
The Impact of Cognitive Impairment on Treatment Toxicity, Treatment Completion, and Survival among Older Adults Receiving Chemotherapy: A Systematic Review

 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Information Sources, Search Strategy, and Selection Process
2.2. Eligibility
- Were clinical trials, prospective cohort, retrospective cohort, or case–control studies;
- Included patients aged ≥65 or a subgroup analysis of patients aged ≥65;
- Focused on patients with a cancer diagnosis (any site, stage; with the exception of brain tumor or brain metastases) AND with CI (screened positive for CI prior to receiving cytotoxic chemotherapy or with documented medical history of CI);
- Examined specific chemotherapy treatment endpoints (i.e., survival, treatment completion, or treatment toxicity); and
- Had their full text published in English or Spanish.
2.3. Data Collection Process and Data Items
2.4. Risk of Bias Assessment
2.5. Synthesis Methods
3. Results
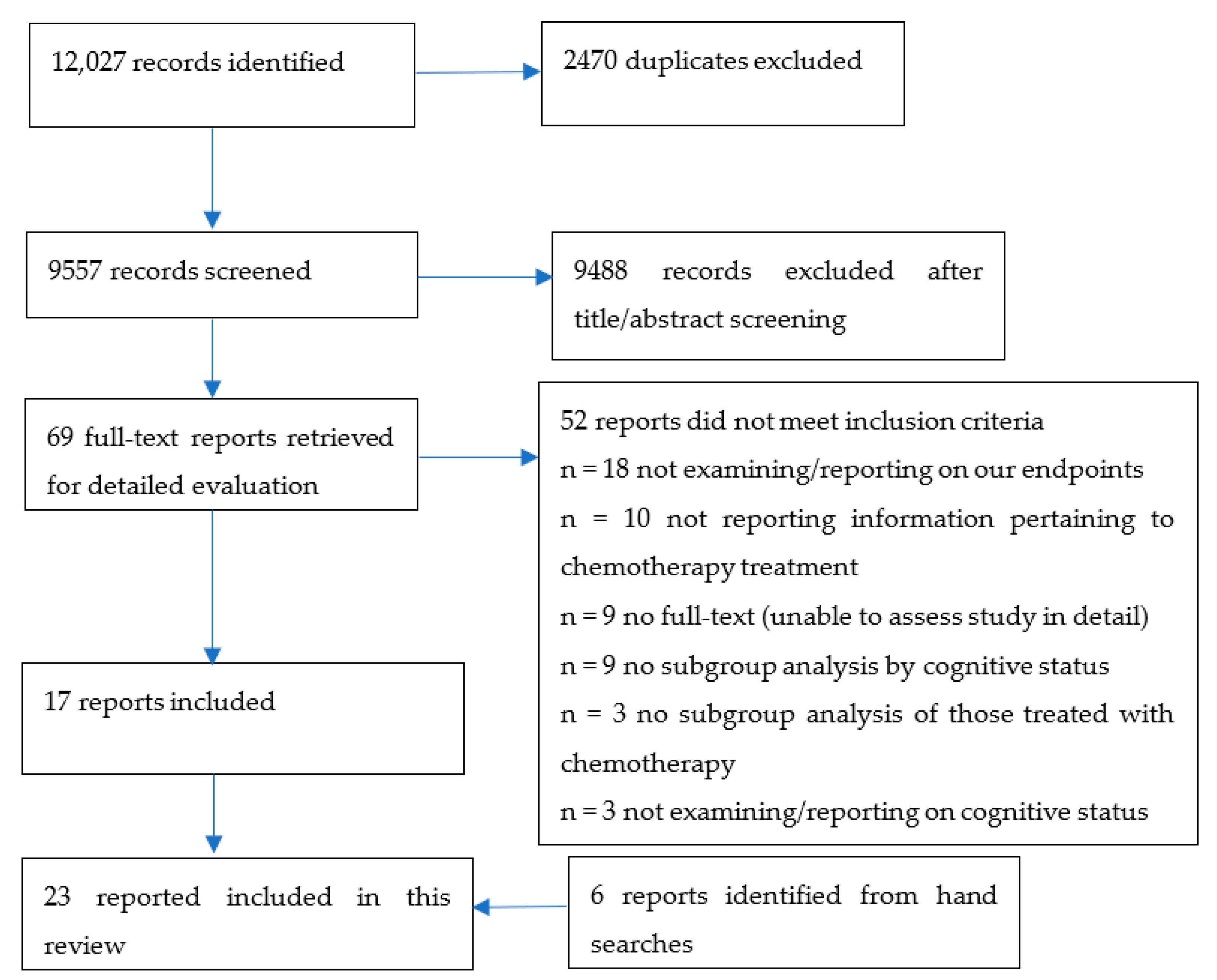
3.1. Study Selections
3.2. Study Characteristics
3.3. Risk of Bias in Studies
3.4. Survival/Mortality
3.5. Chemotherapy Completion
3.6. Chemotherapy Toxicity
4. Discussion
Strength and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Snaedal, J. Does my older cancer patient have cognitive impairment? J. Geriatr. Oncol. 2018, 9, 183–185. [Google Scholar] [CrossRef]
- Wefel, J.S.; Kesler, S.R.; Noll, K.R.; Schagen, S.B. Clinical characteristics, pathophysiology, and management of noncentral nervous system cancer-related cognitive impairment in adults. CA Cancer J. Clin. 2015, 65, 123–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hshieh, T.T.; Jung, W.F.; Grande, L.J.; Chen, J.; Stone, R.M.; Soiffer, R.J.; Driver, J.A.; Abel, G.A. Prevalence of cognitive impairment and association with survival among older patients with hematologic cancers. JAMA Oncol. 2018, 4, 686–693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joly, F.; Lange, M.; Dos Santos, M.; Vaz-Luis, I.; Di Meglio, A. Long-term fatigue and cognitive disorders in breast cancer survivors. Cancers 2019, 11, 1896. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Howlader, N.; Noone, A.M.; Krapcho, M.E.; Miller, D.; Brest, A.; Yu, M.; Ruhl, J.; Tatalovich, Z.; Mariotto, A.; Lewis, D.R. SEER Cancer Statistics Review, 1975–2016; National Cancer Institute: Bethesda, MD, USA, 2019; pp. 1423–1437. [Google Scholar]
- Corre, R.; Greillier, L.; Le Caër, H.; Audigier-Valette, C.; Baize, N.; Bérard, H.; Falchero, L.; Monnet, I.; Dansin, E.; Vergnenègre, A. Use of a comprehensive geriatric assessment for the management of elderly patients with advanced non–small-cell lung cancer: The phase III randomized ESOGIA-GFPC-GECP 08-02 study. J. Clin. Oncol. 2016, 34, 1476–1483. [Google Scholar] [CrossRef]
