Association of Vitamin D Status and Physical Activity with Lipid Profile in Korean Children and Adolescents: A Population-Based Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
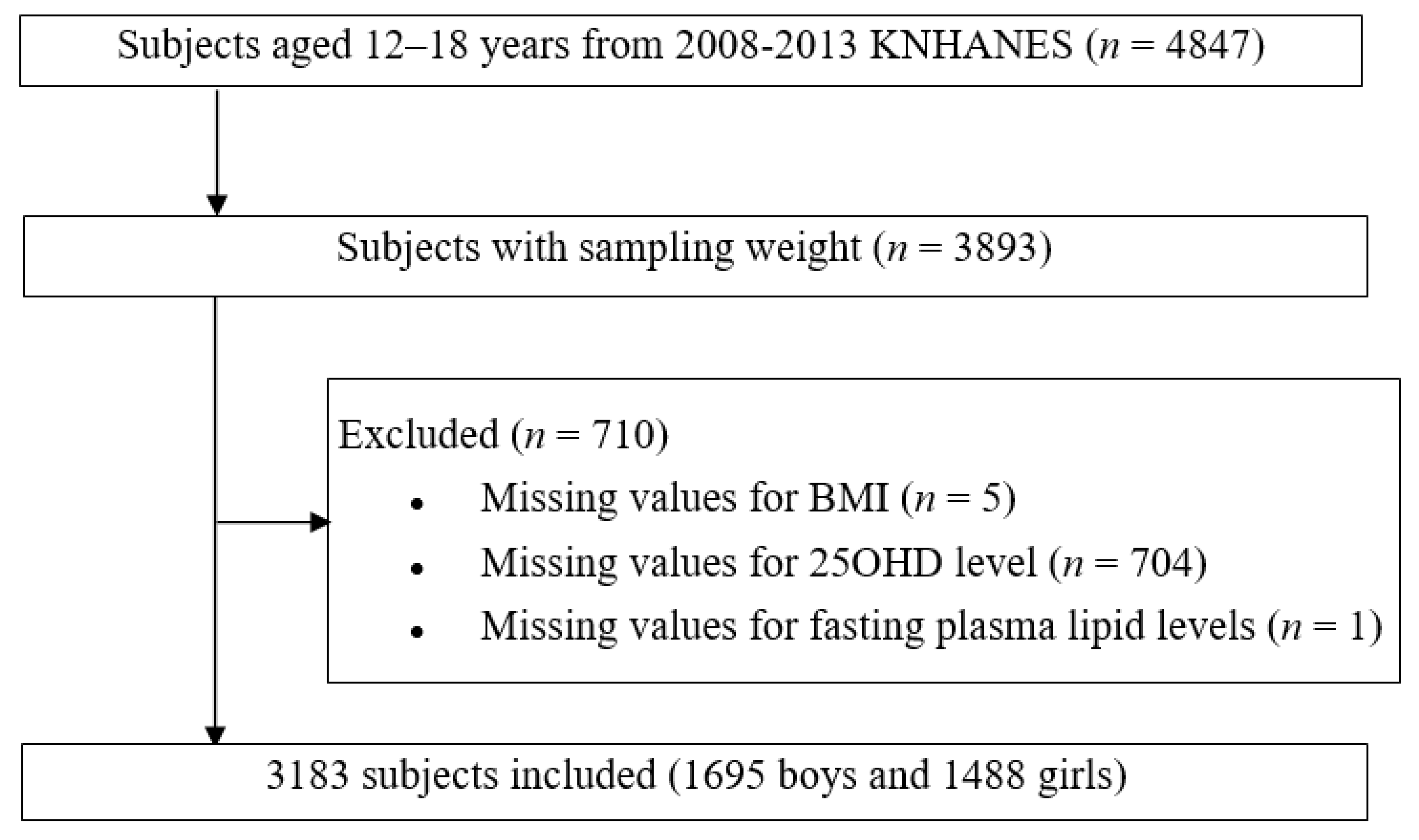
2.1. Study Population
2.2. Study Variables
2.3. Measurement of Serum 25OHD and Lipid Profiles
2.4. Statistical Analysis
3. Results
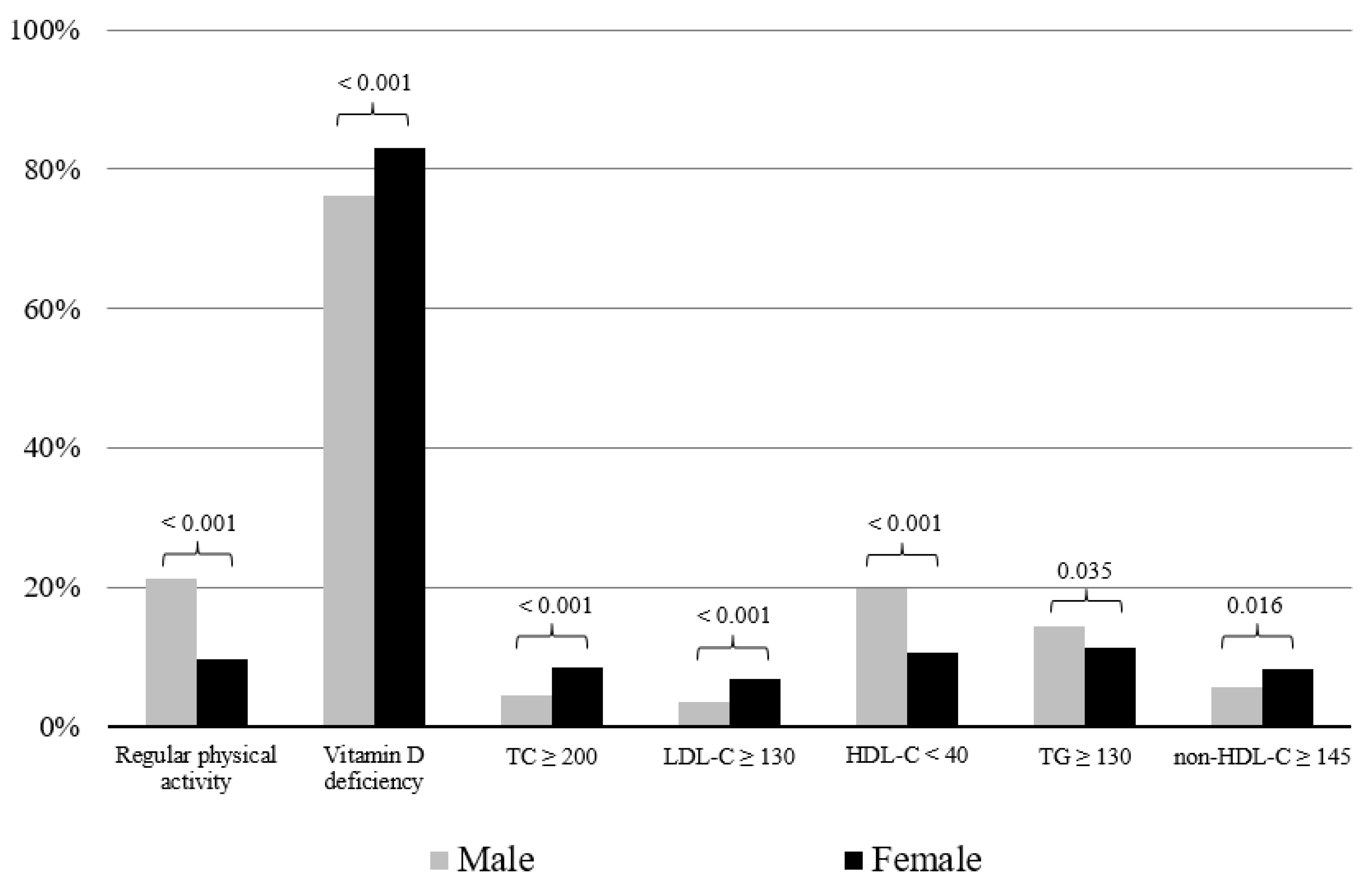
3.1. Baseline Characteristics of Subjects and Comparisons According to Sex
3.2. Association of Dyslipidemia and Physical Activity According to Sex and 25OHD Levels Among the Subjects
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Wang, Y.; Si, S.; Liu, J.; Wang, Z.; Jia, H.; Feng, K.; Sun, L.; Song, S. The Associations of Serum Lipids with Vitamin D Status. PLoS ONE 2016, 11, e0165157. [Google Scholar] [CrossRef]
- Holick, M.F.; Binkley, N.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, Treatment, and Prevention of Vitamin D Deficiency: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [Green Version]
- Misra, M.; Pacaud, D.; Petryk, A.; Collett-Solberg, P.F.; Kappy, M.; On behalf of the Drug and Therapeutics Committee of the Lawson Wilkins Pediatric Endocrine Society. Vitamin D Deficiency in Children and Its Management: Review of Current Knowledge and Recommendations. Pediatrics 2008, 122, 398–417. [Google Scholar] [CrossRef] [Green Version]
- Joseph, P.G.; Leong, D.; McKee, M.; Anand, S.S.; Schwalm, J.-D.; Teo, K.; Mente, A.; Yusuf, S. Reducing the Global Burden of Cardiovascular Disease, Part 1. Circ. Res. 2017, 121, 677–694. [Google Scholar] [CrossRef]
- Perak, A.M.; Ning, H.; Kit, B.K.; De Ferranti, S.D.; Van Horn, L.V.; Wilkins, J.T.; Lloyd-Jones, D.M. Trends in Levels of Lipids and Apolipoprotein B in US Youths Aged 6 to 19 Years, 1999-2016. JAMA 2019, 321, 1895–1905. [Google Scholar] [CrossRef] [Green Version]
- Steinberger, J.; Daniels, S.R.; Hagberg, N.; Isasi, C.R.; Kelly, A.S.; Lloyd-Jones, D.; Pate, R.R.; Pratt, C.; Shay, C.M.; Towbin, J.A.; et al. Cardiovascular Health Promotion in Children: Challenges and Opportunities for 2020 and Beyond: A Scientific Statement from the American Heart Association. Circ. 2016, 134, e236–e255. [Google Scholar] [CrossRef] [Green Version]
