Motor Performance in Children Diagnosed with Cancer: A Longitudinal Observational Study

 , , , and
, , , and
Abstract
:1. Introduction
2. Subjects and Methods
2.1. The Research Questions
- (1)
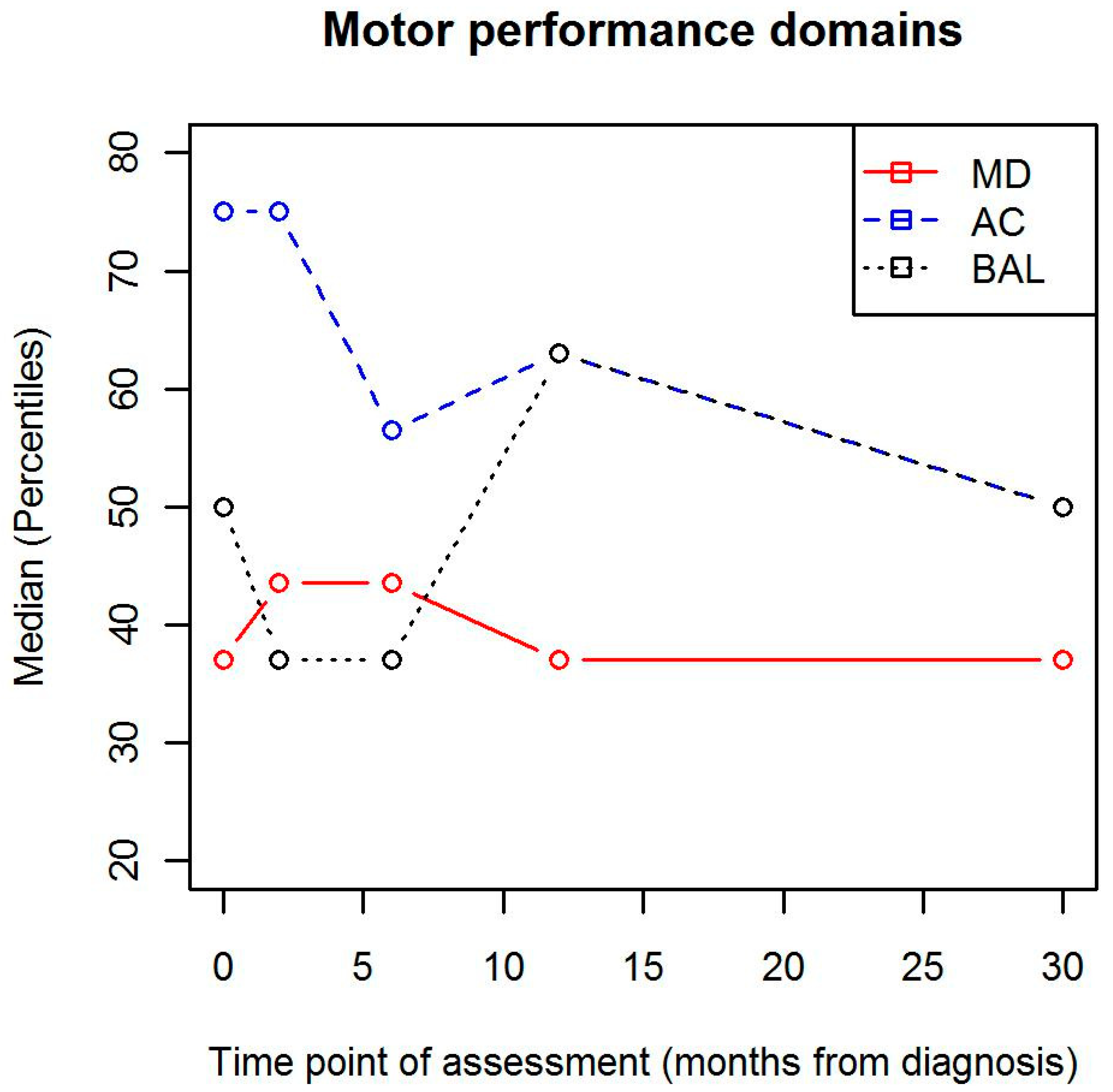
- How does motor performance change within its different domains from the beginning of the treatment to 2, 6, 12 and 30 months from the diagnoses?