- Klepin, H.D.; Geiger, A.M.; Tooze, J.A.; Kritchevsky, S.B.; Williamson, J.D.; Ellis, L.R.; Levitan, D.; Pardee, T.S.; Isom, S.; Powell, B.L. The feasibility of inpatient geriatric assessment for older adults receiving induction chemotherapy for acute myelogenous leukemia. J. Am. Geriatr. Soc. 2011, 59, 1837–1846. [Google Scholar] [CrossRef]
- Loh, K.P.; Pandya, C.; Zittel, J.; Kadambi, S.; Flannery, M.; Reizine, N.; Magnuson, A.; Braganza, G.; Mustian, K.; Dale, W. Associations of sleep disturbance with physical function and cognition in older adults with cancer. Support. Care Cancer 2017, 25, 3161–3169. [Google Scholar] [CrossRef]
- Magnuson, A.; Mohile, S.; Janelsins, M. Cognition and cognitive impairment in older adults with cancer. Curr. Geriatr. Rep. 2016, 5, 213–219. [Google Scholar] [CrossRef] [Green Version]
- Dos Santos, M.; Licaj, I.; Bellera, C.; Cany, L.; Binarelli, G.; Soubeyran, P.; Joly, F. Cognitive Impairment in Older Cancer Patients Treated with First-Line Chemotherapy. Cancers 2021, 13, 6171. [Google Scholar] [CrossRef]
- Karuturi, M.; Wong, M.L.; Hsu, T.; Kimmick, G.G.; Lichtman, S.M.; Holmes, H.M.; Inouye, S.K.; Dale, W.; Loh, K.P.; Whitehead, M.I. Understanding cognition in older patients with cancer. J. Geriatr. Oncol. 2016, 7, 258–269. [Google Scholar] [CrossRef] [Green Version]
- Jayani, R.V.; Magnuson, A.M.; Sun, C.-L.; Ma, H.; Tew, W.P.; Mohile, S.G.; Gajra, A.; Klepin, H.D.; Gross, C.P.; Muss, H.B. Association between a cognitive screening test and severe chemotherapy toxicity in older adults with cancer. J. Geriatr. Oncol. 2020, 11, 284–289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farias, S.T.; Mungas, D.; Reed, B.R.; Harvey, D.; DeCarli, C. Progression of mild cognitive impairment to dementia in clinic-vs community-based cohorts. Arch. Neurol. 2009, 66, 1151–1157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hurria, A.; Rosen, C.; Hudis, C.; Zuckerman, E.; Panageas, K.S.; Lachs, M.S.; Witmer, M.; Van Gorp, W.G.; Fornier, M.; D’Andrea, G. Cognitive function of older patients receiving adjuvant chemotherapy for breast cancer: A pilot prospective longitudinal study. J. Am. Geriatr. Soc. 2006, 54, 925–931. [Google Scholar] [CrossRef] [PubMed]
- Ahles, T.A.; Saykin, A.J.; McDonald, B.C.; Li, Y.; Furstenberg, C.T.; Hanscom, B.S.; Mulrooney, T.J.; Schwartz, G.N.; Kaufman, P.A. Longitudinal assessment of cognitive changes associated with adjuvant treatment for breast cancer: Impact of age and cognitive reserve. J. Clin. Oncol. 2010, 28, 4434. [Google Scholar] [CrossRef] [Green Version]
- Clough-Gorr, K.M.; Stuck, A.E.; Thwin, S.S.; Silliman, R.A. Older breast cancer survivors: Geriatric assessment domains are associated with poor tolerance of treatment adverse effects and predict mortality over 7 years of follow-up. J. Clin. Oncol. 2010, 28, 380. [Google Scholar] [CrossRef]
