Development of the Help Overcoming Pain Early (HOPE) Programme Built on a Person-Centred Approach to Support School Nurses in the Care of Adolescents with Chronic Pain—A Feasibility Study

 , , ,
, , ,
Abstract
:1. Introduction
Purpose
- developing a pain education/management programme based on an evidence-based person-centred approach and existing evidence-based stress and pain management guidelines and
- determining the feasibility of conducting an effectiveness trial of the primary outcome in terms of self-efficacy.
2. Materials and Methods
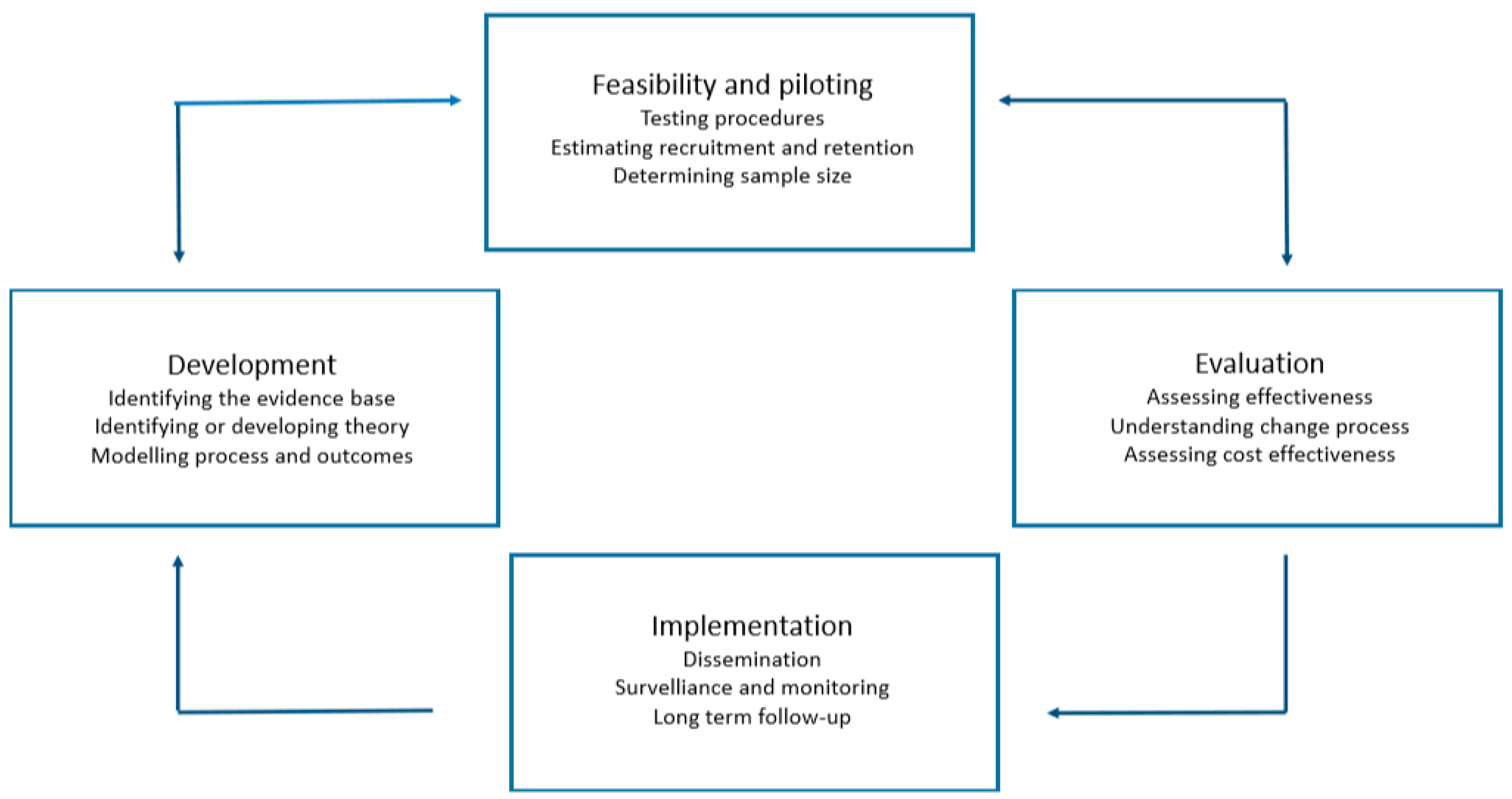
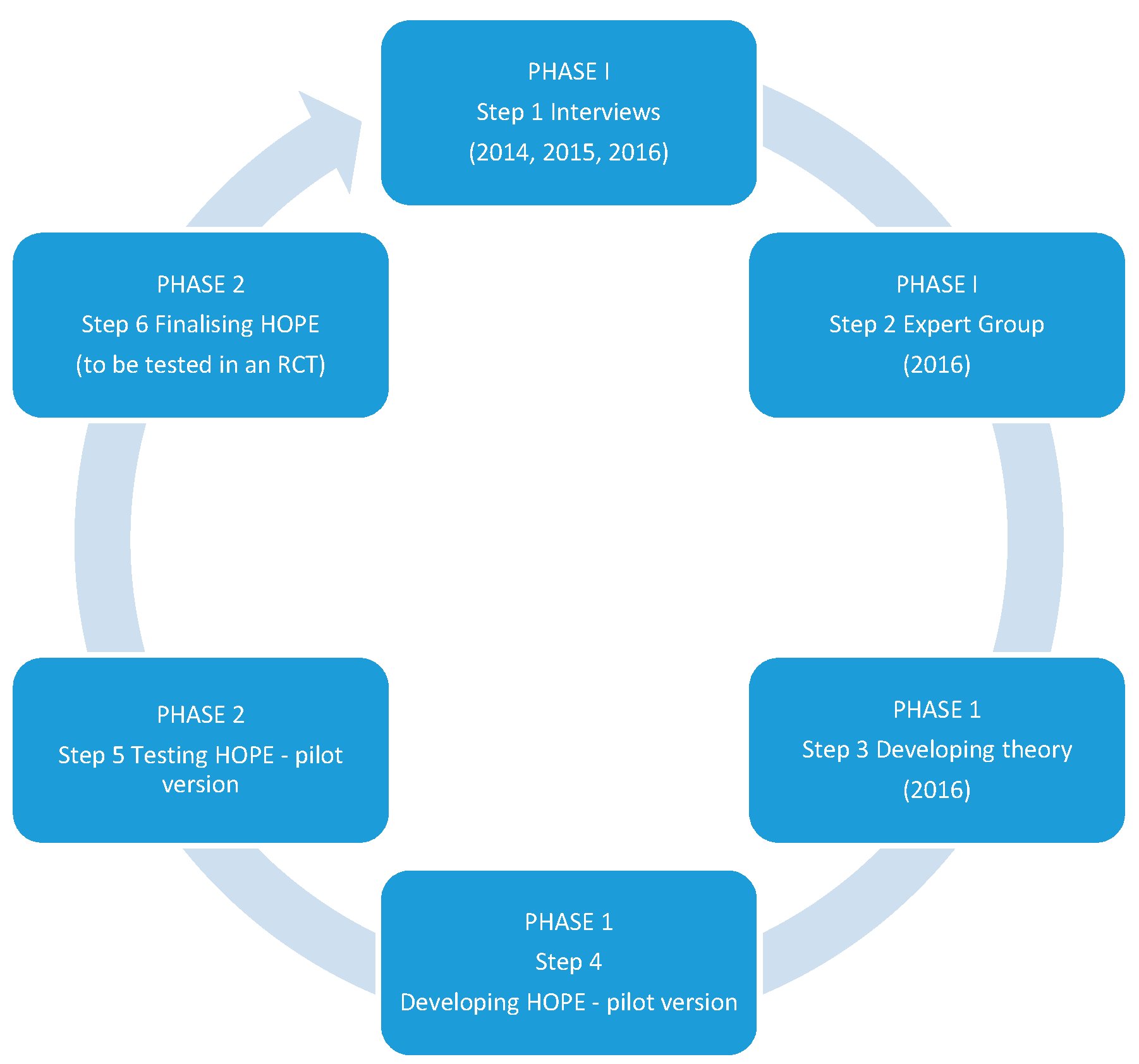
2.1. MRC Phase 1: Development
2.1.1. Identifying the Evidence-Based Practice
2.1.2. Identifying and Developing the Theory
HOPE–Person-Centred Care
HOPE–Stress and Pain Education/Management
HOPE–Gender Perspectives
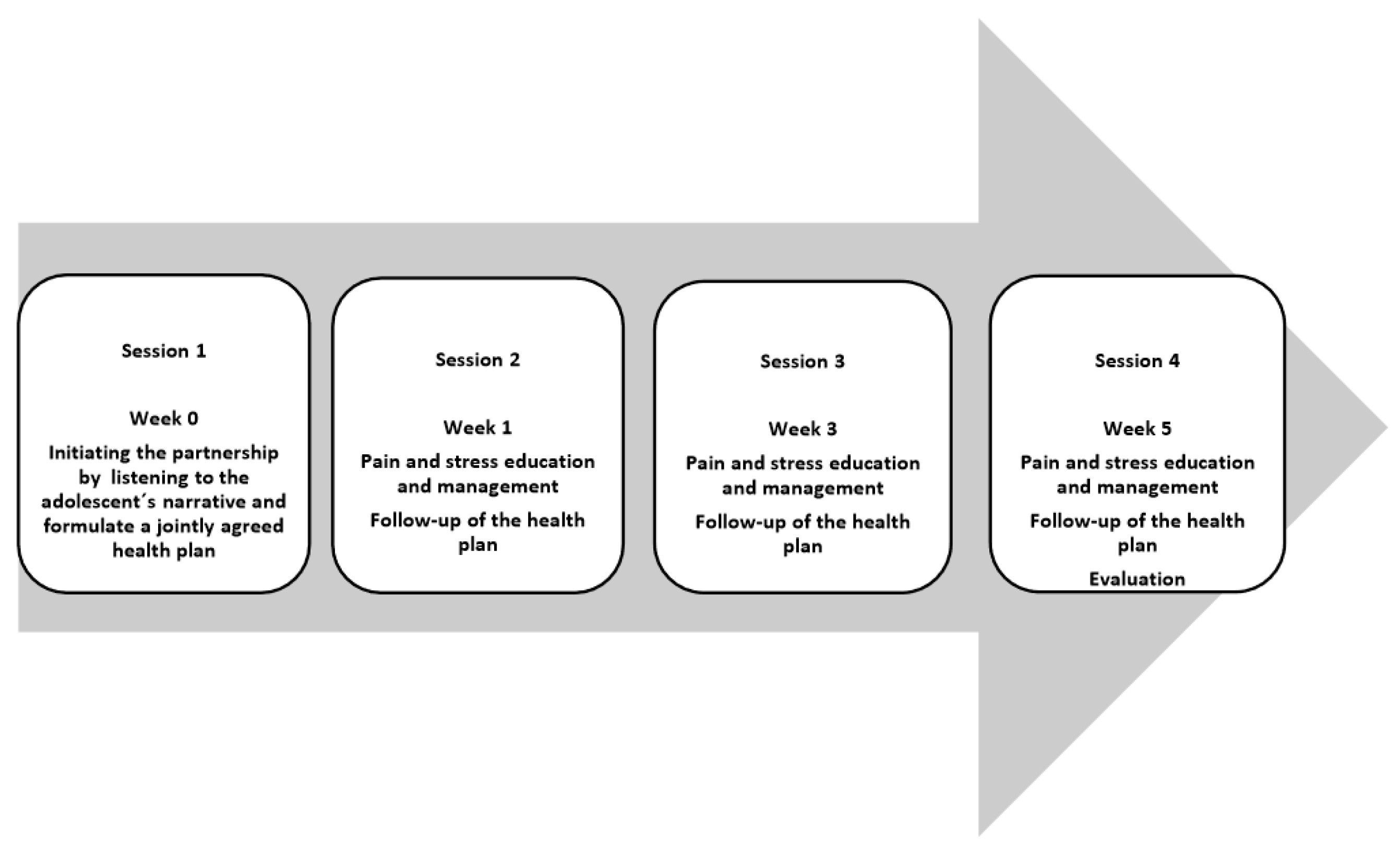
2.1.3. The HOPE Intervention
2.1.4. Modelling Process and Outcomes
Person-Centred Care
Stress and Pain Management
2.2. MRC Phase 2: Development: Feasibility and Piloting
2.2.1. Ethical Considerations
