A Psychosocial Intervention’s Impact on Quality of Life in AYAs with Cancer: A Post Hoc Analysis from the Promoting Resilience in Stress Management (PRISM) Randomized Controlled Trial

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design, Setting, and Participants:
2.2. Recruitment and Randomization:
2.3. Intervention:
2.4. Procedures:
2.5. Patient-Reported Outcomes:
2.6. Study Outcomes:
2.7. Statistical Analyses:
3. Results
3.1. Generic Quality of Life
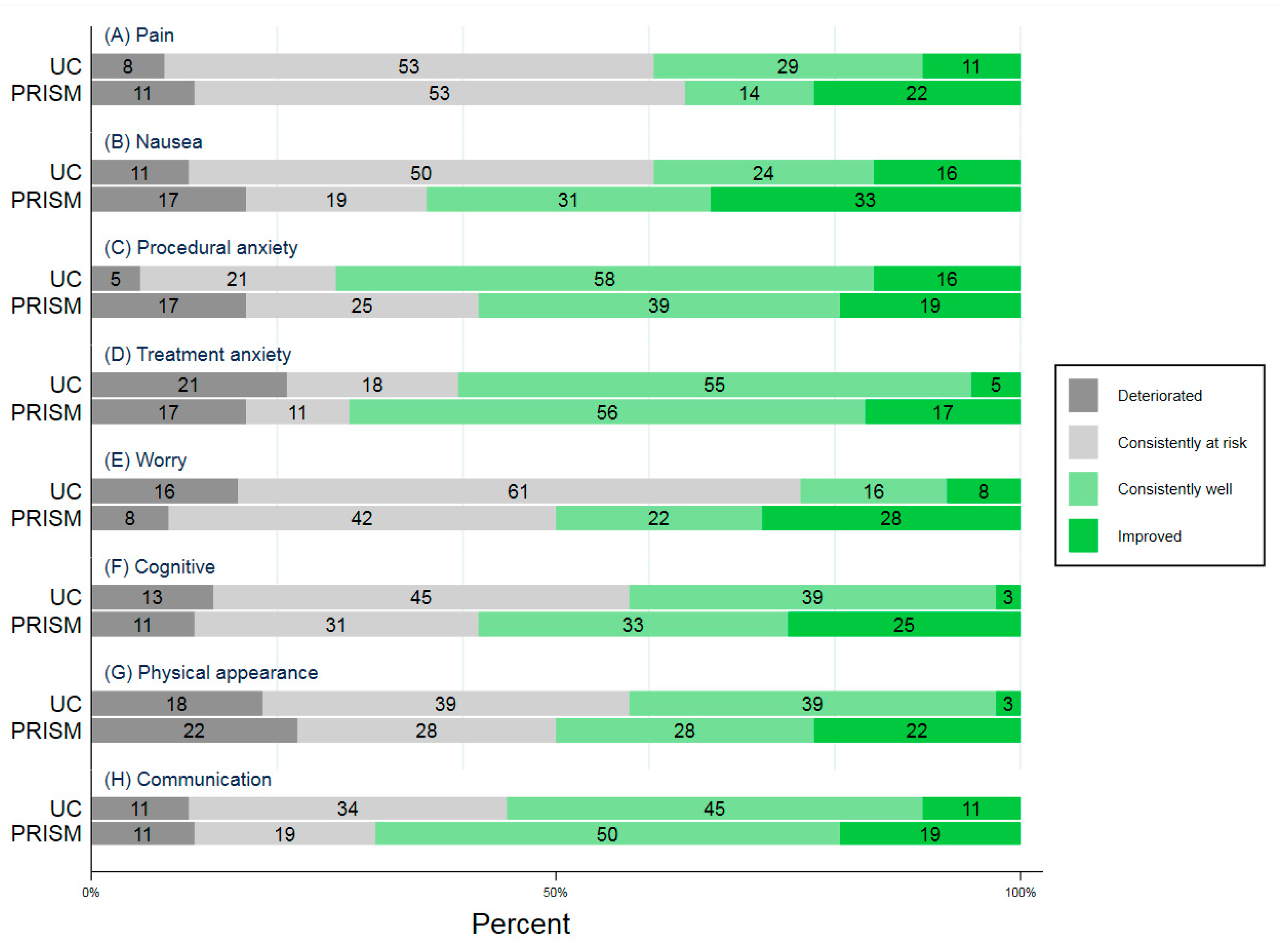
3.2. Cancer-Specific Quality of Life
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Varni, J.W.; Burwinkle, T.M.; Katz, E.R.; Meeske, K.; Dickinson, P. The PedsQL in pediatric cancer: Reliability and validity of the Pediatric Quality of Life Inventory Generic Core Scales, Multidimensional Fatigue Scale, and Cancer Module. Cancer 2002, 94, 2090–2106. [Google Scholar] [CrossRef] [PubMed]
- Dobrozsi, S.; Yan, K.; Hoffmann, R.; Panepinto, J. Patient-reported health status during pediatric cancer treatment. Pediatr. Blood Cancer 2017, 64, e26295. [Google Scholar] [CrossRef] [PubMed]
- Cheng, K.K.; Yeung, R.M. Impact of mood disturbance, sleep disturbance, fatigue and pain among patients receiving cancer therapy. Eur. J. Cancer Care 2013, 22, 70–78. [Google Scholar] [CrossRef] [PubMed]
- Nathan, P.C.; Ness, K.K.; Greenberg, M.L.; Hudson, M.; Wolden, S.; Davidoff, A.; Laverdiere, C.; Mertens, A.; Whitton, J.; Robison, L.L.; et al. Health-related quality of life in adult survivors of childhood Wilms tumor or neuroblastoma: A report from the childhood cancer survivor study. Pediatr. Blood Cancer 2007, 49, 704–715. [Google Scholar] [CrossRef]
- Zebrack, B.J.; Landier, W. The perceived impact of cancer on quality of life for post-treatment survivors of childhood cancer. Qual. Life Res. 2011, 20, 1595–1608. [Google Scholar] [CrossRef]
- Badawy, S.M.; Thompson, A.A.; Lai, J.S.; Penedo, F.J.; Rychlik, K.; Liem, R.I. Adherence to hydroxyurea, health-related quality of life domains, and patients’ perceptions of sickle cell disease and hydroxyurea: A cross-sectional study in adolescents and young adults. Health Qual. Life Outcomes 2017, 15, 136. [Google Scholar] [CrossRef]
- Cheville, A.L.; Alberts, S.R.; Rummans, T.A.; Basford, J.R.; Lapid, M.I.; Sloan, J.A.; Satele, D.V.; Clark, M.M. Improving Adherence to Cancer Treatment by Addressing Quality of Life in Patients with Advanced Gastrointestinal Cancers. J. Pain Symptom Manag. 2015, 50, 321–327. [Google Scholar] [CrossRef]
- Miller, K.A.; Wojcik, K.Y.; Ramirez, C.N.; Ritt-Olson, A.; Freyer, D.R.; Hamilton, A.S.; Milam, J.E. Supporting long-term follow-up of young adult survivors of childhood cancer: Correlates of healthcare self-efficacy. Pediatr. Blood Cancer 2017, 64, 358–363. [Google Scholar] [CrossRef]
