
Segmental Evaluation of Thoracic Aortic Calcium and Their Relations with Cardiovascular Risk Factors in the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil)

 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Cardiovascular Risk Assessment
2.3. Imaging Techniques
2.4. Statistical Analyses
3. Results
3.1. Patient Characteristics
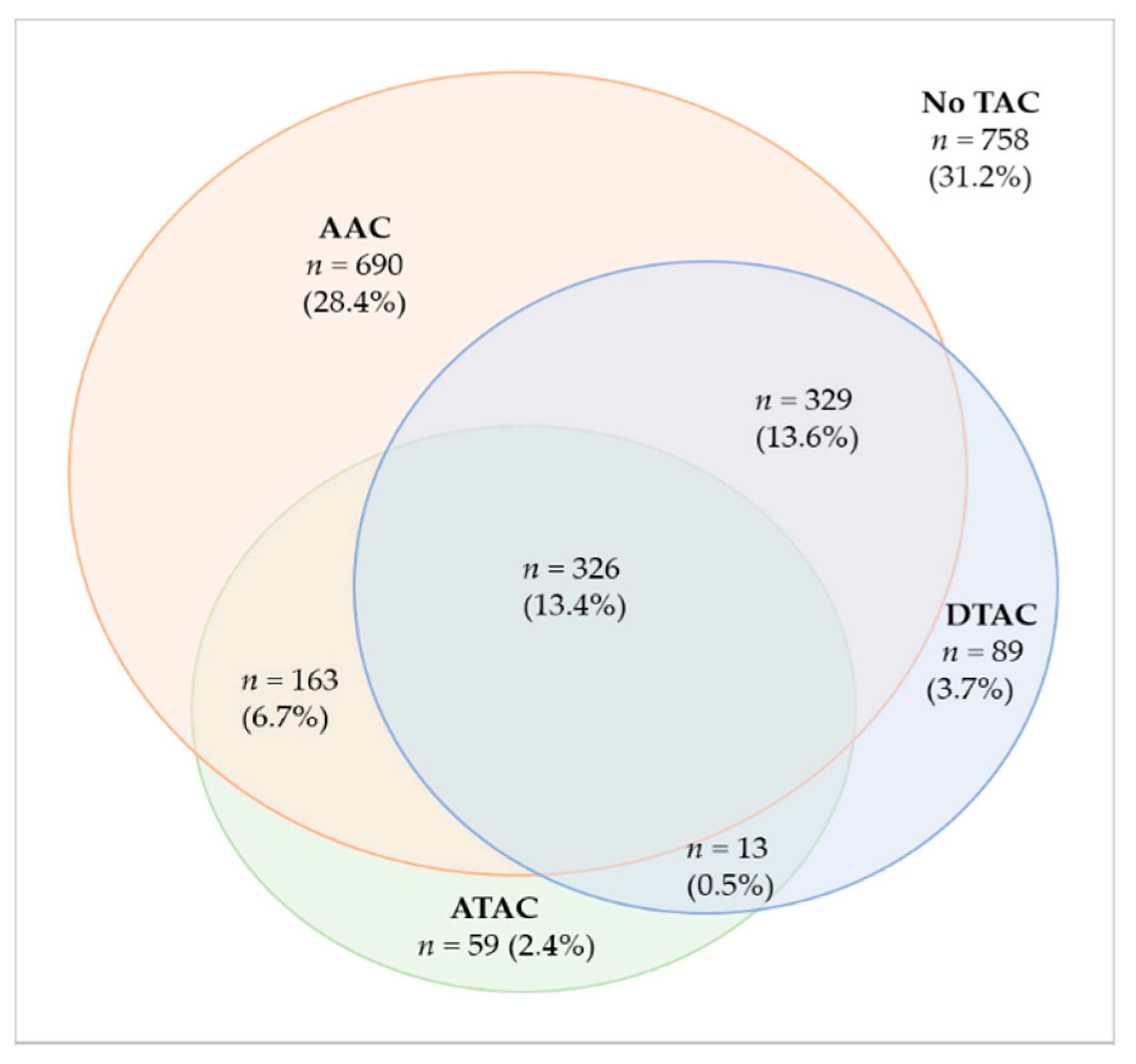
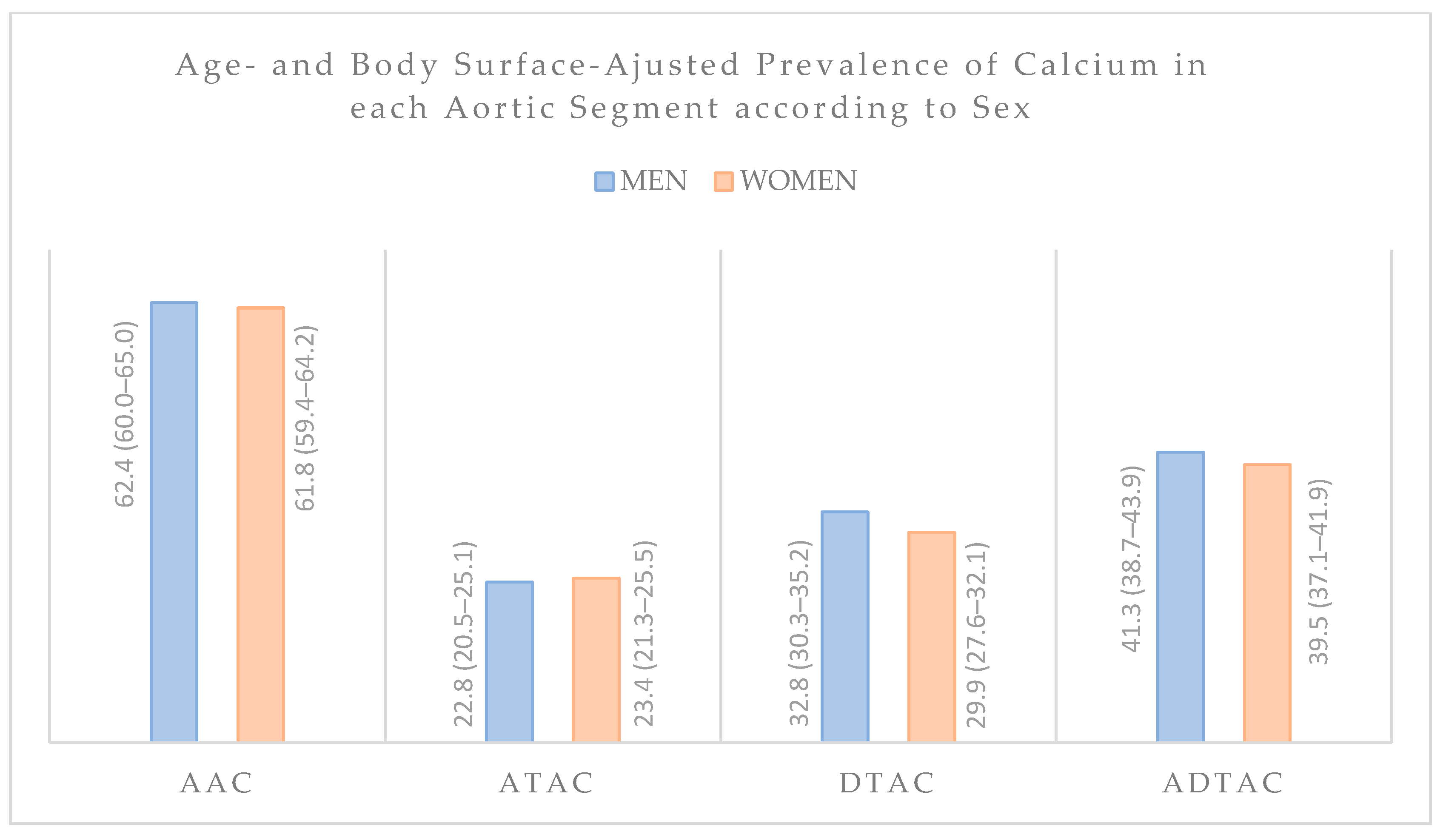
3.2. Calcium Distribution along Thoracic Aorta
3.3. Association between Risk Factors and Calcification
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Desai, M.Y.; Cremer, P.C.; Schoenhagen, P. Thoracic Aortic Calcification: Diagnostic, Prognostic, and Management Considerations. JACC Cardiovasc. Imaging 2018, 11, 1012–1026. [Google Scholar] [CrossRef]
- Ahmad, M.M.; Pir, S.H.A.; Muhammad, M.N.; Hussaini, S.; Kiani, I.A.; Ahmad, M.N.; Razzaque, I.; Syed, M.N.; Ullah, R.; Allaqaband, S.; et al. Influence of Differential Calcification in the Descending Thoracic Aorta on Aortic Pulse Pressure. J. Patient-Cent. Res. Rev. 2017, 4, 104–113. [Google Scholar] [CrossRef]
- Mitchell, G.F. Effects of central arterial aging on the structure and function of the peripheral vasculature: Implications for end-organ damage. J. Appl. Physiol. 2008, 105, 1652–1660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pedrosa, J.F.; Ribeiro, A.L.P.; Santana, P.C.; Araújo, L.F.; Barreto, S.M. Relation of Thoracic Aortic and Coronary Artery Calcium to Cardiovascular Risk Factors (from The Brazilian Longitudinal Study of Adult Health [ELSA-Brazil]). Am. J. Cardiol. 2019, 124, 1655–1661. [Google Scholar] [CrossRef] [PubMed]
- Kälsch, H.; Lehmann, N.; Möhlenkamp, S.; Hammer, C.; Mahabadi, A.A.; Moebus, S.; Schmermund, A.; Stang, A.; Bauer, M.; Jöckel, K.H.; et al. Prevalence of thoracic aortic calcification and its relationship to cardiovascular risk factors and coronary calcification in an unselected population-based cohort: The Heinz Nixdorf Recall Study. Int. J. Cardiovasc. Imaging 2013, 29, 207–216. [Google Scholar] [CrossRef] [PubMed]
- Nasir, K.; Roguin, A.; Sarwar, A.; Rumberger, J.A.; Blumenthal, R.S. Gender differences in coronary arteries and thoracic aorta calcification. Arterioscler. Thromb. Vasc. Biol. 2007, 27, 1220–1222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rivera, J.J.; Nasir, K.; Katz, R.; Takasu, J.; Allison, M.; Wong, N.D.; Barr, R.G.; Carr, J.J.; Blumenthal, R.S.; Budoff, M.J. Relationship of Thoracic Aortic Calcium to Coronary Calcium and Its Progression (from the Multi-Ethnic Study of Atherosclerosis [MESA]). Am. J. Cardiol. 2009, 103, 1562–1567. [Google Scholar] [CrossRef] [PubMed]
