
Optical Chemical Sensor Based on Fast-Protein Liquid Chromatography for Regular Peritoneal Protein Loss Assessment in End-Stage Renal Disease Patients on Continuous Ambulatory Peritoneal Dialysis

 , and
, and
Abstract
:1. Introduction
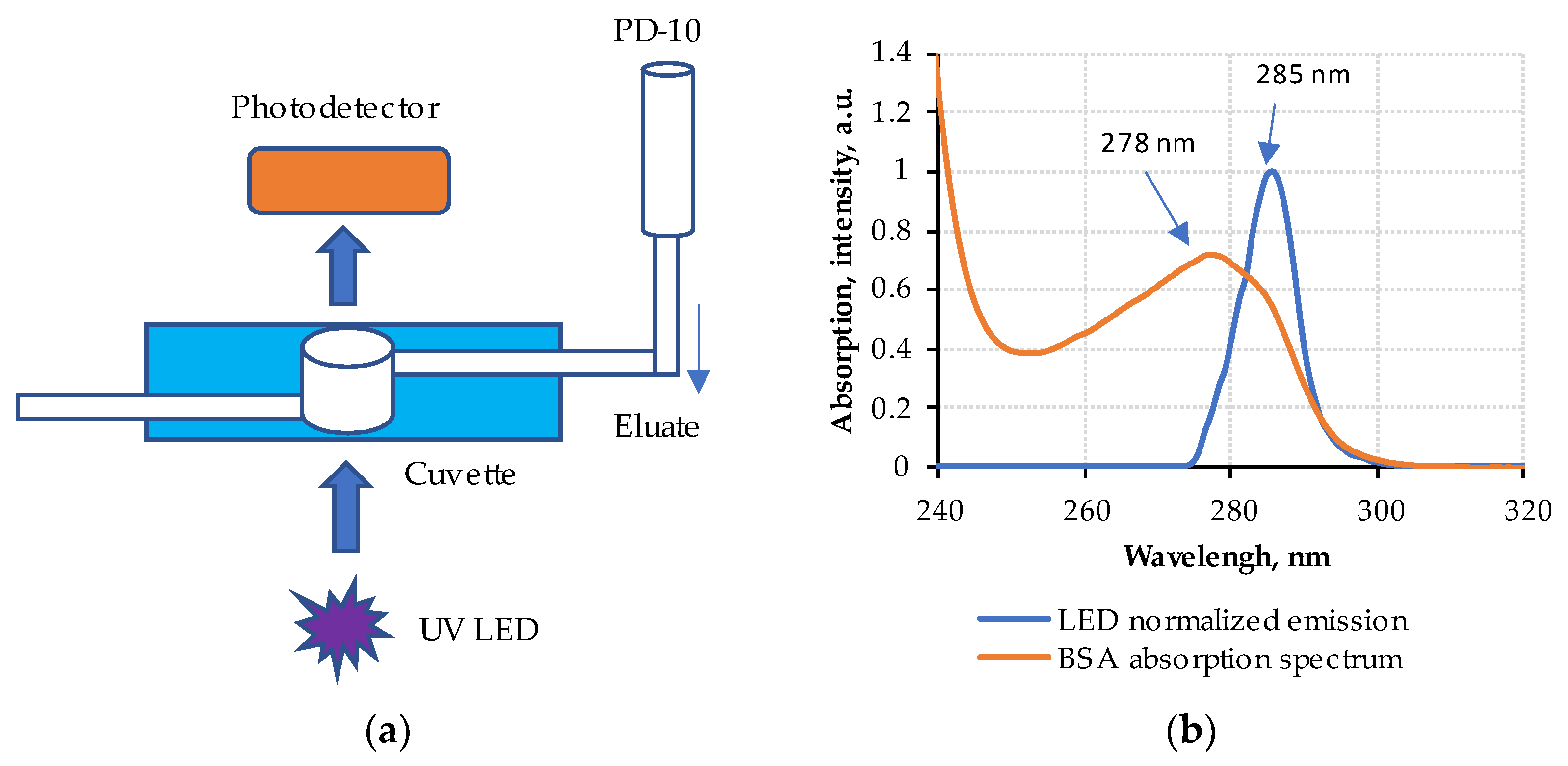
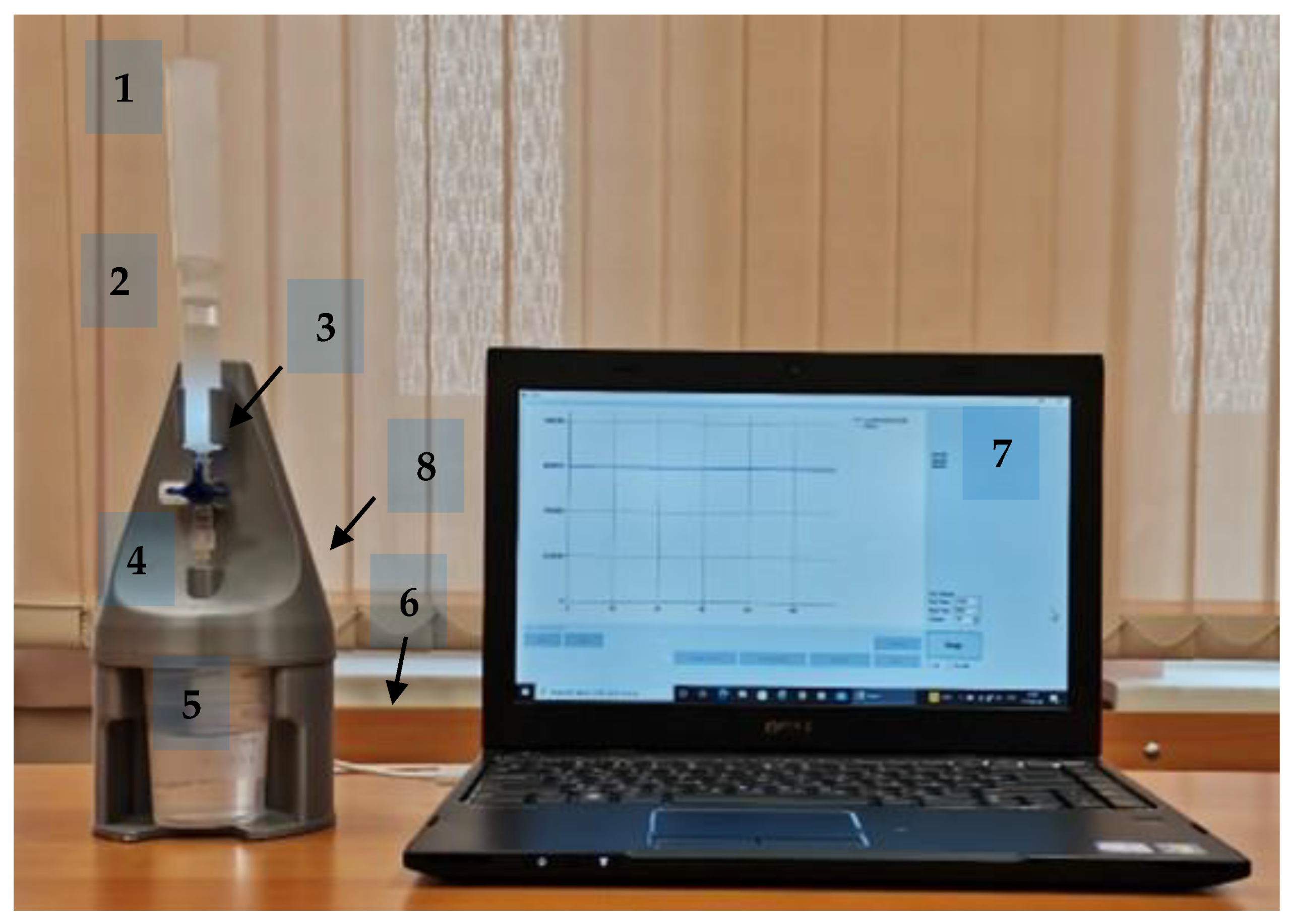
2. Materials and Methods
3. Results
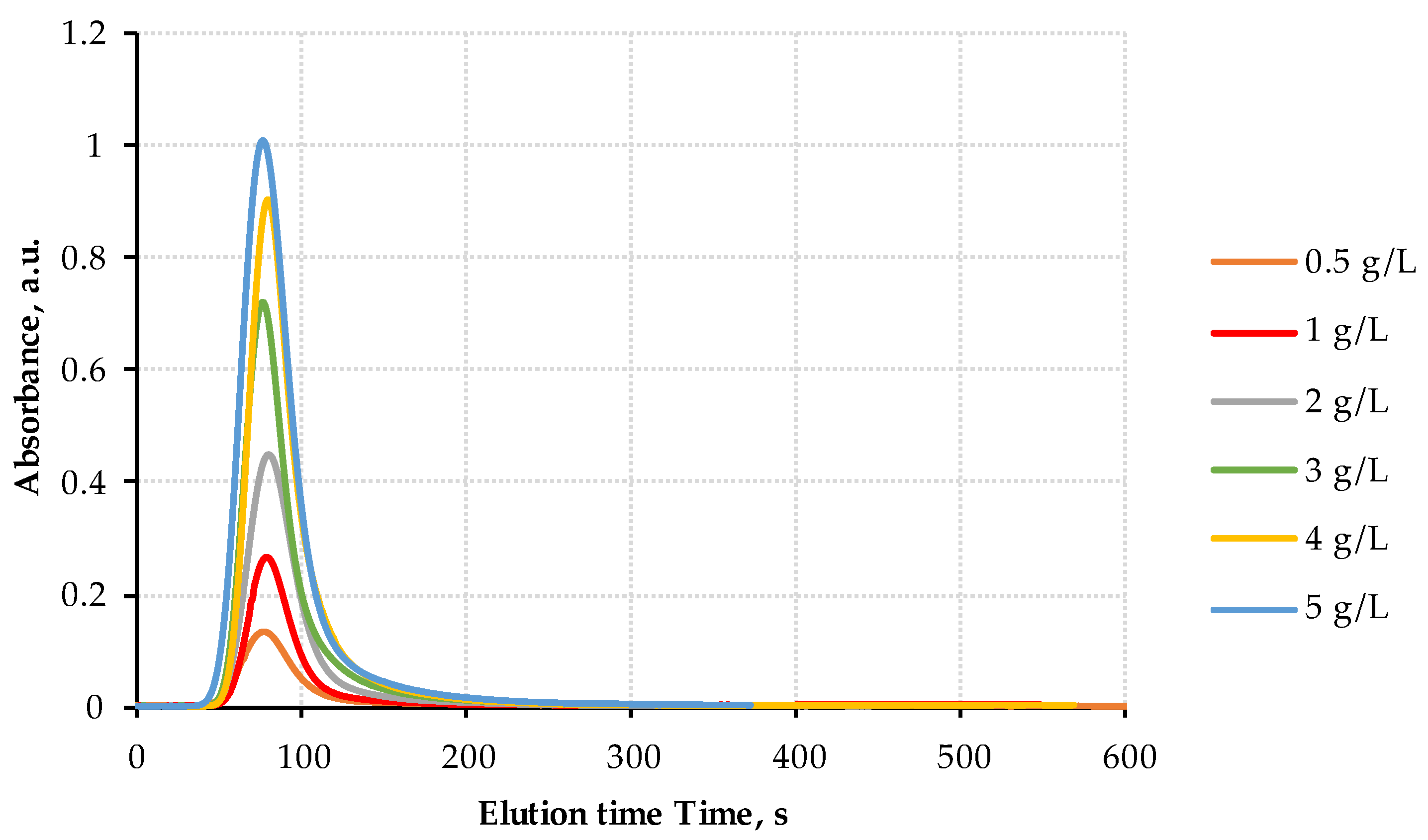
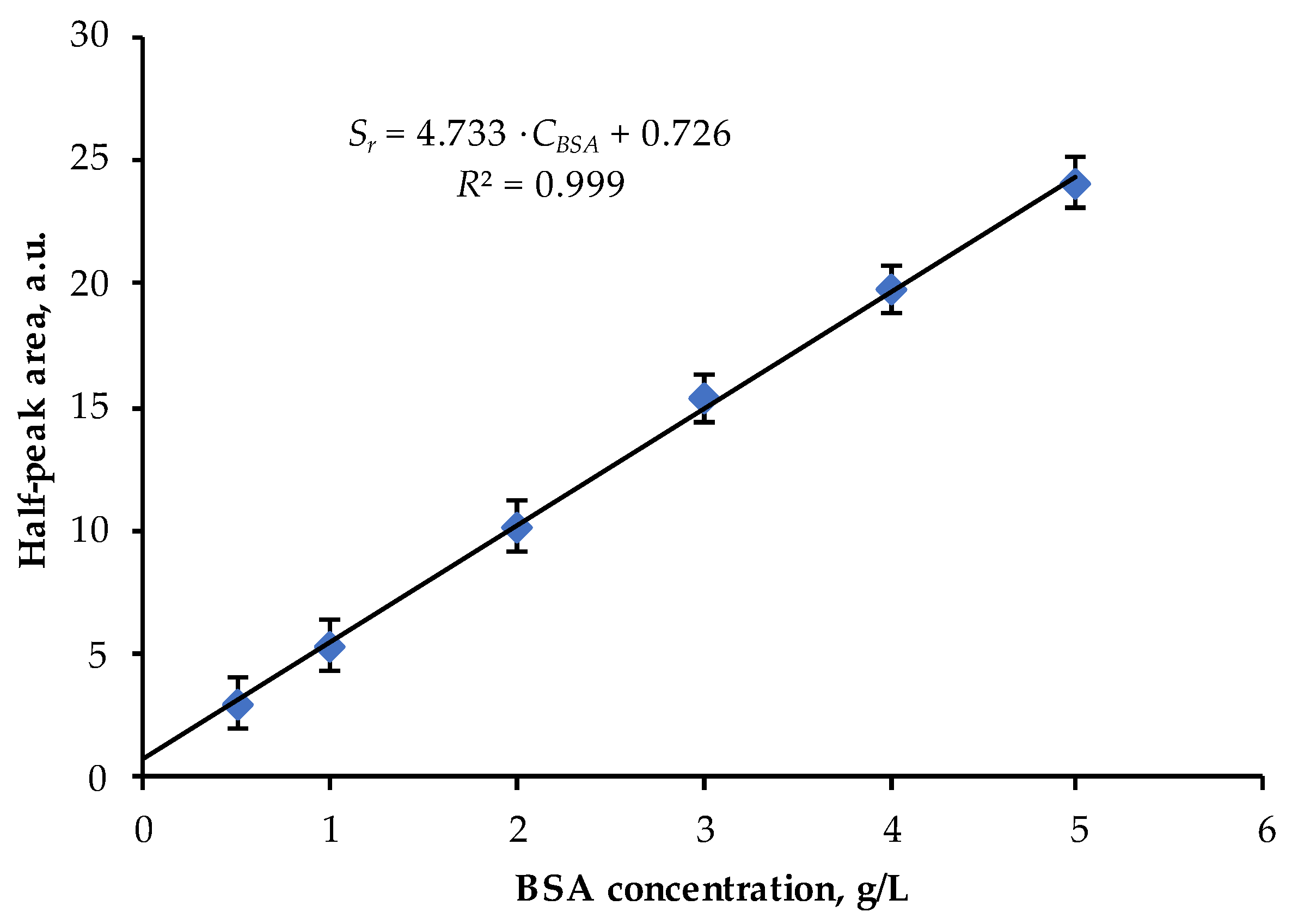
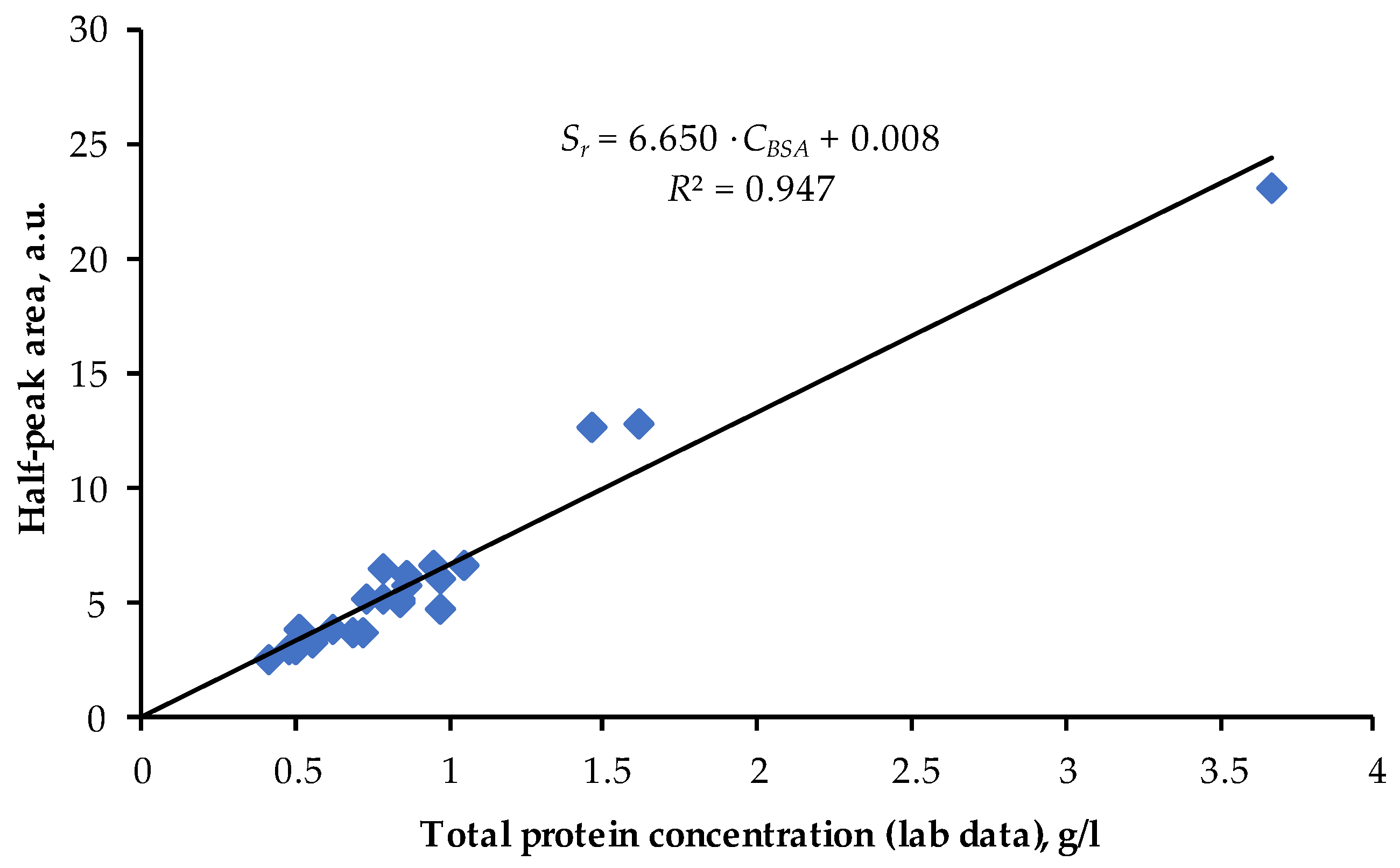
3.1. Calibration with BSA Solutions
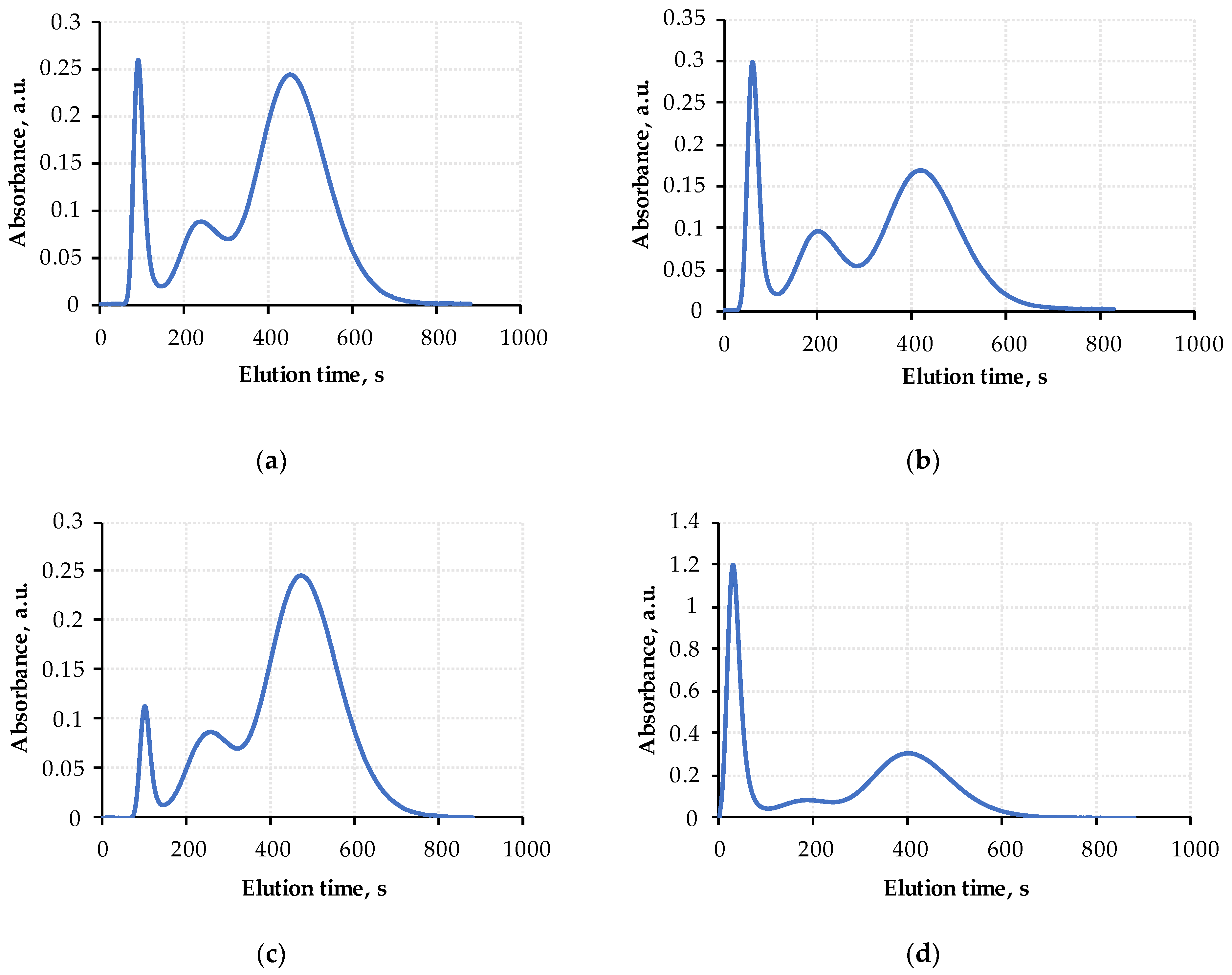
3.2. Effluent Peritoneal Dialysate Analysis
3.3. PD-10 Columns’ Regeneration and Life-Time
3.4. Chromatograms’ Approximation and Analysis
4. Discussion
5. Concluding Remarks
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lewandrowski, K. Point-of-Care Testing: An Overview and a Look to the Future (Circa 2009, United States). Clin. Lab. Med. 2009, 29, 421–432. [Google Scholar] [CrossRef] [PubMed]
- Wick, J.Y. Small Miracles: Point-of-Care Testing. Consult. Pharm. 2010, 25, 416–431. [Google Scholar] [CrossRef]
- Pezzuto, F.; Scarano, A.; Marini, C.; Rossi, G.; Stocchi, R.; Cerbo, A.D.; Cerbo, A.D. Assessing the Reliability of Commercially Available Point of Care in Various Clinical Fields. Open Public Health J. 2019, 12, 342–368. [Google Scholar] [CrossRef]
- Toppenberg, M.D.; Christiansen, T.E.M.; Rasmussen, F.; Nielsen, C.P.; Damsgaard, E.M. Mobile X-ray outside the hospital: A scoping review. BMC Health Serv. Res. 2020, 20, 767. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.; DeCara, J.M. Point-of-Care Ultrasound. Curr. Cardiol. Rep. 2020, 22, 149. [Google Scholar] [CrossRef]
- Siontis, K.C.; Noseworthy, P.A.; Attia, Z.I.; Friedman, P.A. Artificial intelligence-enhanced electrocardiography in cardiovascular disease management. Nat. Rev. Cardiol. 2021, 18, 465–478. [Google Scholar] [CrossRef]
- Rajsic, S.; Breitkopf, R.; Bachler, M.; Treml, B. Diagnostic Modalities in Critical Care: Point-of-Care Approach. Diagnostics 2021, 11, 2202. [Google Scholar] [CrossRef] [PubMed]