2.2.2. Testing the Feasibility of the HOPE Programme
Purpose of Testing the Feasibility
Testing a Pilot Version of the HOPE Programme
2.3. Data Analysis
3. Results
3.1. Person-Centred Care
3.2. Stress and Pain Education/Management
3.3. Gender Perspectives
3.4. The Final Version of the HOPE Programme after Cultural Adaption
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hwang, J.; Louie, P.K.; Phillips, F.M.; An, H.S.; Samartzis, D. Low back pain in children: A rising concern. Eur. Spine J. 2019, 28, 211–213. [Google Scholar] [CrossRef] [PubMed]
- Gobina, I.; Villberg, J.; Valimaa, R.; Tynjala, J.; Whitehead, R.; Cosma, A.; Brooks, F.; Cavallo, F.; Ng, K.; de Matos, M.G.; et al. Prevalence of self-reported chronic pain among adolescents: Evidence from 42 countries and regions. Eur. J. Pain 2019, 23, 316–326. [Google Scholar] [CrossRef] [PubMed]
- Shannon, R.A.; Bergren, M.D.; Matthews, A. Frequent visitors: Somatization in school-age children and implications for school nurses. J. Sch. Nurs. 2010, 26, 169–182. [Google Scholar] [CrossRef] [PubMed]