- Yang, S.; Hwang, J.S.; Park, H.K.; Lee, H.S.; Kim, H.S.; Kim, E.Y.; Lim, J.S. Serum Lipid Concentrations, Prevalence of Dyslipidemia, and Percentage Eligible for Pharmacological Treatment of Korean Children and Adolescents; Data from the Korea National Health and Nutrition Examination Survey IV (2007–2009). PLoS ONE 2012, 7, e49253. [Google Scholar] [CrossRef]
- Elkins, J.C.; Fruh, S.M.; Jones, L.; Bydalek, K. Clinical Practice Recommendations for Pediatric Dyslipidemia. J. Pediatrics Heal. Care 2019, 33, 494–504. [Google Scholar] [CrossRef] [Green Version]
- Jellinger, P.S.; Handelsman, Y.; Rosenblit, P.D.; Bloomgarden, Z.T.; Fonseca, V.A.; Garber, A.J.; Grunberger, G.; Guerin, C.K.; Bell, D.S.H.; Mechanick, J.I.; et al. American association of clinical endocrinologists and american college of endocrinology guidelines for management of dyslipidemia and prevention of cardiovascular disease. Endocr. Pract. 2017, 23, 1–87. [Google Scholar] [CrossRef] [Green Version]
- Shen, Z.; Munker, S.; Wang, C.; Xu, L.; Ye, H.; Chen, H.; Xu, G.; Zhang, H.; Chen, L.; Yu, C.; et al. Association between alcohol intake, overweight, and serum lipid levels and the risk analysis associated with the development of dyslipidemia. J. Clin. Lipidol. 2014, 8, 273–278. [Google Scholar] [CrossRef]
- Expert PANEL ON INTEGRATED GUIDELINES FOR CARDIOVASCULAR HEALTH AND RISK REDUCTION IN CHILDREN AND ADOLESCENTS. Expert Panel on Integrated Guidelines for Cardiovascular Health and Risk Reduction in Children and Adolescents: Summary Report. Pediatrics 2011, 128, S213–S256. [Google Scholar] [CrossRef] [Green Version]
- Gulati, A.; Dalal, J.J.; Padmanabhan, T.N.C.; Jain, P.; Patil, S.; Vasnawala, H. Lipitension: Interplay between dyslipidemia and hypertension. Indian J. Endocrinol. Metab. 2012, 16, 240–245. [Google Scholar] [CrossRef]
- Leblanc, A.G.; Janssen, I. Dose-response relationship between physical activity and dyslipidemia in youth. Can. J. Cardiol. 2010, 26, e201–e205. [Google Scholar] [CrossRef]