- (2)
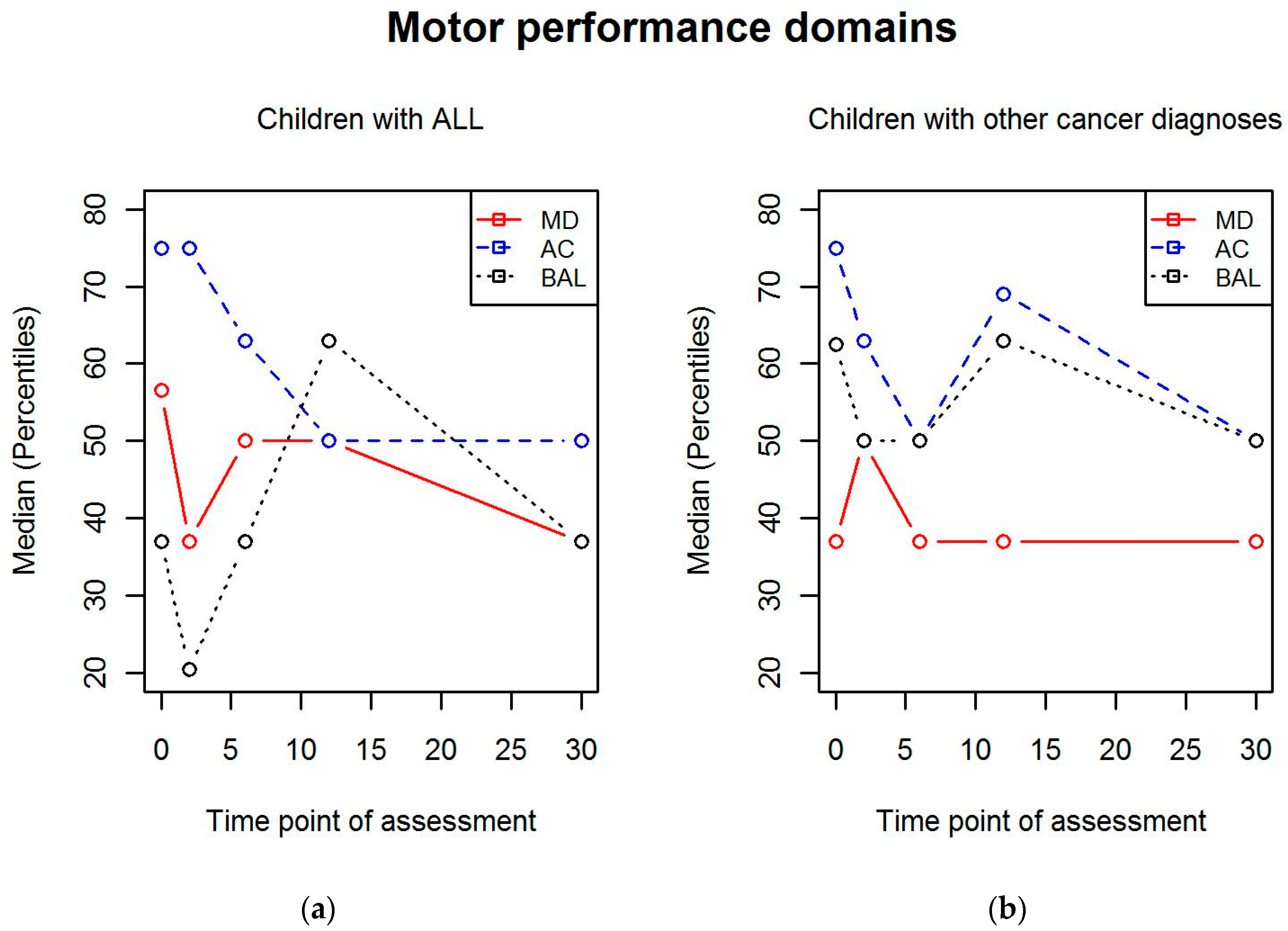
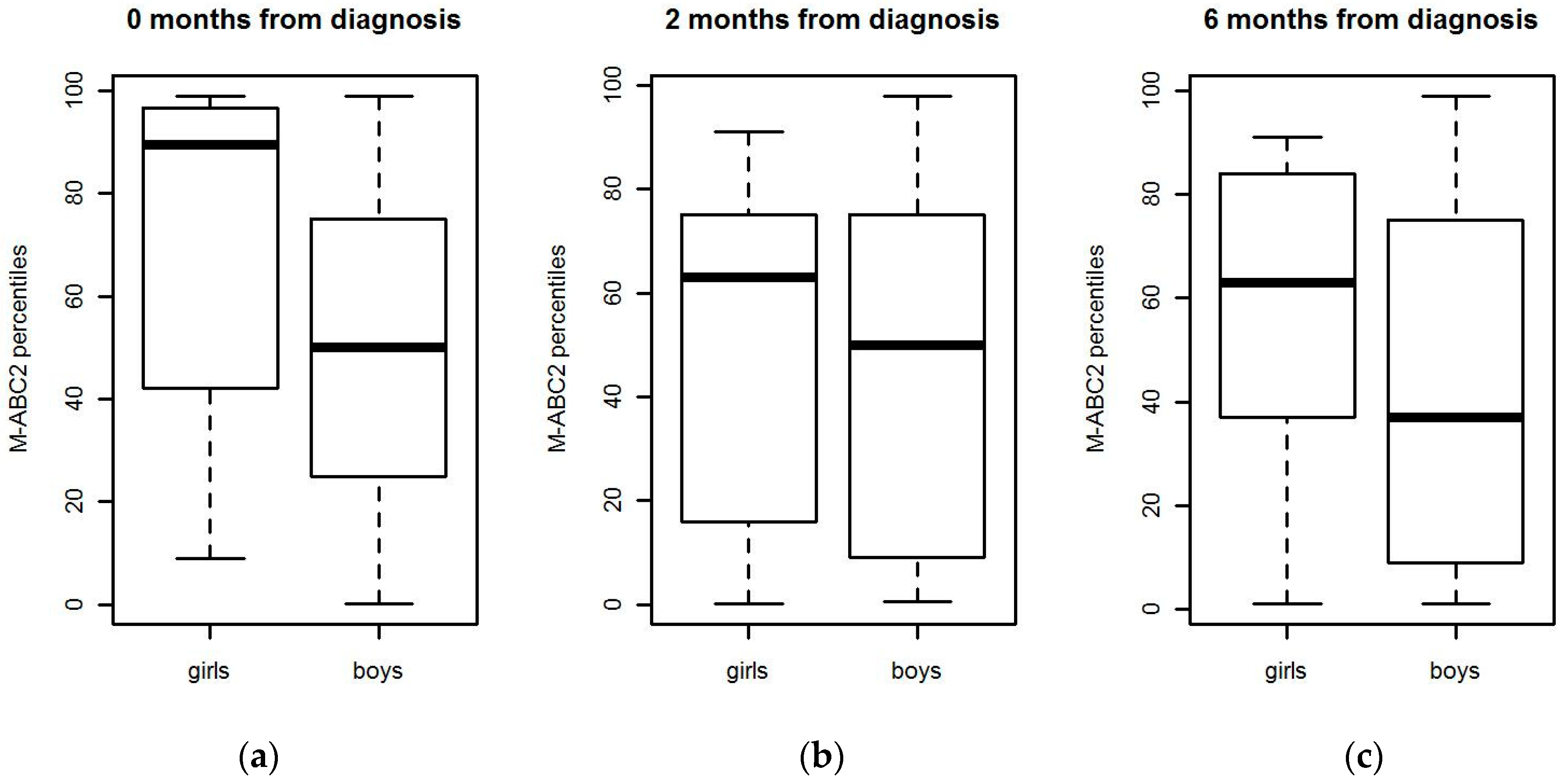
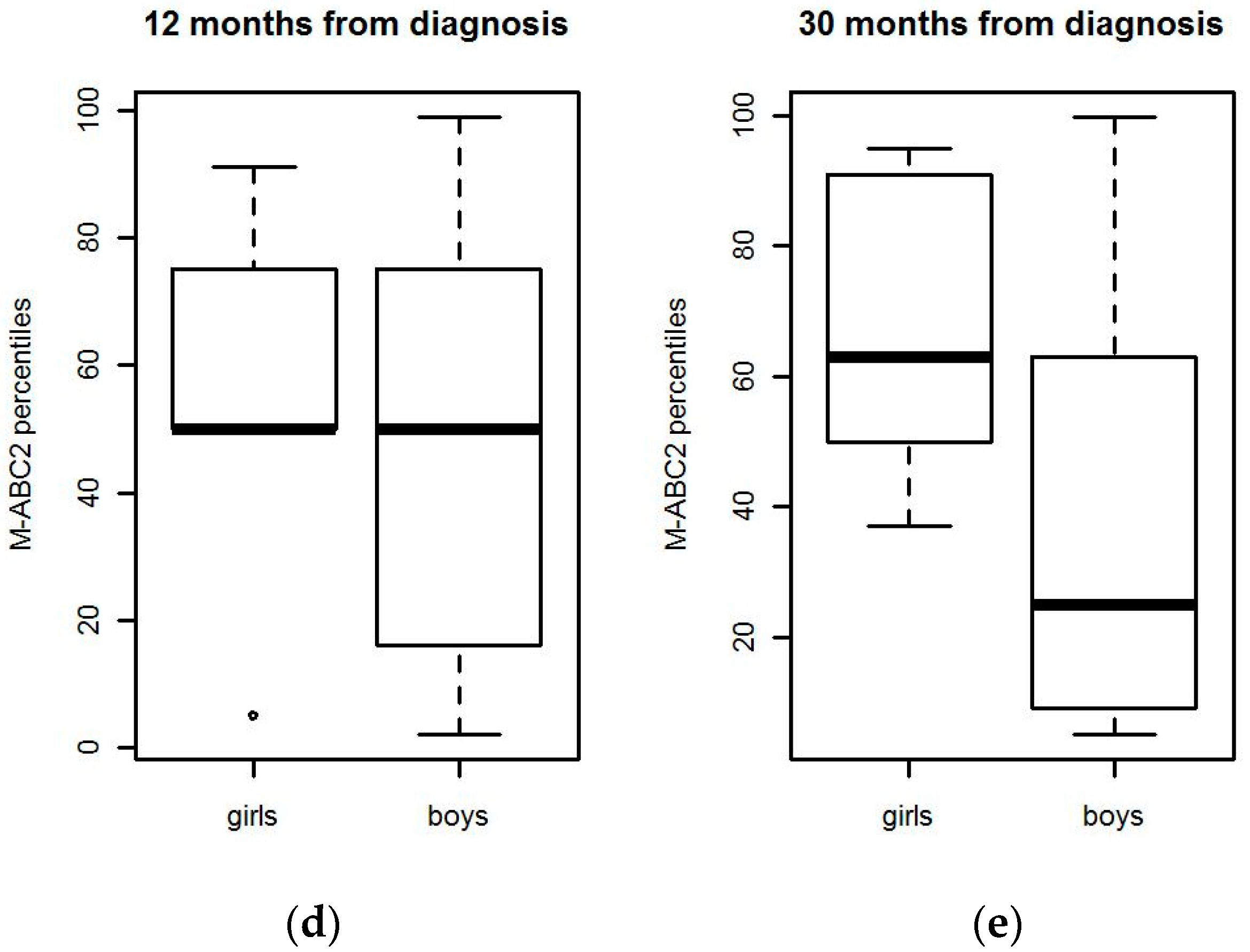
- What are the differences in motor performance domains between boys and girls and within different cancer diagnoses?
2.2. Participants
2.3. Outcome Measurement: Motor Performance
2.4. Data Analysis
3. Results
3.1. Demographics
3.2. Change in Motor Performance Domains during Treatment
3.3. Difference in Motor Performance between Different Diagnoses
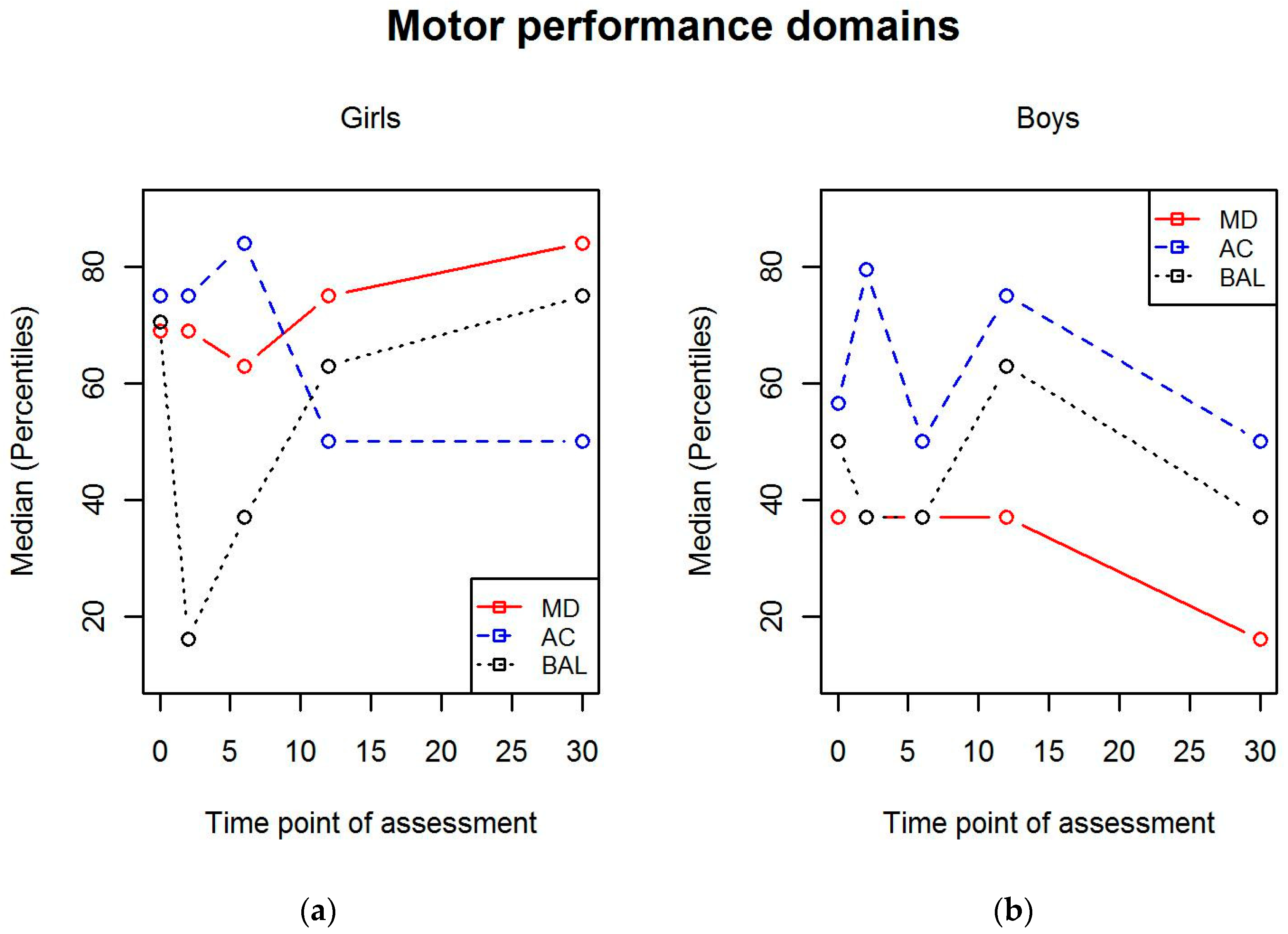
3.4. Differences between Gender in Motor Performance
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Armstrong, G.T.; Kawashima, T.; Leisenring, W.; Stratton, K.; Stovall, M.; Hudson, M.M.; Sklar, C.A.; Robison, L.L.; Oeffinger, K.C. Aging and risk of severe, disabling, life-threatening, and fatal events in the childhood cancer survivor study. J. Clin. Oncol. 2014, 32, 1218–1227. [Google Scholar] [CrossRef]
