
Outcomes of Different Haploidentical Transplantation Strategies from the Taiwan Blood and Marrow Transplantation Registry

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods and Materials
2.1. Patients and Stem Cell Source
2.2. Conditioning Regimens and Graft-Versus-Host-Disease Prophylaxis/Diagnosis
2.3. Endpoint Definitions and Statistical Analysis
3. Results
3.1. Basic Characteristics
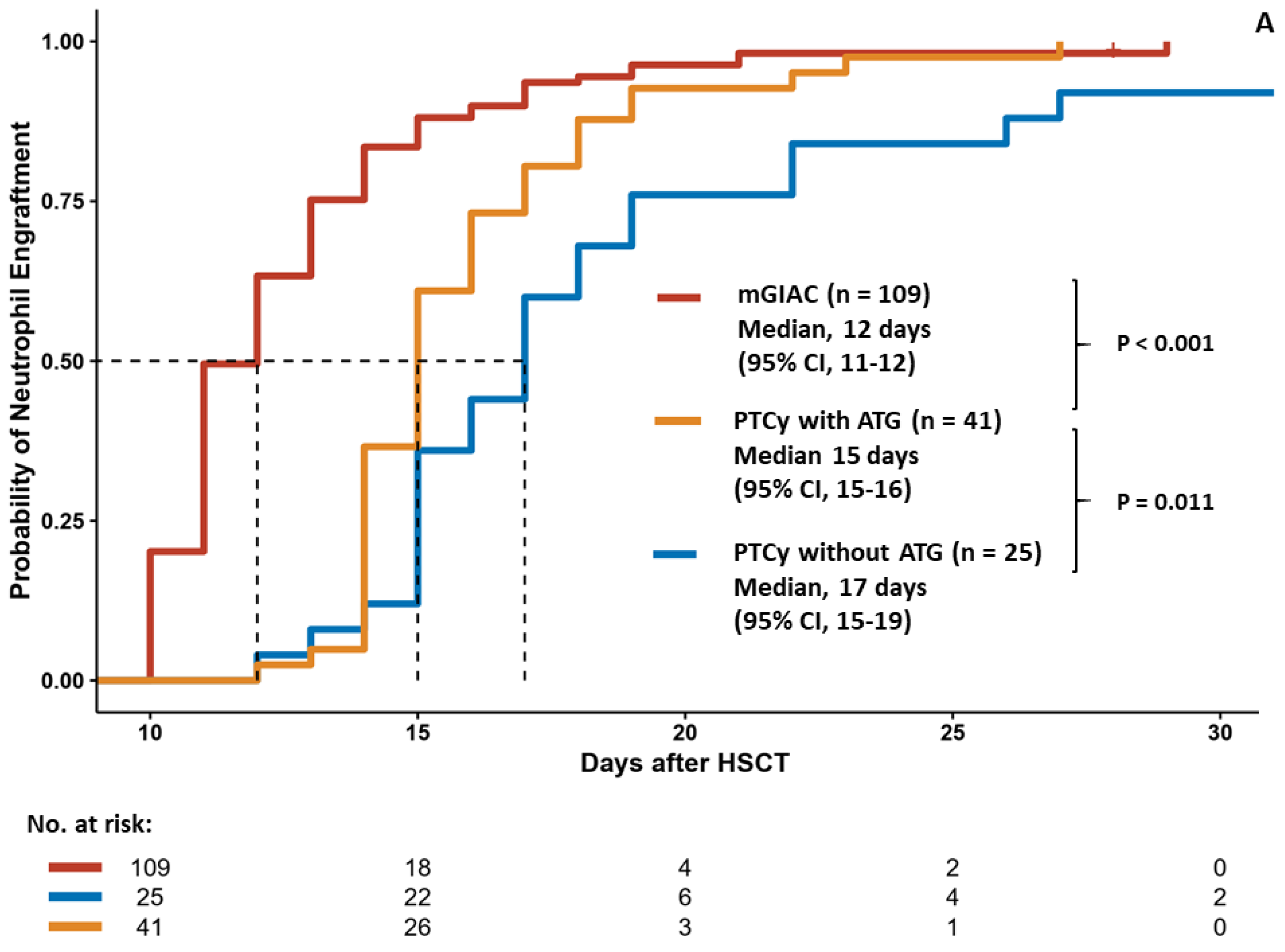
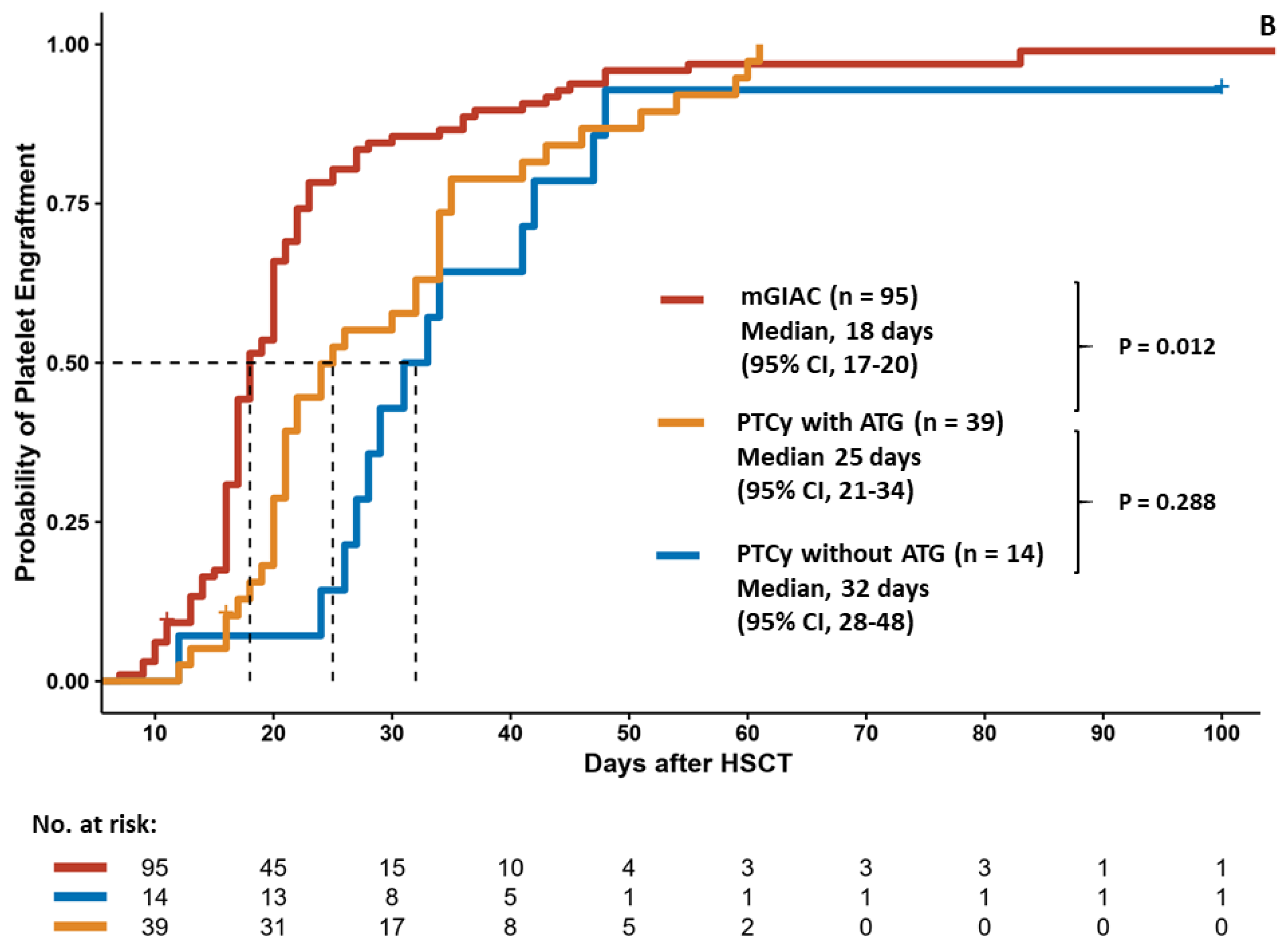
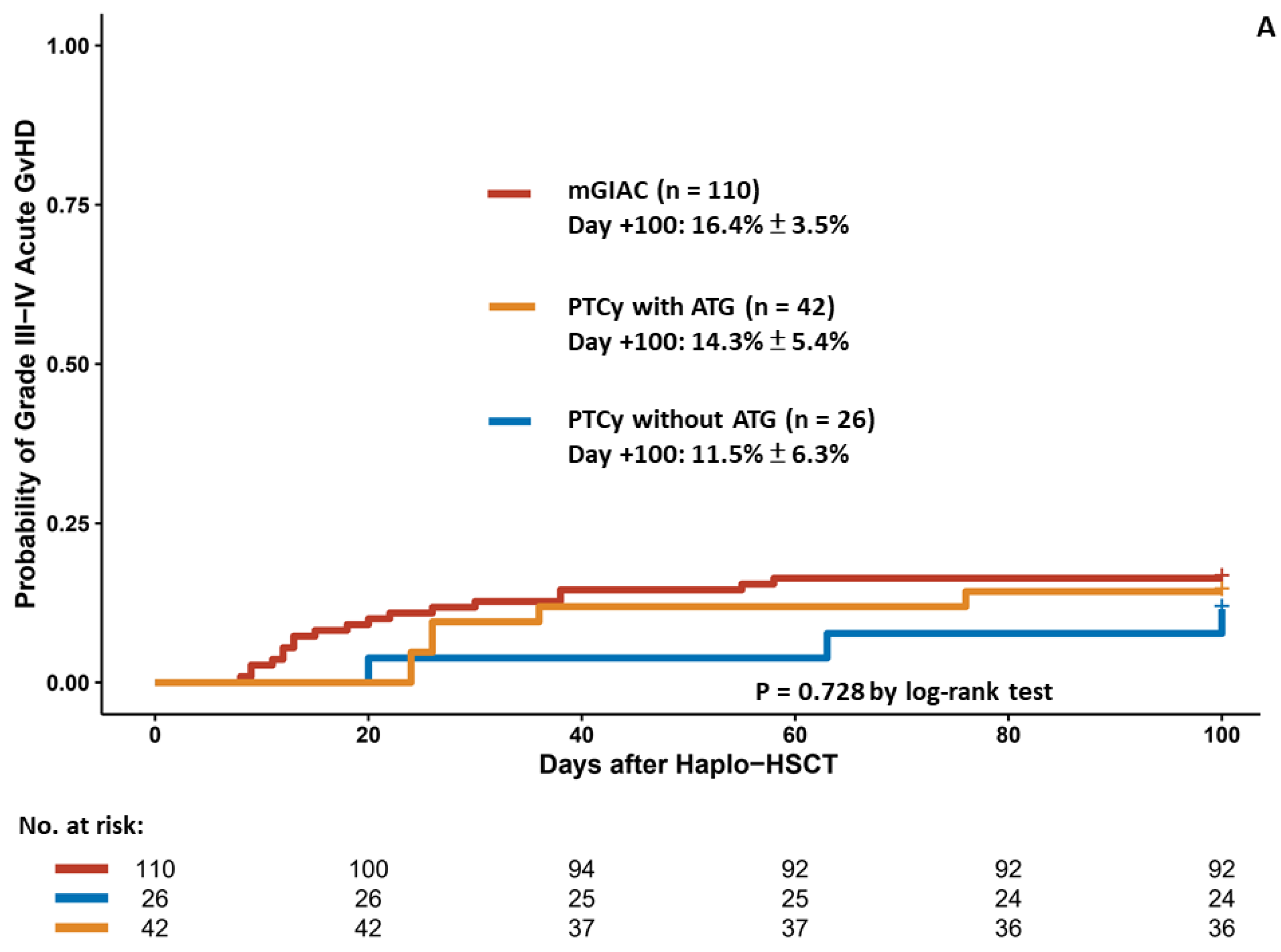
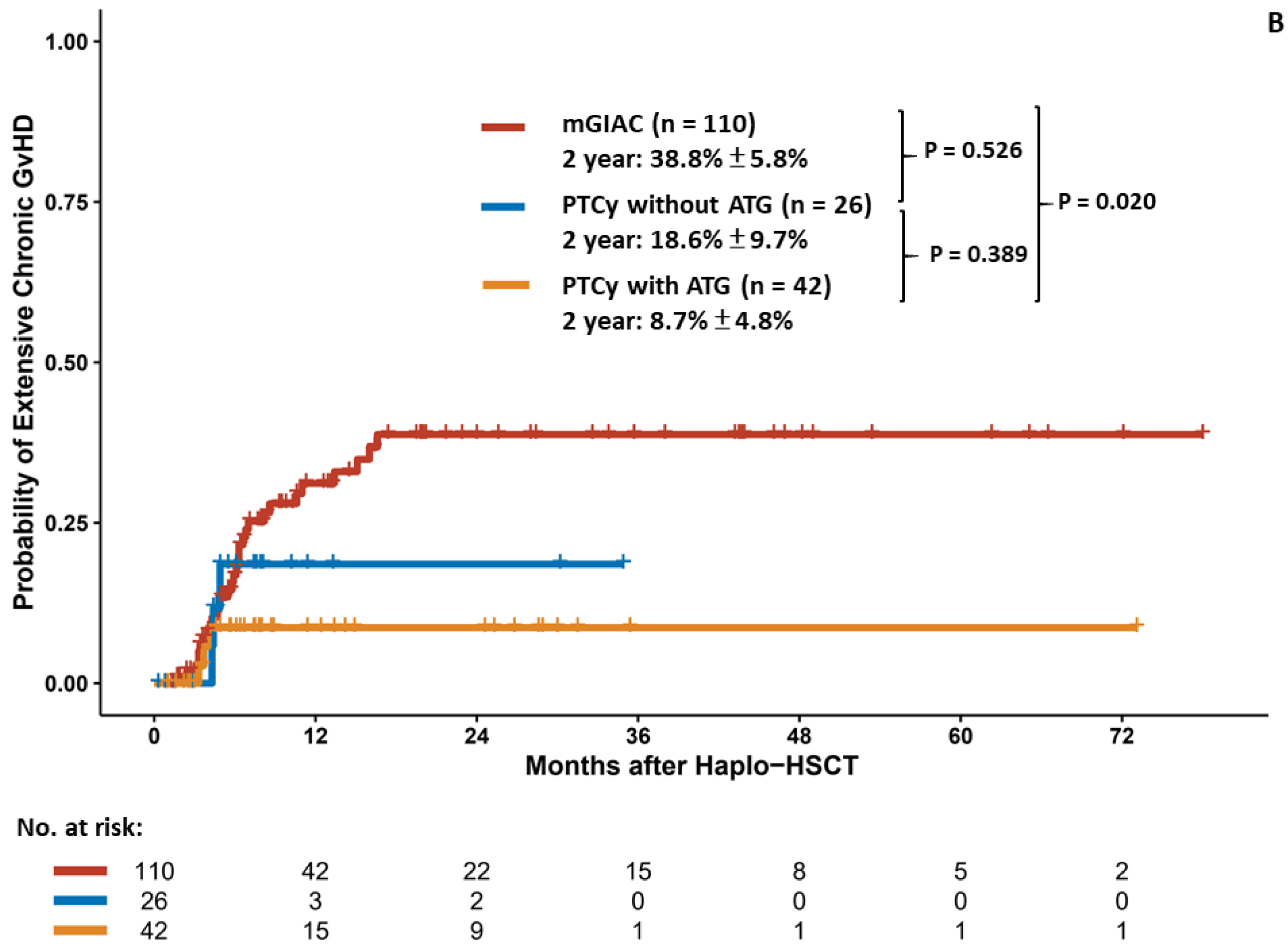
3.2. Engraftment Kinetics and Graft–Versus–Host Disease
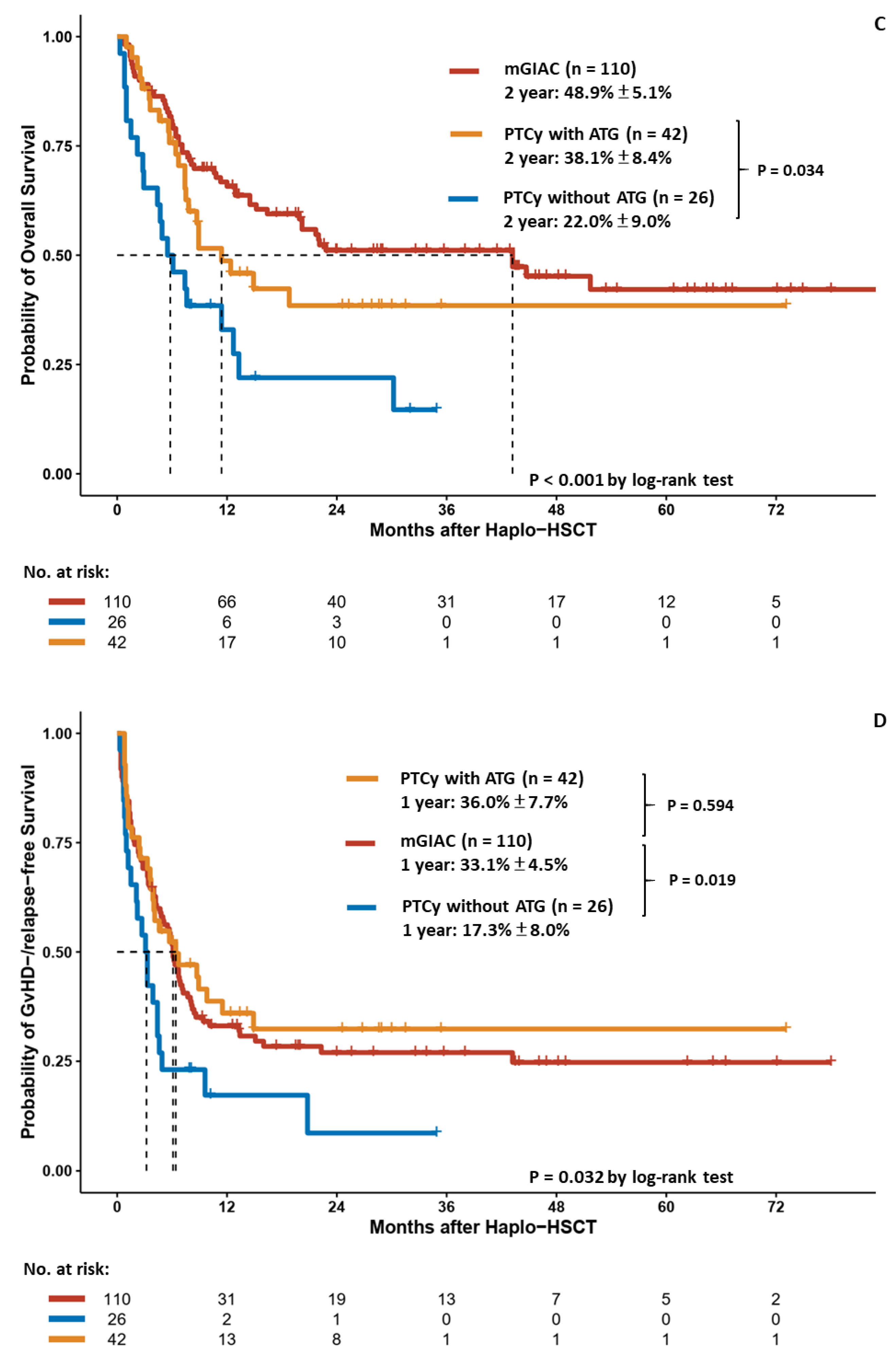
3.3. Relapse and Survival Analyses of Different Haplo–HSCT Strategies
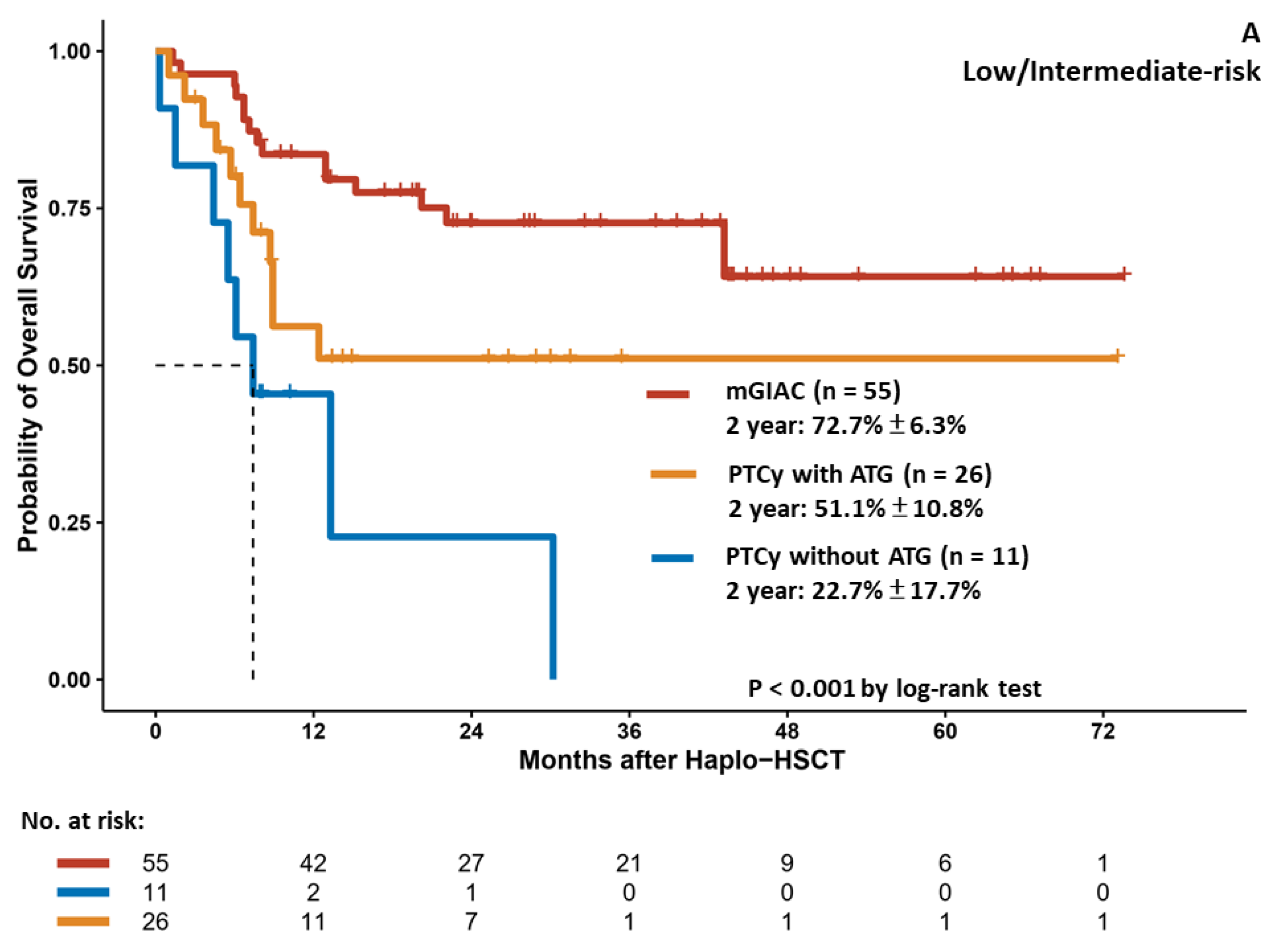
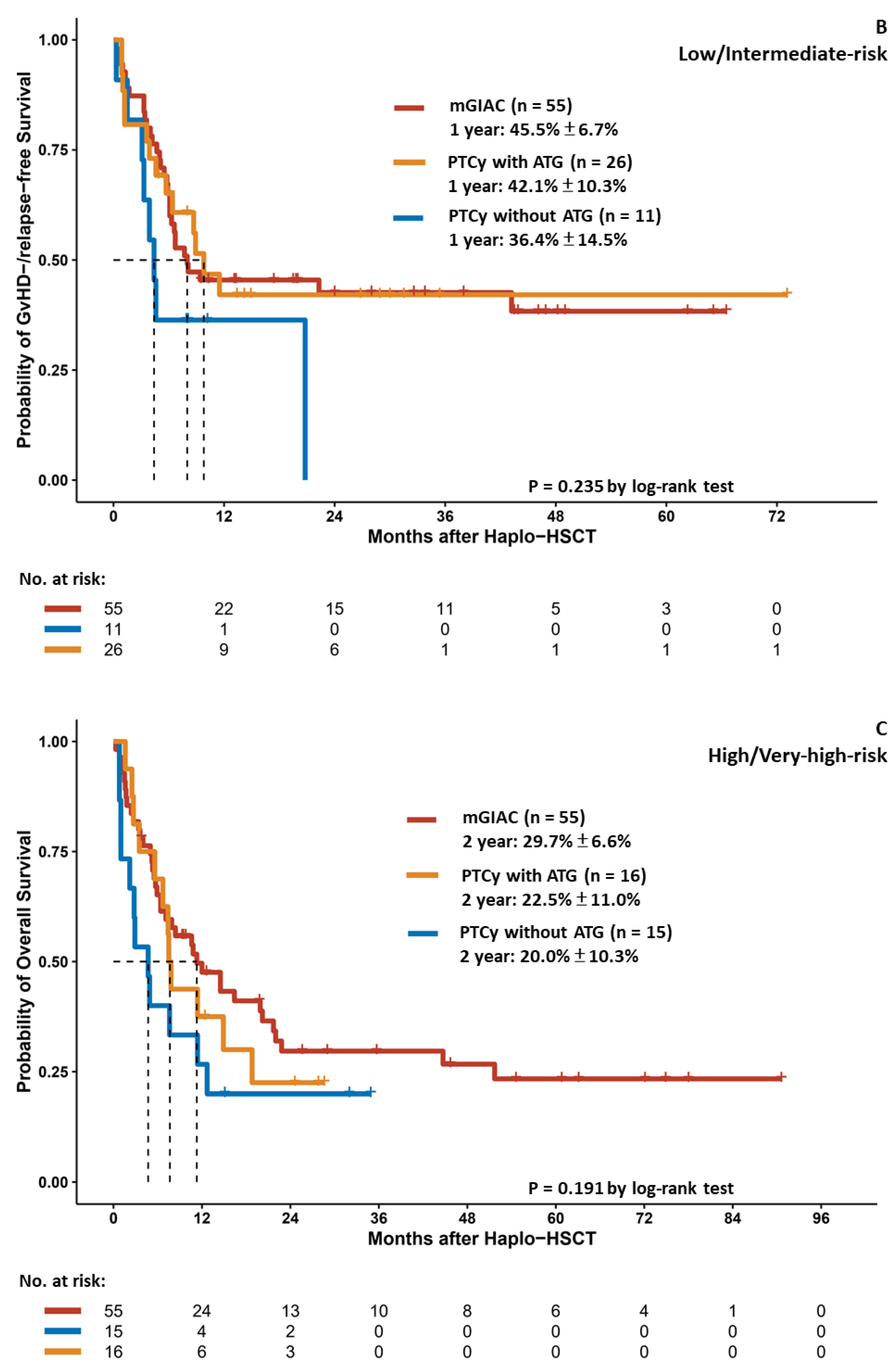
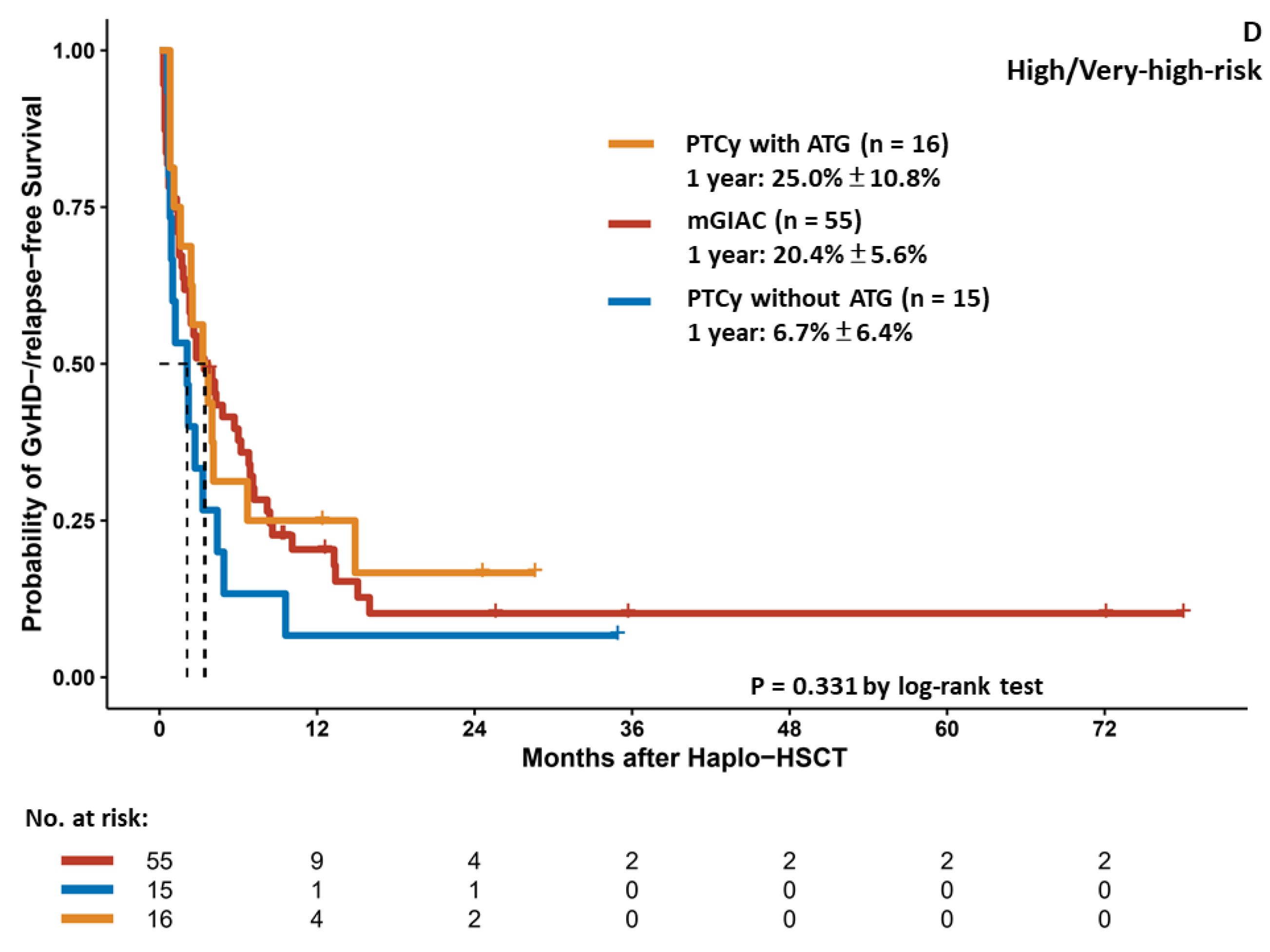
3.4. Outcome Analysis of Different Haplo–HSCT Strategies Stratified by Pre–HSCT Disease Status
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ottinger, H.; Grosse-Wilde, M.; Schmitz, A.; Grosse-Wilde, H. Immunogenetic marrow donor search for 1012 patients: A retrospective analysis of strategies, outcome and costs. Bone Marrow Transplant. 1994, 14 (Suppl. S4), S34–S38. [Google Scholar]
- Gragert, L.; Eapen, M.; Williams, E.; Freeman, J.; Spellman, S.; Baitty, R.; Hartzman, R.; Rizzo, J.D.; Horowitz, M.; Confer, D.; et al. HLA match likelihoods for hematopoietic stem-cell grafts in the U.S. registry. N. Engl. J. Med. 