Self-Reported Physical Activity is Not a Valid Method for Measuring Physical Activity in 15-Year-Old South African Boys and Girls


Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Objectively Measured Physical Activity
2.3. Measurement of Subjective Physical Activity
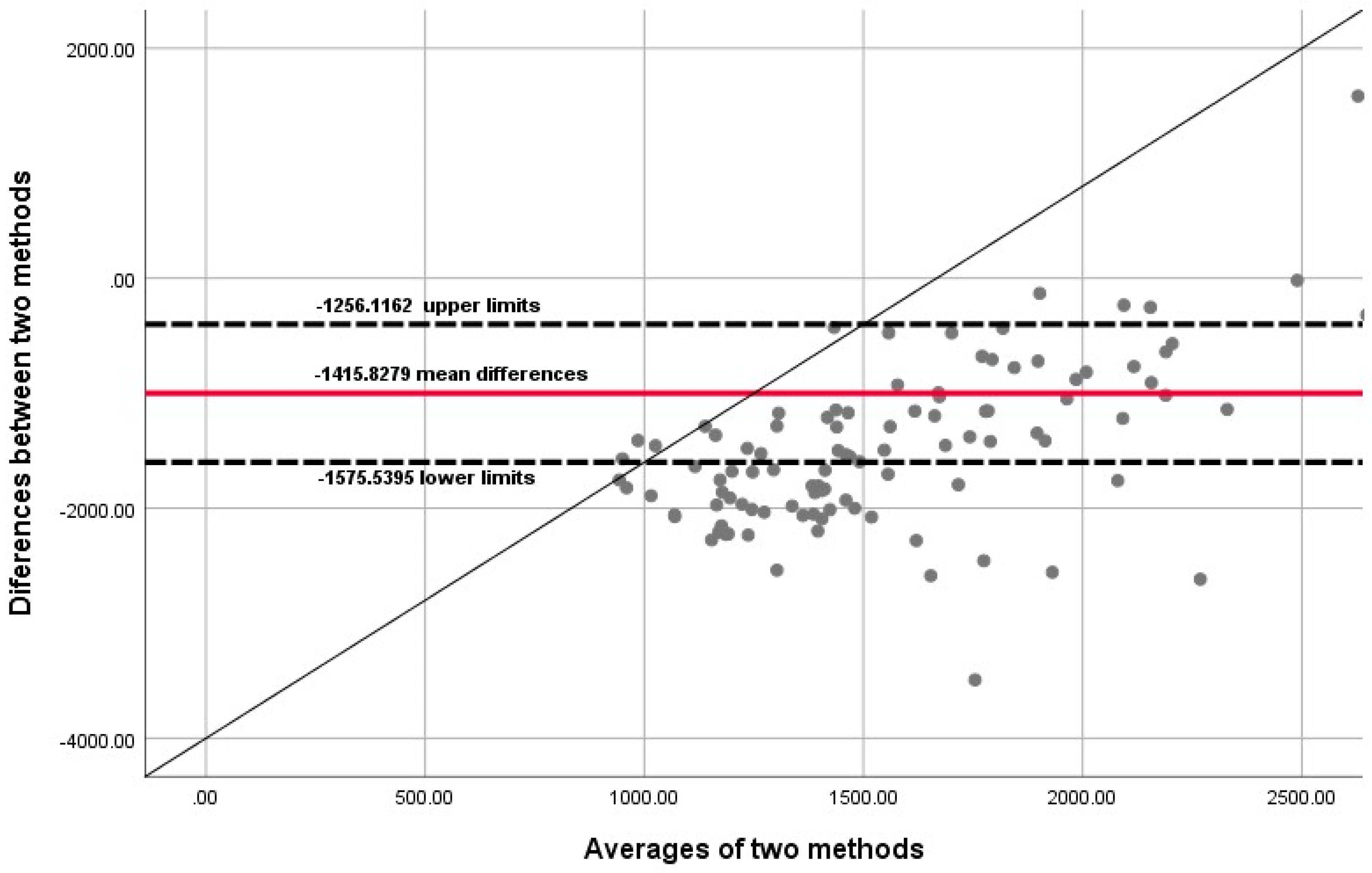
2.4. Statistical Analyses
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Disclaimer
References
- Montgomery, C.; Reilly, J.J.; Jackson, D.M.J.; Kelly, L.A.; Slater, C.; Paton, J.Y.; Grant, S. Relationship between physical activity and energy expenditure in a representative sample of young children. Am. J. Clin. Nutr. 2004, 80, 591–596. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation (WHO). Global Recommendations on Physical Activity for Health; WHO: Geneva, Switzerland, 2010. [Google Scholar]
- Haskell, W.L.; Lee, I.M.; Pate, R.R.; Powell, K.E.; Blair, S.N.; Franklin, B.A.; Macera, C.A.; Heath, G.W.; Thompson, P.D.; Bauman, A. Physical activity and public health: Updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Med. Sci. Sports Exerc. 2007, 39, 1423–1434. [Google Scholar] [CrossRef] [PubMed]
- Bonomi, A.G.; Westerterp, K.R. Advances in physical activity monitoring and lifestyle intervention in obesity: A review. Int. J. Obes. 2012, 36, 167–177. [Google Scholar] [CrossRef] [PubMed]
- Mciza, Z.J.; Goedecke, J.H.; Lambert, E.V. Validity and reliability of a physical activity/inactivity questionnaire in South African primary schoolgirls. S. Afr. J. Sports Med. 2007, 19, 117–123. [Google Scholar] [CrossRef]
- Haskell, W.L.; Blair, S.N.; Hill, J.O. Physical activity: Health outcomes and importance for public health policy. Prev. Med. 2009, 48, 280–282. [Google Scholar] [CrossRef] [PubMed]
- Montoye, H.J.; Kemper, H.C.G.; Saris, W.H.M.; Washburn, R.A. Measuring Physical Activity and Energy Expenditure; Human Kinetics: Champaign, IL, USA, 1996. [Google Scholar]
- Barreira, T.V.; Kang, M.; Caputo, J.L.; Farley, R.S.; Renfrow, M.S. Validation of the Actiheart monitor for measurement of physical activity. Int. J. Exerc. Sci. 2009, 2, 60–71. [Google Scholar]
- Loney, T.; Standage, M.; Thompson, D.; Sebire, S.J.; Cumming, S. Self-reported vs. objectively assessed physical activity: Which is right for public health? J. Phys. Act. Health 2011, 8, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Helmerhorst, H.J.F.; Brage, S.; Warren, J.; Besson, H.; Ekelund, U. A systematic review of reliability and objective criterion-related validity of physical activity questionnaires. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ainsworth, B.E. How do I measure physical activity in my patients? Questionnaires and objective methods. Br. J. Sports Med. 2009, 43, 6–9. [Google Scholar] [CrossRef] [PubMed]