- Carey, V.J.; Bishop, L.; Laranjo, N.; Harshfield, B.J.; Kwiat, C.; Sacks, F.M. Contribution of High Plasma Triglycerides and Low High-Density Lipoprotein Cholesterol to Residual Risk of Coronary Heart Disease After Establishment of Low-Density Lipoprotein Cholesterol Control. Am. J. Cardiol. 2010, 106, 757–763. [Google Scholar] [CrossRef] [Green Version]
- Young, C.E.; Karas, R.H.; Kuvin, J.T. High-Density Lipoprotein Cholesterol and Coronary Heart Disease. Cardiol. Rev. 2004, 12, 107–119. [Google Scholar] [CrossRef]
- Cox, R.A.; García-Palmieri, M.R. Cholesterol, triglycerides, and associated lipoproteins. In Clinical Methods: The History, Physical, and Laboratory Examinations; Walker, H.K., Hall, W.D., Hurst, J.W., Eds.; Butterworths. Copyright © 1990; Butterworth Publishers, a Division of Reed Publishing: Boston, MA, USA, 1990. [Google Scholar]
- Birken, C.S.; Lebovic, G.; Anderson, L.N.; McCrindle, B.W.; Mamdani, M.; Kandasamy, S.; Khovratovich, M.; Parkin, P.C.; Maguire, J.L. TARGet Kids! collaboration Association between Vitamin D and Circulating Lipids in Early Childhood. PLoS ONE 2015, 10, e0131938. [Google Scholar] [CrossRef] [Green Version]
- Kim, M.R.; Jeong, S.J. Relationship between Vitamin D Level and Lipid Profile in Non-Obese Children. Metab. 2019, 9, 125. [Google Scholar] [CrossRef] [Green Version]
- Kelishadi, R.; Farajzadegan, Z.; Bahreynian, M. Association between vitamin D status and lipid profile in children and adolescents: A systematic review and meta-analysis. Int. J. Food Sci. Nutr. 2014, 65, 404–410. [Google Scholar] [CrossRef]
- Dolinsky, D.H.; Armstrong, S.; Mangarelli, C.; Kemper, A.R. The Association Between Vitamin D and Cardiometabolic Risk Factors in Children. Clin. Pediatrics 2013, 52, 210–223. [Google Scholar] [CrossRef]
- Kweon, S.; Kim, Y.; Jang, M.-J.; Kim, Y.; Kim, K.; Choi, S.; Chun, C.; Khang, Y.-H.; Oh, K. Data resource profile: The Korea National Health and Nutrition Examination Survey (KNHANES). Int. J. Epidemiol. 2014, 43, 69–77. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.H.; Yun, S.; Hwang, S.