- Yager, P.; Domingo, G.J.; Gerdes, J. Point-of-Care Diagnostics for Global Health. Annu. Rev. Biomed. Eng. 2008, 10, 107–144. [Google Scholar] [CrossRef]
- Mondal, S.; Zehra, N.; Choudhury, A.; Iyer, P.K. Wearable Sensing Devices for Point of Care Diagnostics. ACS Appl. Bio Mater. 2020, 4, 47–70. [Google Scholar] [CrossRef]
- Zhang, S.; Zeng, J.; Wang, C.; Feng, L.; Song, Z.; Zhao, W.; Wang, Q.; Liu, C. The Application of Wearable Glucose Sensors in Point-of-Care Testing. Front. Bioeng. Biotechnol. 2021, 9, 774210. [Google Scholar] [CrossRef]
- Steinhubl, S.R.; Muse, E.D.; Topol, E.J. The emerging field of mobile health. Sci. Transl. Med. 2015, 7, 283rv3. [Google Scholar] [CrossRef] [Green Version]
- Yetisen, A.K.; Akram, M.S.; Lowe, C.R. Paper-based microfluidic point-of-care diagnostic devices. Lab Chip 2013, 13, 2210–2251. [Google Scholar] [CrossRef] [PubMed]
- Viderman, D.; Seri, E.; Aubakirova, M.; Abdildin, Y.; Badenes, R.; Bilotta, F. Remote Monitoring of Chronic Critically Ill Patients after Hospital Discharge: A Systematic Review. J. Clin. Med. 2022, 11, 1010. [Google Scholar] [CrossRef]
- Goble, J.A.; Rocafort, P.T. Point-of-Care Testing: Future of Chronic Disease State Management? J. Pharm. Pract. 2016, 30, 229–237. [Google Scholar] [CrossRef]
- Udugama, B.; Kadhiresan, P.; Kozlowski, H.N.; Malekjahani, A.; Osborne, M.; Li, V.Y.C.; Chan, W.C.W. Diagnosing COVID-19: The Disease and Tools for Detection. ACS Nano 2020, 14, 3822–3835. [Google Scholar] [CrossRef] [Green Version]
- Drain, P.K.; Hyle, E.P.; Noubary, F.; Freedberg, K.A.; Wilson, D.; Bishai, W.R.; Rodriguez, W.; Bassett, I.V. Diagnostic point-of-care tests in resource-limited settings. Lancet Infect. Dis. 2014, 14, 239–249. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Hong, X.-Z.; Li, Y.-W.; Li, Y.; Wang, J.; Chen, P.; Liu, B.-F. Microfluidics-based strategies for molecular diagnostics of infectious diseases. Mil. Med. Res. 2022, 9, 11. [Google Scholar] [CrossRef]
