Usefulness of Gastrojejunostomy Prior to Fundoplication in Severe Gastro-Esophageal Reflux Complicating Long-Gap Esophageal Atresia Repair: A Preliminary Study

 , and
, and
Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Surgical Management
3. Methods
3.1. TGJ Insertion
3.2. Nutritional Planning
3.3. Post-Surgical Monitoring
- (1)
- weight increases after the placement of the jejunal tube, at the time of fundoplication surgery. Bodyweight was measured with a beam scale and it was used as the most sensitive parameter to detect short-term weight variations;
- (2)
- the number of hospital admissions during a period ranging from 3 months before to 3 months after TGJ positioning;
- (3)
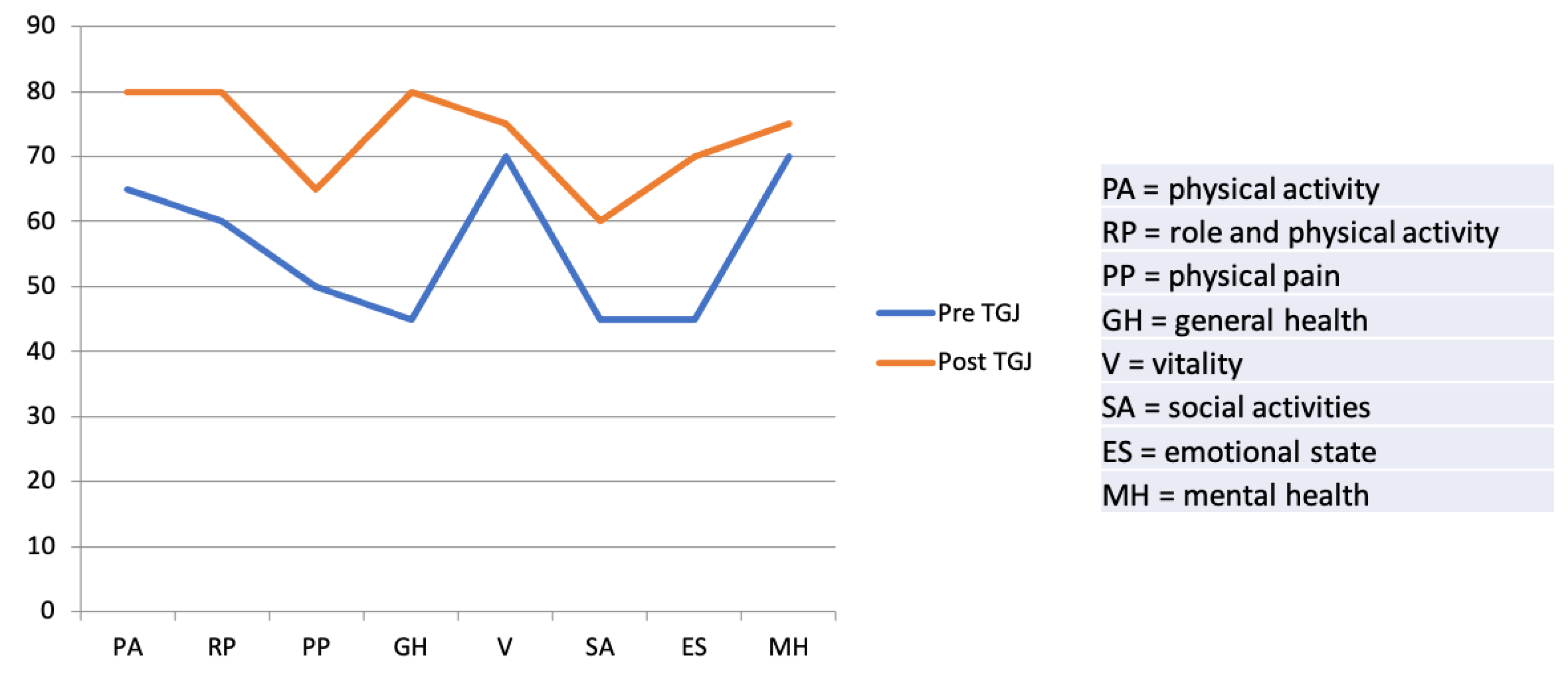
- parental quality of life (QoL) before and after TGJ positioning (by administration of Short-Form 36 questionnaire version 1.6 to parents before fundoplication). The questionnaire is a common patient-reported survey to assess the patients’ health. It is based on the evaluation of eight items: physical activity, role and physical activity, physical pain, general health, vitality, social activities, emotional state and mental health. Each item is associated with a score with a maximum value of 100; the lower the score, the more severe the disability.