-S.; Shim, J.O.; Chae, H.W.; Lee, Y.J.; Lee, J.H.; Kim, S.C.; Lim, D.; Yang, S.W.; et al. The 2017 Korean National Growth Charts for children and adolescents: Development, improvement, and prospects. Korean J. Pediatrics 2018, 61, 135–149. [Google Scholar] [CrossRef]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Global trends in insufficient physical activity among adolescents: A pooled analysis of 298 population-based surveys with 1·6 million participants. Lancet Child Adolesc. Health 2020, 4, 23–35. [Google Scholar] [CrossRef]
- Roberts, W.C. The Friedewald-Levy-Fredrickson formula for calculating low-density lipoprotein cholesterol, the basis for lipid-lowering therapy. Am. J. Cardiol. 1988, 62, 345–346. [Google Scholar] [CrossRef]
- Blumenthal, R.S.; Blumenthal, R.S.; Flaws, J.A.; Whiteman, M.K.; Langenberg, P.; Bachorik, P.S.; Bush, T.L. Non–High-Density Lipoprotein Cholesterol Level as a Predictor of Cardiovascular Disease Mortality. Arch. Intern. Med. 2001, 161, 1413–1419. [Google Scholar] [CrossRef]
- Rusconi, R.E.; De Cosmi, V.; Gianluca, G.; Giavoli, C.; Agostoni, C. Vitamin D insufficiency in obese children and relation with lipid profile. Int. J. Food Sci. Nutr. 2015, 66, 132–134. [Google Scholar] [CrossRef]
- Wehmeier, K.R.; Beers, A.; Haas, M.J.; Wong, N.C.; Steinmeyer, A.; Zugel, U.; Mooradian, A.D. Inhibition of apolipoprotein AI gene expression by 1, 25-dihydroxyvitamin D3. Biochim. Biophys. Acta (BBA)-Mol. Cell Biol. Lipids 2005, 1737, 16–26. [Google Scholar] [CrossRef]
- Johnson, M.D.; Nader, N.D.; Weaver, A.L.; Singh, R.; Kumar, S. Relationships between 25-Hydroxyvitamin D Levels and Plasma Glucose and Lipid Levels in Pediatric Outpatients. J. Pediatrics 2010, 156, 444–449.e1. [Google Scholar] [CrossRef]
- Auwerx, J.; Bouillon, R.; Kesteloot, H. Relation between 25-hydroxyvitamin D3, apolipoprotein A-I, and high density lipoprotein cholesterol. Arter. Thromb. A J. Vasc. Biol. 1992, 12, 671–674. [Google Scholar] [CrossRef] [Green Version]
- Arnberg, K.; Østergård, M.; Madsen, A.; Krarup, H.B.; Michaelsen, K.F.; Mølgaard, C. Associations between vitamin D status in infants and blood lipids, body mass index and waist circumference. Acta Paediatr. 2011, 100, 1244–1248. [Google Scholar] [CrossRef]
- Gonzalez, F.J.; Moschetta, A. Potential role of the vitamin D receptor in control of cholesterol levels. Gastroenterol. 2014, 146, 899–902. [Google Scholar] [CrossRef]