- Schneller, M.B.; Pedersen, M.T.; Gupta, N.; Aadehl, M.; Holtermann, A. Validation of five minimally obstructive methods to estimate physical activity energy expenditure in young adults in semi-standardized settings. Sensors 2015, 15, 6133–6151. [Google Scholar] [CrossRef] [PubMed]
- Hills, A.P.; Mokhtar, N.; Byrne, N.M. Assessment of physical activity and energy expenditure: An overview of objective measures. Nutrition 2014, 11, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Sallis, J.F.; Saelens, B.E. Assessment of physical activity by self-report: Status, limitations, and future directions. Res. Q. Exerc. Sport 2000, 71, S1–S14. [Google Scholar] [CrossRef] [PubMed]
- Welk, G.J.; Wood, K. Physical activity assessments in physical education—A practical review of instruments and their use in the curriculum. J. Phys. Educ. Recreat. Dance 2000, 71, 30–40. [Google Scholar] [CrossRef]
- Koplan, J.P.; Liverman, C.T.; Kraak, V.I. Predicting childhood obesity: Health in the balance: Executive summary. J. Am. Diet. Assoc. 2005, 105, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Treuth, M.S.; Hou, N.Q.; Young, D.R.; Maynard, L.M. Validity and reliability of the Fels Physical Activity Questionnaire for children. Med. Sci. Sports Exerc. 2005, 37, 488–495. [Google Scholar] [CrossRef] [PubMed]
- Brage, S.; Brage, N.; Franks, P.W.; Ekelund, U.; Wareham, N.J. Reliability and validity of the combined heart rate and movement sensor Actiheart. Eur. J. Clin. Nutr. 2005, 59, 561–570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rennie, K.L.; Waren, N.J. The validation of physical activity instruments for measuring energy expenditure: Problems and pitfalls. Public Health Nutr. 1998, 1, 265–271. [Google Scholar] [CrossRef] [PubMed]
- Rangul, V.; Holmen, T.L.; Kurtze, N.; Cuypers, K.; Midthjell, K. Reliability and validity of two frequently used self-administered physical activity questionnaires in adolescents. BMC Med. Res. Methodol. 2008, 8, 47. [Google Scholar] [CrossRef] [PubMed]
- Lagerros, Y.T.; Lagiou, P. Assessment of physical activity and energy expenditure in epidemiological research of chronic diseases. Eur. J. Epidemiol. 2007, 22, 353–362. [Google Scholar] [CrossRef] [PubMed]
- Craig, C.; Marshall, A.L.; Sjostrom, L.; Bauman, A.; Booth, M.; Ainsworth, B.; Pratt, M.U.; Yngve, A.; Sallis, J. International physical questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Ainsworth, B.E.; Bassett, D.R., Jr.; Strath, S.J.; Swart, A.M.; O’Brien, W.L.; Thompson, R.W.; Jones, D.A.; Macera, C.A.; Kimsey, C.A. Comparison of three methods for measuring the time spent in physical activity. Med. Sci. Sports Exerc. 2000, 32, S457–S464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bland, J.M.; Altman, D.G. Measuring agreement in method comparison studies. Stat. Methods Med. Res. 1999, 8, 135–160. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.E.; Steindorf, K. Statistical methods for the validation of questionnaires–discrepancy between theory and practice. Methods Inf. Med. 2006, 45, 409–413. [Google Scholar] [CrossRef] [PubMed]
