The Intergenerational Transmission of Chronic Pain from Parents to Survivors of Childhood Cancer

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
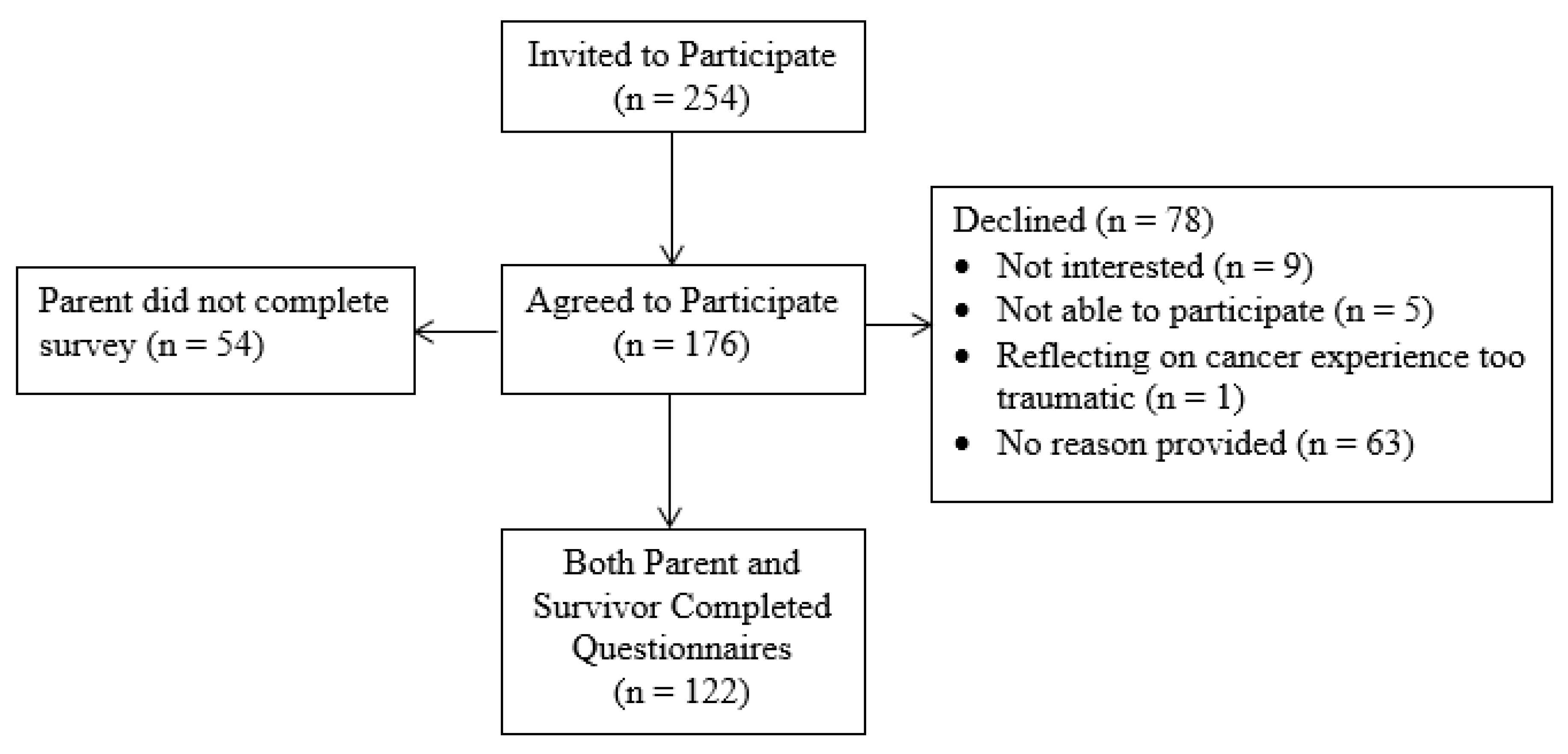
2.1. Participants
2.2. Measures
2.3. Procedure
2.4. Statistical Analyses
3. Results
3.1. Demographic Information
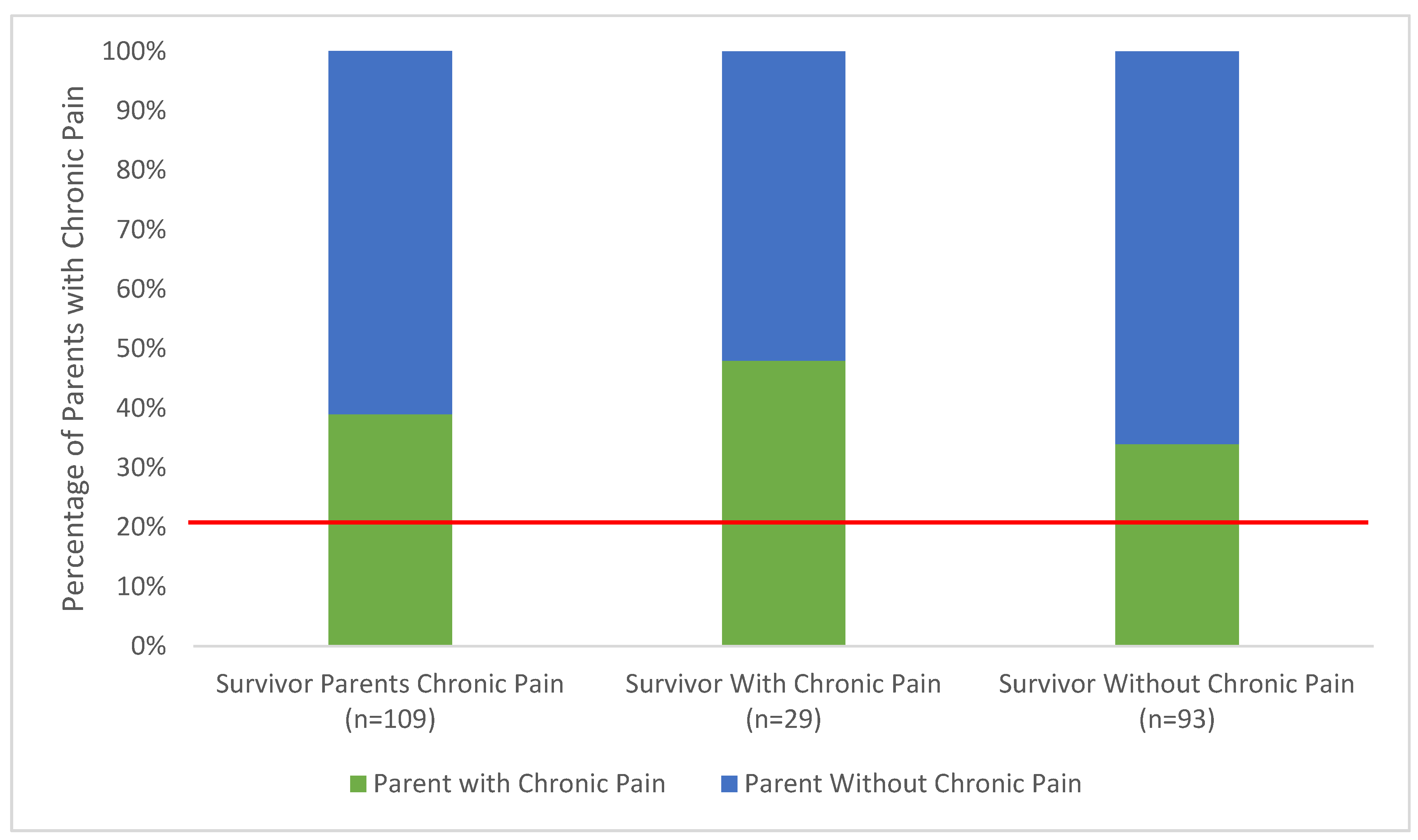
3.2. Aim 1: Identify Rates of Chronic Pain among Parents of SCCs
3.3. Aim 2: Test Group Differences in Psychological Symptoms in Parents with Chronic Pain Versus without Chronic Pain
3.4. Aim 3: Test Group Differences in Psychosocial Outcomes (i.e., Pain Interference, Quality of Life, Depression, Anxiety, and PTSS) in SCCs with Parents with Chronic Pain Versus SCCs with Parents without Chronic Pain
4. Discussion
5. Implications for Pain Management
6. Limitations and Future Directions
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Force, C.P.T. Chronic Pain in Canada: Laying a Foundation for Action; Health Canada: Ottawa, ON, Canada, 2019; pp. 1–50.
