z.; Heij, L.R.; Luedde, T.; Wiltberger, G.; Dulk, M.D.; Bruners, P.; Lang, S.A.; Ulmer, T.F.; Neumann, U.P. The prognostic role of tumor-associated unilateral portal vein occlusion in perihilar cholangiocarcinoma. HPB 2021, 23, 1565–1577. [Google Scholar] [CrossRef]
- Bednarsch, J.; Czigany, Z.; Lurje, I.; Amygdalos, I.; Strnad, P.; Halm, P.; Wiltberger, G.; Ulmer, T.F.; Schulze-Hagen, M.; Bruners, P.; et al. Insufficient future liver remnant and preoperative cholangitis predict perioperative outcome in perihilar cholangiocarcinoma. HPB 2021, 23, 99–108. [Google Scholar] [CrossRef]
- Bednarsch, J.; Czigany, Z.; Heij, L.R.; Luedde, T.; van Dam, R.; Lang, S.A.; Ulmer, T.F.; Hornel, M.W.; Neumann, U.P. Bacterial bile duct colonization in perihilar cholangiocarcinoma and its clinical significance. Sci. Rep. 2021, 11, 2926. [Google Scholar] [CrossRef] [PubMed]
- Ulich, T.R.; del Castillo, J.; Keys, M.; Granger, G.A.; Ni, R.X. Kinetics and mechanisms of recombinant human interleukin 1 and tumor necrosis factor-alpha-induced changes in circulating numbers of neutrophils and lymphocytes. J. Immunol. 1987, 139, 3406–3415. [Google Scholar] [PubMed]
- Riesco, A. Five-year cancer cure: Relation to total amount of peripheral lymphocytes and neutrophils. Cancer 1970, 25, 135–140. [Google Scholar] [CrossRef]
- Plantureux, L.; Mege, D.; Crescence, L.; Dignat-George, F.; Dubois, C.; Panicot-Dubois, L. Impacts of cancer on platelet production, activation and education and mechanisms of cancer-associated thrombosis. Cancers 2018, 10, 441. [Google Scholar] [CrossRef] [Green Version]
- Krenn-Pilko, S.; Langsenlehner, U.; Thurner, E.M.; Stojakovic, T.; Pichler, M.; Gerger, A.; Kapp, K.S.; Langsenlehner, T. The elevated preoperative platelet-to-lymphocyte ratio predicts poor prognosis in breast cancer patients. Brit. J. Cancer 2014, 110, 2524–2530. [Google Scholar] [CrossRef] [Green Version]
- Seretis, C.; Seretis, F.; Lagoudianakis, E.; Politou, M.; Gemenetzis, G.; Salemis, N.S. Enhancing the accuracy of platelet to lymphocyte ratio after adjustment for large platelet count: A pilot study in breast cancer patients. Int. J. Surg. Oncol. 2012, 2012, 653608. [Google Scholar] [CrossRef] [Green Version]
- Yu, P.; Fu, Y.X. Tumor-infiltrating T lymphocytes: Friends or foes? Lab. Investig. 2006, 86, 231–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mantovani, A.; Allavena, P.; Sica, A.; Balkwill, F. Cancer-related inflammation. Nature 2008, 454, 436–444. [Google Scholar] [CrossRef]
- Eli Pikarsky, R.M.P.; Stein, I.; Abramovitch, R.; Amit, S.; Kasem, S.; Gutkovich-Pyest, E.; Urieli-Shoval, S.; Galun, E.; Ben-Neriah, Y. NF-kappaB functions as a tumour promoter in inflammation-associated cancer. Nature 2004, 431, 461–466. [Google Scholar] [CrossRef]
