
The Barcelona Predictive Model of Clinically Significant Prostate Cancer

 , , , , , ,
, , , , , ,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
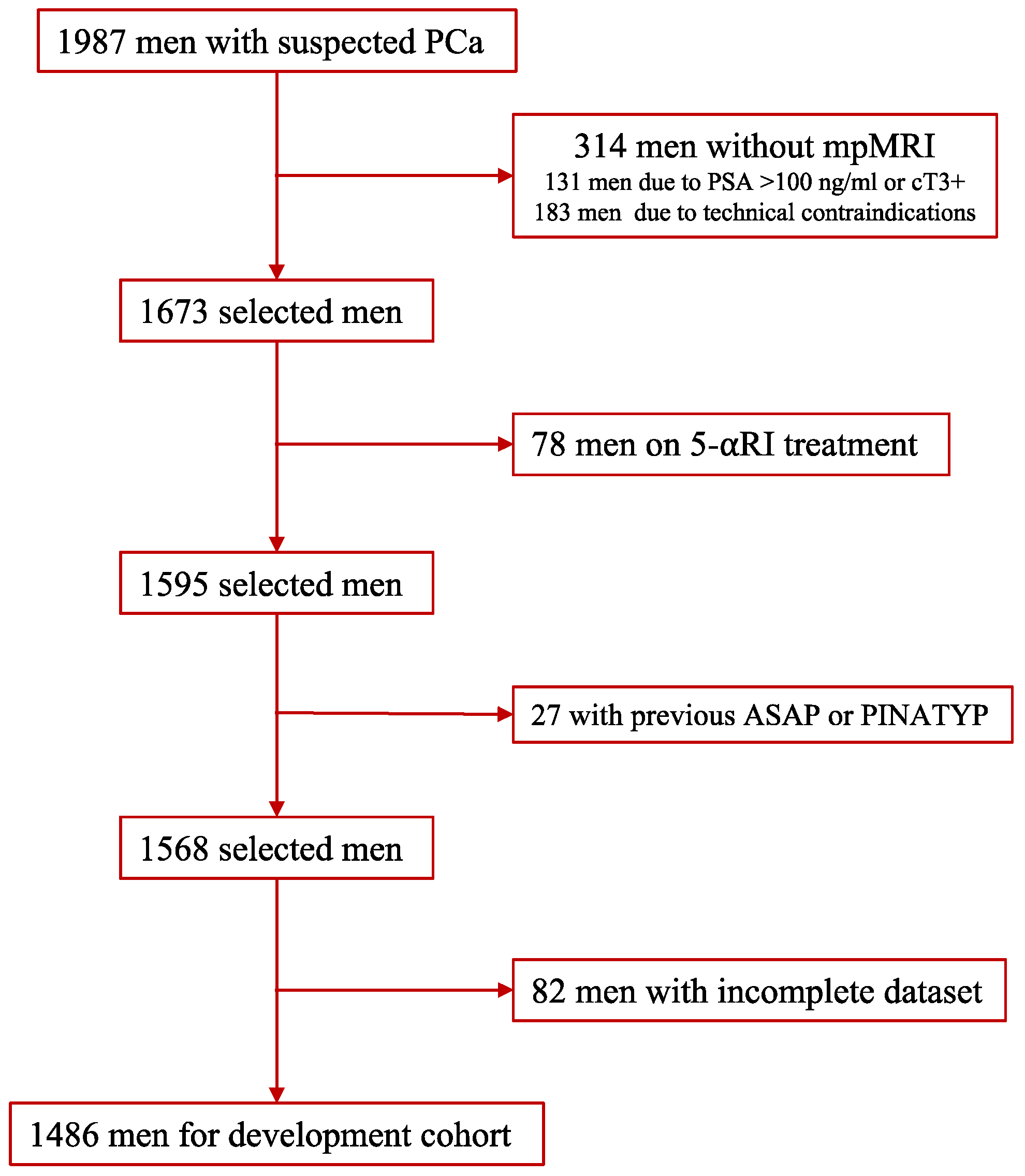
2.1. Development Cohort
2.2. External Validation Cohort
2.3. MRI Technique and Evaluation
2.4. Prostate Biopsy Procedure
2.5. Pathologic Analysis and csPCa Definition
2.6. Development of MRI-PM
2.7. Endpoint Measurements for the Performance Analysis of MRIPM
2.8. Statistical Analysis
3. Results
3.1. Characteristics of Development and External Validation Cohorts
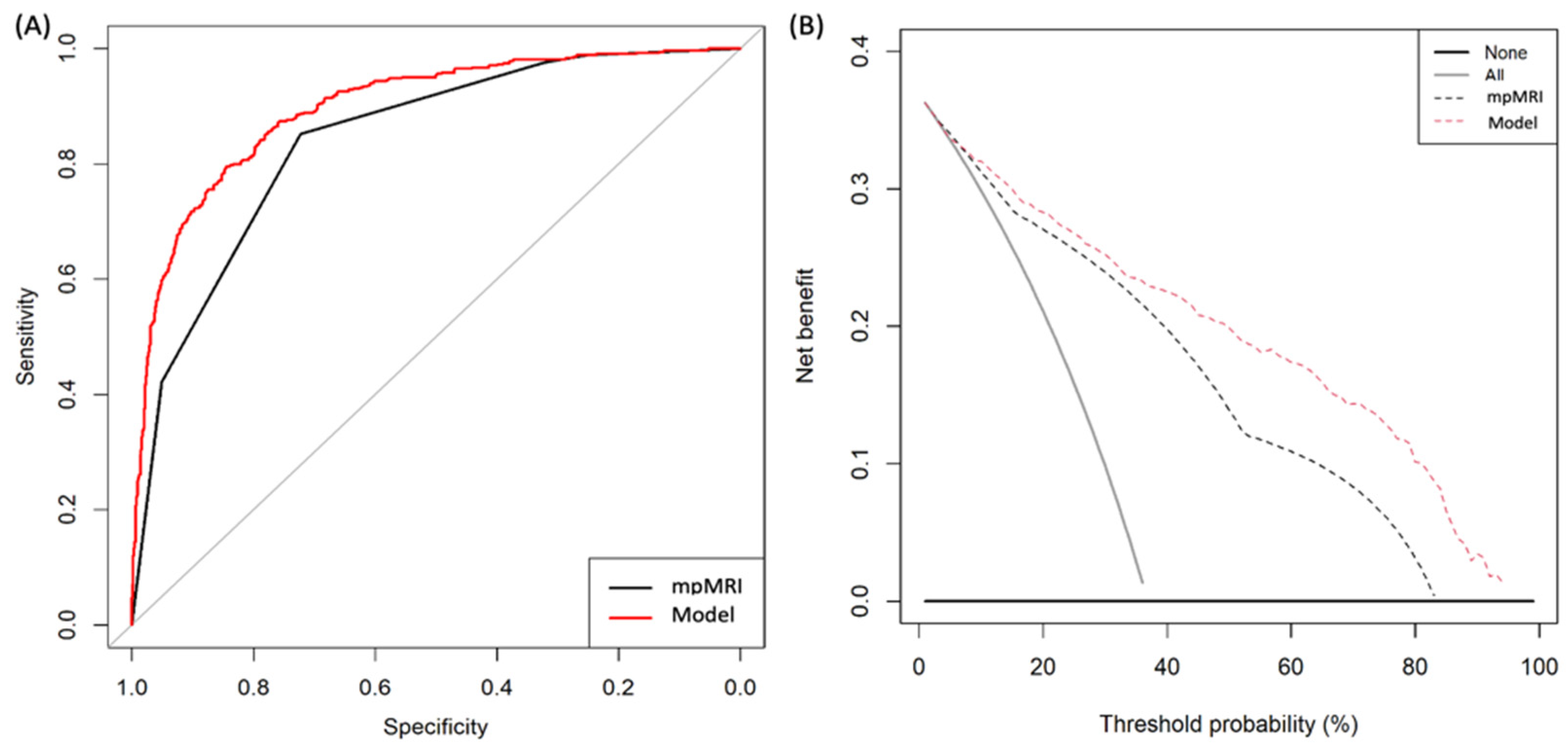
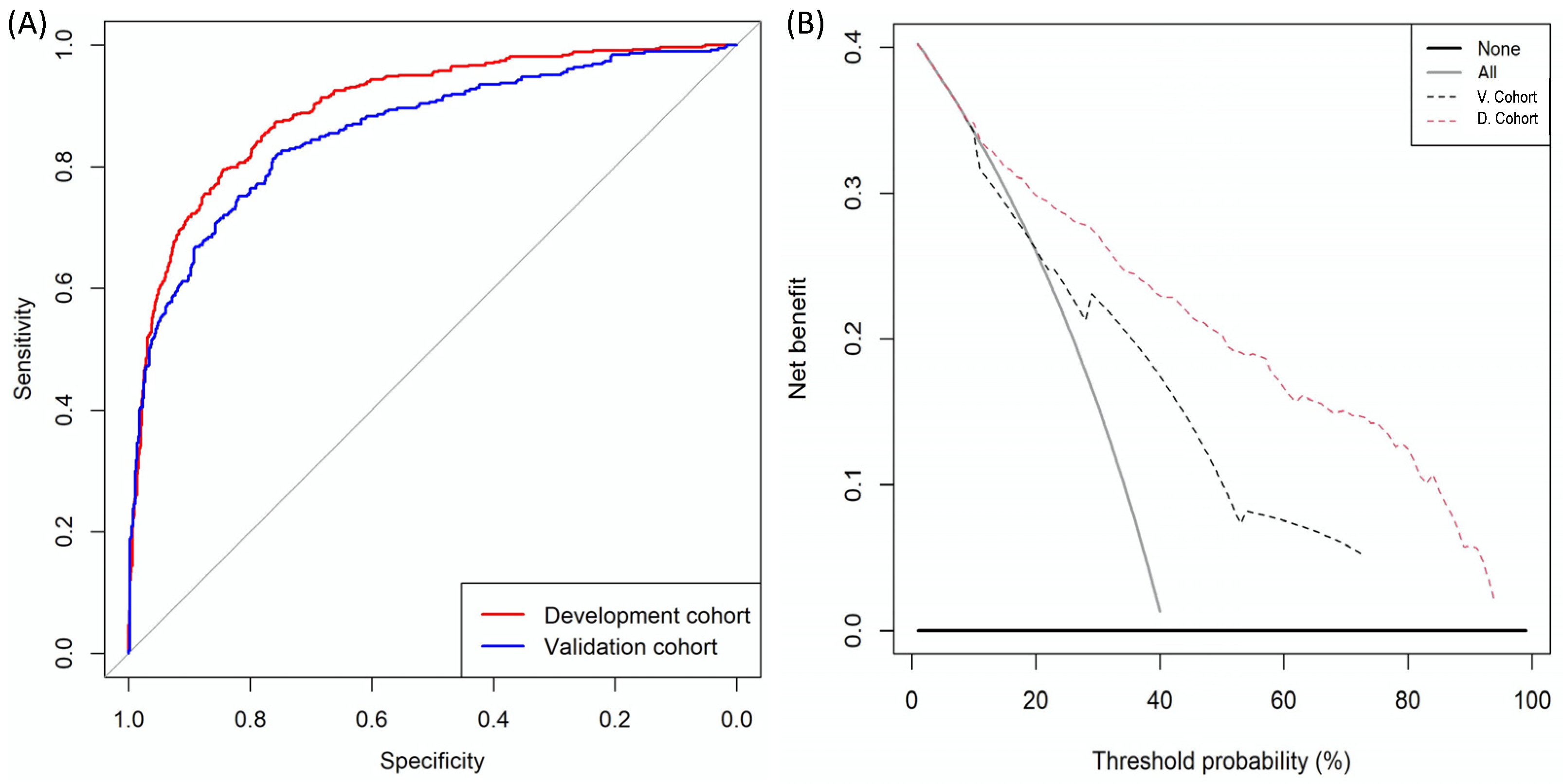
3.2. MRI-Based Predictive Model Development and Performance
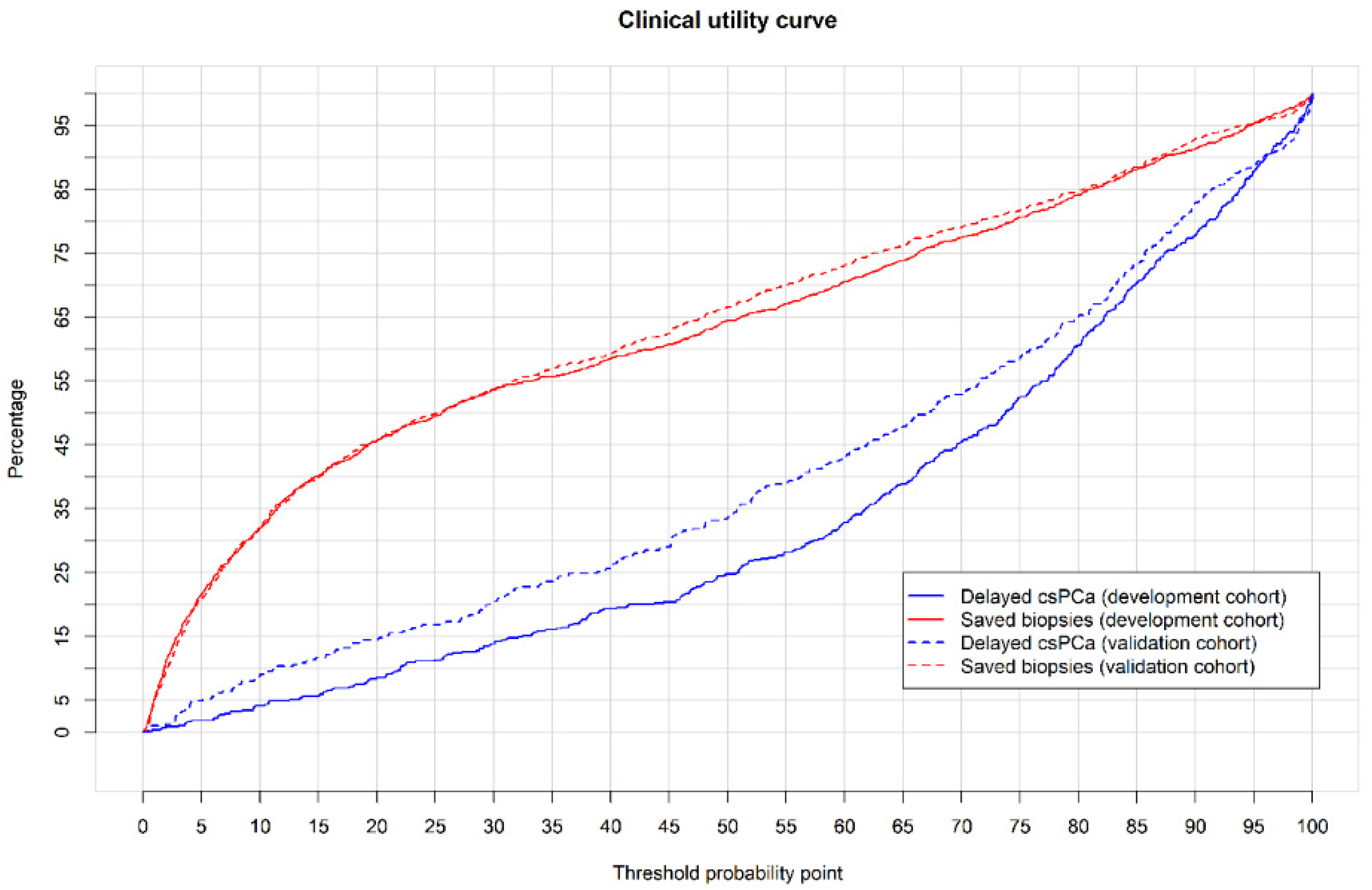
3.3. External Validation of MRI-PM and Its Performance
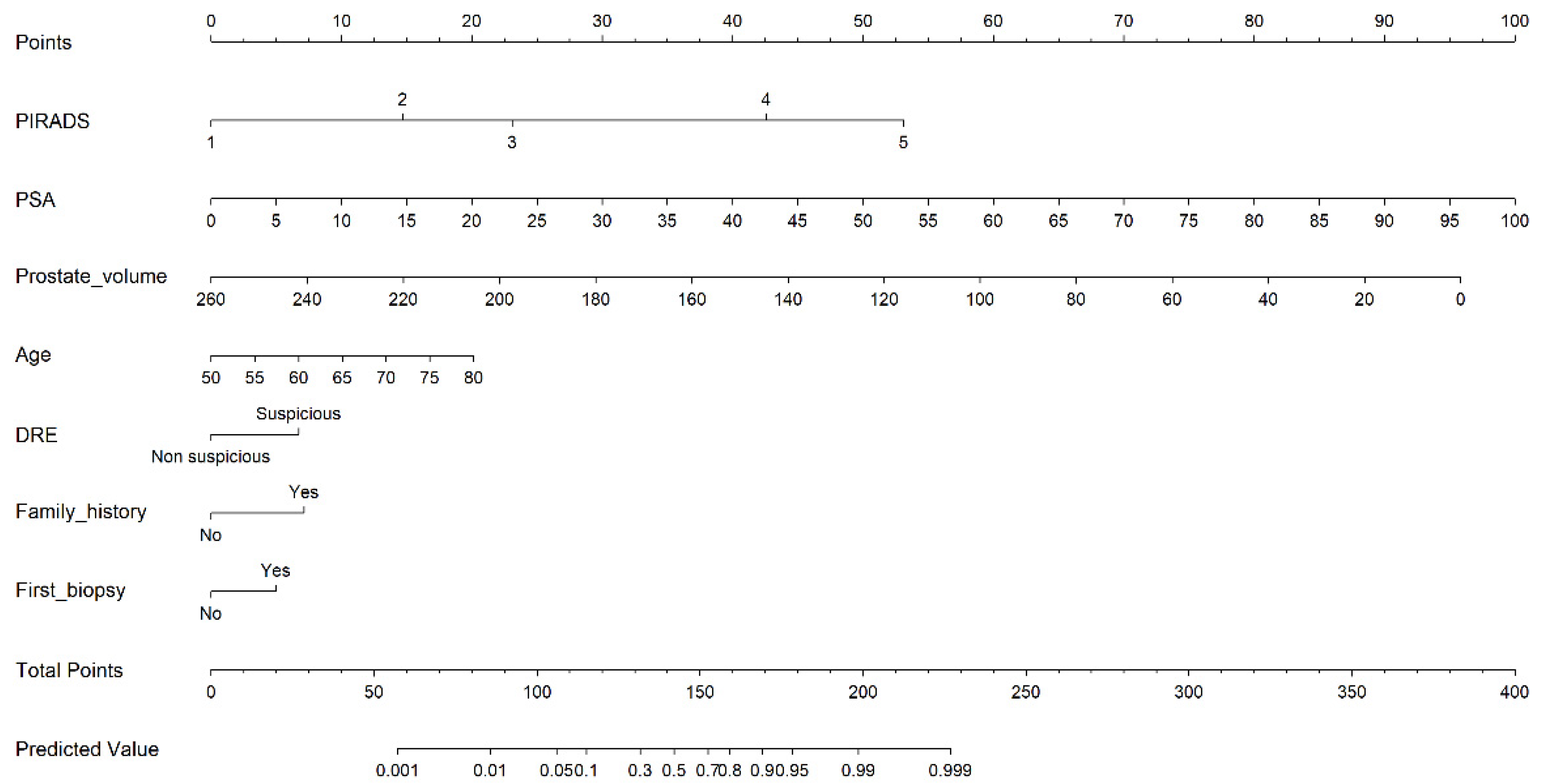
3.4. Web-RC Design
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mottet, N.; van den Bergh, R.C.N.; Briesrs, E.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer-2020 Update. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2021, 79, 243–262. [Google Scholar] [CrossRef] [PubMed]
- Drazer, M.W.; Huo, D.; Eggener, S.E. National Prostate Cancer Screening Rates After the 2012 US Preventive Services Task Force Recommendation Discouraging Prostate-Specific Antigen-Based Screening. J. Clin. Oncol. 2015, 33, 2416–2423. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, H.U.; El-Shater Bosaily, A.; Brown, L.C.; Gabe, R.; Kaplan, R.; Parmar, M.K.; Collaco-Moraes, Y.; Ward, K.; Hindley, R.G.; Freeman, A.; et al. Diagnostic accuracy of multi-parametric MRI and TRUSbiopsy in prostate cancer (PROMIS): A paired validating confirmatory study. Lancet 2017, 389, 815–822. [Google Scholar] [CrossRef] [Green Version]
- Schoots, I.G.; Padhani, A.R.; Rouvière, O.; Barentsz, J.O.; Richenberg, J. Analysis of Magnetic Resonance Imaging-directed Biopsy Strategies for Changing the Paradigm of Prostate Cancer Diagnosis. Eur. Urol. Oncol. 2020, 3, 32–41. [Google Scholar] [CrossRef]
