Does Sex Dimorphism Exist in Dysfunctional Movement Patterns during the Sensitive Period of Adolescence?

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
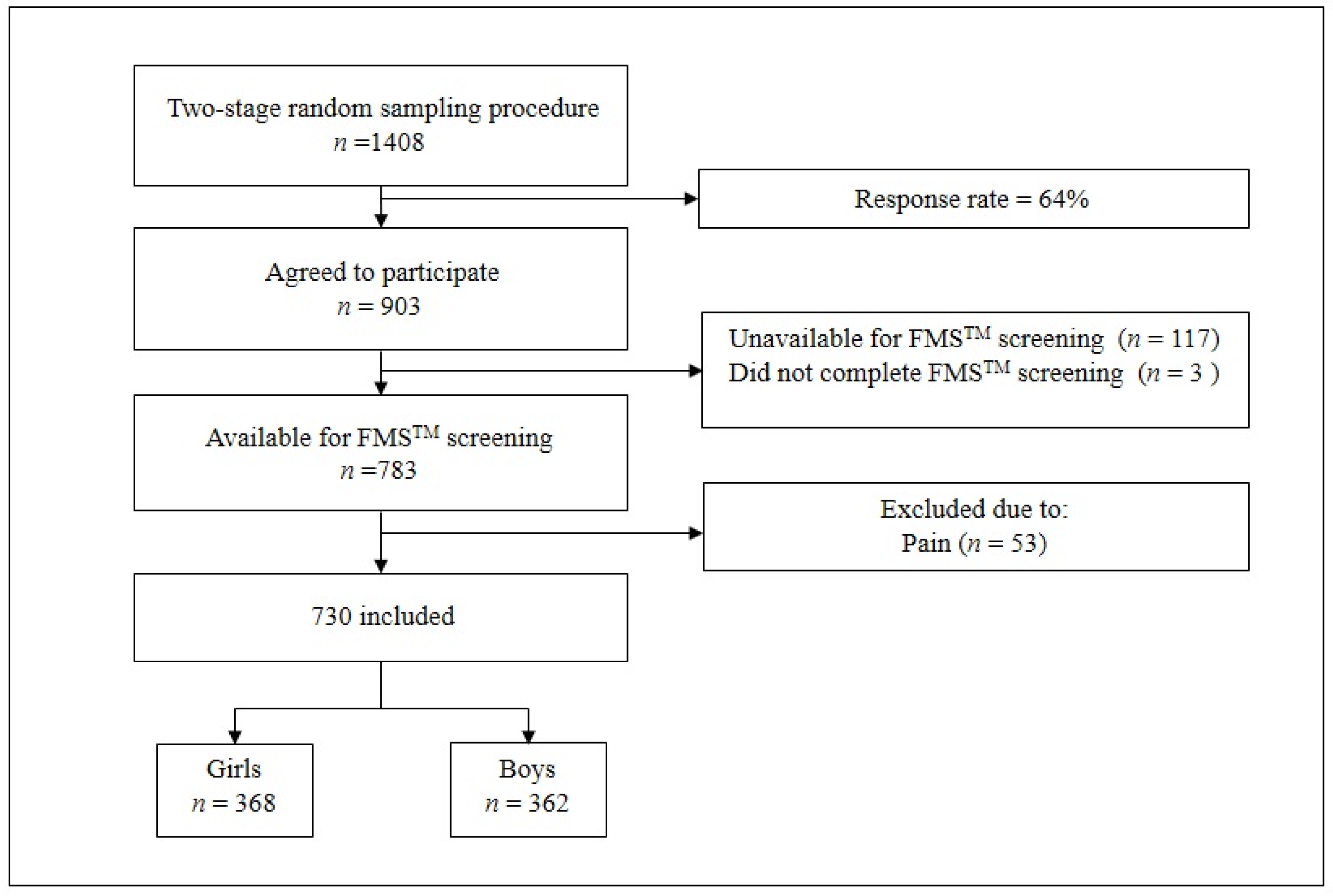
2.1. Participants
2.2. Functional Movement Screen
2.3. Sport Participation
2.4. Statistical Analysis
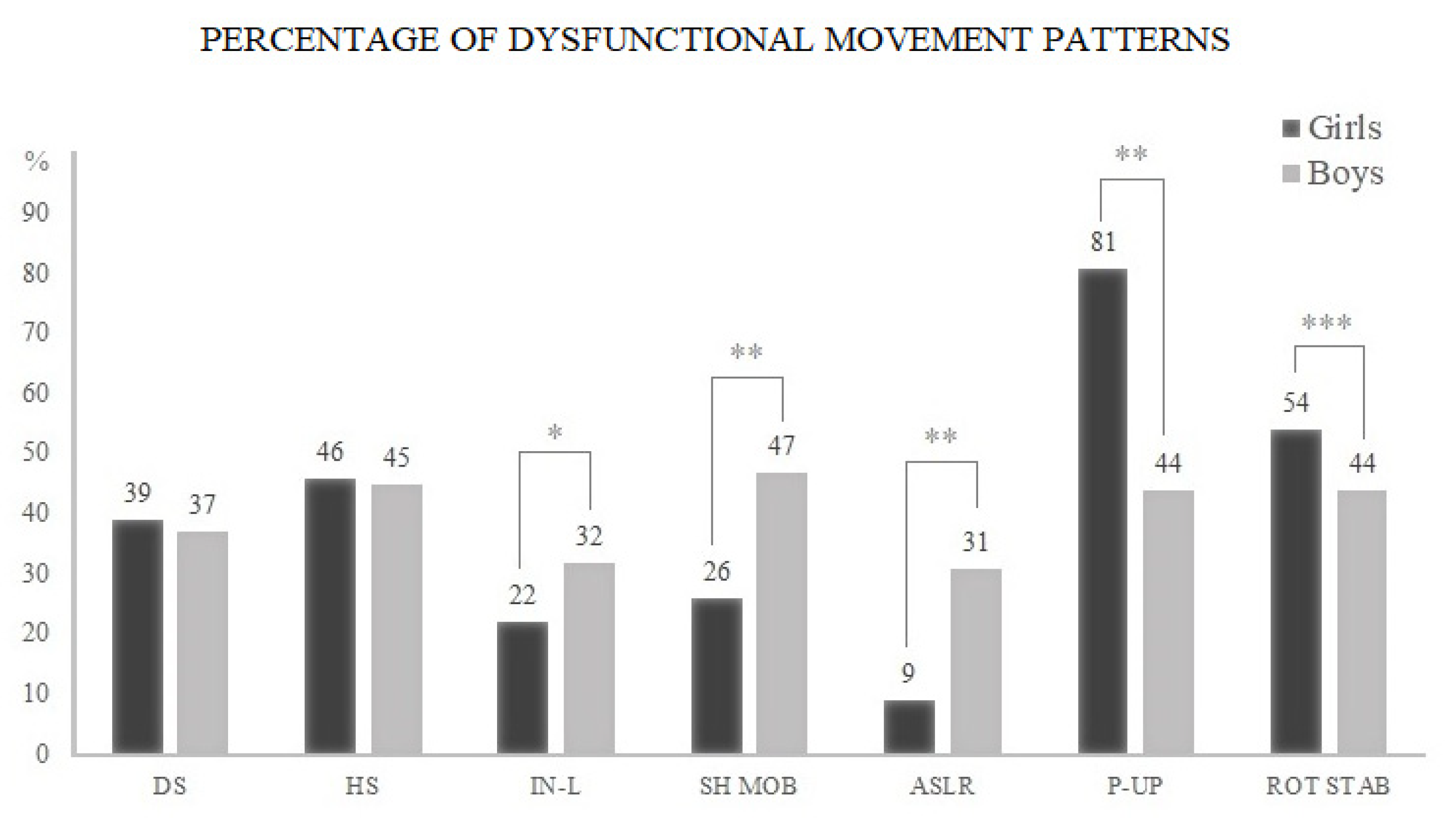
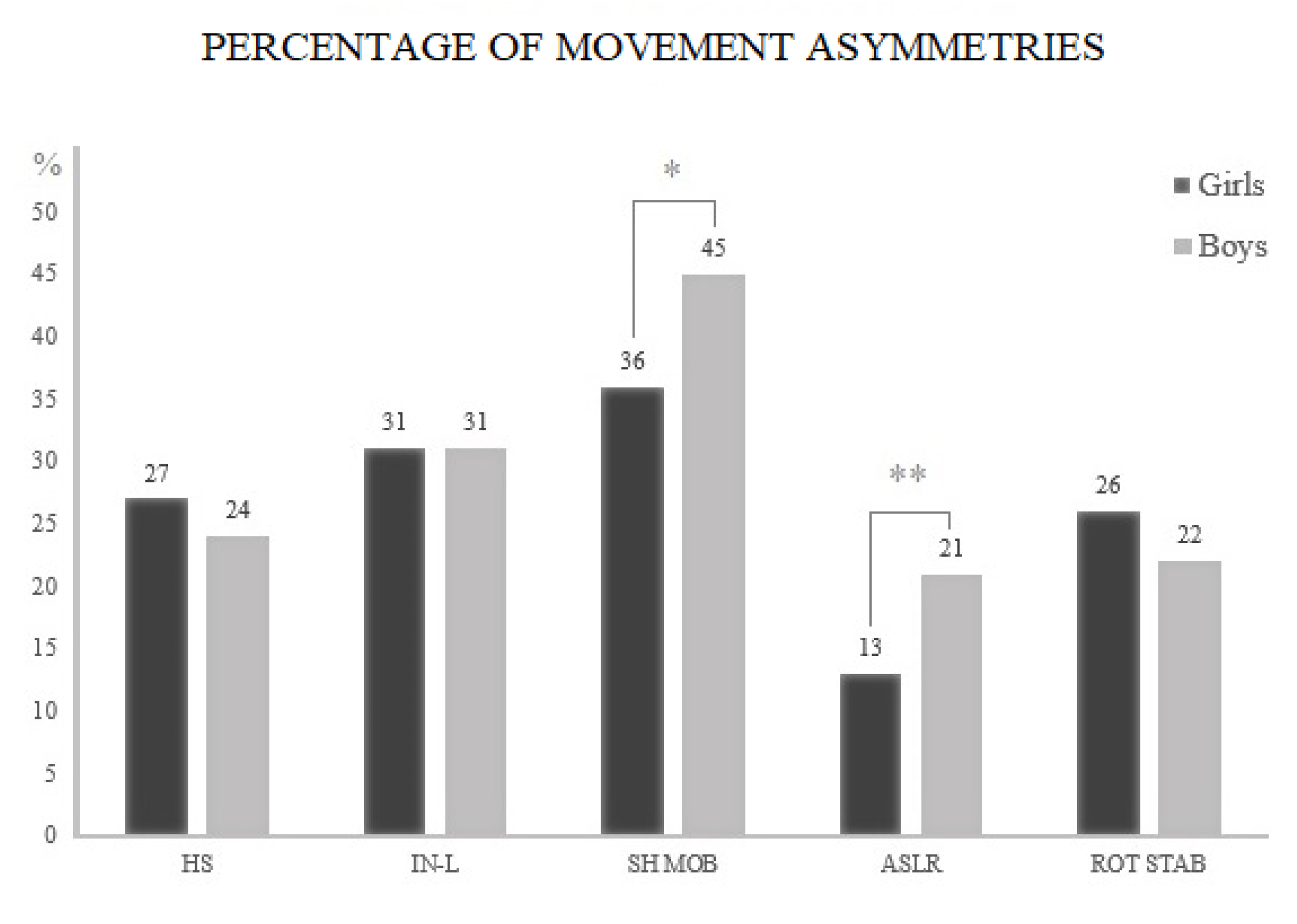
3. Results
Subgroup Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Warburton, D.; Charlesworth, S.; Ivey, A.; Nettlefold, L.; Bredin, S.S. A systematic review of the evidence for Canada’s Physical Activity Guidelines for Adults. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ekelund, U.; Anderssen, S.A.; Froberg, K.; Sardinha, L.N.; Andersen, L.B.; Brage, S. Independent associations of physical activity and cardiorespiratory fitness with metabolic risk factors in children: The European youth heart study. Diabetologia 2007, 50, 18320–18400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andersen, L.B.; Harro, M.; Sardinha, L.B.; Froberg, K.; Ekelund, U.; Brage, S.; Anderssen, S.A. Physical activity and clustered cardiovascular risk in children: A cross-sectional study (The European Youth Heart Study). Lancet 2006, 368, 299–304. [Google Scholar] [CrossRef]
- Ondrak, K.S.; Morgan, D.W. Physical Activity, Calcium Intake and Bone Health in Children and Adolescents. Sports Med. 2007, 37, 587–600. [Google Scholar] [CrossRef]
- Chalmers, S.; Fuller, J.T.; De Benedictis, T.A.; Townsley, S.; Lynagh, M.; Gleeson, C.; Zacharia, A.; Thomson, S.; Magarey, M. Asymmetry during preseason Functional Movement Screen testing is associated with injury during a junior Australian football season. J. Sci. Med. Sport 2017, 20, 653–657. [Google Scholar] [CrossRef]