- Warner, E.L.; Nam, G.E.; Zhang, Y.; McFadden, M.; Wright, J.; Spraker-Perlman, H.; Kinney, A.Y.; Oeffinger, K.C.; Kirchhoff, A.C. Health behaviors, quality of life, and psychosocial health among survivors of adolescent and young adult cancers. J. Cancer Surviv. 2016, 10, 280–290. [Google Scholar] [CrossRef]
- Kazak, A.E.; Derosa, B.W.; Schwartz, L.A.; Hobbie, W.; Carlson, C.; Ittenbach, R.F.; Mao, J.J.; Ginsberg, J.P. Psychological outcomes and health beliefs in adolescent and young adult survivors of childhood cancer and controls. J. Clin. Oncol. 2010, 28, 2002–2007. [Google Scholar] [CrossRef]
- Dimeo, F.; Schmittel, A.; Fietz, T.; Schwartz, S.; Kohler, P.; Boning, D.; Thiel, E. Physical performance, depression, immune status and fatigue in patients with hematological malignancies after treatment. Ann. Oncol. 2004, 15, 1237–1242. [Google Scholar] [CrossRef] [PubMed]
- Ness, K.K.; Bhatia, S.; Baker, K.S.; Francisco, L.; Carter, A.; Forman, S.J.; Robison, L.L.; Rosenthal, J.; Gurney, J.G. Performance limitations and participation restrictions among childhood cancer survivors treated with hematopoietic stem cell transplantation: The bone marrow transplant survivor study. Arch. Pediatr. Adolesc. Med. 2005, 159, 706–713. [Google Scholar] [CrossRef] [PubMed]
- Ness, K.K.; Mertens, A.C.; Hudson, M.M.; Wall, M.M.; Leisenring, W.M.; Oeffinger, K.C.; Sklar, C.A.; Robison, L.L.; Gurney, J.G. Limitations on physical performance and daily activities among long-term survivors of childhood cancer. Ann. Intern. Med. 2005, 143, 639–647. [Google Scholar] [CrossRef] [PubMed]
- Ness, K.K.; Gurney, J.G.; Zeltzer, L.K.; Leisenring, W.; Mulrooney, D.A.; Nathan, P.C.; Robison, L.L.; Mertens, A.C. The impact of limitations in physical, executive, and emotional function on health-related quality of life among adult survivors of childhood cancer: A report from the Childhood Cancer Survivor Study. Arch. Phys. Med. Rehabil. 2008, 89, 128–136. [Google Scholar] [CrossRef] [PubMed]
- Zebrack, B.J.; Gurney, J.G.; Oeffinger, K.; Whitton, J.; Packer, R.J.; Mertens, A.; Turk, N.; Castleberry, R.; Dreyer, Z.; Robison, L.L.; et al. Psychological outcomes in long-term survivors of childhood brain cancer: A report from the childhood cancer survivor study. J. Clin. Oncol. 2004, 22, 999–1006. [Google Scholar] [CrossRef]
- Janson, C.; Leisenring, W.; Cox, C.; Termuhlen, A.M.; Mertens, A.C.; Whitton, J.A.; Goodman, P.; Zeltzer, L.; Robison, L.L.; Krull, K.R.; et al. Predictors of marriage and divorce in adult survivors of childhood cancers: A report from the Childhood Cancer Survivor Study. Cancer Epidemiol. Prev. Biomark. 2009, 18, 2626–2635. [Google Scholar] [CrossRef]
- Nagarajan, R.; Neglia, J.P.; Clohisy, D.R.; Yasui, Y.; Greenberg, M.; Hudson, M.; Zevon, M.A.; Tersak, J.M.; Ablin, A.; Robison, L.L. Education, employment, insurance, and marital status among 694 survivors of pediatric lower extremity bone tumors: A report from the childhood cancer survivor study. Cancer 2003, 97, 2554–2564. [Google Scholar] [CrossRef]