- Alfven, G.; Ostberg, V.; Hjern, A. Stressor, perceived stress and recurrent pain in swedish schoolchildren. J. Psychosom. Res. 2008, 65, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Alvarez, P.; Green, P.G.; Levine, J.D. Stress in the adult rat exacerbates muscle pain induced by early-life stress. Biol. Psychiatry 2013, 74, 688–695. [Google Scholar] [CrossRef] [PubMed]
- Hjern, A.; Alfven, G.; Ostberg, V. School stressors, psychological complaints and psychosomatic pain. Acta Paediatr. 2008, 97, 112–117. [Google Scholar] [CrossRef]
- Logan, D.E.; Simons, L.E.; Stein, M.J.; Chastain, L. School impairment in adolescents with chronic pain. J. Pain 2008, 9, 407–416. [Google Scholar] [CrossRef]
- Ragnarsson, S.; Myleus, A.; Hurtig, A.K.; Sjoberg, G.; Rosvall, P.A.; Petersen, S. Recurrent pain and academic achievement in school-aged children: A systematic review. J. Sch. Nurs. 2019. [Google Scholar] [CrossRef]
- Logan, D.E.; Gray, L.S.; Iversen, C.N.; Kim, S. School self-concept in adolescents with chronic pain. J. Pediatr. Psychol. 2017, 42, 892–901. [Google Scholar] [CrossRef]