- Kelly, A.K.W. Physical Activity Prescription for Childhood Cancer Survivors. Curr. Sports Med. Rep. 2011, 10, 352–359. [Google Scholar] [CrossRef]
- Ness, K.K.; Kaste, S.C.; Zhu, L.; Pui, C.H.; Jeha, S.; Nathan, P.C.; Inaba, H.; Wasilewski-Masker, K.; Shah, D.; Wells, R.J.; et al. Skeletal, neuromuscular and fitness impairments among children with newly diagnosed acute lymphoblastic leukemia. Leuk. Lymphoma 2015, 56, 1004–1011. [Google Scholar] [CrossRef] [Green Version]
- Beulertz, J.; Bloch, W.; Prokop, A.; Rustler, V.; Fitzen, C.; Herich, L.; Streckmann, F.; Baumann, F.T. Limitations in Ankle Dorsiflexion Range of Motion, Gait, and Walking Efficiency in Childhood Cancer Survivors. Cancer Nurs. 2016, 39, 117–124. [Google Scholar] [CrossRef]
- Deisenroth, A.; Sontgerath, R.; Schuster, A.J.; von Busch, C.; Huber, G.; Eckert, K.; Kulozik, A.E.; Wiskemann, J. Muscle strength and quality of life in patients with childhood cancer at early phase of primary treatment. Pediatr. Hematol. Oncol. 2016, 33, 393–407. [Google Scholar] [CrossRef]
- Green, J.L.; Knight, S.J.; McCarthy, M.; De Luca, C.R. Motor functioning during and following treatment with chemotherapy for pediatric acute lymphoblastic leukemia. Pediatr. Blood Cancer 2013, 60, 1261–1266. [Google Scholar] [CrossRef] [PubMed]
- Hartman, A.; van den Bos, C.; Stijnen, T.; Pieters, R. Decrease in motor performance in children with cancer is independent of the cumulative dose of vincristine. Cancer 2006, 106, 1395–1401. [Google Scholar] [CrossRef] [PubMed]
- Braam, K.I.; van der Torre, P.; Takken, T.; Veening, M.A.; van Dulmen-den Broeder, E.; Kaspers, G.J. Physical exercise training interventions for children and young adults during and after treatment for childhood cancer. Cochrane Database Syst. Rev. 2016, 3, CD008796. [Google Scholar] [CrossRef] [Green Version]
- Götte, M.; Kesting, S.V.; Winter, C.C.; Rosenbaum, D.; Boos, J. Motor performance in children and adolescents with cancer at the end of acute treatment phase. Eur. J. Pediatr. 2015, 174, 791–799. [Google Scholar] [CrossRef] [PubMed]
- Wurz, A.; McLaughlin, E.; Lategan, C.; Ellis, K.; Culos-Reed, S.N. Synthesizing the literature on physical activity among children and adolescents affected by cancer: Evidence for the international Pediatric Oncology Exercise Guidelines (iPOEG). Submitted.