- Kristjansson, S.R.; Nesbakken, A.; Jordhøy, M.S.; Skovlund, E.; Audisio, R.A.; Johannessen, H.-O.; Bakka, A.; Wyller, T.B. Comprehensive geriatric assessment can predict complications in elderly patients after elective surgery for colorectal cancer: A prospective observational cohort study. Crit. Rev. Oncol. Hematol. 2010, 76, 208–217. [Google Scholar] [CrossRef] [Green Version]
- Hamaker, M.E.; Vos, A.G.; Smorenburg, C.H.; De Rooij, S.E.; Van Munster, B.C. The value of geriatric assessments in predicting treatment tolerance and all-cause mortality in older patients with cancer. Oncologist 2012, 17, 1439. [Google Scholar] [CrossRef] [Green Version]
- Sourdet, S.; Brechemier, D.; Steinmeyer, Z.; Gerard, S.; Balardy, L. Impact of the comprehensive geriatric assessment on treatment decision in geriatric oncology. BMC Cancer 2020, 20, 384. [Google Scholar] [CrossRef]
- Smith, B.D.; Smith, G.L.; Hurria, A.; Hortobagyi, G.N. Future of Cancer Incidence in the United States: Burdens Upon an Aging, Changing Nation. J. Clin. Oncol. 2009, 27, 2758. [Google Scholar] [CrossRef]
- Van Abbema, D.L.; van den Akker, M.; Janssen-Heijnen, M.L.; van den Berkmortel, F.; Hoeben, A.; de Vos-Geelen, J.; Buntinx, F.; Kleijnen, J.; Tjan-Heijnen, V.C. Patient-and tumor-related predictors of chemotherapy intolerance in older patients with cancer: A systematic review. J. Geriatr. Oncol. 2019, 10, 31–41. [Google Scholar] [CrossRef] [Green Version]
- Hayden, J.A.; van der Windt, D.A.; Cartwright, J.L.; Côté, P.; Bombardier, C. Assessing bias in studies of prognostic factors. Ann. Intern. Med. 2013, 158, 280–286. [Google Scholar] [CrossRef]
- Hayden, J.A.; Côté, P.; Bombardier, C. Evaluation of the quality of prognosis studies in systematic reviews. Ann. Intern. Med. 2006, 144, 427–437. [Google Scholar] [CrossRef] [PubMed]
- Abe, S.; Kanaya, K.; Kikukawa, M.; Sakai, M.; Akai, T.; Takata, Y.; Sakurai, H.; Shin, K.; Mori, M.; Iwamoto, T. Clinical results and issues of acute myeloid leukemia in elderly patients aged 75 years and older. Geriatr. Gerontol. Int. 2011, 11, 290–296. [Google Scholar] [CrossRef] [PubMed]
- Aaldriks, A.A.; Maartense, E.; Le Cessie, S.; Giltay, E.J.; Verlaan, H.; Van der Geest, L.G.M.; Kloosterman-Boele, W.M.; Peters-Dijkshoorn, M.T.; Blansjaar, B.A.; Van Schaick, H.W. Predictive value of geriatric assessment for patients older than 70 years, treated with chemotherapy. Crit. Rev. Oncol. Hematol. 2011, 79, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Aaldriks, A.A.; van der Geest, L.G.; Giltay, E.J.; le Cessie, S.; Portielje, J.E.; Tanis, B.C.; Nortier, J.W.; Maartense, E. Frailty and malnutrition predictive of mortality risk in older patients with advanced colorectal cancer receiving chemotherapy. J. Geriatr. Oncol. 2013, 4, 218–226. [Google Scholar] [CrossRef] [PubMed]
- Aaldriks, A.A.; Giltay, E.J.; Le Cessie, S.; van der Geest, L.G.M.; Portielje, J.E.A.; Tanis, B.C.; Nortier, J.W.R.; Maartense, E. Prognostic value of geriatric assessment in older patients with advanced breast cancer receiving chemotherapy. Breast 2013, 22, 753–760. [Google Scholar] [CrossRef] [PubMed]