2014, 371, 339–348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aversa, F.; Terenzi, A.; Tabilio, A.; Falzetti, F.; Carotti, A.; Ballanti, S.; Felicini, R.; Falcinelli, F.; Velardi, A.; Ruggeri, L.; et al. Full haplotype-mismatched hematopoietic stem-cell transplantation: A phase II study in patients with acute leukemia at high risk of relapse. J. Clin. Oncol. 2005, 23, 3447–3454. [Google Scholar] [CrossRef]
- Luznik, L.; O’Donnell, P.V.; Symons, H.J.; Chen, A.R.; Leffell, M.S.; Zahurak, M.; Gooley, T.A.; Piantadosi, S.; Kaup, M.; Ambinder, R.F.; et al. HLA-haploidentical bone marrow transplantation for hematologic malignancies using nonmyeloablative conditioning and high-dose, posttransplantation cyclophosphamide. Biol. Blood Marrow Transplant. 2008, 14, 641–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Solomon, S.R.; Sizemore, C.A.; Sanacore, M.; Zhang, X.; Brown, S.; Holland, H.K.; Morris, L.E.; Bashey, A. Haploidentical transplantation using T cell replete peripheral blood stem cells and myeloablative conditioning in patients with high-risk hematologic malignancies who lack conventional donors is well tolerated and produces excellent relapse-free survival: Results of a prospective phase II trial. Biol. Blood Marrow Transplant. 2012, 18, 1859–1866. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castagna, L.; Crocchiolo, R.; Furst, S.; Bramanti, S.; El Cheikh, J.; Sarina, B.; Granata, A.; Mauro, E.; Faucher, C.; Mohty, B.; et al. Bone marrow compared with peripheral blood stem cells for haploidentical transplantation with a nonmyeloablative conditioning regimen and post-transplantation cyclophosphamide. Biol. Blood Marrow Transplant. 2014, 20, 724–729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Law, A.D.; Salas, M.Q.; Lam, W.; Michelis, F.V.; Thyagu, S.; Kim, D.D.H.; Lipton, J.H.; Kumar, R.; Messner, H.; Viswabandya, A. Reduced-Intensity Conditioning and Dual T Lymphocyte Suppression with Antithymocyte Globulin and Post-Transplant Cyclophosphamide as Graft-versus-Host Disease Prophylaxis in Haploidentical Hematopoietic Stem Cell Transplants for Hematological Malignancies. Biol. Blood Marrow Transplant. 2018, 24, 2259–2264. [Google Scholar] [CrossRef] [Green Version]
- Al Dawsari, G.; Hassanein, M.F.R.; Rasheed, W.; Almohareb, F.; Chaudhri, N.A.; Alsharif, F.; Al Zahrani, H.; Mohamed, S.Y.; Hanbali, A.; Ahmed, S.O.; et al. Addition of ATG to Myeloablative Haplo Conditioning with Post-Transplantation Cyclophosphamide Might Decrease the Risk of Gvhd and TRM without Increasing the Risk of Relapse. Blood 2016, 128, 5871. [Google Scholar] [CrossRef]
- Luznik, L.; Jalla, S.; Engstrom, L.W.; Iannone, R.; Fuchs, E.J. Durable engraftment of major histocompatibility complex-incompatible cells after nonmyeloablative conditioning with fludarabine, low-dose total body irradiation, and posttransplantation cyclophosphamide. Blood 2001, 98, 3456–3464. [Google Scholar] [CrossRef] [Green Version]