- Noel, M.; Groenewald, C.B.; Beals-Erickson, S.E.; Gebert, J.T.; Palermo, T.M. Chronic pain in adolescence and internalizing mental health disorders: A nationally representative study. Pain 2016, 157, 1333–1338. [Google Scholar] [CrossRef] [PubMed]
- Rabbitts, J.A.; Holley, A.L.; Groenewald, C.B.; Palermo, T.M. Association Between Widespread Pain Scores and Functional Impairment and Health-Related Quality of Life in Clinical Samples of Children. J. Pain 2016, 17, 678–684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tham, S.W.; Holley, A.L.; Zhou, C.; Clarke, G.N.; Palermo, T.M. Longitudinal course and risk factors for fatigue in adolescents: The mediating role of sleep disturbances. J. Pediatr. Psychol. 2013, 38, 1070–1080. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fales, J.L.; Murphy, L.K.; Rights, J.D.; Palermo, T.M. Daily Peer Victimization Experiences of Adolescents With and Without Chronic Pain: Associations With Mood, Sleep, Pain, and Activity Limitations. J. Pain 2019. [Google Scholar] [CrossRef] [PubMed]
- Beveridge, J.K.; Neville, A.; Wilson, A.C.; Noel, M. Intergenerational examination of pain and posttraumatic stress disorder symptoms among youth with chronic pain and their parents. Pain Rep. 2018, 3, e667. [Google Scholar] [CrossRef]
- Higgins, K.S.; Birnie, K.A.; Chambers, C.T.; Wilson, A.C.; Caes, L.; Clark, A.J.; Lynch, M.; Stinson, J.; Campbell-Yeo, M. Offspring of parents with chronic pain: A systematic review and meta-analysis of pain, health, psychological, and family outcomes. Pain 2015, 156, 2256–2266. [Google Scholar] [CrossRef] [PubMed]
- Stone, A.L.; Wilson, A.C. Transmission of risk from parents with chronic pain to offspring: An integrative conceptual model. Pain 2016, 157, 2628–2639. [Google Scholar] [CrossRef]
- Lynch, A.M.; Kashikar-Zuck, S.; Goldschneider, K.R.; Jones, B.A. Psychosocial risks for disability in children with chronic back pain. J. Pain 2006, 7, 244–251. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2016. CA Cancer J. Clin. 2016, 66, 7–30. [Google Scholar] [CrossRef] [Green Version]
- Lu, Q.; Krull, K.R.; Leisenring, W.; Owen, J.E.; Kawashima, T.; Tsao, J.C.; Zebrack, B.; Mertens, A.; Armstrong, G.T.; Stovall, M.; et al. Pain in long-term adult survivors of childhood cancers and their siblings: A report from the Childhood Cancer Survivor Study. Pain 2011, 152, 2616–2624. [Google Scholar] [CrossRef] [Green Version]
- Blaauwbroek, R.; Groenier, K.H.; Kamps, W.A.; Meyboom-de Jong, B.; Postma, A. Late effects in adult survivors of childhood cancer: The need for life-long follow-up. Ann. Oncol. 2007, 18, 1898–1902. [Google Scholar] [CrossRef] [PubMed]
- Patton, M.; Forster, V.; Forbes, C.; Stokoe, M.; Noel, M.; Carlson, C.A.; Reynolds, K.; Schulte, F. Characterizing Pain in Long-Term Survivors of Childhood Cancer; University of Calgary: Calgary, AB, Canada, 2020; Under Review. [Google Scholar]
- McGrath, P.A. Pain in Children: Nature, Assessment, and Treatment; Guilford: New York, NY, USA, 1990. [Google Scholar]