- Ong, K.-L.; McClelland, R.L.; Rye, K.-A.; Cheung, B.M.Y.; Post, W.S.; Vaidya, D.; Criqui, M.H.; Cushman, M.; Barter, P.J.; Allison, M.A. The relationship between insulin resistance and vascular calcification in coronary arteries, and the thoracic and abdominal aorta: The Multi-Ethnic Study of Atherosclerosis. Atherosclerosis 2014, 236, 257–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, I.C.; Thompson, C.A.; Yang, M.; Allison, M.A.; Forbang, N.I.; Michos, E.D.; McClelland, R.L.; Budoff, M.J.; Criqui, M.H. Thoracic aorta calcification and noncardiovascular disease-related mortality the multi-ethnic study of atherosclerosis. Arterioscler. Thromb. Vasc. Biol. 2018, 38, 1926–1932. [Google Scholar] [CrossRef] [Green Version]
- Mahabadi, A.A.; Lehmann, N.; Möhlenkamp, S.; Pundt, N.; Dykun, I.; Roggenbuck, U.; Moebus, S.; Jöckel, K.-H.; Erbel, R.; Kälsch, H.; et al. Noncoronary Measures Enhance the Predictive Value of Cardiac CT Above Traditional Risk Factors and CAC Score in the General Population. JACC Cardiovasc. Imaging 2016, 9, 1177–1185. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, U.; Massaro, J.M.; D’Agostino, R.B.; Kathiresan, S.; Fox, C.S.; O’Donnell, C.J. Cardiovascular Event Prediction and Risk Reclassification by Coronary, Aortic, and Valvular Calcification in the Framingham Heart Study. J. Am. Heart Assoc. 2016, 5, e003144. [Google Scholar] [CrossRef] [Green Version]
- Brodov, Y.; Gransar, H.; Rozanski, A.; Hayes, S.W.; Friedman, J.D.; Thomson, L.E.J.; Dey, D.; Slomka, P.J.; Min, J.K.; Shaw, L.J.; et al. Extensive thoracic aortic calcification is an independent predictor of development of coronary artery calcium among individuals with coronary artery calcium score of zero. Atherosclerosis 2015, 238, 4–8. [Google Scholar] [CrossRef] [PubMed]
- Pedrosa, J.F.; Barreto, S.M.; Bittencourt, M.S.; Ribeiro, A.L.P. Anatomical References to Evaluate Thoracic Aorta Calcium by Computed Tomography. Curr. Atheroscler. Rep. 2019, 21, 51. [Google Scholar] [CrossRef] [PubMed]
- Leroux-Berger, M.; Queguiner, I.; MacIel, T.T.; Ho, A.; Relaix, F.; Kempf, H. Pathologic calcification of adult vascular smooth muscle cells differs on their crest or mesodermal embryonic origin. J. Bone Miner. Res. 2011, 26, 1543–1553. [Google Scholar] [CrossRef]