- Van Poppel, H.; Roobol, M.J.; Chapple, C.R.; Catto, J.W.F.; N’Dow, J.; Sønksen, J.; Stenzl, A.; Wirth, M. Prostate-specific Antigen Testing as Part of a Risk-Adapted Early Detection Strategy for Prostate Cancer: European Association of Urology Position and Recommendations for 2021. Eur. Urol. 2021, 80, 703–711. [Google Scholar] [CrossRef]
- Van Poppel, H.; Hogenhout, R.; Albers, P.; van den Bergh, R.C.N.; Barentsz, J.O.; Roobol, M.J. A European Model for an Organised Risk-stratified Early Detection Programme for Prostate Cancer. Eur. Urol. Oncol. 2021, 4, 731–739. [Google Scholar] [CrossRef]
- Morote, J.; Celma, A.; Diaz, F.; Regis, L.; Roche, S.; Mast, R.; Semidey, M.E.; de Torres, I.M.; Planas, J.; Trilla, E. Prostatic-specific antigen density behavior according to multiparametric magnetic resonance imaging result. Urol. Oncol. 2020, 38, 410–417. [Google Scholar] [CrossRef]
- Schoots, I.G.; Roobol, M.J. Multivariate risk prediction tools including MRI for individualized biopsy decision in prostate cancer diagnosis: Current status and future directions. World J. Urol. 2020, 38, 517–529. [Google Scholar] [CrossRef] [Green Version]
- Becerra, M.F.; Atluri, V.S.; Bhattu, A.S.; Punnen, S. Serum and urine biomarkers for detecting clinically significant prostate cancer. Urol. Oncol. 2021, 39, 686–690. [Google Scholar] [CrossRef]
- Dianat, S.S.; Rancier Ruiz, R.M.; Bonekamp, D.; Carter, H.B.; Macura, K.J. Prostate volumetric assessment by magnetic resonance imaging and transrectal ultrasound: Impact of variation in calculated prostate-specific antigen density on patient eligibility for active surveillance program. J. Comput. Assist. Tomogr. 2013, 37, 589–595. [Google Scholar] [CrossRef]
- Borque-Fernando, A.; Esteban, L.M.; Celma, A.; Regis, L.; de Torres, I.M.; Semidey, M.E.; Trilla, E.; Morote, J. How to implement magnetic resonance imaging before prostate biopsy in clinical practice: Nomograms for saving biopsies. World J. Urol. 2019, 38, 1481–1491. [Google Scholar] [CrossRef] [PubMed]