- Anderson, B.E.; Neumann, M.L.; Bliven, K.C.H. Functional Movement Screen Differences Between Male and Female Secondary School Athletes. J. Strength Cond. Res. 2015, 29, 1098–1106. [Google Scholar] [CrossRef]
- Molina-Garcia, P.; Migueles, J.H.; Cadenas-Sanchez, C.; Esteban-Cornejo, I.; Mora-Gonzalez, J.; Rodriguez-Ayllon, M.; Plaza-Florido, A.; Molina-Molina, A.; Garcia-Delgado, G.; D’Hondt, E.; et al. Fatness and fitness in relation to functional movement quality in overweight and obese children. J. Sports Sci. 2019, 37, 878–885. [Google Scholar] [CrossRef]
- Paszkewicz, J.R.; Mccarty, C.W.; Van Lunen, B. Comparison of Functional and Static Evaluation Tools among Adolescent Athletes. J. Strength Cond. Res. 2013, 27, 2842–2850. [Google Scholar] [CrossRef]
- Kramer, T.A.; Sacko, R.S.; Pfeifer, C.E.; Gatens, D.R.; Goins, J.M.; Stodden, D.F. The association between the Functional Movement Screen™, Y-balance test, and physical performance tests in male and female high school athletes. Int. J. Sports Phys. Ther. 2019, 14, 911–919. [Google Scholar] [CrossRef]
- Pfeifer, C.E.; Sacko, R.S.; Ortaglia, A.; Monsma, E.V.; Beattie, P.F.; Goins, J.; Stodden, D.F. Functional movement Screen™ in youth sport participants: Evaluating the proficiency barrier for injury. Int. J. Sports Phys. Ther. 2019, 14, 436–444. [Google Scholar] [CrossRef]
- Mitchell, U.H.; Johnson, A.W.; Adamson, B. Relationship Between Functional Movement Screen Scores, Core Strength, Posture, and Body Mass Index in School Children in Moldova. J. Strength Cond. Res. 2015, 29, 1172–1179. [Google Scholar] [CrossRef] [PubMed]
- Duncan, M.J.; Stanley, M. Functional Movement Is Negatively Associated with Weight Status and Positively Associated with Physical Activity in British Primary School Children. J. Obes. 2012, 2012, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Duncan, M.J.; Stanley, M.; Leddington-Wright, S. The association between functional movement and overweight and obesity in British primary school children. Sports Med. Arthrosc. Rehabil. Ther. Technol. 