- Wong, N.D.; Gransar, H.; Shaw, L.; Polk, D.; Moon, J.H.; Miranda-Peats, R.; Hayes, S.W.; Thomson, L.E.J.; Rozanski, A.; Friedman, J.D.; et al. Thoracic Aortic Calcium Versus Coronary Artery Calcium for the Prediction of Coronary Heart Disease and Cardiovascular Disease Events. JACC Cardiovasc. Imaging 2009, 2, 319–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kälsch, H.; Lehmann, N.; Moebus, S.; Hoffmann, B.; Stang, A.; Jöckel, K.; Erbel, R.; Mahabadi, A.A. Aortic Calcification Onset and Progression: Association With the Development of Coronary Atherosclerosis. J. Am. Heart Assoc. 2017, 6, e005093. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dudink, E.A.M.P.; Peeters, F.E.C.M.; Altintas, S.; Heckman, L.I.B.; Haest, R.J.; Kragten, H.; Kietselaer, B.L.J.H.; Wildberger, J.; Luermans, J.G.L.M.; Weijs, B.; et al. Agatston score of the descending aorta is independently associated with coronary events in a low-risk population. Open Heart 2018, 5, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Thomas, I.C.; McClelland, R.L.; Michos, E.D.; Allison, M.A.; Forbang, N.I.; Longstreth, W.T.; Post, W.S.; Wong, N.D.; Budoff, M.J.; Criqui, M.H. Density of calcium in the ascending thoracic aorta and risk of incident cardiovascular disease events. Atherosclerosis 2017, 265, 190–196. [Google Scholar] [CrossRef]
- Thomas, I.C.; McClelland, R.L.; Allison, M.A.; Ix, J.H.; Michos, E.D.; Forbang, N.I.; Post, W.S.; Wong, N.D.; Budoff, M.J.; Criqui, M.H. Progression of calcium density in the ascending thoracic aorta is inversely associated with incident cardiovascular disease events. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 1343–1350. [Google Scholar] [CrossRef] [Green Version]
- Churchill, T.W.; Rasania, S.P.; Rafeek, H.; Mulvey, C.K.; Terembula, K.; Ferrari, V.; Jha, S.; Lilly, S.M.; Eraso, L.H.; Reilly, M.P.; et al. Ascending and descending thoracic aorta calcification in type 2 diabetes mellitus. J. Cardiovasc. Comput. Tomogr. 2015, 9, 373–381. [Google Scholar] [CrossRef]
- Aquino, E.M.L.; Barreto, S.M.; Bensenor, I.M.; Carvalho, M.S.; Chor, D.; Duncan, B.B.; Lotufo, P.A.; Mill, J.G.; Molina, M.D.C.; Mota, E.L.A.; et al. Brazilian Longitudinal Study of Adult Health (ELSA-Brasil): Objectives and Design. Am. J. Epidemiol. 2012, 175, 315–324. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, M.I.; Duncan, B.B.; Mill, J.G.; Lotufo, P.A.; Chor, D.; Barreto, S.M.; Aquino, E.M.L.; Passos, V.M.A.; Matos, S.M.A.; Molina, M.D.C.B.; et al. Cohort profile: Longitudinal study of adult health (ELSA-Brasil). Int. J. Epidemiol. 2015, 44, 68–75. [Google Scholar] [CrossRef] [Green Version]