- Alberts, A.R.; Roobol, M.J.; Verbeek, J.F.M.; Schoots, I.G.; Chiu, P.K.; Osses, D.F.; Tijsterman, J.D.; Beerlage, H.P.; Mannaerts, C.K.; Schimmöller, L.; et al. Prediction of High-grade Prostate Cancer Following Multiparametric Magnetic Resonance Imaging: Improving the Rotterdam European Randomized Study of Screening for Prostate Cancer Risk Calculators. Eur. Urol. 2019, 75, 310–318. [Google Scholar] [CrossRef] [PubMed]
- Fang, D.; Zhao, C.; Ren, D.; Yu, W.; Wang, R.; Wang, H.; Li, X.; Yin, W.; Yu, X.; Yang, K.; et al. Could Magnetic Resonance Imaging Help to Identify the Presence of Prostate Cancer Before Initial Biopsy? The Development of Nomogram Predicting the Outcomes of Prostate Biopsy in the Chinese Population. Ann. Surg. Oncol. 2016, 23, 4284–4292. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.H.; Weaver, J.K.; Shetty, A.S.; Vetter, J.M.; Andriole, G.L.; Strope, S.A. Magnetic Resonance Imaging Provides Added Value to the Prostate Cancer Prevention Trial Risk Calculator for Patients With Estimated Risk of High-grade Prostate Cancer Less Than or Equal to 10. Urology 2017, 102, 183–189. [Google Scholar] [CrossRef]
- Radtke, J.P.; Wiesenfarth, M.; Kesch, C.; Freitag, M.T.; Alt, C.D.; Celik, K.; Distler, F.; Roth, W.; Wieczorek, K.; Stock, C.; et al. Combined Clinical Parameters and Multiparametric Magnetic Resonance Imaging for Advanced Risk Modeling of Prostate Cancer-Patient-tailored Risk Stratification Can Reduce Unnecessary Biopsies. Eur. Urol. 2017, 72, 888–896. [Google Scholar] [CrossRef]
- Bjurlin, M.A.; Rosenkrantz, A.B.; Sarkar, S.; Lepor, H.; Huang, W.C.; Huang, R.; Venkataraman, R.; Taneja, S. Prediction of Prostate Cancer Risk Among Men Undergoing Combined MRI-targeted and Systematic Biopsy Using Novel Pre-biopsy Nomograms That Incorporate MRI Findings. Urology 2018, 112, 112–120. [Google Scholar] [CrossRef]
- Lee, S.M.; Liyanage, S.H.; Wulaningsih, W.; Wolfe, K.; Carr, T.; Younis, C.; Van Hemelrijck, M.; Popert, R.; Acher, P. Toward an MRI-based nomogram for the prediction of transperineal prostate biopsy outcome: A physician and patient decision tool. Urol. Oncol. 2017, 35, 66411–66418. [Google Scholar] [CrossRef] [Green Version]