- Luznik, L.; Bolanos-Meade, J.; Zahurak, M.; Chen, A.R.; Smith, B.D.; Brodsky, R.; Huff, C.A.; Borrello, I.; Matsui, W.; Powell, J.D.; et al. High-dose cyclophosphamide as single-agent, short-course prophylaxis of graft-versus-host disease. Blood 2010, 115, 3224–3230. [Google Scholar] [CrossRef] [Green Version]
- Huang, X.J.; Liu, D.H.; Liu, K.Y.; Xu, L.P.; Chen, H.; Han, W.; Chen, Y.H.; Wang, J.Z.; Gao, Z.Y.; Zhang, Y.C.; et al. Haploidentical hematopoietic stem cell transplantation without in vitro T-cell depletion for the treatment of hematological malignancies. Bone Marrow Transplant. 2006, 38, 291–297. [Google Scholar] [CrossRef] [Green Version]
- Chang, Y.J.; Huang, X.J. Haploidentical stem cell transplantation: Anti-thymocyte globulin-based experience. Semin. Hematol. 2016, 53, 82–89. [Google Scholar] [CrossRef]
- Ciurea, S.O.; Zhang, M.J.; Bacigalupo, A.A.; Bashey, A.; Appelbaum, F.R.; Aljitawi, O.S.; Armand, P.; Antin, J.H.; Chen, J.; Devine, S.M.; et al. Haploidentical transplant with posttransplant cyclophosphamide vs matched unrelated donor transplant for acute myeloid leukemia. Blood 2015, 126, 1033–1040. [Google Scholar] [CrossRef] [Green Version]
- Gagelmann, N.; Bacigalupo, A.; Rambaldi, A.; Hoelzer, D.; Halter, J.; Sanz, J.; Bonifazi, F.; Meijer, E.; Itala-Remes, M.; Markova, M.; et al. Haploidentical Stem Cell Transplantation With Posttransplant Cyclophosphamide Therapy vs Other Donor Transplantations in Adults With Hematologic Cancers: A Systematic Review and Meta-analysis. JAMA Oncol. 2019, 5, 1739–1748. [Google Scholar] [CrossRef]