- Aaldriks, A.A.; Maartense, E.D.; Nortier, H.J.; van der Geest, L.G.; le Cessie, S.; Tanis, B.C.; Portielje, J.E.; Ypma, P.; Giltay, E.J. Prognostic factors for the feasibility of chemotherapy and the Geriatric Prognostic Index (GPI) as risk profile for mortality before chemotherapy in the elderly. Acta Oncol. 2016, 55, 15–23. [Google Scholar] [CrossRef] [Green Version]
- Aparicio, T.; Jouve, J.-L.; Teillet, L.; Gargot, D.; Subtil, F.; Le Brun-Ly, V.; Cretin, J.; Locher, C.; Bouché, O.; Breysacher, G. Geriatric factors predict chemotherapy feasibility: Ancillary results of FFCD 2001-02 phase III study in first-line chemotherapy for metastatic colorectal cancer in elderly patients. J. Clin. Oncol. 2013, 31, 1464–1470. [Google Scholar] [CrossRef]
- Biesma, B.; Wymenga, A.N.M.; Vincent, A.; Dalesio, O.; Smit, H.J.M.; Stigt, J.A.; Smit, E.F.; van Felius, C.L.; van Putten, J.W.G.; Slaets, J.P.J. Quality of life, geriatric assessment and survival in elderly patients with non-small-cell lung cancer treated with carboplatin–gemcitabine or carboplatin–paclitaxel: NVALT-3 a phase III study. Ann. Oncol. 2011, 22, 1520–1527. [Google Scholar] [CrossRef]
- Dubruille, S.; Libert, Y.; Roos, M.; Vandenbossche, S.; Collard, A.; Meuleman, N.; Maerevoet, M.; Etienne, A.-M.; Reynaert, C.; Razavi, D. Identification of clinical parameters predictive of one-year survival using two geriatric tools in clinically fit older patients with hematological malignancies: Major impact of cognition. J. Geriatr. Oncol. 2015, 6, 362–369. [Google Scholar] [CrossRef]
- Extermann, M.; Boler, I.; Reich, R.R.; Lyman, G.H. Predicting the risk of chemotherapy toxicity in older patients: The Chemotherapy Risk Assessment Scale for High-Age Patients (CRASH) score. Cancer 2012, 118, 3377. [Google Scholar] [CrossRef] [PubMed]
- Falandry, C.; Weber, B.; Savoye, A.-M.; Tinquaut, F.; Tredan, O.; Sevin, E.; Stefani, L.; Savinelli, F.; Atlassi, M.; Salvat, J. Development of a geriatric vulnerability score in elderly patients with advanced ovarian cancer treated with first-line carboplatin: A GINECO prospective trial. Ann. Oncol. 2013, 24, 2808–2813. [Google Scholar] [CrossRef] [PubMed]
- Falandry, C.; Brain, E.; Bonnefoy, M.; Mefti, F.; Jovenin, N.; Rigal, O.; Guillem, O.; El Kouri, C.; Uwer, L.; Abadie-Lacourtoisie, S. Impact of geriatric risk factors on pegylated liposomal doxorubicin tolerance and efficacy in elderly metastatic breast cancer patients: Final results of the DOGMES multicentre GINECO trial. Eur. J. Cancer 2013, 49, 2806–2814. [Google Scholar] [CrossRef]