- Mitby, P.A.; Robison, L.L.; Whitton, J.A.; Zevon, M.A.; Gibbs, I.C.; Tersak, J.M.; Meadows, A.T.; Stovall, M.; Zeltzer, L.K.; Mertens, A.C.; et al. Utilization of special education services and educational attainment among long-term survivors of childhood cancer: A report from the Childhood Cancer Survivor Study. Cancer 2003, 97, 1115–1126. [Google Scholar] [CrossRef]
- Guy, G.P., Jr.; Yabroff, K.R.; Ekwueme, D.U.; Smith, A.W.; Dowling, E.C.; Rechis, R.; Nutt, S.; Richardson, L.C. Estimating the health and economic burden of cancer among those diagnosed as adolescents and young adults. Health Aff. 2014, 33, 1024–1031. [Google Scholar] [CrossRef]
- Guy, G.P., Jr.; Yabroff, K.R.; Ekwueme, D.U.; Rim, S.H.; Li, R.; Richardson, L.C. Economic Burden of Chronic Conditions Among Survivors of Cancer in the United States. J. Clin. Oncol. 2017, 35, 2053–2061. [Google Scholar] [CrossRef]
- Zebrack, B.J. Psychological, social, and behavioral issues for young adults with cancer. Cancer 2011, 117, 2289–2294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walker, E.; Martins, A.; Aldiss, S.; Gibson, F.; Taylor, R.M. Psychosocial Interventions for Adolescents and Young Adults Diagnosed with Cancer During Adolescence: A Critical Review. J. Adolesc. Young Adult Oncol. 2016, 5, 310–321. [Google Scholar] [CrossRef] [PubMed]
- Kato, P.M.; Cole, S.W.; Bradlyn, A.S.; Pollock, B.H. A video game improves behavioral outcomes in adolescents and young adults with cancer: A randomized trial. Pediatrics 2008, 122, e305–e317. [Google Scholar] [CrossRef] [PubMed]
- Jones, J.K.; Kamani, S.A.; Bush, P.J.; Hennessy, K.A.; Marfatia, A.; Shad, A.T. Development and evaluation of an educational interactive CD-ROM for teens with cancer. Pediatr. Blood Cancer 2010, 55, 512–519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robb, S.L.; Burns, D.S.; Stegenga, K.A.; Haut, P.R.; Monahan, P.O.; Meza, J.; Stump, T.E.; Cherven, B.O.; Docherty, S.L.; Hendricks-Ferguson, V.L.; et al. Randomized clinical trial of therapeutic music video intervention for resilience outcomes in adolescents/young adults undergoing hematopoietic stem cell transplant: A report from the Children’s Oncology Group. Cancer 2014, 120, 909–917. [Google Scholar] [CrossRef]
- Schwartz, C.E.; Feinberg, R.G.; Jilinskaia, E.; Applegate, J.C. An evaluation of a psychosocial intervention for survivors of childhood cancer: Paradoxical effects of response shift over time. Psychooncology 1999, 8, 344–354. [Google Scholar] [CrossRef]
- Sansom-Daly, U.M.; Wakefield, C.E.; Bryant, R.A.; Patterson, P.; Anazodo, A.; Butow, P.; Sawyer, S.M.; McGill, B.C.; Evans, H.E.; Cohn, R.J.; et al. Feasibility, acceptability, and safety of the Recapture Life videoconferencing intervention for adolescent and young adult cancer survivors. Psychooncology 2018, 28, 284–292. [Google Scholar] [CrossRef]