- Holtan, S.G.; Versluis, J.; Weisdorf, D.J.; Cornelissen, J.J. Optimizing Donor Choice and GVHD Prophylaxis in Allogeneic Hematopoietic Cell Transplantation. J. Clin. Oncol. 2021, 39, 373–385. [Google Scholar] [CrossRef]
- Nagler, A.; Dholaria, B.; Labopin, M.; Savani, B.N.; Angelucci, E.; Koc, Y.; Arat, M.; Pioltelli, P.; Sica, S.; Gulbas, Z.; et al. Bone marrow versus mobilized peripheral blood stem cell graft in T-cell-replete haploidentical transplantation in acute lymphoblastic leukemia. Leukemia 2020, 34, 2766–2775. [Google Scholar] [CrossRef]
- Armand, P.; Kim, H.T.; Logan, B.R.; Wang, Z.; Alyea, E.P.; Kalaycio, M.E.; Maziarz, R.T.; Antin, J.H.; Soiffer, R.J.; Weisdorf, D.J.; et al. Validation and refinement of the Disease Risk Index for allogeneic stem cell transplantation. Blood 2014, 123, 3664–3671. [Google Scholar] [CrossRef]
- Bacigalupo, A.; Ballen, K.; Rizzo, D.; Giralt, S.; Lazarus, H.; Ho, V.; Apperley, J.; Slavin, S.; Pasquini, M.; Sandmaier, B.M.; et al. Defining the intensity of conditioning regimens: Working definitions. Biol. Blood Marrow Transplant. 2009, 15, 1628–1633. [Google Scholar] [CrossRef] [Green Version]