- Van Leeuwen, P.J.; Hayen, A.; Thompson, J.E.; James, E.; Moses, D.; Shnier, R.; Böhm, M.; Abuodha, M.; Haynes, A.M.; Ting, F.; et al. Multiparametric magnetic resonance imaging-based risk model to determine the risk of significant prostate cancer prior to biopsy. BJU Int. 2017, 120, 774–781. [Google Scholar] [CrossRef] [Green Version]
- Niu, X.K.; Li, J.; Das, S.K.; Yang, C.B.; Peng, T. Developing a nomogram based on multiparametric magnetic resonance imaging for forecasting high-grade prostate cancer to reduce unnecessary biopsies within the prostate-specific antigen gray zone. BMC Med. Imaging 2017, 17, 11. [Google Scholar] [CrossRef] [Green Version]
- Truong, M.; Wang, B.; Gordetsky, J.B.; Nix, J.W.; Frye, T.P.; Messing, E.M.; Thomas, J.V.; Feng, C.; Rais-Bahrami, S. Multi-institutional nomogram predicting benign prostate pathology on magnetic resonance/ultrasound fusion biopsy in men with a prior negative 12-core systematic biopsy. Cancer 2018, 124, 278–285. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.; Song, G.; Wang, H.; Li, J.; Chen, Y.; Fan, Y.; Fang, D.; Xiong, G.; Xin, Z.; Zhou, L. Multiparametric Magnetic Resonance Imaging-Based Nomogram for Predicting Prostate Cancer and Clinically Significant Prostate Cancer in Men Undergoing Repeat Prostate Biopsy. Biomed. Res. Int. 2018, 6368309. [Google Scholar] [CrossRef] [Green Version]
- Mehralivand, S.; Shih, J.H.; Rais-Bahrami, S.; Oto, A.; Bednarova, S.; Nix, J.W.; Thomas, J.V.; Gordetsky, J.B.; Gaur, S.; Harmon, S.A.; et al. A Magnetic Resonance Imaging-Based Prediction Model for Prosate Biopsy Risk Stratification. JAMA Oncol. 2018, 4, 678–685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boesen, L.; Thomsen, F.B.; Nørgaard, N.; Løgager, V.; Balslev, I.; Bisbjerg, R.; Thomsen, H.S.; Jakobsen, H. A predictive model based on biparametric magnetic resonance imaging and clinical parameters for improved risk assessment and selection of biopsy-naïve men for prostate biopsies. Prostate Cancer Prostatic Dis. 2019, 2, 311–319. [Google Scholar] [CrossRef] [PubMed]