- Logan, D.E.; Curran, J.A. Adolescent chronic pain problems in the school setting: Exploring the experiences and beliefs of selected school personnel through focus group methodology. J. Adolesc. Health 2005, 37, 281–288. [Google Scholar] [CrossRef]
- Logan, D.E.; Catanese, S.P.; Coakley, R.M.; Scharff, L. Chronic pain in the classroom: Teachers’ attributions about the causes of chronic pain. J. Sch. Health 2007, 77, 248–256. [Google Scholar] [CrossRef] [PubMed]
- Sato, A.F.; Keri, R.; Hainsworth, K.R.; Anderson Khan, K.; Ladwig, R.J.; Weisman, S.J.; Hobart Davies, W. School absenteeism in pediatric chronic pain: Identifying lessons learned from the general school absenteeism literature. Child. Healthc. 2007, 36, 355–372. [Google Scholar] [CrossRef]
- Skundberg-Kletthagen, H.; Moen, O.L. Mental health work in school health services and school nurses’ involvement and attitudes, in a norwegian context. J. Clin. Nurs. 2017, 26, 5044–5051. [Google Scholar] [CrossRef] [PubMed]
- Socialstyrelsen&Skolverket. Vägledning för elevhälsan. 2014. Available online: https://www.uppdragpsykiskhalsa.se/assets/uploads/2016/03/vagledning-for-elevhalsan.pdf (accessed on 1 July 2019).