- Bacigalupo, A.; Dominietto, A.; Ghiso, A.; Di Grazia, C.; Lamparelli, T.; Gualandi, F.; Bregante, S.; Van Lint, M.T.; Geroldi, S.; Luchetti, S.; et al. Unmanipulated haploidentical bone marrow transplantation and post-transplant cyclophosphamide for hematologic malignanices following a myeloablative conditioning: An update. Bone Marrow Transplant. 2015, 50 (Suppl. S2), S37–S39. [Google Scholar] [CrossRef]
- Przepiorka, D.; Weisdorf, D.; Martin, P.; Klingemann, H.G.; Beatty, P.; Hows, J.; Thomas, E.D. 1994 Consensus Conference on Acute GVHD Grading. Bone Marrow Transplant. 1995, 15, 825–828. [Google Scholar]
- Lee, S.J.; Vogelsang, G.; Flowers, M.E. Chronic graft-versus-host disease. Biol. Blood Marrow Transplant. 2003, 9, 215–233. [Google Scholar] [CrossRef] [Green Version]
- Abraham, S.K.; Arnon, N.; Bipin, S. Summary of Scientific and Statistical Methods, Study Endpoints and Definitions for Observational and Registry-Based Studies in Hematopoietic Cell Transplantation. Clin. Hematol. Int. 2019, 2, 2–4. [Google Scholar]
- Passweg, J.R.; Baldomero, H.; Chabannon, C.; Basak, G.W.; Corbacioglu, S.; Duarte, R.; Dolstra, H.; Lankester, A.C.; Mohty, M.; Montoto, S.; et al. The EBMT activity survey on hematopoietic-cell transplantation and cellular therapy 2018: CAR-T’s come into focus. Bone Marrow Transplant. 2020, 55, 1604–1613. [Google Scholar] [CrossRef] [Green Version]
- Phelan, R.; Arora, M.; Chen, M. Current Use and Outcome of Hematopoietic Stem Cell Transplantation: CIBMTR US Summary Slides. 2020. Available online: https://www.cibmtr.org/ReferenceCenter/SlidesReports/SummarySlides/pages/index.aspx (accessed on 20 January 2022).