- Yang, Z.; Zhou, D.M. Cardiac markers and their point-of-care testing for diagnosis of acute myocardial infarction. Clin. Biochem. 2006, 39, 771–780. [Google Scholar] [CrossRef]
- Lingervelder, D.; Koffijberg, H.; Kusters, R.; IJzerman, M.J. Point-of-care testing in primary care: A systematic review on implementation aspects addressed in test evaluations. Int. J. Clin. Pract. 2019, 73, e13392. [Google Scholar] [CrossRef] [Green Version]
- Mejía-Salazar, J.R.; Rodrigues Cruz, K.; Materón Vásques, E.M.; Novais de Oliveira, O. Microfluidic Point-of-Care Devices: New Trends and Future Prospects for eHealth Diagnostics. Sensors 2020, 20, 1951. [Google Scholar] [CrossRef] [Green Version]
- Nasseri, B.; Soleimani, N.; Rabiee, N.; Kalbasi, A.; Karimi, M.; Hamblin, M.R. Point-of-care microfluidic devices for pathogen detection. Biosens. Bioelectron. 2018, 117, 112–128. [Google Scholar] [CrossRef] [PubMed]
- Arshavsky-Graham, S.; Segal, E. Lab-on-a-Chip Devices for Point-of-Care Medical Diagnostics. In Advances in Biochemical Engineering/Biotechnology; Scheper, T., Ulber, R., Eds.; Springer: Berlin/Heidelberg, Germany, 2020; pp. 1–19. [Google Scholar] [CrossRef]
- Haleem, A.; Javaid, M.; Singh, R.P.; Suman, R.; Rab, S. Biosensors applications in medical field: A brief review. Sens. Int. 2021, 2, 100100. [Google Scholar] [CrossRef]
- Xie, X.; Citterio, D.; Chumbimuni-Torres, K.; Xue, M.; Wang, X. Editorial: Chemical Sensors for Biomedical Use. Front. Chem. 2021, 9, 685563. [Google Scholar] [CrossRef] [PubMed]
- Bikbov, B.; Purcell, C.A.; Levey, A.S.; Smith, M.; Abdoli, A.; Abebe, M.; Adebayo, O.M.; Afarideh, M.; Agarwal, S.A.; Agudelo-Botero, M.; et al. Global, regional, and national burden of chronic kidney disease, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2020, 395, 709–733. [Google Scholar] [CrossRef] [Green Version]
- Thurlow, J.S.; Joshi, M.; Yan, G.; Norris, K.C.; Agodoa, L.Y.; Yuan, C.M.; Nee, R. Global Epidemiology of End-Stage Kidney Disease and Disparities in Kidney Replacement Therapy. Am. J. Nephrol. 2021, 52, 98–107. [Google Scholar] [CrossRef]