- Mizrahi, D.; Wakefield, C.E.; Fardell, J.E.; Quinn, V.F.; Lim, Q.; Clifford, B.K.; Simar, D.; Ness, K.K.; Cohn, R.J. Distance-delivered physical activity interventions for childhood cancer survivors: A systematic review and meta-analysis. Crit. Rev. Oncol. Hematol. 2017, 118, 27–41. [Google Scholar] [CrossRef] [PubMed]
- Morales, J.S.; Valenzuela, P.L.; Rincón-Castanedo, C.; Takken, T.; Fiuza-Luces, C.; Santos-Lozano, A.; Lucia, A. Exercise training in childhood cancer: A systematic review and meta-analysis of randomized controlled trials. Cancer Treat. Rev. 2018, 70, 154–167. [Google Scholar] [CrossRef] [PubMed]
- Rossi, F.; Coppo, M.; Zucchetti, G.; Bazzano, D.; Ricci, F.; Vassallo, E.; Nesi, F.; Fagioli, F. Rehabilitative intervention during and after pediatric hematopoietic stem cell transplantation: An analysis of the existing literature. Pediatr. Blood Cancer 2016, 63, 1895–1904. [Google Scholar] [CrossRef]
- Sharkey, A.M.; Carey, A.B.; Heise, C.T.; Barber, G. Cardiac rehabilitation after cancer therapy in children and young adults. Am. J. Cardiol. 1993, 71, 1488–1490. [Google Scholar] [CrossRef]
- Oberoi, S.; Robinson, P.D.; Cataudella, D.; Culos-Reed, S.N.; Davis, H.; Duong, N.; Gibson, F.; Götte, M.; Hinds, P.; Nijhof, S.L.; et al. Physical activity reduces fatigue in patients with cancer and hematopoietic stem cell transplant recipients: A systematic review and meta-analysis of randomized trials. Crit. Rev. Oncol. Hematol. 2018, 122, 52–59. [Google Scholar] [CrossRef] [PubMed]
- Coombs, A.; Schilperoort, H.; Sargent, B. The effect of exercise and motor interventions on physical activity and motor outcomes during and after medical intervention for children and adolescents with acute lymphoblastic leukemia: A systematic review. Crit. Rev. Oncol. Hematol. 2020, 152, 103004. [Google Scholar] [CrossRef] [PubMed]
- Wurz, A.; Daeggelmann, J.; Albinati, N.; Kronlund, L.; Chamorro-Viña, C.; Culos-Reed, S.N. Physical activity programs for children diagnosed with cancer: An international environmental scan. Support. Care Cancer 2019, 27, 1153–1162. [Google Scholar] [CrossRef] [PubMed]
- Hamari, L.; Järvelä, L.S.; Lähteenmäki, P.M.; Arola, M.; Axelin, A.; Vahlberg, T.; Salanterä, S. The effect of an active video game intervention on physical activity, motor performance, and fatigue in children with cancer: A randomized controlled trial. BMC Res. Notes 2019, 12, 784. [Google Scholar] [CrossRef]
- Kauhanen, L.; Järvelä, L.; Lähteenmäki, P.M.; Arola, M.; Heinonen, O.J.; Axelin, A.; Lilius, J.; Vahlberg, T.; Salanterä, S. Active video games to promote physical activity in children with cancer: A randomized clinical trial with follow-up. BMC Pediatr. 2014, 14, 94. [Google Scholar] [CrossRef] [Green Version]
- Henderson, S.E.; Sugden, D.A.; Barnett, A.L. Movement Assessment Battery for Children. Examiner’s Manual, 2nd ed.; Harcourt Assessment: London, UK, 2007. [Google Scholar]
- Croce, R.V.; Horvat, M.; McCarthy, E. Reliability and concurrent validity of the movement assessment battery for children. Percept. Mot. Ski. 2001, 93, 275–280. [Google Scholar] [CrossRef]
- De Luca, C.R.; McCarthy, M.; Galvin, J.; Green, J.L.; Murphy, A.; Knight, S.; Williams, J. Gross and fine motor skills in children treated for acute lymphoblastic leukaemia. Dev. Neurorehabil. 2013, 16, 180–187. [Google Scholar] [CrossRef]
- Bjornard, K.L.; Gilchrist, L.S.; Inaba, H.; Diouf, B.; Hockenberry, M.J.; Kadan-Lottick, N.S.; Bowers, D.C.; Dolan, M.E.; Ullrich, N.J.; Evans, W.E.; et al. Peripheral neuropathy in children and adolescents treated for cancer. Lancet Child Adolesc. Health 2018, 2, 744–754. [Google Scholar] [CrossRef]