- Boon, R.M.; Hamlin, M.J.; Steel, G.D.; Ross, J.J. Validation of the New Zealand physical activity questionnaire (NZPAQ-LF) and the international physical activity questionnaire (IPAQ-LF) with accelerometry. Br. J. Sports Med. 2010, 44, 741–746. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.H.; Macfarlan, D.J.; Lam, T.H.; Stewart, S.M. Validity of the international physical activity questionnaire short form (IPAQ-SF): A systematic review. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shephard, R.J. Limits to the measurement of habitual physical activity by questionnaires. Br. J. Sports Med. 2003, 37, 197–206. [Google Scholar] [CrossRef] [PubMed]
- Saint-Maurice, P.F.; Welk, G. Calibration of context-specific survey items to assess youth physical activity behaviour. J. Sports Sci. 2017, 35, 866–872. [Google Scholar] [CrossRef] [PubMed]
- Welk, G.J.; Bai, Y.; Saint-Maurice, P.F.; Allums-Featherston, K.; Candelaria, N. Design and evaluation of the NFL PLAY 60 FITNESSGRAM® Partnership Project. Res. Q. Exec. Sport 2016, 87, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Celis-Morales, C.A.; Perez-Bravo, F.; Ibañez, L.; Salas, C.; Bailey, M.E.S.; Gill, J.M.R. Objective vs. Self-Reported Physical Activity and Sedentary Time: Effects of Measurement Method on Relationships with Risk Biomarkers. PLoS ONE 2012, 7, e36345. [Google Scholar] [CrossRef] [PubMed]
- Monyeki, M.A.; Neetens, R.; Moss, S.J.; Twisk, J. The relationship between body composition and physical fitness in 14 years old adolescents residing within the Tlokwe local municipality, South Africa: The PAHL study. BMC Public Health 2012, 12, 374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marfell-Jones, M.; Old, T.; Steward, A.; Carter, J.E.L. International Standards for Anthropometric Assessment; ISAK: Palmerston North, New Zealand, 2006. [Google Scholar]
- Campbell, N.; Prapavessis, H.; Gray, C. The Actiheart in Adolescents: A Doubly Labelled Water Validation. Pediatr. Exerc. Sci. 2012, 24, 589–602. [Google Scholar] [CrossRef] [PubMed]
- Department of Health and Human Services. Centers for Disease Control and Prevention (CDC): Promoting Better Health for Young People through Physical Activity and Sports; Department of Health and Human Services: Washington, DC, USA, 2009. [Google Scholar]
- World Health Organisation (WHO). Obesity and Physical Activity, Technical Report Series; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Guidelines for the Data Processing and Analysis of the International Physical Activity Questionnaire 2005. Available online: http:// www.ipaq.ki.se (accessed on 15 November 2016).