- Christensen, R.; Lorenzen, J.K.; Svith, C.R.; Bartels, E.M.; Melanson, E.L.; Saris, W.H.; Tremblay, A.; Astrup, A. Effect of calcium from dairy and dietary supplements on faecal fat excretion: A meta-analysis of randomized controlled trials. Obes. Rev. 2009, 10, 475–486. [Google Scholar] [CrossRef]
- Vaskonen, T.; Mervaala, E.; Sumuvuori, V.; Seppänen-Laakso, T.; Karppanen, H. Effects of calcium and plant sterols on serum lipids in obese zucker rats on a low-fat diet. Br. J. Nutr. 2002, 87, 239–245. [Google Scholar] [CrossRef] [Green Version]
- Jiang, X.; Peng, M.; Chen, S.; Wu, S.; Zhang, W. Vitamin D deficiency is associated with dyslipidemia: A cross-sectional study in 3788 subjects. Curr. Med Res. Opin. 2019, 35, 1059–1063. [Google Scholar] [CrossRef]
- Park, J.-H.; Hong, I.Y.; Chung, J.W.; Choi, H.S. Vitamin D status in South Korean population. Med. 2018, 97, e11032. [Google Scholar] [CrossRef]
- Schleicher, R.L.; Sternberg, M.R.; A Lacher, D.; Sempos, C.T.; Looker, A.C.; A Durazo-Arvizu, R.; A Yetley, E.; Chaudhary-Webb, M.; Maw, K.L.; Pfeiffer, C.M.; et al. The vitamin D status of the US population from 1988 to 2010 using standardized serum concentrations of 25-hydroxyvitamin D shows recent modest increases. Am. J. Clin. Nutr. 2016, 104, 454–461. [Google Scholar] [CrossRef] [Green Version]
- Mithal, A.; on behalf of the IOF Committee of Scientific Advisors (CSA) Nutrition Working Group; Wahl, D.A.; Bonjour, J.-P.; Burckhardt, P.; Dawson-Hughes, B.; Eisman, J.A.; Fuleihan, G.E.-H.; Josse, R.G.; Lips, P.; et al. Global vitamin D status and determinants of hypovitaminosis D. Osteoporos. Int. 2009, 20, 1807–1820. [Google Scholar] [CrossRef] [Green Version]
- Ford, E.S.; Li, C.; Zhao, G.; Mokdad, A.H. Concentrations of Low-Density Lipoprotein Cholesterol and Total Cholesterol among Children and Adolescents in the United States. Circulation 2009, 119, 1108–1115. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Total (n = 3183) | Male (n = 1695) | Female (n = 1488) | p | |
|---|---|---|---|---|
| Age (year), mean (SE) | 15.09 (0.04) | 15.11 (0.05) | 15.08 (0.06) | 0.709 |