- Jordi Rius, M.G.; Schachtrup, C.; Akassoglou, K.; Zinkernagel, A.S.; Nizet, V.; Johnson, R.S.; Haddad, G.G.; Karin, M. NF-kappaB links innate immunity to the hypoxic response through transcriptional regulation of HIF-1alpha. Nature 2008, 453, 807–811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mizukami, Y.; Jo, W.S.; Duerr, E.M.; Gala, M.; Li, J.; Zhang, X.; Zimmer, M.A.; Lliopoulos, O.; Zukerberg, L.R.; Kohgo, Y.; et al. Induction of interleukin-8 preserves the angiogenic response in HIF-1alpha-deficient colon cancer cells. Nat. Med. 2005, 11, 992–997. [Google Scholar] [CrossRef] [Green Version]
- Szlosarek, P.W.; Balkwill, F.R. Tumour necrosis factor alpha: A potential target for the therapy of solid tumours. Lancet Oncol. 2003, 4, 565–573. [Google Scholar] [CrossRef]
- Seubwai, W.; Wongkham, C.; Puapairoj, A.; Khuntikeo, N.; Pugkhem, A.; Hahnvajanawong, C.; Chaiyagoo, J.; Ymezawa, K.; Okada, S.; Wongkham, S. Aberrant expression of NF-kappaB in liver fluke associated cholangiocarcinoma: Implications for targeted therapy. PLoS ONE 2014, 9, e106056. [Google Scholar] [CrossRef]
- Yang, X.W.; Li, L.; Hou, G.J.; Yan, X.Z.; Xu, Q.G.; Chen, L.; Zhang, B.H.; Shen, F. STAT3 overexpression promotes metastasis in intrahepatic cholangiocarcinoma and correlates negatively with surgical outcome. Oncotarget 2017, 8, 7710–7721. [Google Scholar]
- Yu, A.; Zhao, L.; Kang, Q.; Li, J.; Chen, K.; Fu, H. Transcription factor HIF1alpha promotes proliferation, migration, and invasion of cholangiocarcinoma via long noncoding RNA H19/microRNA-612/Bcl-2 axis. Transl. Res. 2020, 224, 26–39. [Google Scholar] [CrossRef]
- Kwon, H.C.; Kim, S.H.; Oh, S.Y.; Lee, S.; Lee, J.H.; Choi, H.J.; Park, K.J.; Roh, M.S.; Kim, S.G.; Kim, H.J.; et al. Clinical significance of preoperative neutrophil-lymphocyte versus platelet-lymphocyte ratio in patients with operable colorectal cancer. Biomarkers 2012, 17, 216–222. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Wu, M.; Feng, F.Z.; Huang, H.F.; Ynag, J.X.; Shen, K.; Xiang, Y. Pretreatment neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios do not predict survival in patients with cervical cancer treated with neoadjuvant chemotherapy and radical hysterectomy. Chin. Med. J. 2013, 126, 1464–1468. [Google Scholar] [PubMed]
- Saeed, A.; Park, R.; Al-Jumayli, M.; Al-Rajabi, R.; Sun, W. Biologics, immunotherapy, and future directions in the treatment of advanced cholangiocarcinoma. Clin. Colorectal. Cancer 2019, 18, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Y. Spatial heterogeneity in the tumor microenvironment. Cold Spring Harb. Perspect. Med. 2016, 6, a026583. [Google Scholar] [CrossRef] [Green Version]
- Bai, R.; Lv, Z.; Xu, D.; Cui, J. Predictive biomarkers for cancer immunotherapy with immune checkpoint inhibitors. Biomark Res. 2020, 8, 34. [Google Scholar] [CrossRef] [PubMed]
- Zhang, N.; Jiang, J.; Tang, S.; Sun, G. Predictive value of neutrophil-lymphocyte ratio and platelet-lymphocyte ratio in non-small cell lung cancer patients treated with immune checkpoint inhibitors: A meta-analysis. Int. Immunopharmacol. 2020, 85, 106677. [Google Scholar] [CrossRef]