- Crouter, S.E.; Horton, M.; Bassett, D.R., Jr. Validity of ActiGraph Child-Specific Equations during Various Physical Activities. Med. Sci. Sports Exerc. 2013, 45, 1403–1409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cain, K.L.; Sallis, J.F.; Conway, T.L.; Van Dyck, D.; Calhoon, L. Using Accelerometers in Youth Physical Activity Studies: A Review of Methods. J. Phys. Act. Health 2013, 10, 437–450. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services [Internet]. Atlanta: 2008 Physical Activity Guidelines for Americans. Available online: http://www.health.gov/paguidelines (accessed on 20 February 2017).
- Dixon, P.M.; Pechmann, J.H.K. A statistical test to show negligible trend. Ecology 2005, 86, 1751–1756. [Google Scholar] [CrossRef]
- Welk, G.J. Principles of design and analyses for the calibration of accelerometry-based activity monitors. Med. Sci. Sports Exerc. 2005, 37, S501–S511. [Google Scholar] [CrossRef] [PubMed]
- Hauck, W.W.; Anderson, S. A new statistical procedure for testing equivalence in two-group comparative bioavailability trials. J. Pharmacokinet. Biopharm. 1984, 12, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.K.; Crouter, S.E.C.; Lee, J.M.; Dixon, P.M.; Gaessere, G.A.; Welk, G.J. Comparison of prediction equations for estimating energy expenditure in youth. J. Sci. Med. Sport 2016, 19, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Altman, D.G. Practical Statistics for Medical Research; Chapman & Hall/CRC Press: New York, NY, USA, 1999. [Google Scholar]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed]
- Vandoni, M.; Buzzachera, C.; Ottobrini, S.; Coreale, L.; Borrelli, P.; Berzolari, F.G.; Codrons, E. Perceived and objective measured physical activity in high school students: Is there any link between aerobic fitness, psychological responses and acute exercise? Sport Sci. Health 2016. [Google Scholar] [CrossRef]
- Assah, K.K.; Ekelund, U.; Brage, S.; Wright, A.; Mbanya, J.C.; Wareham, N.J. Accuracy and validity of a combined heart rate and motion sensor for the measurement of free-living physical activity energy expenditure in adults in Cameroon. Int. J. Epidemiol. 2011, 40, 112–120. [Google Scholar] [CrossRef] [PubMed]
- Spierer, D.; Haggins, M.; Rundle, A.; Pappas, E. A comparison of energy expenditure estimates from the Actiheart and Actical physical activity monitors during low intensity activities, walking & jogging. Eur. J. Appl. Physiol. 2011, 111, 659–667. [Google Scholar] [PubMed]
- Trost, S.G.; Way, R.; Okely, A.D. Predictive validity of three Actigraph energy expenditure equations for children. Med. Sci. Sports Exerc. 2006, 38, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Wilson, H.; Dickson, F.; Griffiths, P.; Bogin, B.; Varela-Silva, M. Logistics of using Actiheart physical activity monitor in urban Mexico among 7 to 9-year old children. Am. J. Hum. Biol. 2011, 23, 426–428. [Google Scholar] [CrossRef] [PubMed]
- Morgan, D.W. Economy of locomotion. In Paediatric Exercise Science and Medicine; Armstrong, N., van Mechelen, W., Eds.; Oxford University Press: New York, NY, USA, 2000; pp. 183–190. [Google Scholar]