- Haase, J.E. The adolescent resilience model as a guide to interventions. J. Pediatr. Oncol. Nurs. 2004, 21, 289–299. [Google Scholar] [CrossRef]
- Carver, C.S. Enhancing adaptation during treatment and the role of individual differences. Cancer 2005, 104, 2602–2607. [Google Scholar] [CrossRef]
- Van der Lee, M.L.; Garssen, B. Mindfulness-based cognitive therapy reduces chronic cancer-related fatigue: A treatment study. Psychooncology 2012, 21, 264–272. [Google Scholar] [CrossRef]
- Compen, F.; Bisseling, E.; Schellekens, M.; Donders, R.; Carlson, L.; van der Lee, M.; Speckens, A. Face-to-Face and Internet-Based Mindfulness-Based Cognitive Therapy Compared with Treatment as Usual in Reducing Psychological Distress in Patients with Cancer: A Multicenter Randomized Controlled Trial. J. Clin. Oncol. 2018, 36, 2413–2421. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, A.R.; Yi-Frazier, J.P.; Eaton, L.; Wharton, C.; Cochrane, K.; Pihoker, C.; Baker, K.S.; McCauley, E. Promoting Resilience in Stress Management: A Pilot Study of a Novel Resilience-Promoting Intervention for Adolescents and Young Adults with Serious Illness. J. Pediatr. Psychol. 2015, 40, 992–999. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, A.R.; Bradford, M.C.; McCauley, E.; Curtis, J.R.; Wolfe, J.; Baker, K.S.; Yi-Frazier, J.P. Promoting Resilience in Adolescents and Young Adults with Cancer: Results from the PRISM Randomized Controlled Trial. Cancer 2018, 124, 3909–3917. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, A.R.; Bradford, M.C.; Barton, K.S.; Etsekson, N.; McCauley, E.; Curtis, J.R.; Wolfe, J.; Baker, K.S.; Yi-Frazier, J.P. Hope and benefit finding: Results from the PRISM randomized controlled trial. Pediatr. Blood Cancer 2019, 66, e27485. [Google Scholar] [CrossRef]
- Hinds, P.S.; Gattuso, J.S.; Billups, C.A.; West, N.K.; Wu, J.; Rivera, C.; Quintana, J.; Villarroel, M.; Daw, N.C. Aggressive treatment of non-metastatic osteosarcoma improves health-related quality of life in children and adolescents. Eur. J. Cancer 2009, 45, 2007–2014. [Google Scholar] [CrossRef] [Green Version]
- Varni, J.W.; Seid, M.; Kurtin, P.S. PedsQL 4.0: Reliability and validity of the Pediatric Quality of Life Inventory version 4.0 generic core scales in healthy and patient populations. Med. Care 2001, 39, 800–812. [Google Scholar] [CrossRef]
- Varni, J.W.; Limbers, C.A. The PedsQL 4.0 Generic Core Scales Young Adult Version: Feasibility, reliability and validity in a university student population. J. Health Psychol. 2009, 14, 611–622. [Google Scholar] [CrossRef]