- Li, P.K.-T.; Chow, K.M.; Van de Luijtgaarden, M.W.M.; Johnson, D.W.; Jager, K.J.; Mehrotra, R.; Naicker, S.; Pecoits-Filho, R.; Yu, X.Q.; Lameire, N. Changes in the worldwide epidemiology of peritoneal dialysis. Nat. Rev. Nephrol. 2017, 13, 90–103. [Google Scholar] [CrossRef]
- Mehrotra, R.; Devuyst, O.; Davies, S.J.; Johnson, D.W. The Current State of Peritoneal Dialysis. J. Am. Soc. Nephrol. 2016, 27, 3238–3252. [Google Scholar] [CrossRef] [Green Version]
- Walker, R.C.; Howard, K.; Morton, R.L. Home hemodialysis: A comprehensive review of patient-centered and economic considerations. Clinicoecon. Outcomes Res. 2017, 9, 149–161. [Google Scholar] [CrossRef] [Green Version]
- Hörl, W.H.; Koch, K.-M.; Lindsay, R.M.; Ronco, C.; Winchester, J.F. Replacement of Renal Function by Dialysis, 5th ed.; Kluwer Academic Publishers: Amsterdam, The Netherlands, 2004; pp. 73–95. ISBN 1-4020-0083-9. [Google Scholar]
- Nissenson, A.; Fine, R. Handbook of Dialysis Therapy, 5th ed.; Elsevier: Amsterdam, The Netherlands, 2016; pp. 3–486. ISBN 978-0-323-39154-2. [Google Scholar]
- Grunert, T.; Herzog, R.; Wiesenhofer, F.M.; Vychytil, A.; Ehling-Schulz, M.; Kratochwill, K. Vibrational Spectroscopy of Peritoneal Dialysis Effluent for Rapid Assessment of Patient Characteristics. Biomolecules 2020, 10, 965. [Google Scholar] [CrossRef]
- Wang, Z.; Jiang, H.; Chen, X.; Song, X.; Xu, F.; Chen, F.; Mao, Z.; Gao, S.; Chen, W. A rapid and sensitive method for simultaneous determination of eight protein-bound uremic toxins in human serum by UHPLC-MS/MS: Application in assessing peritoneal dialysis. J. Pharm. Biomed. Anal. 2020, 186, 113312. [Google Scholar] [CrossRef]
- Teitelbaum, I.; Glickman, J.; Neu, A.; Neumann, J.; Rivara, M.B.; Shen, J.; Wallace, E.; Watnick, S.; Mehrotra, R. KDOQI US Commentary on the 2020 ISPD Practice Recommendations for Prescribing High-Quality Goal-Directed Peritoneal Dialysis. Am. J. Kidney Dis. 2021, 77, 157–171. [Google Scholar] [CrossRef]