- Noh, T.I.; Hyun, C.W.; Kang, H.E.; Jin, H.J.; Tae, J.H.; Shim, J.S.; Kang, S.G.; Sung, D.J.; Cheon, J.; Lee, J.G.; et al. A Predictive Model Based on Bi-parametric Magnetic Resonance Imaging and Clinical Parameters for Clinically Significant Prostate Cancer in the Korean Population. Cancer Res. Treat. 2021, 53, 1148–1155. [Google Scholar] [CrossRef]
- Chen, I.A.; Chu, C.H.; Lin, J.T.; Tsai, J.Y.; Yu, C.C.; Sridhar, A.N.; Sooriakumaran, P.; Loureiro, R.C.V.; Chand, M. Prostate Cancer Risk Calculator Apps in a Taiwanese Population Cohort: Validation Study. J. Med. Internet Res. 2020, 22, e16322. [Google Scholar] [CrossRef]
- Bossuyt, P.M.; Reitsma, J.B.; Bruns, D.E.; Korevaar, D.A.; STARD Group. STARD 2015: An updated list of essential items for reporting diagnostic accuracy studies. BMJ 2015, 351, h5527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weinreb, J.C.; Barentsz, J.O.; Choyke, P.L.; Choyke, P.L.; Cornud, F.; Haider, M.A.; Macura, K.J.; Margolis, D.; Schnall, M.D.; Shtern, F.; et al. PI-RADS Prostate Imaging—Reporting and Data System: 2015, Version 2. Eur. Urol. 2016, 69, 16–40. [Google Scholar] [CrossRef]
- Epstein, J.I.; Egevad, L.; Amin, M.B.; Delahunt, B.; Srigley, J.R.; Humphrey, P.A.; Grading Committee. The 2014 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma: Definition of Grading Patterns and Proposal for a New Grading System. Am. J. Surg. Pathol. 2016, 40, 244–252. [Google Scholar] [CrossRef]
- Deniffel, D.; Healy, G.M.; Dong, X.; Ghai, S.; Salinas-Miranda, E.; Fleshner, N.; Hamilton, R.; Kulkarni, G.; Toi, A.; van der Kwast, T.; et al. Avoiding Unnecessary Biopsy: MRI-based Risk Models versus a PI-RADS and PSA Density Strategy for Clinically Significant Prostate Cancer. Radiology 2021, 300, 369–379. [Google Scholar] [CrossRef]
- Remmers, A.; Kasivisvanathan, V.; Verbeek, J.; Moore, C.M.; Roobol, M.J.; ERSPC Rotterdam Study Group and PRECISION Investigators Group. Reducing Biopsies and Magnetic Resonance Imaging Scans During the Diagnostic Pathway of Prostate Cancer: Applying the Rotterdam Prostate Cancer Risk Calculator to the PRECISION Trial Data. Eur. Urol. Open Sci. 2022, 36, 1–8. [Google Scholar] [CrossRef]