- Chan, K.S.; Mangione-Smith, R.; Burwinkle, T.M.; Rosen, M.; Varni, J.W. The PedsQL: Reliability and validity of the short-form generic core scales and Asthma Module. Med. Care 2005, 43, 256–265. [Google Scholar] [CrossRef]
- Varni, J.W.; Burwinkle, T.M.; Seid, M.; Skarr, D. The PedsQL 4.0 as a pediatric population health measure: Feasibility, reliability, and validity. Ambul. Pediatr. 2003, 3, 329–341. [Google Scholar] [CrossRef]
- Varni, J.W.; Limbers, C.; Burwinkle, T.M. Literature review: Health-related quality of life measurement in pediatric oncology: Hearing the voices of the children. J. Pediatr. Psychol. 2007, 32, 1151–1163. [Google Scholar] [CrossRef]
- Rosenberg, A.R.; Orellana, L.; Ullrich, C.; Kang, T.; Geyer, J.R.; Feudtner, C.; Dussel, V.; Wolfe, J. Quality of Life in Children with Advanced Cancer: A Report from the PediQUEST Study. J. Pain Symptom Manag. 2016, 52, 243–253. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, H.R.; Lu, X.; Myers, R.M.; Sung, L.; Balsamo, L.M.; Carroll, W.L.; Raetz, E.; Loh, M.L.; Mattano, L.A., Jr.; Winick, N.J.; et al. Prospective, longitudinal assessment of quality of life in children from diagnosis to 3 months off treatment for standard risk acute lymphoblastic leukemia: Results of Children’s Oncology Group study AALL0331. Int. J. Cancer 2016, 138, 332–339. [Google Scholar] [CrossRef] [PubMed]
- Kwak, M.; Zebrack, B.J.; Meeske, K.A.; Embry, L.; Aguilar, C.; Block, R.; Hayes-Lattin, B.; Li, Y.; Butler, M.; Cole, S. Trajectories of psychological distress in adolescent and young adult patients with cancer: A 1-year longitudinal study. J. Clin. Oncol. 2013, 31, 2160–2166. [Google Scholar] [CrossRef] [PubMed]
- Cebolla, A.; Demarzo, M.; Martins, P.; Soler, J.; Garcia-Campayo, J. Unwanted effects: Is there a negative side of meditation? A multicentre survey. PLoS ONE 2016, 12, e0183137. [Google Scholar] [CrossRef] [PubMed]
- Baer, R.; Crane, C.; Miller, E.; Kuyken, W. Doing no harm in mindfulness-based programs: Conceptual issues and empirical findings. Clin. Psychol. Rev. 2019, 71, 101–114. [Google Scholar] [CrossRef]
- Kaal, S.E.J.; Husson, O.; van Duivenboden, S.; Jansen, R.; Manten-Horst, E.; Servaes, P.; Prins, J.B.; van den Berg, S.W.; van der Graaf, W.T.A. Empowerment in adolescents and young adults with cancer: Relationship with health-related quality of life. Cancer 2017, 123, 4039–4047. [Google Scholar] [CrossRef]
- Lorgelly, P.K.; Doble, B.; Rowen, D.; Brazier, J.; Cancer, I. Condition-specific or generic preference-based measures in oncology? A comparison of the EORTC-8D and the EQ-5D-3L. Qual. Life Res. 2017, 26, 1163–1176. [Google Scholar] [CrossRef]
- Teckle, P.; Peacock, S.; McTaggart-Cowan, H.; van der Hoek, K.; Chia, S.; Melosky, B.; Gelmon, K. The ability of cancer-specific and generic preference-based instruments to discriminate across clinical and self-reported measures of cancer severities. Health Qual. Life Outcomes 2011, 9, 106. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| At Baseline | At 6 Months | |||||