- Bargnoux, A.-S.; Kuster, N.; Sutra, T.; Laroche, L.; Rodriguez, A.; Morena, M.; Chenine, L.; Chalabi, L.; Dupuy, A.-M.; Badiou, S.; et al. Evaluation of a new point-of-care testing for creatinine and urea measurement. Scand. J. Clin. Lab. Investig. 2021, 81, 290–297. [Google Scholar] [CrossRef] [PubMed]
- Nataatmadja, M.; Fung, A.W.S.; Jacobson, B.; Ferera, J.; Bernstein, E.; Komenda, P.; Mattman, A.; Seccombe, D.; Levin, A. Performance of StatSensor Point-of-Care Device for Measuring Creatinine in Patients with Chronic Kidney Disease and Postkidney Transplantation. Can. J. Kidney Health Dis. 2020, 7, 2054358120970716. [Google Scholar] [CrossRef] [PubMed]
- Fan, J.; Ye, H.; Zhang, X.; Cao, P.; Guo, Q.; Mao, H.; Yu, X.; Yang, X. Association of Lean Body Mass Index and Peritoneal Protein Clearance in Peritoneal Dialysis Patients. Kidney Blood Press. Res. 2019, 44, 94–102. [Google Scholar] [CrossRef] [PubMed]
- Asano, M.; Ishii, T.; Hirayama, A.; Mizuno, M.; Suzuki, Y.; Sakata, F.; Akiyama, S.; Maruyama, S.; Soga, T.; Kinashi, H.; et al. Differences in peritoneal solute transport rates in peritoneal dialysis. Clin. Exp. Nephrol. 2018, 23, 122–134. [Google Scholar] [CrossRef] [PubMed]
- Chang, T.I.; Kang, E.W.; Lee, Y.K.; Shin, S.K. Higher Peritoneal Protein Clearance as a Risk Factor for Cardiovascular Disease in Peritoneal Dialysis Patient. PLoS ONE 2013, 8, e56223. [Google Scholar] [CrossRef] [Green Version]
- Guedes, A.M. Peritoneal Protein Loss, Leakage or Clearance in Peritoneal Dialysis, Where Do We Stand? Perit. Dial. Int. 2019, 39, 201–209. [Google Scholar] [CrossRef]
- Lu, W.; Pang, W.-F.; Jin, L.; Li, H.; Chow, K.M.; Kwan, B.C.-H.; Leung, C.B.; Li, P.K.-T.; Szeto, C.C. Peritoneal protein clearance predicts mortality in peritoneal dialysis patients. Clin. Exp. Nephrol. 2018, 23, 551–560. [Google Scholar] [CrossRef]
- Dong, J.; Chen, Y.; Luo, S.; Xu, R.; Xu, Y. Peritoneal Protein Leakage, Systemic Inflammation, and Peritonitis Risk in Patients on Peritoneal Dialysis. Perit. Dial. Int. 2013, 33, 273–279. [Google Scholar] [CrossRef] [Green Version]