- Ringden, O.; Labopin, M.; Beelen, D.W.; Volin, L.; Ehninger, G.; Finke, J.; Greinix, H.T.; Kyrcz-Krzemien, S.; Bunjes, D.; Brinch, L.; et al. Bone marrow or peripheral blood stem cell transplantation from unrelated donors in adult patients with acute myeloid leukaemia, an Acute Leukaemia Working Party analysis in 2262 patients. J. Int. Med. 2012, 272, 472–483. [Google Scholar] [CrossRef] [PubMed]
- Chiusolo, P.; Bug, G.; Olivieri, A.; Brune, M.; Mordini, N.; Alessandrino, P.E.; Dominietto, A.; Raiola, A.M.; Di Grazia, C.; Gualandi, F.; et al. A Modified Post-Transplant Cyclophosphamide Regimen, for Unmanipulated Haploidentical Marrow Transplantation, in Acute Myeloid Leukemia: A Multicenter Study. Biol. Blood Marrow Transplant. 2018, 24, 1243–1249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kasamon, Y.L.; Fuchs, E.J.; Zahurak, M.; Rosner, G.L.; Symons, H.J.; Gladstone, D.E.; Huff, C.A.; Swinnen, L.J.; Brodsky, R.A.; Matsui, W.H.; et al. Shortened-Duration Tacrolimus after Nonmyeloablative, HLA-Haploidentical Bone Marrow Transplantation. Biol. Blood Marrow Transplant. 2018, 24, 1022–1028. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, D.P.; Dong, L.; Wu, T.; Huang, X.J.; Zhang, M.J.; Han, W.; Chen, H.; Liu, D.H.; Gao, Z.Y.; Chen, Y.H.; et al. Conditioning including antithymocyte globulin followed by unmanipulated HLA-mismatched/haploidentical blood and marrow transplantation can achieve comparable outcomes with HLA-identical sibling transplantation. Blood 2006, 107, 3065–3073. [Google Scholar] [CrossRef]
- Bashey, A.; Zhang, M.J.; McCurdy, S.R.; St Martin, A.; Argall, T.; Anasetti, C.; Ciurea, S.O.; Fasan, O.; Gaballa, S.; Hamadani, M.; et al. Mobilized Peripheral Blood Stem Cells Versus Unstimulated Bone Marrow As a Graft Source for T-Cell-Replete Haploidentical Donor Transplantation Using Post-Transplant Cyclophosphamide. J. Clin. Oncol. 2017, 35, 3002–3009. [Google Scholar] [CrossRef]
- Grosso, D.; Carabasi, M.; Filicko-O’Hara, J.; Kasner, M.; Wagner, J.L.; Colombe, B.; Cornett Farley, P.; O’Hara, W.; Flomenberg, P.; Werner-Wasik, M.; et al. A 2-step approach to myeloablative haploidentical stem cell transplantation: A phase 1/2 trial performed with optimized T-cell dosing. Blood 2011, 118, 4732–4739. [Google Scholar] [CrossRef] [Green Version]
- Raj, K.; Pagliuca, A.; Bradstock, K.; Noriega, V.; Potter, V.; Streetly, M.; McLornan, D.; Kazmi, M.; Marsh, J.; Kwan, J.; et al. Peripheral blood hematopoietic stem cells for transplantation of hematological diseases from related, haploidentical donors after reduced-intensity conditioning. Biol. Blood Marrow Transplant. 2014, 20, 890–895. [Google Scholar] [CrossRef] [Green Version]
- Kanakry, C.G.; Fuchs, E.J.; Luznik, L. Modern approaches to HLA-haploidentical blood or marrow transplantation. Nat. Rev. Clin. Oncol. 2016, 13, 10–24. [Google Scholar] [CrossRef] [Green Version]
- Wolschke, C.; Zabelina, T.; Ayuk, F.; Alchalby, H.; Berger, J.; Klyuchnikov, E.; Pein, U.M.; Schumacher, S.; Amtsfeld, G.; Adjalle, R.; et al. Effective prevention of GVHD using in vivo T-cell depletion with anti-lymphocyte globulin in HLA-identical or -mismatched sibling peripheral blood stem cell transplantation. Bone Marrow Transplant. 2014, 49, 126–130. [Google Scholar] [CrossRef] [Green Version]
- Ravinet, A.; Cabrespine, A.; Socie, G.; Milpied, N.; Yakoub Agha, I.; Nguyen, S.; Michallet, M.; Menard, A.L.; Maillard, N.; Mohty, M.; et al. Impact of Thymoglobulin by Stem Cell Source (Peripheral Blood Stem Cell or Bone Marrow) After Myeloablative Stem Cell Transplantation From HLA 10/10-Matched Unrelated Donors: A Report From the Societe Francaise de Greffe de Moelle et de Therapie Cellulaire. Transplantation 2016, 100, 1732–1739. [Google Scholar] [CrossRef]
- Zander, A.R.; Kroger, N.; Schleuning, M.; Finke, J.; Zabelina, T.; Beelen, D.; Schwerdtfeger, R.; Baurmann, H.; Bornhauser, M.; Ehninger, G.; et al. ATG as part of the conditioning regimen reduces transplant-related mortality (TRM) and improves overall survival after unrelated stem cell transplantation in patients with chronic myelogenous leukemia (CML). Bone Marrow Transplant. 2003, 32, 355–361. [Google Scholar] [CrossRef] [Green Version]
- Kroger, N.; Solano, C.; Wolschke, C.; Bandini, G.; Patriarca, F.; Pini, M.; Nagler, A.; Selleri, C.; Risitano, A.; Messina, G.; et al. Antilymphocyte Globulin for Prevention of Chronic Graft-versus-Host Disease. N. Engl. J. Med. 2016, 374, 43–53. [Google Scholar] [CrossRef]
- Ruggeri, A.; Labopin, M.; Bacigalupo, A.; Gulbas, Z.; Koc, Y.; Blaise, D.; Bruno, B.; Irrera, G.; Tischer, J.; Diez-Martin, J.L.; et al. Bone marrow versus mobilized peripheral blood stem cells in haploidentical transplants using posttransplantation cyclophosphamide. Cancer 2018, 124, 1428–1437. [Google Scholar] [CrossRef]
- Holtick, U.; Albrecht, M.; Chemnitz, J.M.; Theurich, S.; Skoetz, N.; Scheid, C.; von Bergwelt-Baildon, M. Bone marrow versus peripheral blood allogeneic haematopoietic stem cell transplantation for haematological malignancies in adults. Cochrane Database Syst. Rev. 2014. [Google Scholar] [CrossRef]
- Chemaly, R.F.; Ullmann, A.J.; Stoelben, S.; Richard, M.P.; Bornhauser, M.; Groth, C.; Einsele, H.; Silverman, M.; Mullane, K.M.; Brown, J.; et al. Letermovir for cytomegalovirus prophylaxis in hematopoietic-cell transplantation. N. Engl. J. Med. 2014, 370, 1781–1789. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Total (n = 178) | Modified GIAC (n = 110, 61.8%) | PTCy without ATG (n = 26, 14.6%) | PTCy with ATG (n = 42, 23.6%) | p Value |