- Hamaker, M.E.; Seynaeve, C.; Wymenga, A.N.M.; van Tinteren, H.; Nortier, J.W.; Maartense, E.; de Graaf, H.; de Jongh, F.E.; Braun, J.J.; Los, M. Baseline comprehensive geriatric assessment is associated with toxicity and survival in elderly metastatic breast cancer patients receiving single-agent chemotherapy: Results from the OMEGA study of the Dutch breast cancer trialists’ group. Breast 2014, 23, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Klepin, H.D.; Geiger, A.M.; Tooze, J.A.; Kritchevsky, S.B.; Williamson, J.D.; Pardee, T.S.; Ellis, L.R.; Powell, B.L. Geriatric assessment predicts survival for older adults receiving induction chemotherapy for acute myelogenous leukemia. Blood J. Am. Soc. Hematol. 2013, 121, 4287–4294. [Google Scholar] [CrossRef] [PubMed]
- Laurent, M.; Paillaud, E.; Tournigand, C.; Caillet, P.; Le Thuaut, A.; Lagrange, J.-L.; Beauchet, O.; Vincent, H.; Carvahlo-Verlinde, M.; Culine, S. Assessment of solid cancer treatment feasibility in older patients: A prospective cohort study. Oncol. 2014, 19, 275. [Google Scholar] [CrossRef] [Green Version]
- Molga, A.; Wall, M.; Chhetri, R.; Wee, L.Y.; Singhal, D.; Edwards, S.; Singhal, N.; Ross, D.; To, L.B.; Caughey, G. Comprehensive geriatric assessment predicts azacitidine treatment duration and survival in older patients with myelodysplastic syndromes. J. Geriatr. Oncol. 2020, 11, 114–120. [Google Scholar] [CrossRef] [Green Version]
- Robb, C.; Boulware, D.; Overcash, J.; Extermann, M. Patterns of care and survival in cancer patients with cognitive impairment. Crit. Rev. Oncol. Hematol. 2010, 74, 218–224. [Google Scholar] [CrossRef]
- Shin, D.-Y.; Lee, J.-O.; Kim, Y.J.; Park, M.-S.; Lee, K.-W.; Kim, K.-I.; Bang, S.-M.; Lee, J.S.; Kim, C.-H.; Kim, J.H. Toxicities and functional consequences of systemic chemotherapy in elderly Korean patients with cancer: A prospective cohort study using comprehensive geriatric assessment. J. Geriatr. Oncol. 2012, 3, 359–367. [Google Scholar] [CrossRef]
- Soubeyran, P.; Fonck, M.; Blanc-Bisson, C.; Blanc, J.-F.; Ceccaldi, J.; Mertens, C.; Imbert, Y.; Cany, L.; Vogt, L.; Dauba, J. Predictors of early death risk in older patients treated with first-line chemotherapy for cancer. J. Clin. Oncol. 2012, 30, 1829–1834. [Google Scholar] [CrossRef]
- Thibaud, V.; Denève, L.; Dubruille, S.; Kenis, C.; Delforge, M.; Cattenoz, C.; Somme, D.; Wildiers, H.; Pepersack, T.; Lamy, T. Identifying frailty in clinically fit patients diagnosed with hematological malignancies using a simple clinico-biological screening tool: The HEMA-4 study. J. Geriatr. Oncol. 2021, 12, 902–908. [Google Scholar] [CrossRef] [PubMed]
- Wildes, T.M.; Ruwe, A.P.; Fournier, C.; Gao, F.; Carson, K.R.; Piccirillo, J.F.; Tan, B.; Colditz, G.A. Geriatric assessment is associated with completion of chemotherapy, toxicity, and survival in older adults with cancer. J. Geriatr. Oncol. 2013, 4, 227–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.; Fujita, K.; Negoro, E.; Morishita, T.; Oiwa, K.; Tsukasaki, H.; Kinoshita, K.; Kawai, Y.; Ueda, T.; Yamauchi, T. Impact of relative dose intensity of standard regimens on survival in elderly patients aged 80 years and older with diffuse large B-cell lymphoma. Haematologica 2020, 105, e415. [Google Scholar] [CrossRef] [PubMed]