- Camelo, L.D.V.; Giatti, L.; Barreto, S.M. Subjective social status, self-rated health and tobacco smoking: Brazilian Longitudinal Study of Adult Health (ELSA-Brasil). J. Health Psychol. 2014, 19, 1388–1399. [Google Scholar] [CrossRef] [PubMed]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-Country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brant, L.C.C.; Hamburg, N.M.; Barreto, S.M.; Benjamin, E.J.; Ribeiro, A.L.P. Relations of digital vascular function, cardiovascular risk factors, and arterial stiffness: The Brazilian Longitudinal Study of Adult Health (ELSA-Brasil) cohort study. J. Am. Heart Assoc. 2014, 3, e001279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chor, D.; Alves, M.G.D.M.; Giatti, L.; Cade, N.V.; Nunes, M.A.; Molina, M.D.C.B.; Bensenor, I.M.; Aquino, E.M.L.; Passos, V.; Santos, S.M.; et al. Questionario do ELSA-Brasil: Desafios na elaboracao de instrumento multidimensional. Rev. Saúde Pública 2013, 47, 27–36. [Google Scholar] [CrossRef] [Green Version]
- Agatston, A.S.; Janowitz, F.W.R.; Hildner, F.J.; Zusmer, N.R.; Viamonte, M.; Detrano, R. Quantification of coronary artery calcium using ultrafast computed tomography. JACC 1990, 15, 827–832. [Google Scholar] [CrossRef] [Green Version]
- Craiem, D.; Chironi, G.; Casciaro, M.E.; Graf, S.; Simon, A. Calcifications of the Thoracic Aorta on Extended Non-Contrast-Enhanced Cardiac CT. PLoS ONE 2014, 9, e109584. [Google Scholar] [CrossRef]
- Takasu, J.; Katz, R.; Nasir, K.; Carr, J.J.; Wong, N.; Detrano, R.; Budoff, M.J. Relationships of thoracic aortic wall calcification to cardiovascular risk factors: The Multi–Ethnic Study of Atherosclerosis (MESA). Am. Heart J. 2008, 155, 765–771. [Google Scholar] [CrossRef] [Green Version]
- Ku, D.N.; Giddens, D.P.; Zarins, C.K.; Glagov, S. Pulsatile flow and atherosclerosis in the human carotid bifurcation. Positive correlation between plaque location and low and oscillating shear stress. Arteriosclerosis 1985, 5, 293–302. [Google Scholar] [CrossRef] [Green Version]
- Durham, A.L.; Speer, M.Y.; Scatena, M.; Giachelli, C.M.; Shanahan, C.M. Role of smooth muscle cells in vascular calcification: Implications in atherosclerosis and arterial stiffness. Cardiovasc. Res. 2018, 114, 590–600. [Google Scholar] [CrossRef]