- Mazzone, E.; Stabile, A.; Pellegrino, F.; Basile, G.; Cignoli, D.; Cirulli, G.O.; Sorce, G.; Barletta, F.; Scuderi, S.; Bravi, C.A.; et al. Positive Predictive Value of Prostate Imaging Reporting and DataSystem Version 2 for the Detection of Clinically Significant Prostate Cancer: A Systematic Review and Meta-analysis. Eur. Urol. Oncol. 2020, 4, 697–713. [Google Scholar] [CrossRef] [PubMed]
- Schoots, I.G. MRI in early prostate cancer detection: How to manage indeterminate or equivocal PI-RADS 3lesions. Transl. Urol. 2018, 7, 70–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osses, D.F.; Roobol, M.J.; Schoots, I.G. Prediction Medicine: Biomarkers, Risk Calculators and Magnetic Resonance Imaging as Risk Stratification Tools in Prostate Cancer Diagnosis. Int. J. Mol. Sci. 2019, 20, 1637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abreu-Gomez, J.; Wu, M.; McInnes, M.D.F.; Thornhill, R.E.; Flood, T.A.; Schieda, N. Shape Analysis of Peripheral Zone Observations on Prostate DWI: Correlation to Histopathology Outcomes After Radical Prostatectomy. AJR. Am. J. Roentgenol. 2020, 214, 1239–1247. [Google Scholar] [CrossRef]
- Boschheidgen, M.; Schimmöller, L.; Arsov, C.; Ziayee, F.; Morawitz, J.; Valentin, B.; Radke, K.L.; Giessing, M.; Esposito, I.; Albers, P.; et al. MRI grading for the prediction of prostate cancer aggressiveness. Eur. Radiol. 2021, 32, 2351–2359. [Google Scholar] [CrossRef] [PubMed]
- Rapisarda, S.; Bada, M.; Crocetto, F.; Barone, B.; Arcaniolo, D.; Polara, A.; Imbimbo, C.; Grosso, G. The role of multiparametric resonance and biopsy in prostate cancer detection: Comparison with definitive histological report after laparoscopic/robotic radical prostatectomy. Abdom. Radiol. 2020, 45, 4178–4184. [Google Scholar] [CrossRef] [PubMed]
- Khoo, C.; Eldred-Evans, D.; Peters, M.; van Son, M.; van Rossum, P.S.N.; Connor, M.J.; Hosking-Jervis, F.; Tanaka, M.B.; Reddy, D.; Bass, E.; et al. Comparison of Prostate Cancer Detection between Visual Estimation (Cognitive Registration) and Image Fusion (Software Registration) Targeted Transperineal Prostate Biopsy. J. Urol. 2021, 205, 1075–10781. [Google Scholar] [CrossRef] [PubMed]