- Hurria, A.; Togawa, K.; Mohile, S.G.; Owusu, C.; Klepin, H.D.; Gross, C.P.; Lichtman, S.M.; Gajra, A.; Bhatia, S.; Katheria, V. Predicting chemotherapy toxicity in older adults with cancer: A prospective multicenter study. J. Clin. Oncol. 2011, 29, 3457. [Google Scholar] [CrossRef] [Green Version]
- Hurria, A.; Mohile, S.; Gajra, A.; Klepin, H.; Muss, H.; Chapman, A.; Feng, T.; Smith, D.; Sun, C.-L.; De Glas, N. Validation of a prediction tool for chemotherapy toxicity in older adults with cancer. J. Clin. Oncol. 2016, 34, 2366. [Google Scholar] [CrossRef]
- Van Deudekom, F.J.; Klop, H.G.; Hartgrink, H.H.; Boonstra, J.J.; Lips, I.M.; Slingerland, M.; Mooijaart, S.P. Functional and cognitive impairment, social functioning, frailty and adverse health outcomes in older patients with esophageal cancer, a systematic review. J. Geriatr. Oncol. 2018, 9, 560–568. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Author/Year | Country | Study Type | Sample Size | Sampling Method | Cancer Site(s) | Cancer Stage/Type | Age | % Women | Educaton | Endpoint Outcomes Examined * | How CI Ascertained at Baseline |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Abe (2011) | Japan | Retrospective cohort | N = 31; of whom n = 7 (22.6%) had mild/moderate CI Total 7/31 had CI (22.6%) N = 4 Mild (MMSE: 20–23) N = 3 Moderate (MMSE: 14–19) | NR | Hematological (all patients had AML) | M0-M6 (French-American-British classification) | Median 79 (total sample) | 35.5% (total sample) | NR | chemotherapy discontinuation | MMSE (no cut off given) performed on patients with suspected clinically depressed cognitive function. |
| Aldricks (2011) | The Netherlands | Prospective | 202 | Consecutive | Colorectal, Hematological, breast, ovarian, upper GI, other | various | Mean 77.2 (71–92) SD 4.22 | 55% | NR | Chemotherapy completion Mortality | MMSE <= 24 IQCODE >= 3.3 |
| Aaldriks (2013) | The Netherlands | Prospective cohort | 143 13% positive for CI ((IQCODE >= 3.3) 8% positive for CI (MMSE <= 24) | NR | colorectal | II–IV | 75 (range 70–92) | 41% | NR | Mortality | MMSE ≤ 24 IQCODE > 3.31 |
| Aaldriks (2013) | The Netherlands | Prospective cohort | 55 (n = 10 [41%] positive for CI [IQCODE]) (n = 5 [13%] positive for CI [MMSE]) | Consecutive | Breast | IV | 76 (SD 4.8), range 70–88 | 96% | NR | Mortality | MMSE ≤ 24 IQCODE ≥ 3.3 |
| Aaldriks (2016) | The Netherlands | Prospective | N = 494 | Consecutive | Upper GI, Lower GI, Hematological, Breast, Gynecological, prostate, lung, urinary tract, other | I–IV | Median 75 (70–92) | 50.1 | NR | Chemotherapy completion (labelled as ‘feasibility’ in study) Survival | |