- Derogatis, L.R.; Melisaratos, N. The Brief Symptom Inventory: An introductory report. Psychol. Med. 1983, 13, 595–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varni, J.W.; Seid, M.; Kurtin, P.S. PedsQL™ 4.0: Reliability and Validity of the Pediatric Quality of Life Inventory™ Version 4.0 Generic Core Scales in Healthy and Patient Populations. Med. Care 2001, 39, 800–812. [Google Scholar] [CrossRef] [PubMed]
- Varni, J.W. Family functioning predictors of adjustment in children with newly diagnosed cancer: A prospective analysis. J. Child Psychol. Psychiatry 1996, 37, 321–328. [Google Scholar] [CrossRef]
- Foa, E.B.; Johnson, K.M.; Feeny, N.C.; Treadwell, K.R. The child PTSD Symptom Scale: A preliminary examination of its psychometric properties. J. Clin. Child Psychol. 2001, 30, 376–384. [Google Scholar] [CrossRef]
- Stewart, R.W.; Ebesutani, C.; Drescher, C.F.; Young, J. The Child PTSD Symptom Scale: An Investigation of Its Psychometric Properties. J. Interpers Violence 2017, 32, 2237–2256. [Google Scholar] [CrossRef]
- Nixon, R.D.; Meiser-Stedman, R.; Dalgleish, T.; Yule, W.; Clark, D.M.; Perrin, S.; Smith, P. The Child PTSD Symptom Scale: An update and replication of its psychometric properties. Psychol. Assess. 2013, 25, 1025–1031. [Google Scholar] [CrossRef] [Green Version]
- Kaplan, L.M.; Kaal, K.J.; Bradley, L.; Alderfer, M.A. Cancer-related traumatic stress reactions in siblings of children with cancer. Fam. Syst. Health 2013, 31, 205–217. [Google Scholar] [CrossRef] [Green Version]
- Blevins, C.A.; Weathers, F.W.; Davis, M.T.; Witte, T.K.; Domino, J.L. The Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5): Development and Initial Psychometric Evaluation. J. Trauma Stress 2015, 28, 489–498. [Google Scholar] [CrossRef]
- Ashbaugh, A.R.; Houle-Johnson, S.; Herbert, C.; El-Hage, W.; Brunet, A. Psychometric Validation of the English and French Versions of the Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5). PLoS ONE 2016, 11, e0161645. [Google Scholar] [CrossRef]
- Cella, D.; Riley, W.; Stone, A.; Rothrock, N.; Reeve, B.; Yount, S.; Amtmann, D.; Bode, R.; Buysse, D.; Choi, S.; et al. The Patient-Reported Outcomes Measurement Information System (PROMIS) developed and tested its first wave of adult self-reported health outcome item banks: 2005-2008. J. Clin. Epidemiol. 2010, 63, 1179–1194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hinds, P.S.; Nuss, S.L.; Ruccione, K.S.; Withycombe, J.S.; Jacobs, S.; DeLuca, H.; Faulkner, C.; Liu, Y.; Cheng, Y.I.; Gross, H.E.; et al. PROMIS pediatric measures in pediatric oncology: Valid and clinically feasible indicators of patient-reported outcomes. Pediatr. Blood Cancer 2013, 60, 402–408. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Treede, R.D.; Rief, W.; Barke, A.; Aziz, Q.; Bennett, M.I.; Benoliel, R.; Cohen, M.; Evers, S.; Finnerup, N.B.; First, M.B.; et al. A classification of chronic pain for ICD-11. Pain 2015, 156, 1003–1007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruce, M. A systematic and conceptual review of posttraumatic stress in childhood cancer survivors and their parents. Clin. Psychol. Rev. 2006, 26, 233–256. [Google Scholar] [CrossRef] [PubMed]