2013, 5, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abraham, A.; Sannasi, R.; Nair, R. Normative values for the functional movement Screen™ in adolescent school aged children. Int. J. Sports Phys. Ther. 2015, 10, 29–36. [Google Scholar] [PubMed]
- García-Pinillos, F.; Roche-Seruendo, L.E.; Delgado-Floody, P.; Mayorga, D.J.; Latorre-Román, P.Á. Original is there any relationship between functional movement and weight status. Nutr. Hosp. 2018, 35, 805–810. [Google Scholar] [CrossRef]
- O’Brien, W.; Duncan, M.J.; Farmer, O.; Lester, D. Do Irish Adolescents Have Adequate Functional Movement Skill and Confidence? J. Mot. Learn. Dev. 2018, 6, S301–S319. [Google Scholar] [CrossRef]
- Cook, G.; Burton, L.; Hoogenboom, B. Pre-Participation Screening: The Use of Fundamental Movements as an Assessment of Function—Part 1. N. Am. J. Sport. Phys. Ther. 2006, 1, 62–72. [Google Scholar] [CrossRef]
- Cook, G.; Burton, L.; Hoogenboom, B. Pre-Participation Screening: The Use of Fundamental Movements as an Assessment of Function—Part 2. N. Am. J. Sport. Phys. Ther. 2006, 1, 132–139. [Google Scholar] [CrossRef]
- Kiesel, K.B.; Butler, R.J.; Plisky, P.J. Prediction of Injury by Limited and Asymmetrical Fundamental Movement Patterns in American Football Players. J. Sport Rehabil. 2014, 23, 88–94. [Google Scholar] [CrossRef]
- Garrison, M.; Westrick, R.; Johnson, M.R.; Benenson, J. Association between the functional movement screen and injury development in college athletes. Int. J. Sports Phys. Ther. 2015, 10, 21–28. [Google Scholar]
- Letafatkar, A.; Hadadnezhad, M.; Shojaedin, S.; Mohamadi, E. Relationship between functional movement screening score and history of injury. Int. J. Sports Phys. Ther. 2014, 9, 21–27. [Google Scholar] [PubMed]