- Sorokin, V.; Vickneson, K.; Kofidis, T.; Woo, C.C.; Lin, X.Y.; Foo, R.; Shanahan, C.M. Role of Vascular Smooth Muscle Cell Plasticity and Interactions in Vessel Wall Inflammation. Front. Immunol. 2020, 11, 3053. [Google Scholar] [CrossRef]
- Gurung, R.; Choong, A.M.; Woo, C.C.; Foo, R.; Sorokin, V. Genetic and epigenetic mechanisms underlying vascular smooth muscle cell phenotypic modulation in abdominal aortic aneurysm. Int. J. Mol. Sci. 2020, 21, 6334. [Google Scholar] [CrossRef]
- Tadic, M.; Cuspidi, C. Pulse pressure and aortic calcification: Did we learn something? J. Clin. Hypertens. 2020, 22, 886–887. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Youssef, G.; Guo, M.; McClelland, R.L.; Shavelle, D.M.; Nasir, K.; Rivera, J.; Carr, J.J.; Wong, N.D.; Budoff, M.J. Risk Factors for the Development and Progression of Thoracic Aorta Calcification: The Multi-Ethnic Study of Atherosclerosis. Acad. Radiol. 2015, 22, 1536–1545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iribarren, C.; Sidney, S.; Sternfeld, B.; Browner, W.S. Calcification of the Aortic Arch. JAMA 2000, 283, 2810–2815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, N.D.; Sciammarella, M.; Arad, Y.; Miranda-Peats, R.; Polk, D.; Hachamovich, R.; Friedman, J.; Hayes, S.; Daniell, A.; Berman, D.S. Relation of thoracic aortic and aortic valve calcium to coronary artery calcium and risk assessment. Am. J. Cardiol. 2003, 92, 951–955. [Google Scholar] [CrossRef]
- Renaud, S.; Blache, D.; Dumont, E.; Thevenon, C.; Wissendanger, T. Platelet function after cigarette smoking in relation to nicotine and carbon monoxide. Clin. Pharmacol. Ther. 1984, 36, 389–395. [Google Scholar] [CrossRef] [PubMed]
- Allison, M.A.; Hsi, S.; Wassel, C.L.; Morgan, C.; Ix, J.H.; Wright, C.M.; Criqui, M.H. Calcified atherosclerosis in different vascular beds and the risk of mortality. Arterioscler. Thromb. Vasc. Biol. 2012, 32, 140–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, M.; Chern, M.; Chen, L.; Lin, Y.; Sheu, M. Electron Beam Computed Tomography Evidence of Aortic Calcification as an Independent Determinant of Coronary Artery Calcification. J. Chin. Med Assoc. 2006, 69, 409–414. [Google Scholar] [CrossRef] [Green Version]
- Odink, A.E.; van der Lugt, A.; Hofman, A.; Hunink, M.G.M.; Breteler, M.M.B.; Krestin, G.P.; Witteman, J.C.M. Association between calcification in the coronary arteries, aortic arch and carotid arteries: The Rotterdam study. Atherosclerosis 2007, 193, 408–413. [Google Scholar] [CrossRef] [PubMed]