- Skollag. 2010. Available online: https://www.riksdagen.se/sv/dokument-lagar/dokument/svensk-forfattningssamling/skollag-2010800_sfs-2010-800 (accessed on 1 July 2019).
- Institute of Medicine (US) Committee on Quality of Health Care in America. Crossing the Quality Chasm: A New Health System for the 21st Century; National Academies Press: Washington, DC, USA, 2001. [Google Scholar]
- Epping-Jordan, J.E.; Pruitt, S.D.; Bengoa, R.; Wagner, E.H. Improving the quality of health care for chronic conditions. Qual. Saf. Health Care 2004, 13, 299–305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nyborg, V.N.; Hvalvik, S.; McCormack, B. Understanding care in the past to develop caring science of the future: A historical methodological approach. Scand. J. Caring Sci. 2018, 32, 1485–1491. [Google Scholar] [CrossRef] [PubMed]
- Ekman, I. The gpcc. Eur. Heart J. 2018, 39, 495–496. [Google Scholar] [CrossRef] [PubMed]
- WHO. World Health Statistics. Available online: https://www.who.int/gho/publications/world_health_statistics/en/ (accessed on 1 July 2019).
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new medical research council guidance. BMJ 2008, 337, a1655. [Google Scholar] [CrossRef]
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new medical research council guidance. Int. J. Nurs. Stud. 2013, 50, 587–592. [Google Scholar] [CrossRef]
- Haijes, H.A.; van Thiel, G.J. Participatory methods in pediatric participatory research: A systematic review. Pediatr. Res. 2016, 79, 676–683. [Google Scholar] [CrossRef]
- Alfredsson, C.; Karlsson, J. Skolsköterskans erfarenheter av att hantera barn med psykosomatisk smärta; University of Borås: Borås, Sweden, 2014. [Google Scholar]
- Ekelund, L.; Wikander, G. Skolsköterskans betydelse vid hantering av återkommande smärta—Kvalitativ intervjustudie av ungdomars upplevelse; University of Borås: Borås, Sweden, 2014. [Google Scholar]
- Rosvall, P.-A.; Nilsson, S. Challenges of engagement with health services in sweden’s schools: Listening to the views of school nurses and students with recurrent pain. Pastoral Care Educ. 2016, 34, 3–12. [Google Scholar] [CrossRef]
- Nilsson, S.; Rosvall, P.Å.; Jonsson, A. Adolescent-centered pain management in school when adolescents have chronic pain: A qualitative study. Glob. J. Health Sci. 2017, 9, 8–19. [Google Scholar] [CrossRef]
- Alfven, G.; Grillner, S.; Andersson, E. Review of childhood pain highlights the role of negative stress. Acta Paediatr. 2019. [Google Scholar] [CrossRef] [PubMed]
- Ekman, I.; Swedberg, K.; Taft, C.; Lindseth, A.; Norberg, A.; Brink, E.; Carlsson, J.; Dahlin-Ivanoff, S.; Johansson, I.L.; Kjellgren, K.; et al. Person-centered care--ready for prime time. Eur. J. Cardiovasc. Nurs. 2011, 10, 248–251. [Google Scholar] [CrossRef] [PubMed]
- Moseley, G.L.; Butler, D.S. Fifteen years of explaining pain: The past, present, and future. J. Pain 2015, 16, 807–813. [Google Scholar] [CrossRef] [PubMed]
- Alfven, G.; Grillner, S.; Andersson, E. Children with chronic stress-induced recurrent muscle pain have enhanced startle reaction. Eur. J. Pain 2017, 21, 1561–1570. [Google Scholar] [CrossRef] [PubMed]