- Dossa, K.; Cashman, G.; Howitt, S.; West, B.; Murray, N. Can injury in major junior hockey players be predicted by a pre-season functional movement screen—A prospective cohort study. J. Can. Chiropr. Assoc. 2014, 58, 421–427. [Google Scholar] [PubMed]
- Bardenett, S.M.; Micca, J.J.; De Noyelles, J.T.; Miller, S.D.; Jenk, D.T.; Brooks, G.S. Functional Movement Screen Normative Values and Validity in High School Athletes: Can the FmsTM be Used as a Predictor of Injury? Int. J. Sports Phys. Ther. 2015, 10, 303–308. [Google Scholar] [PubMed]
- Dorrel, B.S.; Long, T.; Shaffe, S.; Myer, G.D. Evaluation of the Functional Movement Screen as an Injury Prediction Tool among Active Adult Populations: A Systematic Review and Meta-analysis. Sports Health 2015, 7, 532–537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quatman-Yates, C.C.; Quatman, C.E.; Meszaros, A.J.; Paterno, M.V.; Hewett, T.E. A systematic review of sensorimotor function during adolescence: A developmental stage of increased motor awkwardness? Br. J. Sports Med. 2012, 46, 649–655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Štefan, L.; Sorić, M.; Devrnja, A.; Podnar, H.; Mišigoj-Duraković, M. Is school type associated with objectively measured physical activity in 15-year-olds? Int. J. Environ. Res. Public Health 2017, 14, 1417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gulgin, H.; Hoogenboom, B. The Functional Movement screening (FMSTM): An Inter-rater Reliability Study between Raters of Varied Experience. Int. J. Sports. Phys. Ther. 2014, 9, 14–20. [Google Scholar]
- Teyhen, D.S.; Shaffer, S.W.; Lorenson, C.L.; Halfpap, J.P.; Donofry, D.F.; Walker, M.J.; Dugan, J.L.; Childs, J.D. The Functional Movement Screen: A Reliability Study. J. Orthop. Sports Phys. Ther. 2012, 42, 530–540. [Google Scholar] [CrossRef] [Green Version]