- Gerber, T.C.; Jeffrey Carr, J.; Arai, A.E.; Dixon, R.L.; Ferrari, V.A.; Gomes, A.S.; Heller, G.V.; McCollough, C.H.; McNitt-Gray, M.F.; Mettler, F.A.; et al. Ionizing radiation in cardiac imaging: A science advisory from the American Heart Association Committee on cardiac imaging of the council on clinical cardiology and committee on cardiovascular imaging and intervention of the council on cardiovascular radi. Circulation 2009, 119, 1056–1065. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Variables | Population n = 2427 (100%) | AAC > 0 n = 1508 (62.1%) | ATAC > 0 n = 561 (23.1%) | DTAC > 0 n = 757 (31.2%) | ADTAC > 0 n = 979 (40.3%) |
|---|---|---|---|---|---|
| Age, years | 55.59 ± 8.68 | 58.46 ± 8.25 | 61.07 ± 7.90 | 60.79 ± 8.50 | 60.13 ± 8.36 |
| Women | 54.10 | 53.85 | 54.72 | 51.78 | 53.01 |
| Race/Skin color | |||||
| White | 48.69 | 50.23 | 53.79 | 51.94 | 51.50 |
| Brown | 35.29 | 34.21 | 32.31 | 32.80 | 33.40 |
| Black | 13.31 | 13.21 | 11.37 | 12.99 | 12.31 |
| Others (Asian, Indigenous) | 2.71 | 2.35 | 2.53 | 2.28 | 2.79 |
| Educational level | |||||
| University degree | 67.01 | 63.57 | 63.21 | 62.70 | 62.99 |
| Complete secondary | 25.24 | 26.28 | 24.82 | 25.53 | 25.97 |
| Complete elementary | 4.21 | 5.57 | 5.71 | 5.56 | 5.11 |
| Incomplete elementary | 3.55 | 4.58 | 6.25 | 6.22 | 5.93 |
| Smoker | |||||
| Never | 61.48 | 55.11 | 45.63 | 54.03 | 53.01 |
| Past | 28.99 | 33.29 | 41.00 | 33.42 | 34.83 |
| Current | 9.53 | 11.60 | 13.37 | 12.55 | 12.16 |
| Physical activity | |||||
| Insufficient | 71.26 | 70.09 | 67.02 | 71.07 | 70.38 |
| Moderate | 20.45 | 22.35 | 25.13 | 20.87 | 21.65 |
| Vigorous | 8.29 | 7.56 | 7.84 | 8.06 | 7.97 |
| Excessive use of alcohol | 10.47 | 11.07 | 13.73 | 12.15 | 12.36 |
| Family history of CVD | 33.13 | 36.74 | 39.04 | 36.72 | 37.08 |
| Body mass index, kg/m2 | 26.98 ± 4.73 | 27.44 ± 4.86 | 28.10 ± 5.30 | 27.75 ± 5.00 | 27.72 ± 5.01 |
| Dyslipidemia | 41.28 | 46.20 | 56.89 | 51.26 | 51.75 |
| Hypertension | 38.87 | 47.15 | 57.93 | 58.92 | 55.46 |
| Diabetes | 16.20 | 20.11 | 27.86 | 25.93 | 25.05 |
| Variables | AAC > 0 OR (95% Cl) | ATAC > 0 OR (95% CI) | DTAC > 0 OR (95% CI) | ADTAC > 0 OR (95% CI) |
|---|---|---|---|---|
| Age (years) | 1.12 (1.10–1.13) ‡ | 1.09 (1.08–1.11) ‡ | 1.11 (1.10–1.13) ‡ | 1.11 (1.10–1.13) ‡ |
| Women | 0.95 (0.78–1.16) | 1.14 (0.91–1.41) | 0.84 (0.68–1.02) | 0.93 (0.77–1.13) |