|---|---|---|---|---|---|
| Sex α | 0.518 | ||||
| Male | 88 (49.4%) | 52 (47.3%) | 12 (46.2%) | 24 (57.1%) | |
| Female | 90 (50.6%) | 58 (52.7%) | 14 (53.8%) | 18 (42.9%) | |
| Age, years βγ | 45.2 (18.7–75.6) | 42.3 (18.7–69.2) | 50.1 (21.8–75.6) | 49.4 (18.9–68.3) | 0.098 |
| Disease α | |||||
| AML | 106 (59.6%) | 65 (59.1%) | 13 (50.0%) | 28 (66.7%) | 0.391 |
| MDS | 11 (6.2%) | 9 (8.2%) | 0 (0%) | 2 (4.8%) | 0.270 |
| MDS/MPN | 5 (2.8%) | 1 (0.9%) | 3 (11.5%) | 1 (2.4%) | 0.013 |
| ALL | 32 (18.0%) | 24 (21.8%) | 3 (11.5%) | 5 (11.9%) | 0.237 |
| MPAL | 2 (1.1%) | 2 (1.8%) | 0 (0%) | 0 (0%) | 0.535 |
| CML | 6 (3.4%) | 3 (2.5%) | 1 (3.8%) | 2 (4.8%) | 0.816 |
| NHL | 12 (6.7%) | 3 (2.7%) | 6 (23.1%) | 3 (7.1%) | 0.001 |
| HL | 3 (1.7%) | 2 (1.8%) | 0 (0%) | 1 (2.4%) | 0.748 |
| Myeloma | 1 (0.6%) | 1 (0.9%) | 0 (0%) | 0 (0%) | 0.733 |
| Conditioning α | 0.229 | ||||
| Myeloablative | 53 (29.8%) | 25 (22.7%) | 10 (38.5%) | 18 (42.9%) | |
| Reduced intensity | 125 (70.2%) | 85 (77.3%) | 16 (61.5%) | 24 (57.1%) | |
| ATG dose per kilogram β | 6.0 (2.0–7.5) | 6.0 (5.0–7.5) | 0 | 4.0 (2.0–7.5) | <0.001 |
| Stem cell source α | <0.001 | ||||
| BM + mobilized PB | 110 (61.8%) | 110 (100%) | 0 (0%) | 0 (0%) | |
| Mobilized PB | 68 (38.2%) | 0 (0%) | 26 (100%) | 42 (100%) | |
| Donor relationship α | 0.106 | ||||
| Child | 85 (47.8%) | 46 (41.8%) | 17 (65.4%) | 22 (52.4%) | |
| Parent | 43 (24.2%) | 33 (30.0%) | 2 (7.7%) | 8 (19.0%) | |
| Sibling | 50 (28.1%) | 31 (28.2%) | 7 (26.9%) | 12 (28.6%) | |
| Donor–recipient sex combination α | 0.659 | ||||
| Female donor to male recipient | 47 (26.4%) | 30 (27.3%) | 5 (19.2%) | 12 (28.6%) | |
| Other combinations | 131 (73.6%) | 80 (72.7%) | 21 (80.8%) | 30 (71.4%) | |
| Donor–recipient CMV serostatus αδ | 0.073 γ | ||||
| Negative–Negative | 3 (1.7%) | 1 (0.9%) | 1 (3.8%) | 1 (2.4%) | |
| Negative–Positive | 40 (22.5%) | 23 (20.9%) | 11 (42.3%) | 6 (14.3%) | |
| Positive–Negative | 11 (6.2%) | 9 (8.2%) | 1 (3.8%) | 1 (2.4%) | |
| Positive–Positive | 121 (68.0%) | 77 (70.0%) | 12 (46.2%) | 32 (76.2%) | |
| Missing | 3 (1.7%) | 0 (0%) | 1 (3.8%) | 2 (4.8) | |
| CD34 (106/kg) βε | 5.08 (1.3–21.2) | 5.0 (2.2–8.5) | 5.87 (3.0–20.7) | 6.0 (1.3–21.2) | <0.001 |
| Disease Risk Index α | 0.069 | ||||
| Low | 11 (6.2%) | 8 (7.3%) | 0 (0%) | 3 (7.1%) | |
| Intermediate | 81 (45.5%) | 47 (42.7%) | 11 (42.3%) | 23 (54.8%) | |
| High | 71 (39.9%) | 46 (41.8%) | 15 (57.7%) | 10 (23.8%) | |
| Very high | 15 (8.4%) | 9 (8.2%) | 0 (0%) | 6 (14.3%) | |
| Year of HSCT | 2016 (2011–2019) | 2016 (2012–2019) | 2016 (2014–2019) | 2016 (2011–2019) | 0.980 |
| Variables | Cumulative Incidence of Relapse | Nonrelapse Mortality | GvHD/Relapse-Free Survival | Overall Survival | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HR | Lower | Upper | p Value | HR | Lower | Upper | p Value | HR | Lower | Upper | p Value | HR | Lower | Upper | p Value | |
| Age α | 0.986 | 0.969 | 1.001 | 0.125 | 1.015 | 0.992 | 1.039 | 0.198 | 0.997 | 0.985 | 1.010 | 0.650 | 1.002 | 0.987 | 1.016 | 0.803 |
| Disease risk index β | 4.421 | 2..422 | 8.070 | <0.001 | 1.157 | 0.595 | 2.248 | 0.668 | 1.976 | 1.326 | 2.944 | 0.001 | 2.565 | 1.625 | 4.049 | <0.001 |
| Conditioning intensity γ | 0.591 | 0.325 | 1.077 | 0.086 | 1.607 | 0.716 | 3.608 | 0.250 | 0.871 | 0.558 | 1.359 | 0.543 | 1.059 | 0.635 | 1.765 | 0.826 |
| Acute GvHD, gr III–IV | 1.460 | 0.748 | 2.850 | 0.267 | 2.431 | 1.124 | 5.260 | 0.024 | 11.327 | 6.485 | 19.785 | <0.001 | 1.695 | 0.999 | 2.877 | 0.051 |
| Chronic GvHD, extensive | 0.585 | 0.310 | 1.105 | 0.099 | 0.192 | 0.057 | 0.652 | 0.008 | 1.758 | 1.137 | 2.719 | 0.011 | 0.348 | 0.191 | 0.633 | 0.001 |
| Recipient CMV serostatus δ | 1.969 | 0.589 | 6.579 | 0.271 | 2.375 | 0.310 | 18.212 | 0.405 | 1.313 | 0.657 | 2.627 | 0.441 | 3.723 | 0.894 | 15.498 | 0.071 |
| Haplo-HSCT strategies | ||||||||||||||||
| PTCy with ATG vs. mGIAC | 1.069 | 0.547 | 2.064 | 0.858 | 1.305 | 0.608 | 2.801 | 0.494 | 1.013 | 0.630 | 1.630 | 0.957 | 1.316 | 0.783 | 2.121 | 0.300 |
| PTCy without ATG vs. mGIAC | 1.786 | 0.917 | 3.477 | 0.088 | 2.520 | 1.089 | 5.831 | 0.031 | 1.586 | 0.955 | 2.634 | 0.075 | 2.521 | 1.466 | 4.336 | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsai, X.C.-H.; Chen, T.-T.; Gau, J.-P.; Wang, P.-N.; Liu, Y.-C.; Lien, M.-Y.; Li, C.-C.; Yao, M.; Ko, B.-S. Outcomes of Different Haploidentical Transplantation Strategies from the Taiwan Blood and Marrow Transplantation Registry. Cancers 2022, 14, 1097. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14041097
Tsai XC-H, Chen T-T, Gau J-P, Wang P-N, Liu Y-C, Lien M-Y, Li C-C, Yao M, Ko B-S. Outcomes of Different Haploidentical Transplantation Strategies from the Taiwan Blood and Marrow Transplantation Registry. Cancers. 2022; 14(4):1097. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14041097
Chicago/Turabian StyleTsai, Xavier Cheng-Hong, Tzu-Ting Chen, Jyh-Pyng Gau, Po-Nan Wang, Yi-Chang Liu, Ming-Yu Lien, Chi-Cheng Li, Ming Yao, and Bor-Sheng Ko. 2022. "Outcomes of Different Haploidentical Transplantation Strategies from the Taiwan Blood and Marrow Transplantation Registry" Cancers 14, no. 4: 1097. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14041097