| Height (cm), mean (SE) | 165.35 (0.20) | 169.73 (0.25) | 160.06 (0.19) | < 0.001 |
| Weight (kg), mean (SE) | 58.03 (0.29) | 61.81 (0.40) | 53.46 (0.33) | < 0.001 |
| BMI (kg/m2), mean (SE) | 21.08 (0.08) | 21.31 (0.11) | 20.82 (0.11) | 0.002 |
| BMI SDS, mean (SE) | −0.08 (0.03) | −0.12 (0.04) | −0.03 (0.04) | 0.095 |
| BMI group, percentage (SE) | 0.712 | |||
| Normal (%) | 80.71 (0.81) | 80.10 (1.14) | 81.44 (1.26) | |
| Overweight (%) | 9.68 (0.60) | 9.84 (0.84) | 9.49 (0.88) | |
| Obesity (%) | 9.61 (0.65) | 10.06 (0.93) | 9.07 (0.98) | |
| Physical activity (hour/week), mean (SE) | 4.10 (0.18) | 5.33 (0.27) | 2.62 (0.19) | < 0.001 |
| 25OHD (ng/mL), mean (SE) | 16.15 (0.16) | 16.78 (0.20) | 15.40 (0.19) | < 0.001 |
| TC (mg/dL), mean (SE) | 155.72 (0.66) | 150.64 (0.87) | 161.88 (0.84) | < 0.001 |
| LDL-C (mg/dL), mean (SE) | 88.95 (0.55) | 85.57 (0.75) | 93.05 (0.74) | < 0.001 |
| HDL-C (mg/dL), mean (SE) | 49.75 (0.23) | 47.93 (0.27) | 51.96 (0.33) | < 0.001 |
| TG (mg/dL), mean (SE) | 85.09 (1.19) | 85.73 (1.64) | 84.32 (1.53) | 0.507 |
| Non-HDL-C (mg/dL), mean (SE) | 105.97 (0.61) | 102.71 (0.84) | 109.91 (0.81) | < 0.001 |
| Male (n = 1695) | Normal (n = 1358) | Overweight or Obesity (n = 337) | ||||
|---|---|---|---|---|---|---|
| Vitamin D Deficiency (n = 993) | Vitamin D Sufficiency (n = 365) | p | Vitamin D Deficiency (n = 133) | Vitamin D Sufficiency (n = 41) | p | |
| TC ≥ 200, percentage (SE) | 2.39 (0.61) | 4.79 (1.19) | 0.050 | 4.37 (0.73) | 4.83 (1.06) | 0.712 |
| LDL-C ≥ 130, percentage (SE) | 1.42 (0.46) | 3.31 (1.07) | 0.056 | 3.53 (0.67) | 3.44 (0.96) | 0.944 |
| HDL-C < 40, percentage (SE) | 17.08 (1.36) | 12.17 (1.93) | 0.049 | 21.68 (1.36) | 14.30 (1.92) | 0.003 |
| TG ≥ 130, percentage (SE) | 9.15 (1.03) | 11.15 (1.99) | 0.333 | 14.70 (1.21) | 13.21 (2.06) | 0.480 |
| non-HDL-C ≥ 145, percentage (SE) | 2.70 (0.61) | 4.22 (1.08) | 0.192 | 6.07 (0.83) | 4.65 (1.00) | 0.290 |
| Physical activity (h/week), mean (SE) | 4.60 (0.32) | 6.67 (0.75) | 0.011 | 4.85 (0.30) | 6.84 (0.64) | 0.005 |
| Female (n = 1488) | Normal (n = 1223) | Overweight or Obesity (n = 142) | ||||