| Aparicio (2013) | France | RCT | N = 282 randomized Geriatric score for N = 123 were calculate Of whom, (n = 38 [31%] positive for CI [MMSE]) | NR | Colorectal | IV | Mean 80.4 (SD 3.7) | 46% | NR | Chemotherapy toxicity | MMSE ≤ 27 |
| Biesma (2011) | The Netherlands | RCT | N = 181 | NR | Lung | III–IV | Median 74 (70–87) | 23% | NR | Chemotherapy toxicity | MMSE (cutoff not reported) |
| Dubruille (2015) | Belgium | Prospective longitudinal | N = 90 | Consecutive | Hematological | NR | Median 74 (65–89) | 43% | NR | One-year survival | MMSE < 27 MoCA < 26 |
| Extermann (2012) | US | Prospective multicenter | N = 518 | Consecutive | various | I–IV Lung, breast, NHL, colorectal, bladder, other | Mean 75.5 (70–92) | 50.4% | NR | Hematologic Toxicity, non-hematologic toxicity | MMSE (cutoff not reported) |
| Falandry (2013) | France | RCT | N = 111 (29% had MMS score <25) | Consecutive | Ovarian | II–IV | Median 79 (71–93) | 100% | NR | Overall survival | MMSE < 25 |
| Falandry (2013) | France | RCT | N = 60 | N/A | Breast | IV | Median 77 (71–89) | 100% | NR | PFS, overall survival, chemo toxicity | 5 word recall |
| Hamaker (2013) | The Netherlands | RCT | N = 73 | N/A | Breast | IV | Median 75.5 (65.8–86.8) | 100% | NR | Chemotherapy toxicity Survival | MMSE ≤ 23 |
| Hshieh (2018) | US | Prospective observational cohort | 360 341 (94.7%) completed both cognitive screening tests 127 (35.3%) had probable executive dysfunction on the CIB; 62 (17.2%) had probably impairment in working memory (5 word delayed recall) | Consecutive | Hematological | Aggressive; indolent | Mean 79.8 (SD 3.9) | 35.6% | NR | Survival | Clock-in-the-Box (executive function) 7 to 8 as normal 5-word Delayed Recall (working memory) 3 of 5 words possible CI |
| Jayani (2019) | US | Secondary analysis of a prospective cohort study | N = 703; of whom, n = 250 (36%) had CI | Consecutive | Breast, GI, GU, gynecological, lung, other | I–IV Stage III or IV cancer (81.1%) | Mean 73 (65–94) | 32.7% (out of the n = 250 group with CI) | College or higher education (63%) | Chemotherapy toxicity | Blessed Orientation-Memory-Concentration test (BOMC 5–10 as potential CI) |
| Klepin (2013) | US | Prospective cohort study | N = 74, 28.8% had CI | Consecutive | hematological | Cytogenic risk group: Poor: 31.5% Favorable/intermediate: 68.5% | Mean 70 (SD 6.2) | 46% | < high school: 25.0% High school: 23.6% College/above: 51.4% | Overall survival | 100-point Modified Mini-mental State Exam (3MS) (<77 = impairment) |
| Laurent (2014) | France | Prospective | N = 385 | Consecutive | Colorectal, breast, upper GI + liver, urinary tract, prostate, other | Stage IV 47% | Mean 78.9 (+/−5.4) | 52.2% | NR | Chemo discontinuation | MMSE < 24 |
| Lee (2020) | Japan | Retrospective | N = 127 | NR | All patients had diffuse large B-cell lymphoma | Ann Arbor Stage III/IV: 78.7% | Median 83.7 (80–96) | 52.8% | NR | Survival | NR |