- Latremoliere, A.; Woolf, C.J. Central sensitization: A generator of pain hypersensitivity by central neural plasticity. J. Pain 2009, 10, 895–926. [Google Scholar] [CrossRef] [PubMed]
- Swain, M.S.; Henschke, N.; Kamper, S.J.; Gobina, I.; Ottova-Jordan, V.; Maher, C.G. An international survey of pain in adolescents. BMC Public Health 2014, 14, 447. [Google Scholar] [CrossRef] [PubMed]
- Brun Sundblad, G.M.; Saartok, T.; Engstrom, L.M. Prevalence and co-occurrence of self-rated pain and perceived health in school-children: Age and gender differences. Eur. J. Pain 2007, 11, 171–180. [Google Scholar] [CrossRef]
- Walker, S.M. Pain in children: Recent advances and ongoing challenges. Br. J. Anaesth. 2008, 101, 101–110. [Google Scholar] [CrossRef]
- Leveille, S.G.; Zhang, Y.; McMullen, W.; Kelly-Hayes, M.; Felson, D.T. Sex differences in musculoskeletal pain in older adults. Pain 2005, 116, 332–338. [Google Scholar] [CrossRef]
- Mogil, J.S. Sex differences in pain and pain inhibition: Multiple explanations of a controversial phenomenon. Nat. Rev. Neurosci. 2012, 13, 859. [Google Scholar] [CrossRef] [PubMed]
- Melchior, M.; Poisbeau, P.; Gaumond, I.; Marchand, S. Insights into the mechanisms and the emergence of sex-differences in pain. Neuroscience 2016, 338, 63–80. [Google Scholar] [CrossRef] [PubMed]
- Keogh, E. Sex and gender as social-contextual factors in pain. In Social and Interpersonal Dynamics in Pain: We Don’t Suffer alone; Vervoort, T., Karos, K., Trost, Z., Prkachin, K.M., Eds.; Springer: Cham, Switzerland, 2018; pp. 433–453. [Google Scholar]
- Odih, P. Gender and Work in Capitalist Economies; Open University Press: Berkshire, UK, 2007. [Google Scholar]
- Egger, H.L.; Costello, E.J.; Erkanli, A.; Angold, A. Somatic complaints and psychopathology in children and adolescents: Stomach aches, musculoskeletal pains, and headaches. J. Am. Acad. Child Adolesc. Psychiatry 1999, 38, 852–860. [Google Scholar] [CrossRef] [PubMed]
- Hoftun, G.B.; Romundstad, P.R.; Rygg, M. Factors associated with adolescent chronic non-specific pain, chronic multisite pain, and chronic pain with high disability: The young-hunt study 2008. J. Pain 2012, 13, 874–883. [Google Scholar] [CrossRef] [PubMed]
- Luntamo, T.; Sourander, A.; Gyllenberg, D.; Sillanmaki, L.; Aromaa, M.; Tamminen, T.; Kumpulainen, K.; Moilanen, I.; Piha, J. Do headache and abdominal pain in childhood predict suicides and severe suicide attempts? Finnish nationwide 1981 birth cohort study. Child Psychiatry Hum. Dev. 2014, 45, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Kaczynski, K.J.; Claar, R.L.; Logan, D.E. Testing gender as a moderator of associations between psychosocial variables and functional disability in children and adolescents with chronic pain. J. Pediatr. Psychol. 2009, 34, 738–748. [Google Scholar] [CrossRef] [PubMed]
- Garmy, P.; Jakobsson, U.; Carlsson, K.S.; Berg, A.; Clausson, E.K. Evaluation of a school-based program aimed at preventing depressive symptoms in adolescents. J. Sch. Nurs. 2015, 31, 117–125. [Google Scholar] [CrossRef]