- Xu, H.; He, A.; Liu, A.; Tong, W.; Cao, D. Evaluation of the prognostic role of platelet-lymphocyte ratio in cancer patients treated with immune checkpoint inhibitors: A systematic review and meta-analysis. Int. Immunopharmacol. 2019, 77, 105957. [Google Scholar] [CrossRef]
- Diem, S.; Schmid, S.; Krapf, M.; Flatz, L.; Born, D.; Jochum, W.; Templeton, A.J.; Fruh, M. Neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) as prognostic markers in patients with non-small cell lung cancer (NSCLC) treated with nivolumab. Lung. Cancer 2017, 111, 176–181. [Google Scholar] [CrossRef]
- Zer, A.; Sung, M.R.; Walia, P.; Khoja, L.; Maganti, M.; Labbe, C.; Shepherd, F.A.; Bradbury, P.A.; Feld, R.; Liu, G.; et al. Correlation of neutrophil to lymphocyte ratio and absolute neutrophil count with outcomes with PD-1 axis inhibitors in patients with advanced non-small-cell lung cancer. Clin. Lung. Cancer 2018, 19, 426–434.e1. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ref. | Author | Year Published | Country | Tumor Type | Sample Size | Stage | Age (Median) | Male (%) | Treatment | Follow-Up (Months, Median) | Endpoint | Cut-Off Value |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| [22] | Zhao JP | 2021 | China | ICCA | 468 | NR | 58 | 60.30% | Surgery | NR | OS | PLR ≥ 143.5 |
| [23] | Ma B | 2021 | China | ICCA | 174 | I–IV | 58 | 55.90% | Surgery | 25.1 | OS/DFS | PLR ≥ 90 |
| [24] | Zhang ZY | 2020 | China | ICCA | 128 | I–III | 56 | 55.00% | Surgery | NR | OS/DFS | PLR ≥ 156.8 |
| [25] | Tsilimigras DI | 2020 | USA | ICCA | 688 | I–III | 57 | 60.50% | Surgery | 22.3 | OS | PLR ≥ 190 |
| [26] | Ohira M | 2020 | Japan | ICCA | 52 | I–IV | 58 | 78.84% | Surgery | NR | OS | PLR ≥ 98 |
| [27] | Ji F | 2020 | China | ECCA | 59 | I–IV | 57 | 55.93% | Surgery | NR | OS | PLR ≥ 268.9 |
| [28] | Huh G | 2020 | Korea | ICCA | 137 | III–IV | 64 | 60.60% | Non-surgery | 9.9 | OS/DFS | PLR ≥ 148 |
| [29] | Wu Y | 2019 | China | CCA | 119 | NR | 60 | 42.90% | Surgery | 11 | OS/DFS | PLR ≥ 157.3 |
| [30] | Sellers CM | 2019 | USA | ICCA | 131 | I–IV | 65 | 51.90% | Surgery | 13 | OS | PLR ≥ 156.4 |
| [31] | Lin J | 2019 | China | ICCA | 218 | I–IV | 60 | 56.90% | Surgery | NR | OS | PLR ≥ 130.6 |
| [32] | Hu HJ | 2019 | China | ECCA | 134 | I-IV | 60 | 63.01% | Surgery | NR | OS | PLR ≥ 150 |
| [33] | Hoshimoto S | 2019 | Japan | ECCA | 53 | I–IV | 70 | 58.00% | Surgery | 18 | OS/DFS | PLR ≥ 187.8 |
| [34] | Buettner S | 2018 | Netherlands | ICCA | 991 | I–IV | 59 | 54.10% | Surgery | 29 | OS | PLR ≥ 190 |
| [35] | Yoh T | 2017 | Japan | ICCA | 141 | I–IV | 65 | 63.00% | Surgery | NR | OS | PLR ≥ 120 |
| [36] | Kitano Y | 2017 | Japan | ECCA | 120 | I–IV | 58 | 68.33% | Surgery | NR | OS/DFS | PLR ≥ 185 |
| [37] | Cho H | 2017 | Korea | ICCA | 305 | III–IV | 59 | 61.50% | Non-surgery | 25 | OS/DFS | PLR ≥ 128.3 |
| [38] | Saito H | 2016 | Japan | ECCA | 121 | I–IV | 70 | 72.72% | Surgery | NR | OS | PLR ≥ 150 |
| [39] | Okuno M | 2016 | Japan | ECCA | 534 | I-IV | 66 | 62.92% | Surgery | 78 | OS | PLR ≥ 150 |