- Baggott, C.; Dodd, M.; Kennedy, C.; Marina, N.; Matthay, K.K.; Cooper, B.A.; Miaskowski, C. Changes in children’s reports of symptom occurrence and severity during a course of myelosuppressive chemotherapy. J. Pediatr. Oncol. Nurs. 2010, 27, 307–315. [Google Scholar] [CrossRef] [PubMed]
- Collins, J.J.; Byrnes, M.E.; Dunkel, I.J.; Lapin, J.; Nadel, T.; Thaler, H.T.; Polyak, T.; Rapkin, B.; Portenoy, R.K. The measurement of symptoms in children with cancer. J. Pain Symptom Manage. 2000, 19, 363–377. [Google Scholar] [CrossRef]
- Walker, A.J.; Gedaly-Duff, V.; Miaskowski, C.; Nail, L. Differences in symptom occurrence, frequency, intensity, and distress in adolescents prior to and one week after the administration of chemotherapy. J. Pediatr. Oncol. Nurs. 2010, 27, 259–265. [Google Scholar] [CrossRef] [PubMed]
- Moser, T.; Reikerås, E. Motor-life-skills of toddlers—A comparative study of Norwegian and British boys and girls applying the Early Years Movement Skills Checklist. Eur. Early Child. Educ. Res. J. 2016, 24, 115–135. [Google Scholar] [CrossRef]
- Pahkala, K.; Heinonen, O.J.; Lagström, H.; Hakala, P.; Sillanmäki, L.; Simell, O. Leisure-time physical activity of 13-year-old adolescents. Scand. J. Med. Sci. Sports 2007, 17, 324–330. [Google Scholar] [CrossRef]
- Sallis, J.F.; Prochaska, J.J.; Taylor, W.C. A review of correlates of physical activity of children and adolescents. Med. Sci. Sports Exerc. 2000, 32, 963–975. [Google Scholar] [CrossRef]
- Trost, S.G.; Loprinzi, P.D. Parental Influences on Physical Activity Behavior in Children and Adolescents: A Brief Review. Am. J. Lifestyle Med. 2011, 5, 171–181. [Google Scholar] [CrossRef]
- Heitzler, C.D.; Martin, S.L.; Duke, J.; Huhman, M. Correlates of physical activity in a national sample of children aged 9–13 years. Prev. Med. 2006, 42, 254–260. [Google Scholar] [CrossRef]
- Soini, A.; Villberg, J.; Sääkslahti, A.; Gubbels, J.; Mehtälä, A.; Kettunen, T.; Poskiparta, M. Directly Observed Physical Activity among 3-Year-Olds in Finnish Childcare. Int. J. Early Child. 2014, 46, 253–269. [Google Scholar] [CrossRef] [Green Version]
- Pakarinen, A.; Hautala, L.; Hamari, L.; Aromaa, M.; Kallio, H.; Liuksila, P.; Sillanpää, M.; Salanterä, S. The Association between the Preference for Active Play and Neurological Development in Toddlers: A Register-Based Study. Int. J. Environ. Res. Public Health 2020, 17, 2525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, H.G.; Pfeiffer, K.A.; O’Neill, J.R.; Dowda, M.; McIver, K.L.; Brown, W.H.; Pate, R.R. Motor skill performance and physical activity in preschool children. Obesity 2008, 16, 1421–1426. [Google Scholar] [CrossRef] [PubMed]
- Piek, J.P.; Dawson, L.; Smith, L.M.; Gasson, N. The role of early fine and gross motor development on later motor and cognitive ability. Hum. Mov. Sci 2008, 27, 668–681. [Google Scholar] [CrossRef] [PubMed]
- Cliff, D.P.; Okely, A.D.; Smith, L.M.; McKeen, K. Relationships between fundamental movement skills and objectively measured physical activity in preschool children. Pediatr. Exerc. Sci. 2009, 21, 436–449. [Google Scholar] [CrossRef] [Green Version]
- Kantomaa, M.T.; Stamatakis, E.; Kankaanpaa, A.; Kaakinen, M.; Rodriguez, A.; Taanila, A.; Ahonen, T.; Jarvelin, M.R.; Tammelin, T. Physical activity and obesity mediate the association between childhood motor function and adolescents’ academic achievement. Proc. Natl. Acad. Sci. USA 2013, 110, 1917–1922. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N (%) | Age at Diagnosis (Median, Min–Max) | |