4. Statistical Analysis
5. Results
5.1. Growth and Nutritional Aspects
5.2. Post-Surgical Monitoring
5.3. Parental Quality of Life
6. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Van der Zee, D.C.; Bagolan, P.; Faure, C.; Gottrand, F.; Jennings, R.; Laberge, J.M.; Martinez Ferro, M.H.; Parmentier, B.; Sfeir, R.; Teague, W. Position Paper of INoEA Working Group on Long-Gap Esophageal Atresia: For Better Care. Front. Pediatr. 2017, 31, 63. [Google Scholar] [CrossRef] [Green Version]
- Stadil, T.; Koivusalo, A.; Pakarinen, M.; Mikkelsen, A.; Emblem, R.; Svensson, J.F.; Ehrén, H.; Jönsson, L.; Bäckstrand, J.; Lilja, H.E.; et al. Surgical repair of long-gap esophageal atresia: A retrospective study comparing the management of long-gap esophageal atresia in the Nordic countries. J. Pediatr. Surg. 2019, 54, 423–428. [Google Scholar] [CrossRef] [PubMed]
- Puri, P.; Khurana, S. Delayed primary esophageal anastomosis for pure esophageal atresia. Semin. Pediatr. Surg. 1998, 7, 126–129. [Google Scholar] [CrossRef]
- Friedmacher, F.; Puri, P. Delayed primary anastomosis for management of long-gap esophageal atresia: A meta-analysis of complications and long-term outcome. Pediatr. Surg. Int. 2012, 28, 899–906. [Google Scholar] [CrossRef]
- Holland, A.J.; Ron, O.; Pierro, A.; Drake, D.; Curry, J.I.; Kiely, E.M.; Spitz, L. Surgical outcomes of esophageal atresia without fistula for 24 years at a single institution. J. Pediatr. Surg. 2009, 44, 1928–1932. [Google Scholar] [CrossRef]
- Burjonrappa, S.; Thiboutot, E.; Castilloux, J.; St-Vil, D. Type a esophageal atresia: A critical review of management strategies at a single center. J. Pediatr. Surg. 2010, 45, 865–871. [Google Scholar] [CrossRef]
- Conforti, A.; Valfré, L.; Falbo, M.; Bagolan, P.; Cerchiari, A. Feeding and Swallowing Disorders in Esophageal Atresia Patients: A Review of a Critical Issue. Eur. J. Pediatr. Surg. 2015, 25, 318–325. [Google Scholar] [CrossRef]
- Zani, A.; Cobellis, G.; Wolinska, J.; Chiu, P.P.; Pierro, A. Preservation of native esophagus in infants with pure esophageal atresia has good long-term outcomes despite significant postoperative morbidity. Pediatr. Surg. Int. 2016, 32, 113–117. [Google Scholar] [CrossRef]
- Fenton, T.R.; Kim, J.H. A systematic review and meta-analysis to revise the Fenton growth chart for preterm infants. BMC Pediatr. 2013, 20, 59. [Google Scholar] [CrossRef] [Green Version]
- Van der Zee, D.C.; Tytgat, S.H.A.; van Herwaarden, M.Y.A. Esophageal atresia and tracheo-esophageal fistula. Semin. Pediatr. Surg. 2017, 26, 67–71. [Google Scholar] [CrossRef]
- Van der Zee, D.C.; Gallo, G.; Tytgat, S.H. Thoracoscopic traction technique in long gap esophageal atresia: Entering a new era. Surg. Endosc. 2015, 29, 3324–3330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, K.M.; Krosch, T.C.; Eickhoff, J.C.; Sabati, A.A.; Brudney, J.; Rivard, A.L.; Foker, J.E. Achievement of feeding milestones after primary repair of long-gap esophageal atresia. Early Hum. Dev. 2009, 85, 387–392. [Google Scholar] [CrossRef]