| [40] | Ha H | 2016 | Korea | CCA | 534 | III–IV | 60 | 65.20% | Non-surgery | 95.3 | OS | PLR ≥ 89.6 |
| [41] | Chen Q | 2015 | China | ICCA | 322 | I–IV | 58 | 60.25% | Surgery | NR | OS/DFS | PLR ≥ 123 |
| Ref. | Author | Selection | Comparability | Outcomes | Quality Score |
|---|---|---|---|---|---|
| [22] | Zhao JP | ★★★★ | ★★ | ★★ | 9 |
| [23] | Ma B | ★★★ | ★★ | ★★ | 8 |
| [24] | Zhang ZY | ★★★★ | ★★ | ★★ | 9 |
| [25] | Tsilimigras DI | ★★★★ | ★★ | ★★ | 9 |
| [26] | Ohira M | ★★★★ | ★★ | ★★ | 9 |
| [27] | Ji F | ★★★★ | ★★ | ★★ | 9 |
| [28] | Huh G | ★★★★ | ★★ | ★★ | 9 |
| [29] | Wu Y | ★★★★ | ★★ | ★★ | 9 |
| [30] | Sellers CM | ★★★★ | ★★ | ★★ | 9 |
| [31] | Lin J | ★★★★ | ★★ | ★★ | 9 |
| [32] | Hu HJ | ★★★ | ★★ | ★★ | 8 |
| [33] | Hoshimoto S | ★★★ | ★★ | ★★ | 8 |
| [34] | Buettner S | ★★★★ | ★★ | ★ | 8 |
| [35] | Yoh T | ★★★ | ★★ | ★ | 6 |
| [36] | Kitano Y | ★★★★ | ★★ | ★★ | 9 |
| [37] | Cho H | ★★★★ | ★★ | ★ | 8 |
| [38] | Saito H | ★★★★ | ★★ | ★★ | 9 |
| [39] | Okuno M | ★★★★ | ★★ | ★★ | 9 |
| [40] | Ha H | ★★★★ | ★★ | ★★ | 9 |
| [41] | Chen Q | ★★★★ | ★★ | ★★ | 9 |
| Subgroup | Number of Studies | HR (95% CI) | p Value | Heterogeneity | |
|---|---|---|---|---|---|
| I2 | p | ||||
| Cancer type | |||||
| CCA * | 2 | 1.76 (1.21–2.57) | <0.01 | 0% | 0.44 |
| ICCA | 12 | 1.06 (1.00–1.12) | 0.03 | 35% | 0.12 |
| ECCA | 6 | 1.37 (0.93–2.03) | 0.11 | 60% | 0.03 |
| Treatment | |||||
| Surgery | 17 | 1.09 (1.02–1.17) | 0.02 | 48% | 0.01 |
| Non-surgery | 3 | 1.58 (1.23–2.04) | <0.01 | 0% | 0.43 |
| Cut-off value | |||||
| PLR ≥ 150 | 11 | 1.17 (1.02–1.33) | 0.02 | 60% | <0.01 |
| PLR < 150 | 9 | 1.25 (1.03–1.51) | 0.02 | 53% | 0.03 |
| Sample size | |||||
| ≥200 | 10 | 1.07 (1.01–1.13) | 0.02 | 32% | 0.15 |
| <200 | 10 | 1.38 (1.07–1.77) | 0.01 | 69% | 0.01 |
| Age ** | |||||
| ≥60 | 9 | 1.48 (1.18–1.85) | <0.01 | 36% | 0.13 |
| <60 | 11 | 1.06 (1.00–1.12) | 0.05 | 40% | 0.08 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, D.; Czigany, Z.; Heij, L.R.; Bouwense, S.A.W.; van Dam, R.; Lang, S.A.; Ulmer, T.F.; Neumann, U.P.; Bednarsch, J. The Value of Platelet-to-Lymphocyte Ratio as a Prognostic Marker in Cholangiocarcinoma: A Systematic Review and Meta-Analysis. Cancers 2022, 14, 438. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14020438
Liu D, Czigany Z, Heij LR, Bouwense SAW, van Dam R, Lang SA, Ulmer TF, Neumann UP, Bednarsch J. The Value of Platelet-to-Lymphocyte Ratio as a Prognostic Marker in Cholangiocarcinoma: A Systematic Review and Meta-Analysis. Cancers. 2022; 14(2):438. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14020438
Chicago/Turabian StyleLiu, Dong, Zoltan Czigany, Lara R. Heij, Stefan A. W. Bouwense, Ronald van Dam, Sven A. Lang, Tom F. Ulmer, Ulf P. Neumann, and Jan Bednarsch. 2022. "The Value of Platelet-to-Lymphocyte Ratio as a Prognostic Marker in Cholangiocarcinoma: A Systematic Review and Meta-Analysis" Cancers 14, no. 2: 438. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14020438