|---|---|---|---|---|---|---|
| Characteristic | Usual Care (n = 44) | PRISM (n = 48) | All (n = 92) | Usual Care (n = 38) | PRISM (n = 36) | All (n = 74) |
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | |
| Female | 24 (55) | 16 (33) | 40 (43) | 21 (55) | 12 (33) | 33 (45) |
| 12–17 years-old at enrollment | 32 (73) | 35 (73) | 67 (73) | 26 (68) | 27 (75) | 53 (72) |
| 18–25 years-old at enrollment | 12 (27) | 13 (27) | 25 (27) | 12 (32) | 9 (25) | 21 (28) |
| Non-White Race | 19 (43) | 15 (31) | 33 (36) | 17 (45) | 9 (25) | 26 (35) |
| Non-English First language | 10 (23) | 1 (2) | 11 (12) | 9 (24) | 3 (8) | 12 (16) |
| Leukemia/Lymphoma | 29 (66) | 31 (65) | 60 (65) | 25 (66) | 23 (66) | 48 (66) |
| Advanced Cancer at Enrollment | 14 (32) | 10 (21) | 24 (26) | 11 (29) | 6 (17) | 17 (23) |
| UC | PRISM | ||||
|---|---|---|---|---|---|
| Percent | 95% CI | Percent | 95% CI | P from Chi-Squared Test | |
| SF-15 | |||||
| Global | 26 | 15–42 | 47 | 32–63 | 0.06 |
| Physical | 34 | 21–50 | 36 | 22–52 | 0.86 |
| Emotional | 37 | 23–53 | 58 | 42–73 | 0.06 |
| Social | 66 | 50–79 | 83 | 68–92 | 0.08 |
| School | 34 | 21–50 | 44 | 30–60 | 0.37 |
| Cancer Module | |||||
| Pain | 39 | 26–55 | 36 | 22–52 | 0.77 |
| Nausea | 39 | 26–55 | 64 | 48–78 | 0.04 |
| Procedural anxiety | 74 | 58–85 | 58 | 42–73 | 0.16 |
| Treatment anxiety | 61 | 45–74 | 72 | 56–84 | 0.29 |
| Worry | 24 | 13–39 | 50 | 34–66 | 0.02 |
| Cognitive | 42 | 28–58 | 58 | 42–73 | 0.16 |
| Physical appearance | 42 | 28–58 | 50 | 34–66 | 0.50 |
| Communication | 55 | 40–70 | 69 | 53–82 | 0.21 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Steineck, A.; Bradford, M.C.; Lau, N.; Scott, S.; Yi-Frazier, J.P.; Rosenberg, A.R. A Psychosocial Intervention’s Impact on Quality of Life in AYAs with Cancer: A Post Hoc Analysis from the Promoting Resilience in Stress Management (PRISM) Randomized Controlled Trial. Children 2019, 6, 124. https://0-doi-org.brum.beds.ac.uk/10.3390/children6110124
Steineck A, Bradford MC, Lau N, Scott S, Yi-Frazier JP, Rosenberg AR. A Psychosocial Intervention’s Impact on Quality of Life in AYAs with Cancer: A Post Hoc Analysis from the Promoting Resilience in Stress Management (PRISM) Randomized Controlled Trial. Children. 2019; 6(11):124. https://0-doi-org.brum.beds.ac.uk/10.3390/children6110124
Chicago/Turabian StyleSteineck, Angela, Miranda C. Bradford, Nancy Lau, Samantha Scott, Joyce P. Yi-Frazier, and Abby R. Rosenberg. 2019. "A Psychosocial Intervention’s Impact on Quality of Life in AYAs with Cancer: A Post Hoc Analysis from the Promoting Resilience in Stress Management (PRISM) Randomized Controlled Trial" Children 6, no. 11: 124. https://0-doi-org.brum.beds.ac.uk/10.3390/children6110124