- Briefel, R.R.; Reidy, K.; Karwe, V.; Jankowski, L.; Hendricks, K. Toddlers’ transition to table foods: Impact on nutrient intakes and food patterns. J. Am. Diet Assoc. 2004, 104, S38–S44. [Google Scholar] [CrossRef] [PubMed]
- Simpson, C.; Schanler, R.J.; Lau, C. Early introduction of oral feeding in preterm infants. Pediatrics 2002, 110, 517–522. [Google Scholar] [CrossRef] [PubMed]
- Somppi, E.; Tammela, O.; Ruuska, T.; Rahnasto, J.; Laitinen, J.; Turjanmaa, V.; Järnberg, J. Outcome of patients operated on for esophageal atresia: 30 years’ experience. J. Pediatr. Surg. 1998, 33, 1341–1346. [Google Scholar] [CrossRef]
- Koivusalo, A.I.; Rintala, R.J.; Pakarinen, M.P. Outcomes of fundoplication in oesophageal atresia associated gastrooesophageal reflux disease. J. Pediatr. Surg. 2018, 53, 230–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mason, S.J.; Harris, G.; Blissett, J. Tube feeding in infancy: Implications for the development of normal eating and drinking skills. Dysphagia 2005, 20, 46–61. [Google Scholar] [CrossRef] [PubMed]
- Morris, S.E.; Klein, M.D. Pre-Feeding Skills: A Comprehensive Resource for Mealtime Development, 2nd ed.; PRO-ED: Austin, TX, USA, 2000. [Google Scholar]
- Puntis, J.W. Gastro-oesophageal reflux in young babies: Who should be treated? Arch. Dis. Child. 2015, 100, 989–993. [Google Scholar] [CrossRef]
- Lifschitz, C. Thinking outside the box when dealing with patients with GERD and feeding problems. J. Pediatr. Gastroenterol. Nutr. 2011, 53, 358. [Google Scholar] [CrossRef]
- Duca, A.P.; Dantas, R.O.; Rodrigues, A.A.; Sawamura, R. Evaluation of swallowing in children with vomiting after feeding. Dysphagia 2008, 23, 177–182. [Google Scholar] [CrossRef]
- Folaranmi, S.E.; Jawaid, W.B.; Gavin, L.; Jones, M.O.; Losty, P.D. Influence of birth weight on primary surgical management of newborns with esophageal atresia. J. Pediatr. Surg. 2020, 28. [Google Scholar] [CrossRef]
- Bairdain, S.; Zurakowski, D.; Vargas, S.O.; Stenquist, N.; McDonald, M.; Towne, M.C.; Miller, D.T.; Jennings, R.W.; Kantor, D.B.; Agrawal, P.B. Long-Gap Esophageal Atresia Is a Unique Entity within the Esophageal Atresia Defect Spectrum. Neonatology 2017, 111, 140–144. [Google Scholar] [CrossRef] [Green Version]
- Michaud, L.; Coopman, S.; Guimber, D.; Sfeir, R.; Turck, D.; Gottrand, F. Percutaneous gastrojejunostomy in children: Efficacy and safety. Arch. Dis. Child. 2012, 97, 733–734. [Google Scholar] [CrossRef]
- Al-Zubeidi, D.; Demir, H.; Bishop, W.P.; Rahhal, R.M. Gastrojejunal feeding tube use by gastroenterologists in a pediatric academic center. J. Pediatr. Gastroenterol. Nutr. 2013, 56, 523–527. [Google Scholar] [CrossRef] [PubMed]
- Egnell, C.; Eksborg, S.; Grahnquist, L. Jejunostomy enteral feeding in children: Outcome and safety. JPEN J. Parenter. Enteral. Nutr. 2014, 38, 631–636. [Google Scholar] [CrossRef] [PubMed]