- Noel, M.; Wilson, A.C.; Holley, A.L.; Durkin, L.; Patton, M.; Palermo, T.M. Posttraumatic stress disorder symptoms in youth with vs without chronic pain. Pain 2016, 157, 2277–2284. [Google Scholar] [CrossRef] [PubMed]
- Asmundson, G.J.; Coons, M.J.; Taylor, S.; Katz, J. PTSD and the experience of pain: Research and clinical implications of shared vulnerability and mutual maintenance models. Can. J. Psychiatry 2002, 47, 930–937. [Google Scholar] [CrossRef] [Green Version]
- Schulte, F.P.M.; Alberts, N.M.; Kunin-Batson, A.; Olson-Bullis, B.; Forbes, C.; Russell, K.B.; Neville, A.; Heathcote, L.C.; Karlson, C.W.; Racine, N.; et al. Pain in Long-Term Survivors of Childhood Cancer: A Systematic Review of the Current State of Knowledge and A Call to Action from the Children’s Oncology Group. Cancer 2020. [Google Scholar] [CrossRef]
- Lynch-Jordan, A.M.; Peugh, J.; Cunningham, N.R.; Trygier, J.R.; Kashikar-Zuck, S. Maternal Protective Parenting Accounts for the Relationship Between Pain Behaviors and Functional Disability in Adolescents. Clin. J. Pain 2018, 34, 1089–1095. [Google Scholar] [CrossRef]
- Poppert Cordts, K.M.; Stone, A.L.; Beveridge, J.K.; Wilson, A.C.; Noel, M. The (Parental) Whole Is Greater Than the Sum of Its Parts: A Multifactorial Model of Parent Factors in Pediatric Chronic Pain. J. Pain 2019, 20, 786–795. [Google Scholar] [CrossRef] [PubMed]
- Evans, S.; Shipton, E.A.; Keenan, T. The relationship between maternal chronic pain and child adjustment: The role of parenting as a mediator. J. Pain 2006, 7, 236–243. [Google Scholar] [CrossRef] [PubMed]
- Kazak, A.E. Evidence-based interventions for survivors of childhood cancer and their families. J. Pediatr. Psychol. 2005, 30, 29–39. [Google Scholar] [CrossRef] [PubMed]
- Huang, I.C.; Brinkman, T.M.; Mullins, L.; Pui, C.H.; Robison, L.L.; Hudson, M.M.; Krull, K.R. Child symptoms, parent behaviors, and family strain in long-term survivors of childhood acute lymphoblastic leukemia. Psychooncology 2018, 27, 2031–2038. [Google Scholar] [CrossRef] [PubMed]
- Salem, H.; Johansen, C.; Schmiegelow, K.; Winther, J.F.; Wehner, P.S.; Hasle, H.; Rosthoj, S.; Kazak, A.E.; Bidstrup, P.E. FAMily-Oriented Support (FAMOS): Development and feasibility of a psychosocial intervention for families of childhood cancer survivors. Acta Oncol. 2017, 56, 367–374. [Google Scholar] [CrossRef]
- Hilton, L.; Hempel, S.; Ewing, B.A.; Apaydin, E.; Xenakis, L.; Newberry, S.; Colaiaco, B.; Maher, A.R.; Shanman, R.M.; Sorbero, M.E.; et al. Mindfulness Meditation for Chronic Pain: Systematic Review and Meta-analysis. Ann. Behav. Med. 2017, 51, 199–213. [Google Scholar] [CrossRef] [Green Version]
- Williams, A.C.; Eccleston, C.; Morley, S. Psychological therapies for the management of chronic pain (excluding headache) in adults. Cochrane Database Syst. Rev. 2012, 11, CD007407. [Google Scholar] [CrossRef]