- Fung, W.W.-S.; Li, P.K.-T. Recent advances in novel diagnostic testing for peritoneal dialysis-related peritonitis. Kidney Res. Clin. Pract. 2022, 41, 156–164. [Google Scholar] [CrossRef]
- Goodlad, C.; George, S.; Sandoval, S.; Mepham, S.; Parekh, G.; Eberl, M.; Topley, N.; Davenport, A. Measurement of innate immune response biomarkers in peritoneal dialysis effluent using a rapid diagnostic point-of-care device as a diagnostic indicator of peritonitis. Kidney Int. 2020, 97, 1253–1259. [Google Scholar] [CrossRef] [PubMed]
- Dube, J.; Girouard, J.; Leclerc, P.; Douville, P. Problems with the estimation of urine protein by automated assays. Clin. Biochem. 2005, 38, 479–485. [Google Scholar] [CrossRef] [PubMed]
- Sünter, A.; Frorip, A.; Korsakov, V.; Kurruk, R.; Kuznetsov, A.; Ots-Rosenberg, M. Optical method for screening and a new proteinuria focus group. J. Biomed. Photonics Eng. 2015, 1, 236–247. [Google Scholar] [CrossRef] [Green Version]
- Konoplev, G.; Agafonova, D.; Bakhchova, L.; Mukhin, N.; Kurachkina, M.; Schmidt, M.-P.; Verlov, N.; Sidorov, A.; Oseev, A.; Stepanova, O.; et al. Label-Free Physical Techniques and Methodologies for Proteins Detection in Microfluidic Biosensor Structures. Biomedicines 2022, 10, 207. [Google Scholar] [CrossRef] [PubMed]
- Sünter, A.; Kuznetsov, A.; Frorip, A.; Korsakov, V.; Rosenberg, M. Optical methods, devise and statistics of determination of albumin and/or protein concentration in human urine. In Proceedings of the Saratov Fall Meeting 2015, Biophotonics Internet Invited Lecture, Saratov, Russia, 30 September 2015. [Google Scholar]
- Walls, D.; Loughran, S.T. Protein Chromatography: Methods and Protocols, 2011st ed.; Humana Press: Totowa, NJ, USA, 2011; p. 681. ISBN 9781607619123. [Google Scholar]
- Determann, H. Gel Chromatography, Gel Filtration, Gel Permeation, Molecular Sieves: A Laboratory Hand Book, 2nd ed.; Springer: New York, NY, USA, 1969; p. 208. ISBN 978-3642950841. [Google Scholar]
- GE Healthcare. Instructions 52-1308-00 BB. Available online: http://wwwuser.gwdg.de/~jgrossh/protocols/protein-purification/PD10.pdf (accessed on 18 March 2022).