- Bohman, H.; Laftman, S.B.; Cleland, N.; Lundberg, M.; Paaren, A.; Jonsson, U. Somatic symptoms in adolescence as a predictor of severe mental illness in adulthood: A long-term community-based follow-up study. Child Adolesc. Psychiatry Ment. Health 2018, 12, 42. [Google Scholar] [CrossRef]
- Rosvall, P.A.; Nilsson, S. Gender-based generalisations in school nurses’ appraisals of and interventions addressing students’ mental health. BMC Health Serv. Res. 2016, 16, 451. [Google Scholar] [CrossRef]
- Fors, A.; Ekman, I.; Taft, C.; Bjorkelund, C.; Frid, K.; Larsson, M.E.; Thorn, J.; Ulin, K.; Wolf, A.; Swedberg, K. Person-centred care after acute coronary syndrome, from hospital to primary care—A randomised controlled trial. Int. J. Cardiol. 2015, 187, 693–699. [Google Scholar] [CrossRef]
- Wager, J.; Stahlschmidt, L.; Heuer, F.; Troche, S.; Zernikow, B. The impact of a short educational movie on promoting chronic pain health literacy in school: A feasibility study. Eur. J. Pain 2018, 22, 1142–1150. [Google Scholar] [CrossRef] [PubMed]
- Birnie, K.A.; Noel, M.; Chambers, C.T.; Uman, L.S.; Parker, J.A. Psychological interventions for needle-related procedural pain and distress in children and adolescents. Cochrane Database Syst. Rev. 2018, 10, CD005179. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.C.; Wan, L.; Jamison, R.N. Using integrative medicine in pain management: An evaluation of current evidence. Anesth. Analg. 2017, 125, 2081–2093. [Google Scholar] [CrossRef] [PubMed]
- Kichline, T.; Cushing, C.C. A systematic review and quantitative analysis on the impact of aerobic exercise on pain intensity in children with chronic pain. Child. Health Care 2018, 48, 244–261. [Google Scholar] [CrossRef]
- Larsson, B.; Carlsson, J.; Fichtel, A.; Melin, L. Relaxation treatment of adolescent headache sufferers: Results from a school-based replication series. Headache 2005, 45, 692–704. [Google Scholar] [CrossRef]
- McGrath, P.J.; Walco, G.A.; Turk, D.C.; Dworkin, R.H.; Brown, M.T.; Davidson, K.; Eccleston, C.; Finley, G.A.; Goldschneider, K.; Haverkos, L.; et al. Core outcome domains and measures for pediatric acute and chronic/recurrent pain clinical trials: Pedimmpact recommendations. J. Pain 2008, 9, 771–783. [Google Scholar] [CrossRef]
- Fors, A.; Taft, C.; Ulin, K.; Ekman, I. Person-centred care improves self-efficacy to control symptoms after acute coronary syndrome: A randomized controlled trial. Eur. J. Cardiovasc. Nurs. 2016, 15, 186–194. [Google Scholar] [CrossRef]
- Fors, A.; Blanck, E.; Ali, L.; Ekberg-Jansson, A.; Fu, M.; Lindstrom Kjellberg, I.; Makitalo, A.; Swedberg, K.; Taft, C.; Ekman, I. Effects of a person-centred telephone-support in patients with chronic obstructive pulmonary disease and/or chronic heart failure—A randomized controlled trial. PLoS ONE 2018, 13, e0203031. [Google Scholar] [CrossRef]
- Holm, S.; Ljungman, G.; Asenlof, P.; Linton, S.J.; Soderlund, A. Treating youth in pain: Comparing tailored behavioural medicine treatment provided by physical therapists in primary care with physical exercises. Eur. J. Pain 2016, 20, 626–638. [Google Scholar] [CrossRef]