- Harrell, J.S.; McMurray, R.G.; Baggett, C.D.; Pennell, M.L.; Pearce, P.F.; Bangdiwala, S.I. Energy costs of physical activities in children and adolescents. Med. Sci. Sports Exerc. 2005, 37, 329–336. [Google Scholar] [CrossRef] [PubMed]
- McCann, D.J.; Adams, W.C. The size-dependent oxygen cost of running. Med. Sci. Sports Exerc. 2003, 35, 1049–1056. [Google Scholar] [CrossRef] [PubMed]
- Bahler, C.; Bjarnason-Wehrens, B.; Schmid, J.P. SWISSPAQ: Validation of a new physical activity questionnaire in cardiac rehabilitation patients. Swiss Med. Wkly. 2013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Remoortel, H.V.; Giavedoni, S.; Raste, Y.; Burtin, C.; Louvaris, Z.; Gimeno-Santos, E.; Daniel Langer, D.; Glendenning, A.; Hopkinson, N.S.; Vogiatzis, I.; et al. Validity of activity monitors in health and chronic disease: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 84. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Min | Max | Mean | SD | p-Value of Gender | ||
|---|---|---|---|---|---|---|
| Stature (m) | Female | 142.0 | 186.0 | 157.5 | 0.07 | <0.001 |
| Male | 155.0 | 191.0 | 170.0 | 0.08 | ||
| Body Mass (kg) | Female | 33.8 | 93.0 | 55.22 | 11.08 | 0.04 |
| Male | 38.1 | 105.0 | 60.47 | 13.72 | ||
| Body Mass Index (kg/m2) | Female | 15 | 40 | 22.20 | 4.58 | 0.05 |
| Male | 14.9 | 34.0 | 20.56 | 3.63 | ||
| AEE (kCal) | Female | 258 | 1533 | 584.77 | 215.37 | <0.003 |
| Male | 181 | 878 | 462.15 | 153.30 | ||
| TPA (MET.min/week) | Female | 16.0 | 1977.0 | 704.95 | 561.94 | 0.06 |
| Male | 8.0 | 2488.5 | 941.49 | 639.45 |
| PA Level | PAL Categories (ActiHeart®) | IPAQ-SF | |||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Low PA | 100 | 93 | 26 | 24 | |
| Moderate PA | 1 | 1 | 21 | 19 | |
| Vigorous PA | 7 | 6 | 61 | 57 | |
| Total PA | 108 | 100 | 108 | 100 | |
| Symmetric Measures | |||||
| Value | Asymp. Std. Error a | Approx T b | Approx. Sig. | ||
| Measure of Agreement | κ | 0.011 | 0.008 | 1.828 | 0.068 |
| Number of Valid Cases | 108 | ||||
| N | Mean Rank | Sum of Ranks | |||
|---|---|---|---|---|---|
| Averages of two methods – Differences between two methods | Negative Ranks | 2 a | 56.00 | 112.00 | |
| Positive Ranks | 105 b | 53.96 | 5666.00 | ||
| Ties | 0 c | ||||
| Total | 108 | ||||
| Averages of two methods – Differences between two methods (i) | |||||
| Z | −8.63 (ii) | ||||
| Probability level | 0.001 | ||||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Monyeki, M.A.; Moss, S.J.; Kemper, H.C.G.; Twisk, J.W.R. Self-Reported Physical Activity is Not a Valid Method for Measuring Physical Activity in 15-Year-Old South African Boys and Girls. Children 2018, 5, 71. https://0-doi-org.brum.beds.ac.uk/10.3390/children5060071
Monyeki MA, Moss SJ, Kemper HCG, Twisk JWR. Self-Reported Physical Activity is Not a Valid Method for Measuring Physical Activity in 15-Year-Old South African Boys and Girls. Children. 2018; 5(6):71. https://0-doi-org.brum.beds.ac.uk/10.3390/children5060071
Chicago/Turabian StyleMonyeki, Makama Andries, Sarah J. Moss, Han C.G. Kemper, and Jos W.R. Twisk. 2018. "Self-Reported Physical Activity is Not a Valid Method for Measuring Physical Activity in 15-Year-Old South African Boys and Girls" Children 5, no. 6: 71. https://0-doi-org.brum.beds.ac.uk/10.3390/children5060071