| Educational level | ||||
| University degree | 1.00 | 1.00 | 1.00 | 1.00 |
| Complete secondary | 1.18 (0.94–1.46) | 1.02 (0.79–1.30) | 1.03 (0.82–1.29) | 1.07 (0.86–1.34) |
| Complete elementary | 1.77 (1.01–3.11) * | 0.93 (0.57–1.51) | 0.94 (0.60–1.49) | 0.82 (0.52–1.29) |
| Incomplete elementary | 1.69 (0.93–3.08) | 1.79 (1.09–2.94) * | 1.74 (1.06–2.85) * | 2.10 (1.25–3.52) † |
| Smoker | ||||
| Never | 1.00 | 1.00 | 1.00 | 1.00 |
| Past | 1.26 (1.01–1.57) * | 1.79 (1.42–2.26) ‡ | 0.93 (0.74–1.16) | 1.15 (0.93–1.42) |
| Current | 2.07 (1.46–2.93) ‡ | 2.53 (1.80–3.56) ‡ | 1.76 (1.27–2.43) ‡ | 1.87 (1.36–2.56) ‡ |
| Physical activity | ||||
| Insufficient | 1.00 | 1.00 | 1.00 | 1.00 |
| Moderate | 1.22 (0.95–1.56) | 1.36 (1.05–1.76) * | 0.86 (0.67–1.10) | 0.95 (0.75–1.21) |
| Vigorous | 1.03 (0.73–1.44) | 1.32 (0.89–1.98) | 1.27 (0.88–1.83) | 1.29 (0.91–1.83) |
| Family history of CVD | 1.37 (1.12–1.68) † | 1.18 (0.95–1.47) | 1.08 (0.88–1.33) | 1.15 (0.94–1.40) |
| Body mass index (kg/m2) | 1.05 (1.03–1.07) ‡ | 1.06 (1.04–1.09) ‡ | 1.04 (1.02–1.07) ‡ | 1.05 (1.03–1.07) ‡ |
| Dyslipidemia | 1.20 (0.98–1.46) | 1.73 (1.40–2.14) ‡ | 1.29 (1.06–1.58) * | 1.52 (1.25–1.83) ‡ |
| Hypertension | 1.52 (1.24–1.88) ‡ | 1.62 (1.30–2.03) ‡ | 2.09 (1.71–2.57) ‡ | 1.96 (1.61–2.39) ‡ |
| Diabetes | 1.07 (0.80–1.43) | 1.35 (1.03–1.75) * | 1.33 (1.03–1.72) * | 1.46 (1.13–1.89) † |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pedrosa, J.F.; Brant, L.C.C.; de Aquino, S.A.; Ribeiro, A.L.; Barreto, S.M. Segmental Evaluation of Thoracic Aortic Calcium and Their Relations with Cardiovascular Risk Factors in the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil). Cells 2021, 10, 1243. https://0-doi-org.brum.beds.ac.uk/10.3390/cells10051243
Pedrosa JF, Brant LCC, de Aquino SA, Ribeiro AL, Barreto SM. Segmental Evaluation of Thoracic Aortic Calcium and Their Relations with Cardiovascular Risk Factors in the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil). Cells. 2021; 10(5):1243. https://0-doi-org.brum.beds.ac.uk/10.3390/cells10051243
Chicago/Turabian StylePedrosa, Jesiana Ferreira, Luisa Campos Caldeira Brant, Stephanie Alves de Aquino, Antonio Luiz Ribeiro, and Sandhi Maria Barreto. 2021. "Segmental Evaluation of Thoracic Aortic Calcium and Their Relations with Cardiovascular Risk Factors in the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil)" Cells 10, no. 5: 1243. https://0-doi-org.brum.beds.ac.uk/10.3390/cells10051243