- Fascetti-Leon, F.; El Agami, H.; Gobbi, D.; Clarke, S.; Haddad, M.; Choudhry, M. Feeding Jejunostomy: Is It a Safe Route in Pediatric Patients? Single Institution Experience. Eur. J. Pediatr. Surg. 2018, 28, 293–296. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, U.; Mousa, H.; Dall’Oglio, L.; Homaira, N.; Rosen, R.; Faure, C.; Gottrand, F. ESPGHAN-NASPGHAN Guidelines for the Evaluation and Treatment of Gastrointestinal and Nutritional Complications in Children With Esophageal Atresia-Tracheoesophageal Fistula. J. Pediatr. Gastroenterol. Nutr. 2016, 63, 550–570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gottrand, F.; Sullivan, P.B. Gastrostomy tube feeding: When to start, what to feed and how to stop. Eur. J. Clin. Nutr. 2010, 64, S17–S21. [Google Scholar] [CrossRef]
- Godbole, P.; Margabanthu, G.; Crabbe, D.C.; Thomas, A.; Puntis, J.W.; Abel, G.; Arthur, R.J.; Stringer, M.D. Limitations and uses of gastrojejunal feeding tubes. Arch. Dis. Child. 2002, 86, 134–137. [Google Scholar] [CrossRef] [Green Version]
- Fortunato, J.E.; Darbari, A.; Mitchell, S.E.; Thompson, R.E.; Cuffari, C. The limitations of gastro-jejunal (G-J) feeding tubes in children: A 9-year pediatric hospital database analysis. Am. J. Gastroenterol. 2005, 100, 186–189. [Google Scholar] [CrossRef]
- Romeo, C.; Bonanno, N.; Baldari, S.; Centorrino, A.; Scalfari, G.; Antonuccio, P.; Centonze, A.; Gentile, C. Gastric motility disorders in patients operated on for esophageal atresia and tracheoesophageal fistula: Long-term evaluation. J. Pediatr. Surg. 2000, 35, 740–744. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Patient | Sex | Gestational Age (Term/Preterm) | Birth Weight, kg (Z-Score) 1 | EA Type | Associated Anomalies |
|---|---|---|---|---|---|
| 1 | M | Term | 3.1 (−0.77) | A | Aberrant right subclavian artery; severe tracheomalacia |
| 2 | M | Term | 2.9 (−1.23) | A | Cardiac anomaly |
| 3 | F | Preterm * | 1.3 (−2.22) | A | Cardiac anomaly |
| 4 | M | Preterm | 2.1 (−1.01) | C | IVs adrenal neuroblastoma |
| 5 | F | Preterm | 1.4 (−1.37) | C | ARM, right-sided aorta |
| 6 | F | Preterm | 1.5 (−1.85) | A | VACTER; palatoschisis |
| 7 | M | Term | 3.2 (−0.55) | A | Tracheomalacia; congenital airways malformation |
| Patient | Type of EA | Long Gap (Vertebral Bodies) | Type of Anastomosis | EGJ Position after Esophageal Anastomosis | EGJ Position after Fundoplication | Post-Surgical Complications |
|---|---|---|---|---|---|---|
| 1 | A | 5 | -Thoracic elongation -Delayed primary anastomosis | 3 vertebral bodies above the diaphragm | N/A | Anastomotic stenosis; GER; intrathoracic EGJ; short esophagus |
| 2 | A | 4 | -Thoracic elongation -Delayed primary anastomosis | 3 vertebral bodies above the diaphragm | 2.5 intercostal spaces above the diaphragm | Anastomotic stenosis; GER; intrathoracic EGJ; short esophagus |