- Ferro, M.; de Cobelli, O.; Vartolomei, M.D.; Lucarelli, G.; Crocetto, F.; Barone, B.; Sciarra, A.; Del Giudice, F.; Muto, M.; Maggi, M.; et al. Prostate Cancer Radiogenomics-From Imaging to Molecular Characterization. Int. J. Mol. Sci. 2021, 22, 9971. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Development Cohort | External Validation Cohort | p Value |
|---|---|---|---|
| Number of men | 1486 | 946 | - |
| Caucasian race, n (%) | 1465 (98.6) | 931 (98.4) | 0.738 |
| Median age at biopsy (IQR), years | 69 (62–74) | 67 (61–72) | <0.001 |
| Median serum PSA (IQR), ng/mL | 6.0 (4.4–9.2) | 7.4 (5.5–10.9) | <0.001 |
| Abnormal DRE, n (%) | 329 (22.1) | 283 (29.9) | <0.001 |
| PCa family history, n (%) | 127 (8.5) | 34 (3.6) | <0.001 |
| Median prostate volume (IQR), mL | 55 (40–76) | 55 (40–78) | 0.559 |
| Prior negative prostate biopsy, n (%) | 388 (26.1) | 293 (31.0) | 0.010 |
| PI-RADS v.2.0, n (%) | |||
| 1 | 242 (16.3) | 185 (19.6) | <0.001 |
| 2 | 73 (4.9) | 50 (5.3) | |
| 3 | 444 (29.9) | 201 (21.2) | |
| 4 | 450 (30.3) | 391 (41.3) | |
| 5 | 277 (18.6) | 119 (12.6) | |
| PCa detection, n (%) | 693 (46.6) | 521 (55.1) | <0.001 |
| csPCa detection, n (%) | 548 (36.9) | 386 (40.8) | 0.054 |
| iPCa detection, n (%) | 145 (9.8) | 135 (14.3) | <0.001 |
| Predictor | Odds Ratio (95% CI) | p Value |
|---|---|---|
| Age at prostate biopsy, ref. prior year | 1.056 (1.036–1.077) | <0.001 |
| Serum PSA, ref. prior ng/mL | 1.085 (1.056–1.114) | <0.001 |
| DRE, ref. normal. | 1.730 (1.195–2.503) | 0.004 |
| Prostate volume, ref. prior mL | 0.970 (0.964–0.977) | <0.001 |
| Family history of PCa, ref. no | 1.788 (1.066–3.002) | 0.028 |
| Biopsy type, ref. initial | 0.668 (0.478–0.934) | 0.018 |
| PI-RADS v.2.0 score, 2 to ref. 1 | 3.311 (1.008–10.879) | 0.048 |
| 3 to ref. 1 | 6.551 (2.740–15.661) | <0.001 |
| 4 to ref. 1 | 32.088 (13.660–75.377) | <0.001 |
| 5 to ref. 1 | 75.673 (30.738–186.311) | <0.001 |
| Predictor | Development Cohort (A) | External Validation Cohort (B) | ||||||
|---|---|---|---|---|---|---|---|---|