- Duberg, A.; Hagberg, L.; Sunvisson, H.; Moller, M. Influencing self-rated health among adolescent girls with dance intervention: A randomized controlled trial. JAMA Pediatr. 2013, 167, 27–31. [Google Scholar] [CrossRef]
- Faulstich, M.E.; Carey, M.P.; Ruggiero, L.; Enyart, P.; Gresham, F. Assessment of depression in childhood and adolescence: An evaluation of the center for epidemiological studies depression scale for children (ces-dc). Am. J. Psychiatry 1986, 143, 1024–1027. [Google Scholar] [PubMed]
- Broman, J.E.; Smedje, H.; Mallon, L.; Hetta, J. The minimal insomnia symptom scale (miss): A brief measure of sleeping difficulties. Ups J. Med. Sci. 2008, 113, 131–142. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, H.F.; Shannon, S.E. Three approaches to qualitative content analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef] [PubMed]
- Burton, C.D.; Entwistle, V.A.; Elliott, A.M.; Krucien, N.; Porteous, T.; Ryan, M. The value of different aspects of person-centred care: A series of discrete choice experiments in people with long-term conditions. BMJ Open 2017, 7, e015689. [Google Scholar] [CrossRef] [PubMed]
- Gunnarsson, K. Med önskan om kontroll—Figurationer av hälsa i skolors hälsofrämjande arbete; Stockholm University: Stockholm, Sweden, 2015. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
|
| The most dominant pain localisation |
| The second most dominant pain localisation |
| The frequency of the most dominant pain |
| Continuous pain |
| Several times a day |
| Once a day |
| Several hours each time |
| Several times a month |
| Once a month |
| The duration of the most dominant pain |
| Continuous pain |
| Several days each time |
| Several times a week |
| Approximately one hour each time |
| Several minutes each time |
| The intensity of the most dominant pain (0–10) |
| To what extent does all the pain influence you? |
| Not at all |
| Pretty much |
| Little |
| A lot |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nilsson, S.; Wallbing, U.; Alfvén, G.; Dalenius, K.; Fors, A.; Golsäter, M.; Rosvall, P.-Å.; Wigert, H.; Lundberg, M. Development of the Help Overcoming Pain Early (HOPE) Programme Built on a Person-Centred Approach to Support School Nurses in the Care of Adolescents with Chronic Pain—A Feasibility Study. Children 2019, 6, 95. https://0-doi-org.brum.beds.ac.uk/10.3390/children6090095
Nilsson S, Wallbing U, Alfvén G, Dalenius K, Fors A, Golsäter M, Rosvall P-Å, Wigert H, Lundberg M. Development of the Help Overcoming Pain Early (HOPE) Programme Built on a Person-Centred Approach to Support School Nurses in the Care of Adolescents with Chronic Pain—A Feasibility Study. Children. 2019; 6(9):95. https://0-doi-org.brum.beds.ac.uk/10.3390/children6090095
Chicago/Turabian StyleNilsson, Stefan, Ulrika Wallbing, Gösta Alfvén, Kristina Dalenius, Andreas Fors, Marie Golsäter, Per-Åke Rosvall, Helena Wigert, and Mari Lundberg. 2019. "Development of the Help Overcoming Pain Early (HOPE) Programme Built on a Person-Centred Approach to Support School Nurses in the Care of Adolescents with Chronic Pain—A Feasibility Study" Children 6, no. 9: 95. https://0-doi-org.brum.beds.ac.uk/10.3390/children6090095