| 3 | A | 6 | -Jejunal interposition | - | - | Anastomotic stenosis; GER; short esophagus |
| 4 | C | 4 | -Thoracic elongation -Gastric pull-up * | 2 vertebral bodies above the diaphragm | 1.5 intercostal spaces above the diaphragm | Anastomotic stenosis; GER; intrathoracic EGJ |
| 5 | C | 3 | -Thoracic elongation -Delayed primary anastomosis | 2 vertebral bodies above the diaphragm | 1.5 vertebral bodies above diaphragm | no |
| 6 | A | 6 | -Gastric transposition * | - | - | Anastomotic stenosis; GER; intrathoracic EGJ; short esophagus |
| 7 | C | 3 | -Gastric pull-up * | 2 vertebral bodies above the diaphragm | 2 intercostal spaces above the diaphragm | Anastomotic stenosis; GER; intrathoracic EGJ; short esophagus |
| Patient | Gastrostomy | J-Tube-insertion | Fundoplication | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Age (days) | Weight (kg) | Weight z-score | Age (months) | Weight (kg) | Weight z-score | Age (months) | Weight (kg) | Weight z-score | |
| 1 | 1 | 3.1 | −0.77 | 4 | 5.3 | −2.4 | 4.8 | 5.5 | −2.1 |
| 2 | 2 | 2.9 | −1.23 | 5.9 | 5 | −2.6 | 16.5 | 7.5 | −2.3 |
| 3 | 1 | 1.3 | −2.22 | 2.9 | 3.7 | −2.5 | 5 | 5.4 | −2.0 |
| 4 | 1 | 2.1 | −1.01 | 2.8 | 4.6 | −1.5 | 5.5 | 5.8 | −2.3 |
| 5 | 1 | 1.4 | −1.37 | 3.8 | 3.7 | −3.5 | 4.8 | 3.8 | −4.2 |
| 6 | 1 | 1.5 | −1.85 | 10.9 | 5.3 | −4.0 | 17 | 6.5 | −3.7 |
| 7 | 1 | 3.2 | −0.55 | 2.1 | 5 | −0.9 | 6.3 | 6.2 | −2.2 |
| Patient | Admissions pre TGJ (n) | Admissions Post TGJ (n) | TGJ complications |
|---|---|---|---|
| 1 | 4 | 2 | None |
| 2 | 5 | 1 | None |
| 3 | 4 | 2 | Tube dislodgement (endoscopic repositioning) |
| 4 | 6 | 2 | Stoma care |
| 5 | 5 | 1 | None |
| 6 | 5 | 1 | None |
| 7 | 5 | 2 | Tube malfunction (replacement without anesthesia) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Destro, F.; Maestri, L.; Meroni, M.; Rebosio, F.; Del Re, G.; Mantegazza, C.; Calcaterra, V.; Pelizzo, G. Usefulness of Gastrojejunostomy Prior to Fundoplication in Severe Gastro-Esophageal Reflux Complicating Long-Gap Esophageal Atresia Repair: A Preliminary Study. Children 2021, 8, 55. https://0-doi-org.brum.beds.ac.uk/10.3390/children8010055
Destro F, Maestri L, Meroni M, Rebosio F, Del Re G, Mantegazza C, Calcaterra V, Pelizzo G. Usefulness of Gastrojejunostomy Prior to Fundoplication in Severe Gastro-Esophageal Reflux Complicating Long-Gap Esophageal Atresia Repair: A Preliminary Study. Children. 2021; 8(1):55. https://0-doi-org.brum.beds.ac.uk/10.3390/children8010055
Chicago/Turabian StyleDestro, Francesca, Luciano Maestri, Milena Meroni, Federico Rebosio, Giulia Del Re, Cecilia Mantegazza, Valeria Calcaterra, and Gloria Pelizzo. 2021. "Usefulness of Gastrojejunostomy Prior to Fundoplication in Severe Gastro-Esophageal Reflux Complicating Long-Gap Esophageal Atresia Repair: A Preliminary Study" Children 8, no. 1: 55. https://0-doi-org.brum.beds.ac.uk/10.3390/children8010055