- Sterling, M.; Jull, G.; Wright, A. The effect of musculoskeletal pain on motor activity and control. J. Pain 2001, 2, 135–145. [Google Scholar] [CrossRef]
- Bernard, J.; Bard, R.; Pujol, À.; Combey, A.; Boussard, D.; Begué, C.; Salghetti, A. Muscle assessment in healthy teenagers, Comparison with teenagers with low back pain. Ann. Readapt. Med. Phys. 2008, 51, 263–283. [Google Scholar] [CrossRef]
- Jansson, A.; Saartok, T.; Werner, S.; Renstrom, P. General joint laxity in 1845 Swedish school children of different ages: Age and gender-specific distributions. Acta Paediatr. 2004, 93, 1202–1206. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Campos, R.; Andruske, C.L.; Arruda, M.; Sulla-Torres, J.; Pacheco-Carrillo, J.; Urra-Albornoz, C.; Cossio-bolaños, M. Normative data for handgrip strength in children and adolescents in the Maule Region, Chile: Evaluation based on chronological and biological age. PLoS ONE 2018, 13, e0201033. [Google Scholar] [CrossRef] [PubMed]
- Shultz, S.J.; Nguyen, A.D.; Schmitz, R.J. Differences in Lower Extremity Anatomical and Postural Characteristics in Males and Females between Maturation Groups. J. Orthop. Sports Phys. Ther. 2008, 38, 137–149. [Google Scholar] [CrossRef] [PubMed]
- Huseynov, A.; Zollikofer, C.P.; Coudyzer, W.; Gascho, D.; Kellenberger, C.; Hinzpeter, R.; De León, M.S.P. Developmental evidence for obstetric adaptation of the human female pelvis. Proc. Natl. Acad. Sci. USA 2016, 113, 5227–5232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peterson, J.B.; Doan, J.; Bomar, J.D.; Wenger, D.R.; Pennock, A.T.; Upasani, V.V. Sex Differences in Cartilage Topography and Orientation of the Developing Acetabulum: Implications for Hip Preservation Surgery. Clin. Orthop. Relat. Res. 2015, 473, 2489–2494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hooper, P.; Oak, S.R.; Lynch, T.S.; Ibrahim, G.; Goodwin, R.; Rosneck, J. Adolescent Femoroacetabular Impingement: Gender Differences in Hip Morphology. Arthrosc. J. Arthrosc. Relat. Surg. 2016, 32, 2495–2502. [Google Scholar] [CrossRef] [PubMed]