- Bonomini, M.; Borras, F.E.; Troya-Saborido, M.; Carreras-Planella, L.; Di Liberato, L.; Arduini, A. Proteomic Research in Peritoneal Dialysis. Int. J. Mol. Sci. 2020, 21, 5489. [Google Scholar] [CrossRef] [PubMed]
- Di Marco, V.B.; Bombi, G.G. Mathematical functions for the representation of chromatographic peaks. J. Chromatogr. A 2001, 931, 1–30. [Google Scholar] [CrossRef]
- Buys, T.S.; De Clerk, K. Bi-Gaussian fitting of skewed peaks. Anal. Chem. 1972, 44, 1273–1275. [Google Scholar] [CrossRef]
- Lin, W.-T.; Tsai, C.-C.; Chen, C.-Y.; Lee, W.-J.; Su, C.-C.; Wu, Y.-J. Proteomic Analysis of Peritoneal Dialysate Fluid in Patients with Dialysis-Related Peritonitis. Ren. Fail. 2008, 30, 772–777. [Google Scholar] [CrossRef] [Green Version]
- Sritippayawan, S.; Chiangjong, W.; Semangoen, T.; Aiyasanon, N.; Jaetanawanitch, P.; Sinchaikul, S.; Chen, S.-T.; Vasuvattakul, S.; Thongboonkerd, V. Proteomic Analysis of Peritoneal Dialysate Fluid in Patients with Different Types of Peritoneal Membranes. J. Proteome Res. 2007, 6, 4356–4362. [Google Scholar] [CrossRef] [Green Version]
- Park, M.S.; Lee, H.A.; Chu, W.S.; Yang, D.H.; Hwang, S.D. Peritoneal accumulation of AGE and peritoneal membrane permeability. Peritoneal Dial. Int. J. Int. Soc. Perit. Dial. 2000, 20, 452–460. [Google Scholar] [CrossRef]
- Zuo, Y.; Wang, C.; Zhou, J.; Sachdeva, A.; Ruelos, V.C. Simultaneous Determination of Creatinine and Uric Acid in Human Urine by High-Performance Liquid Chromatography. Anal. Sci. 2008, 24, 1589–1592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ResearchGate. Available online: https://www.researchgate.net/post/How_many_times_can_I_use_a_PD10_column (accessed on 18 March 2022).
- Xie, X.; Wang, J.; Xiang, S.; Chen, Z.; Zhang, X.; Chen, J. Dialysate cell-free mitochondrial DNA fragments as a marker of intraperitoneal inflammation and peritoneal solute transport rate in peritoneal dialysis. BMC Nephrol. 2019, 20, 128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korabecna, M.; Pazourkova, E.; Horinek, A.; Rocinova, K.; Tesar, V. Cell-free nucleic acids as biomarkers in dialyzed patients. J. Nephrol. 2013, 26, 1001–1008. [Google Scholar] [CrossRef] [PubMed]
- Vasilevskii, A.M.; Konoplev, G.A. Using UV spectrophotometry to analyze peritoneal dialysate. J. Opt. Technol. 2004, 71, 180–182. [Google Scholar] [CrossRef]
- Vasilevsky, A.M.; Konoplyov, G.A. Peculiar character of dialyzate ultraviolet extinction spectra as an indicator of nucleic acid metabolism in humans. J. Biomed. Opt. 2005, 10, 044026. [Google Scholar] [CrossRef]
- Vasilevsky, A.M.; Gerasimchuk, R.P.; Zemchenkov, A.Y.; Konoplev, G.A.; Rubinsky, A.V.; Stepanova, O.S.; Frorip, A.A. Dual-Wavelength Optoelectronic Sensor for Monitoring Uric Acid Concentration in Dialysate. Biomed. Eng. 2015, 49, 125–128. [Google Scholar] [CrossRef]
- Lauri, K.; Tanner, R.; Jerotskaja, J.; Luman, M.; Fridolin, I. HPLC Study of Uremic Fluids Related to Optical Dialysis Adequacy Monitoring. Int. J. Artif. Organs 2010, 33, 96–104. [Google Scholar] [CrossRef]
- Kuznetsov, A.; Frorip, A.; Gerasimchuk, R.; Konoplev, G.A.; Rosenberg, M.; Sinijärv, H.; Sünter, A.; Vasilevcsky, A.; Zemchenkov, A. Multimode monitoring of AGE excretion in hemodialysis. Nephrol. Dial. Transplant. 2016, 1, 1500–1501. [Google Scholar] [CrossRef]
- Zemchenkov, G.A.; Konoplev, G.A.; Korsakov, V.; Kuznetsov, A.I.; Roshchina, N.V.; Stepanova, O.S.; Frorip, A. An Optoelectronic Spectral Sensor for Monitoring the Elimination of Uremic Markers with Low and Middle Molecular Weight during Hemodialysis Therapy. Biomed. Eng. 2022, 56, 18–23. [Google Scholar] [CrossRef]
- Steenbeke, M.; De Bruyne, S.; Van Aken, E.; Glorieux, G.; Van Biesen, W.; Himpe, J.; De Meester, G.; Speeckaert, M.; Delanghe, J. UV Fluorescence-Based Determination of Urinary Advanced Glycation End Products in Patients with Chronic Kidney Disease. Diagnostics 2020, 10, 34. [Google Scholar] [CrossRef] [Green Version]