| Molga (2019) | Australia | Prospective | N = 98 (n = 11 screened positive for CI at baseline) | NR | Hematological | IPSS (international prognostic scoring system) very low to very high | 77 (66–95) | 36% | NR | Chemotherapy completion Overall survival | MMSE < 24 |
| Robb (2009) | US | Retrospective case-control | CI: n = 86 Non-CI: n = 172 | N/A | Breast, colorectal, prostate, gastric, pancreatic, lung, other | 0-IV Stage IV 33.7% | CI: mean 79.1 (SD 5.47); non-CI: mean 75.4 (SD 4.63) | Case n= 54. Control n= 135 | NR | Survival | MMSE ≤ 24 |
| Shin (2012) | Korea | Prospective | 64 | NR | GI, lung, gynecological, other | I–IV Stage IV 50.0% | Median 71 (65–80) | 25% | NR | Chemotherapy toxicity | MMSE-KC (Korean version) <=24 Mild cognitive decline <16 cognitive impairment |
| Soubeyran (2012) | France | Prospective | 348 | Consecutive | Non-Hodgkin’s lymphoma, GI, lung, ovarian, bladder, prostate, pancreas | Majority were stage IV (65%) | Median 77.5 (70–99.4) | 40.5% | NR | Mortality (early death risk) | MMSE ≤ 23 |
| Thibaud (2021) | Belgium | Prospective | N = 206 31% had MMSE < 27 | NR | Hematological | Based on HEMA-4 score Good prognosis-Poor prognosis | Mean age 76 (65–90) | 46% | NR | Survival | MMSE < 27 |
| Wildes (2013) | US | Prospective | N = 65 | Convenience | Lung, Breast, Lymphoma, colorectal | NR | Median 73 (65–89) | 58.5% | NR | Chemo completion Non-hematologic toxicity Mortality | Short blessed > 9 |
| Category | Number of Studies * Investigating CI ^ in Multivariable Model | Number of Studies * Reporting Statistically Significant Influence of CI on Outcome |
|---|---|---|
| Survival/mortality | 6 | 4 a |
| Chemotherapy completion | 1 | 0 b |
| Chemotherapy toxicity | 1 | 1 c |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sattar, S.; Haase, K.; Tejero, I.; Bradley, C.; Mariano, C.; Kilgour, H.; Verma, R.; Amir, E.; Alibhai, S. The Impact of Cognitive Impairment on Treatment Toxicity, Treatment Completion, and Survival among Older Adults Receiving Chemotherapy: A Systematic Review. Cancers 2022, 14, 1582. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14061582
Sattar S, Haase K, Tejero I, Bradley C, Mariano C, Kilgour H, Verma R, Amir E, Alibhai S. The Impact of Cognitive Impairment on Treatment Toxicity, Treatment Completion, and Survival among Older Adults Receiving Chemotherapy: A Systematic Review. Cancers. 2022; 14(6):1582. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14061582
Chicago/Turabian StyleSattar, Schroder, Kristen Haase, Isabel Tejero, Cara Bradley, Caroline Mariano, Heather Kilgour, Ridhi Verma, Eitan Amir, and Shabbir Alibhai. 2022. "The Impact of Cognitive Impairment on Treatment Toxicity, Treatment Completion, and Survival among Older Adults Receiving Chemotherapy: A Systematic Review" Cancers 14, no. 6: 1582. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14061582