- Slater, A.; Tiggemann, M. Gender differences in adolescent sport participation, teasing, self-objectification and body image concerns. J. Adolesc. 2011, 34, 455–463. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Basic Characteristics | Girls | Boys | |
|---|---|---|---|
| BMI (kg/m2) Mean (SD) | 21.7 (3.2) | 22.4 (3.5) | |
| Waist Circumference (cm) Mean (SD) | 68.7 (6.4) | 76.0 (7.5) | |
| Hips Circumference (cm) Mean (SD) | 96.7 (7.5) | 98.0 (7.5) | |
| Sum of Four Skinfolds (mm) Mean (SD) | 48.8 (15.0) | 37.1 (18.1) | |
| Functional Movement Asymmetries n (%) | 0 | 76 (21) | 86 (23) |
| 1 | 128 (35) | 126 (34) | |
| 2 | 98 (27) | 111 (30) | |
| 3 | 51 (14) | 38 (10) | |
| 4 | 7 (2) | 7 (2) | |
| 5 | 2 (0.5) | 0 (0) | |
| Sport Participation * n (%) | 93 (25) | 173 (48) | |
| SES Median (IQR) | 3 (1) | 2 (1) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karuc, J.; Jelčić, M.; Sorić, M.; Mišigoj-Duraković, M.; Marković, G. Does Sex Dimorphism Exist in Dysfunctional Movement Patterns during the Sensitive Period of Adolescence? Children 2020, 7, 308. https://0-doi-org.brum.beds.ac.uk/10.3390/children7120308
Karuc J, Jelčić M, Sorić M, Mišigoj-Duraković M, Marković G. Does Sex Dimorphism Exist in Dysfunctional Movement Patterns during the Sensitive Period of Adolescence? Children. 2020; 7(12):308. https://0-doi-org.brum.beds.ac.uk/10.3390/children7120308
Chicago/Turabian StyleKaruc, Josip, Mario Jelčić, Maroje Sorić, Marjeta Mišigoj-Duraković, and Goran Marković. 2020. "Does Sex Dimorphism Exist in Dysfunctional Movement Patterns during the Sensitive Period of Adolescence?" Children 7, no. 12: 308. https://0-doi-org.brum.beds.ac.uk/10.3390/children7120308