- Henle, T.; Deppisch, R.; Beck, W.; Hergesell, O.; Hänsch, G.M.; Ritz, E. Advanced glycated end-products (AGE) during haemodialysis treatment: Discrepant results with different methodologies reflecting the heterogeneity of AGE compounds. Nephrol. Dial. Transplant. 1999, 14, 1968–1975. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papanastasiou, P.; Grass, L.; Rodela, H.; Patrikarea, A.; Oreopoulos, D.; Diamandis, E.P. Immunological quantification of advanced glycosylation end-products in the serum of patients on hemodialysis or CAPD. Kidney Int. 1994, 46, 216–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stinghen, A.E.M.; Massy, Z.A.; Vlassara, H.; Striker, G.E.; Boullier, A. Uremic Toxicity of Advanced Glycation End Products in CKD. J. Am. Soc. Nephrol. 2015, 27, 354–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, J.; Zhang, Y.; Chen, J.; Yang, X.; Mei, C.; Xiong, F.; Shi, W.; Zhou, W.; Liu, X.; Sun, S.; et al. Serum and Tissue Levels of Advanced Glycation End Products and Risk of Mortality in Patients on Maintenance Hemodialysis. Am. J. Nephrol. 2021, 52, 8–16. [Google Scholar] [CrossRef]
- Chitra, S.; Jayalakshmi, V. A Review of Healthcare Applications on Internet of Things. In Computer Networks, Big Data and IoT, 1st ed.; Pandian, A.P., Fernando, X., Islam, S.M.S., Eds.; Springer: Singapore, 2021; Volume 3, pp. 227–237. [Google Scholar] [CrossRef]
- Shetty, V.; Yamaguchi, M. Point-of-care Testing in the Time of P5 Medicine: A Preface. Sens. Mater. 2016, 28, 1141–1148. [Google Scholar] [CrossRef] [Green Version]
- Kishnani, V.; Park, S.; Nakate, U.T.; Mondal, K.; Gupta, A. Nano-functionalized paper-based IoT enabled devices for point-of-care testing: A review. Biomed. Microdevices 2022, 24, 2. [Google Scholar] [CrossRef]
- Zainol, M.F.; Mohamed Farook, R.S.; Hassan, R.; Abdul Halim, A.H.; Abdul Rejab, M.R.; Husin, Z. A New IoT Patient Monitoring System for Hemodialysis Treatment. In Proceedings of the 2019 IEEE Conference on Open Systems (ICOS), Pulau Pinang, Malaysia, 19–21 November 2019. [Google Scholar] [CrossRef]
- Nitin Prabhu, S.; Gooneratne, C.P.; Hoang, K.-A.; Mukhopadhyay, S.C. IoT-Associated Impedimetric Biosensing for Point-of-Care Monitoring of Kidney Health. IEEE Sens. J. 2021, 21, 14320–14329. [Google Scholar] [CrossRef]
- Ng, J.K.-C.; Li, P.K.-T. Fluid management and bioimpedance study in peritoneal dialysis. Curr. Opin. Nephrol. Hypertens. 2019, 28, 58–64. [Google Scholar] [CrossRef]
- Eesti Haigekassa Tervishoiuteenuste Loetelu—Riigi Teataja. Available online: https://www.riigiteataja.ee/akt/123032021022 (accessed on 18 March 2022).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient # | Protein Concentration (Lab Data), g/L | First Peak Area, a.u. | Protein Concentration (FPLC Data), g/L | Relative Error, % |
|---|---|---|---|---|
| 1 | 0.41 | 2.54 | 0.42 | 2.8 |
| 2 | 0.48 | 3.03 | 0.49 | 1.7 |
| 3 | 0.5 | 3.00 | 0.48 | 3.2 |
| 4 | 0.51 | 4.01 | 0.62 | 21.5 |
| 5 | 0.55 | 3.26 | 0.52 | 5.7 |
| 6 | 0.62 | 4.10 | 0.62 | 0.7 |
| 7 | 0.69 | 3.73 | 0.58 | 15.7 |
| 8 | 0.72 | 3.69 | 0.58 | 20.0 |
| 9 | 0.73 | 5.22 | 0.78 | 7.0 |
| 10 | 0.79 | 5.24 | 0.78 | 0.8 |
| 11 | 0.79 | 6.59 | 0.97 | 22.2 |
| 12 | 0.84 | 5.03 | 0.76 | 9.7 |
| 13 | 0.84 | 5.23 | 0.78 | 6.8 |
| 14 | 0.85 | 5.35 | 0.80 | 6.1 |
| 15 | 0.86 | 5.78 | 0.86 | 0.4 |
| 16 | 0.86 | 6.20 | 0.91 | 6.2 |
| 17 | 0.95 | 6.60 | 0.97 | 1.8 |
| 18 | 0.97 | 4.67 | 0.71 | 26.7 |
| 19 | 0.97 | 6.06 | 0.89 | 7.8 |
| 20 | 1.05 | 6.76 | 0.99 | 5.9 |
| 21 | 1.46 | 13.08 | 1.84 | 25.8 |
| 22 | 1.62 | 13.02 | 1.83 | 12.9 |
| 23 | 3.67 | 25.88 | 3.55 | 3.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuznetsov, A.; Frorip, A.; Sünter, A.; Korsakov, V.; Konoplev, G.; Stepanova, O.; Roschina, N.; Ovsyannikov, N.; Lialin, D.; Gerasimchuk, R.; et al. Optical Chemical Sensor Based on Fast-Protein Liquid Chromatography for Regular Peritoneal Protein Loss Assessment in End-Stage Renal Disease Patients on Continuous Ambulatory Peritoneal Dialysis. Chemosensors 2022, 10, 232. https://0-doi-org.brum.beds.ac.uk/10.3390/chemosensors10060232
Kuznetsov A, Frorip A, Sünter A, Korsakov V, Konoplev G, Stepanova O, Roschina N, Ovsyannikov N, Lialin D, Gerasimchuk R, et al. Optical Chemical Sensor Based on Fast-Protein Liquid Chromatography for Regular Peritoneal Protein Loss Assessment in End-Stage Renal Disease Patients on Continuous Ambulatory Peritoneal Dialysis. Chemosensors. 2022; 10(6):232. https://0-doi-org.brum.beds.ac.uk/10.3390/chemosensors10060232
Chicago/Turabian StyleKuznetsov, Artur, Aleksandr Frorip, Alar Sünter, Vadim Korsakov, Georgii Konoplev, Oksana Stepanova, Natalia Roschina, Nikolay Ovsyannikov, Daniil Lialin, Roman Gerasimchuk, and et al. 2022. "Optical Chemical Sensor Based on Fast-Protein Liquid Chromatography for Regular Peritoneal Protein Loss Assessment in End-Stage Renal Disease Patients on Continuous Ambulatory Peritoneal Dialysis" Chemosensors 10, no. 6: 232. https://0-doi-org.brum.beds.ac.uk/10.3390/chemosensors10060232