- Sharp, T.J.; Harvey, A.G. Chronic pain and posttraumatic stress disorder: Mutual maintenance? Clin. Psychol. Rev. 2001, 21, 857–877. [Google Scholar] [CrossRef]
- Neville, A.; Soltani, S.; Pavlova, M.; Noel, M. Unravelling the Relationship Between Parent and Child PTSD and Pediatric Chronic Pain: The Mediating Role of Pain Catastrophizing. J. Pain. 2018, 19, 196–206. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Survivors (n = 122) | Parents (n = 122) | |
|---|---|---|
| Current age † | 15.8 (4.8) | - |
| Sex ‡ | ||
| Male | 48 (45.7) | - |
| Female | 57 (54.3) | - |
| Age at diagnosis † | 5.9 (4.7) | - |
| Time since diagnosis (years) † | 10.9 (4.6) | - |
| Duration of chronic pain (years) † | - | 9.3 (10.8) |
| Diagnosis ‡ | ||
| Leukemia | 37 (36.3) | - |
| Solid tumor | 41 (40.2) | - |
| CNS tumor | 10 (9.8) | - |
| Lymphoma | 14 (13.7) | - |
| Time off treatment † | 9.3 (4.5) | - |
| Treatment ‡ | ||
| Chemotherapy | 102 (99.0) | - |
| Radiation | 34 (33.0) | - |
| Surgery | 66 (64.1) | - |
| Transplant | 15 (16.0) | - |
| Ethnicity ‡ | ||
| Caucasian | 91 (82.0) | 102 (91.9) |
| African-Canadian | 2 (1.8) | 0 (0.0) |
| East Asian | 2 (1.8) | 2 (1.8) |
| Southeast Asian | 1 (0.9) | 1 (0.9) |
| First Nations/Métis/Inuit | 1 (0.9) | 2 (1.8) |
| South Asian | 1 (0.9) | 2 (1.8) |
| Arab | 3 (2.7) | 2 (1.8) |
| Latin American | 1 (0.9) | 2 (1.8) |
| Other/Mixed Race | 9 (8.1) | 0 (0.0) |
| All Survivors (n = 122) | Survivors of Parents with Chronic Pain (n = 29) | Survivors of Parents without Chronic Pain (n = 93) | p | Partial η2 | |
|---|---|---|---|---|---|
| Depressive symptoms † | 15.60 (8.29) | 17.40 (10.04) | 13.67 (5.55) | 0.011 | 0.061 |
| Anxiety symptoms † | 16.23 (7.81) | 16.72 (6.63) | 14.39 (6.25) | 0.138 | 0.036 |
| HRQL † | 75.35 (15.72) | 73.06 (16.03) | 76.96 (14.62) | 0.382 | 0.007 |
| Pain interference *,† | 0.00 (1.00) | 0.02 (1.02) | −0.03 (1.04) | 0.914 | 0.000 |
| PTSS **,† | 0.00 (1.00) | 0.26 (1.09) | −0.28 (0.62) | 0.002 | 0.091 †† |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patton, M.; Stokoe, M.; Forbes, C.; Nwaroh, C.; Noel, M.; Reynolds, K.; Schulte, F. The Intergenerational Transmission of Chronic Pain from Parents to Survivors of Childhood Cancer. Children 2020, 7, 246. https://0-doi-org.brum.beds.ac.uk/10.3390/children7110246
Patton M, Stokoe M, Forbes C, Nwaroh C, Noel M, Reynolds K, Schulte F. The Intergenerational Transmission of Chronic Pain from Parents to Survivors of Childhood Cancer. Children. 2020; 7(11):246. https://0-doi-org.brum.beds.ac.uk/10.3390/children7110246
Chicago/Turabian StylePatton, Michaela, Mehak Stokoe, Caitlin Forbes, Chidera Nwaroh, Melanie Noel, Kathleen Reynolds, and Fiona Schulte. 2020. "The Intergenerational Transmission of Chronic Pain from Parents to Survivors of Childhood Cancer" Children 7, no. 11: 246. https://0-doi-org.brum.beds.ac.uk/10.3390/children7110246