| AUC (95% CI) | Specificities According to Sensitivity | AUC (95% CI) | Specificities According to Sensitivity | |||||
| 85% | 90% | 95% | 85% | 90% | 95% | |||
| mpMRI | 0.842 (0.822–0.861) | 72.4 (69.4–75.2%) | 56.8 (53.6–60.0) | 40.7 (37.5–43.9) | 0.743 (0.711–0.776) | 45.5 (41.3–49.7) | 41.3 (32.9–48.3) | 14.3 (11.6–17.5) |
| MRI-PM | 0.897 (0.880–0.914) | 78.1% (75.3–80.7) | 69.5 (66.4–72.4) | 55.7 (52.5–58.9) | 0.858 (0.833–0.883) | 67.7 (63.6–71.5) | 52.3 (48.1–56.5) | 32.3 (28.5–36.4) |
| p Value | =0.011 | p = 0.005 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| PI-RADS | Development Cohort (A) | External Validation Cohort (B) | ||
|---|---|---|---|---|
| Missed csPCa | Avoidable Biopsies | Missed csPCa | Avoidable Biopsies | |
| 1–2, n (%) | 6/9 (66.7) | 203/212 (95.7) | 36/44 (81.8) | 232/248 (93.5) |
| 3, n (%) | 13/46 (28.2) | 185/299 (61.9) | 6/43 (14.0) | 134/212 (63.2) |
| 4, n (%) | 1/159 (0.6) | 12/303 (4.0) | 4/215 (1.9) | 30/413 (7.3%) |
| 5, n (%) | 0/155 (0) | 1/186 (0.5) | 1/106 (0.9) | 3/126 (2.4) |
| All, n (%) | 20/369 (5.4) | 401/1000 (40.1) | 47/408 (11.5) | 399/1000 (39.9) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morote, J.; Borque-Fernando, A.; Triquell, M.; Celma, A.; Regis, L.; Escobar, M.; Mast, R.; de Torres, I.M.; Semidey, M.E.; Abascal, J.M.; et al. The Barcelona Predictive Model of Clinically Significant Prostate Cancer. Cancers 2022, 14, 1589. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14061589
Morote J, Borque-Fernando A, Triquell M, Celma A, Regis L, Escobar M, Mast R, de Torres IM, Semidey ME, Abascal JM, et al. The Barcelona Predictive Model of Clinically Significant Prostate Cancer. Cancers. 2022; 14(6):1589. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14061589
Chicago/Turabian StyleMorote, Juan, Angel Borque-Fernando, Marina Triquell, Anna Celma, Lucas Regis, Manel Escobar, Richard Mast, Inés M. de Torres, María E. Semidey, José M. Abascal, and et al. 2022. "The Barcelona Predictive Model of Clinically Significant Prostate Cancer" Cancers 14, no. 6: 1589. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14061589