| Vitamin D deficiency (n = 993) | Vitamin D sufficiency (n = 230) | p | Vitamin D deficiency (n = 113) | Vitamin D sufficiency (n = 29) | p | |
| TC ≥ 200, percentage (SE) | 8.04 (1.01) | 6.62 (1.73) | 0.505 | 8.84 (0.97) | 6.89 (1.66) | 0.346 |
| LDL-C ≥ 130, percentage (SE) | 6.11 (0.89) | 5.09 (1.45) | 0.572 | 6.93 (0.86) | 6.16 (1.54) | 0.676 |
| HDL-C < 40, percentage (SE) | 5.81 (0.89) | 13.46 (2.74) | 0.001 | 9.45 (1.05) | 16.77 (2.70) | 0.003 |
| TG ≥ 130, percentage (SE) | 8.29 (1.05) | 12.30 (2.55) | 0.102 | 10.86 (1.08) | 13.84 (2.38) | 0.222 |
| non-HDL-C ≥ 145, percentage (SE) | 6.60 (0.92) | 6.84 (1.74) | 0.904 | 8.20 (0.91) | 8.36 (1.86) | 0.937 |
| Physical activity (h/week), mean (SE) | 2.31 (0.21) | 3.04 (0.60) | 0.256 | 2.43 (0.19) | 3.55 (0.57) | 0.055 |
| TC < 200 | TC ≥ 200 | p | LDL-C < 130 | LDL-C ≥ 130 | p | HDL-C ≥ 40 | HDL-C < 40 | p | TG < 130 | TG ≥ 130 | p | non-HDL-C < 145 | non-HDL-C ≥ 145 | p | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Male (n = 1695) | Normal (n = 1358) | No. of Participants (n) | 1314 | 44 | 1331 | 27 | 1140 | 218 | 1224 | 134 | 1314 | 44 | |||||
| Vitamin D deficiency, percentage (SE) | 75.80 (1.60) | 60.39 (8.65) | 0.050 | 75.70 (1.58) | 56.65 (11.32) | 0.056 | 74.25 (1.73) | 81.09 (2.90) | 0.049 | 75.75 (1.63) | 71.48 (4.44) | 0.333 | 75.63 (1.61) | 66.16 (7.69) | 0.192 | ||
| Physical activity (h/week), mean (SE) | 5.13 (0.31) | 4.55 (1.03) | 0.589 | 5.15 (0.31) | 3.32 (0.93) | 0.060 | 5.26 (0.33) | 4.31 (0.68) | 0.192 | 5.11 (0.30) | 5.17 (1.15) | 0.954 | 5.13 (0.31) | 4.59 (1.04) | 0.619 | ||
| Overweight or obesity (n = 337) | No. of Participants (n) | 304 | 34 | 305 | 32 | 218 | 119 | 237 | 100 | 334 | 53 | ||||||
| Vitamin D deficiency, percentage (SE) | 76.25 (1.44) | 74.26 (5.37) | 0.712 | 76.14 (1.43) | 76.58 (6.03) | 0.944 | 74.43 (1.64) | 83.12 (2.23) | 0.003 | 75.79 (1.51) | 78.36 (3.29) | 0.480 | 75.89 (1.46) | 80.62 (3.98) | 0.290 | ||
| Physical activity (h/week), mean (SE) | 5.38 (0.28) | 4.28 (0.71) | 0.150 | 5.38 (0.28) | 3.76 (0.69) | 0.026 | 5.41 (0.29) | 5.01 (0.70) | 0.597 | 5.44 (0.29) | 4.65 (0.67) | 0.266 | 5.41 (0.29) | 4.00 (0.58) | 0.028 | ||