|---|---|---|
| Study cohort | 36 (100) | 6.0 (3–16) |
| Girls | 10 (28) | 6.0 (4–16) |
| Boys | 26 (72) | 6.5 (3–15) |
| All | 17 (47) | 6.0 (3–16) |
| Standard risk | 8 | |
| Intermediate risk | 6 | |
| High risk | 3 | |
| Other | 19 (53) | 10 (3–15) |
| Wilms’ tumor | 2 | |
| Burkitt lymphoma | 3 | |
| Non-Hodgkin lymphoma | 5 | |
| Hodgkin lymphoma | 3 | |
| Other neoplasm | 6 |
| 0 Months Median (IQR) | 2 Months Median (IQR) | 6 Months Median (IQR) | 12 Months Median (IQR) | 30 Months Median (IQR) | |
|---|---|---|---|---|---|
| Total | |||||
| Study cohort | 63 (64.5) n = 29 | 63 (66) n = 31 | 56.5 (68.25) n = 30 | 50 (59) n = 30 | 37 (50) n = 30 |
| Boys | 50 (54.5) n = 21 | 50 (69.25) n = 22 | 37 (66) n = 21 | 50 (59) n = 21 | 25 (54) n = 21 |
| Girls | 89.5 (71.75) n = 8 | 63 (67) n = 9 | 63 (56.5) n = 9 | 50 (29.5) n = 9 | 63 (49.5) n = 9 |
| ALL | 50 (87.5) n = 13 | 37 (63) n = 16 | 63 (75) n = 15 | 50 (59) n = 15 | 37 (50.5) n = 17 |
| Other 1 | 63 (47) n = 16 | 63 (68) n = 15 | 50 (66) n = 15 | 63 (59) n = 15 | 63 (59) n = 13 |
| Aiming and catching | |||||
| Study cohort | 75 (45) | 75 (66) | 56.5 (70) | 63 (47) | 50 (52.25) |
| Boys | 56.5 (37.25) n = 22 | 79.5 (71) n = 22 | 50 (70) n = 21 | 75 (48.75) n = 22 | 50 (44) n = 21 |
| Girls | 75 (42.5) n = 9 | 75 (58.5) n = 9 | 84 (51.5) n = 9 | 50 (53) n = 9 | 50 (59) n = 9 |
| ALL | 75 (52) n = 14 | 75 (57.75) n = 16 | 63 (58) n = 15 | 50 (47) n = 15 | 50 (50) n = 17 |
| Other 1 | 75 (46) n = 17 | 63 (82) n = 15 | 50 (75) n = 15 | 69 (34) n = 16 | 50 (53) n = 13 |
| Balance | |||||
| Study cohort | 50 (66) | 37 (54) | 37 (55) | 63 (57) | 50 (66) |
| Boys | 50 (66) n = 21 | 37 (54) n = 22 | 37 (54) n = 21 | 63 (62.5) n = 21 | 37 (56.5) n = 21 |
| Girls | 70.5 (74.75) n = 8 | 16 (72.45) n = 9 | 37 (51.5) n = 9 | 63 (54) n = 9 | 75 (54) n = 9 |
| ALL | 37 (72) n = 13 | 20.5 (31) n = 16 | 37 (32) n = 15 | 63 (66) n = 15 | 37 (75) n = 17 |
| Other 1 | 62.5 (50.75) n = 16 | 50 (50) n = 15 | 50 (82) n = 15 | 63 (54) n = 15 | 50 (54) n = 13 |
| Manual dexterity | |||||
| Study cohort | 37 (52.25) | 43.5 (69) | 43.5 (54.5) | 37 (66) | 37 (68.25) |
| Boys | 37 (50) n = 24 | 37 (70) n = 22 | 37 (37.5) n = 21 | 37 (42) n = 22 | 16 (32) n = 21 |
| Girls | 69 (52.25) n = 10 | 69 (46) n = 10 | 63 (41) n = 9 | 75 (34) n = 9 | 84 (28.5) n = 9 |
| ALL | 56.5 (65.75) n = 16 | 37 (74.5) n = 17 | 50 (58) n = 15 | 50 (59) n = 15 | 37 (74.5) n = 17 |
| Other 1 | 37 (52.25) n = 18 | 50 (66) n = 15 | 37 (47) n = 15 | 37 (59.75) n = 16 | 37 (53) n = 13 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hamari, L.; Lähteenmäki, P.M.; Pukkila, H.; Arola, M.; Axelin, A.; Salanterä, S.; Järvelä, L.S. Motor Performance in Children Diagnosed with Cancer: A Longitudinal Observational Study. Children 2020, 7, 98. https://0-doi-org.brum.beds.ac.uk/10.3390/children7080098
Hamari L, Lähteenmäki PM, Pukkila H, Arola M, Axelin A, Salanterä S, Järvelä LS. Motor Performance in Children Diagnosed with Cancer: A Longitudinal Observational Study. Children. 2020; 7(8):98. https://0-doi-org.brum.beds.ac.uk/10.3390/children7080098
Chicago/Turabian StyleHamari, Lotta, Päivi M. Lähteenmäki, Heidi Pukkila, Mikko Arola, Anna Axelin, Sanna Salanterä, and Liisa S. Järvelä. 2020. "Motor Performance in Children Diagnosed with Cancer: A Longitudinal Observational Study" Children 7, no. 8: 98. https://0-doi-org.brum.beds.ac.uk/10.3390/children7080098