| Female (n = 1488) | Normal (n = 1223) | No. of Participants (n) | 1126 | 97 | 1151 | 72 | 1128 | 95 | 1107 | 116 | 1137 | 86 | |||||
| Vitamin D deficiency, percentage (SE) | 82.28 (1.51) | 85.14 (3.78) | 0.505 | 82.35 (1.49) | 84.98 (4.20) | 0.572 | 83.69 (1.44) | 67.04 (6.02) | 0.001 | 83.14 (1.48) | 76.08 (4.60) | 0.102 | 82.54 (1.48) | 81.99 (4.45) | 0.904 | ||
| Physical activity (h/week), mean (SE) | 2.37 (0.22) | 3.33 (0.63) | 0.150 | 2.37 (0.21) | 3.58 (0.79) | 0.137 | 2.46 (0.22) | 2.22 (0.49) | 0.661 | 2.50 (0.22) | 1.86 (0.25) | 0.059 | 2.39 (0.21) | 3.08 0.67) | 0.330 | ||
| Overweight or obesity (n = 265) | No. of Participants (n) | 237 | 28 | 237 | 28 | 196 | 69 | 207 | 58 | 223 | 42 | ||||||
| Vitamin D deficiency, percentage (SE) | 82.77 (1.40) | 86.31 (3.23) | 0.346 | 82.96 (1.38) | 84.66 (3.73) | 0.676 | 84.23 (1.35) | 73.45 (3.98) | 0.003 | 83.55 (1.36) | 79.39 (3.52) | 0.222 | 83.10 (1.38) | 82.80 (3.65) | 0.937 | ||
| Physical activity (h/week), mean (SE) | 2.55 (0.20) | 3.41 (0.56) | 0.146 | 2.56 (0.20) | 3.47 (0.63) | 0.175 | 2.62 (0.21) | 2.60 (0.41) | 0.956 | 2.69 (0.21) | 2.04 (0.26) | 0.056 | 2.57 (0.20) | 3.13 (0.50) | 0.307 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, K.; Park, G.; Choi, Y.; Oh, J.S.; Choi, H.S.; Suh, J.; Kwon, A.; Kim, H.-S.; Chae, H.W. Association of Vitamin D Status and Physical Activity with Lipid Profile in Korean Children and Adolescents: A Population-Based Study. Children 2020, 7, 241. https://0-doi-org.brum.beds.ac.uk/10.3390/children7110241
Song K, Park G, Choi Y, Oh JS, Choi HS, Suh J, Kwon A, Kim H-S, Chae HW. Association of Vitamin D Status and Physical Activity with Lipid Profile in Korean Children and Adolescents: A Population-Based Study. Children. 2020; 7(11):241. https://0-doi-org.brum.beds.ac.uk/10.3390/children7110241
Chicago/Turabian StyleSong, Kyungchul, Gihong Park, Youngha Choi, Jun Suk Oh, Han Saem Choi, Junghwan Suh, Ahreum Kwon, Ho-Seong Kim, and Hyun Wook Chae. 2020. "Association of Vitamin D Status and Physical Activity with Lipid Profile in Korean Children and Adolescents: A Population-Based Study" Children 7, no. 11: 241. https://0-doi-org.brum.beds.ac.uk/10.3390/children7110241