
A Case of Prenatally Diagnosed Uhl’s Anomaly with Absent Pulmonary Valve Leaflets and Dysplastic Tricuspid Valve

 , , ,
, , , {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
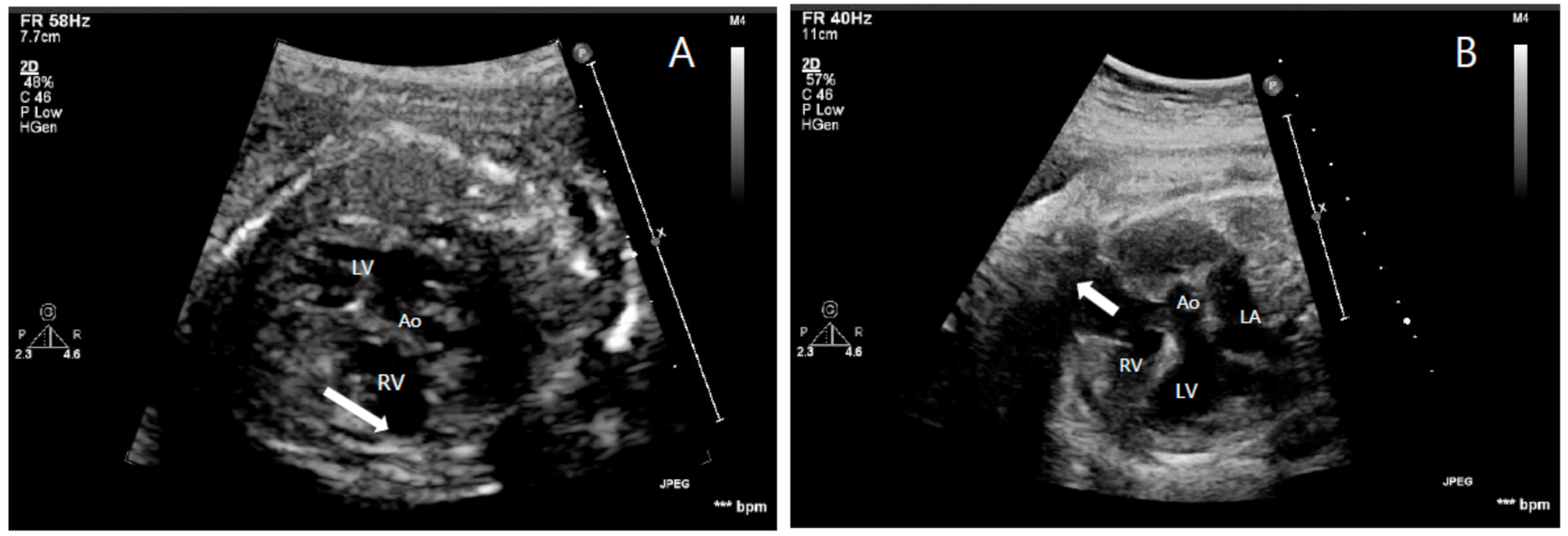
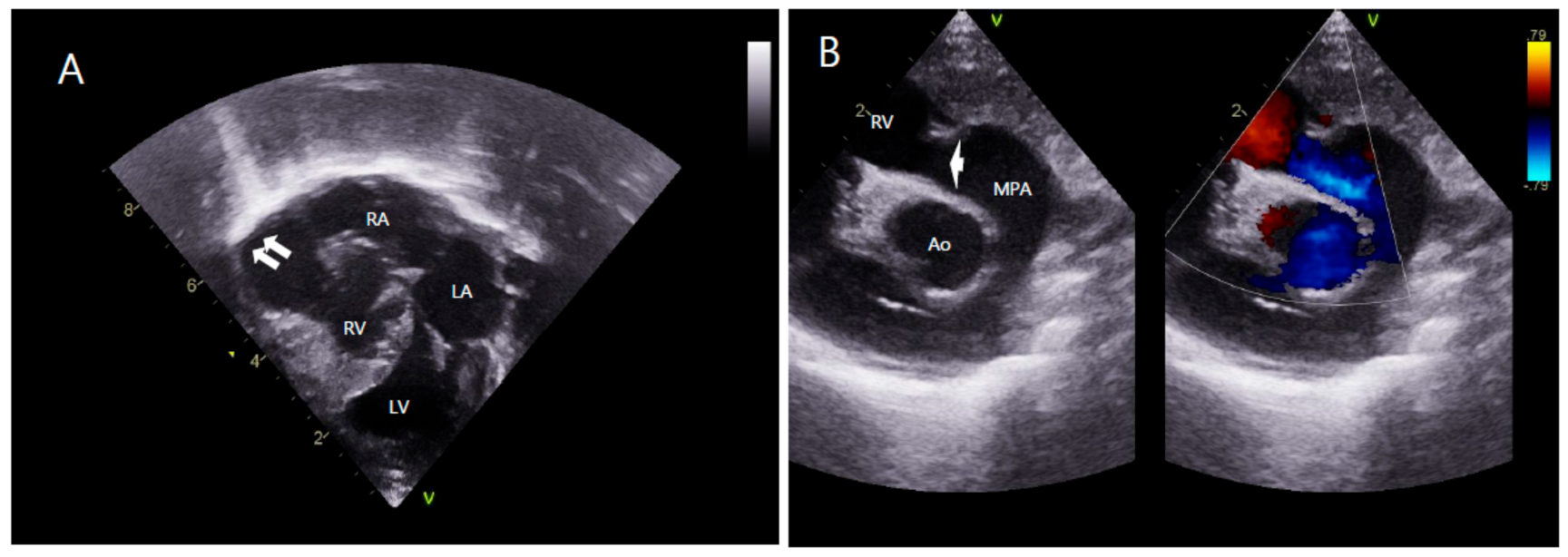
2. Case Report
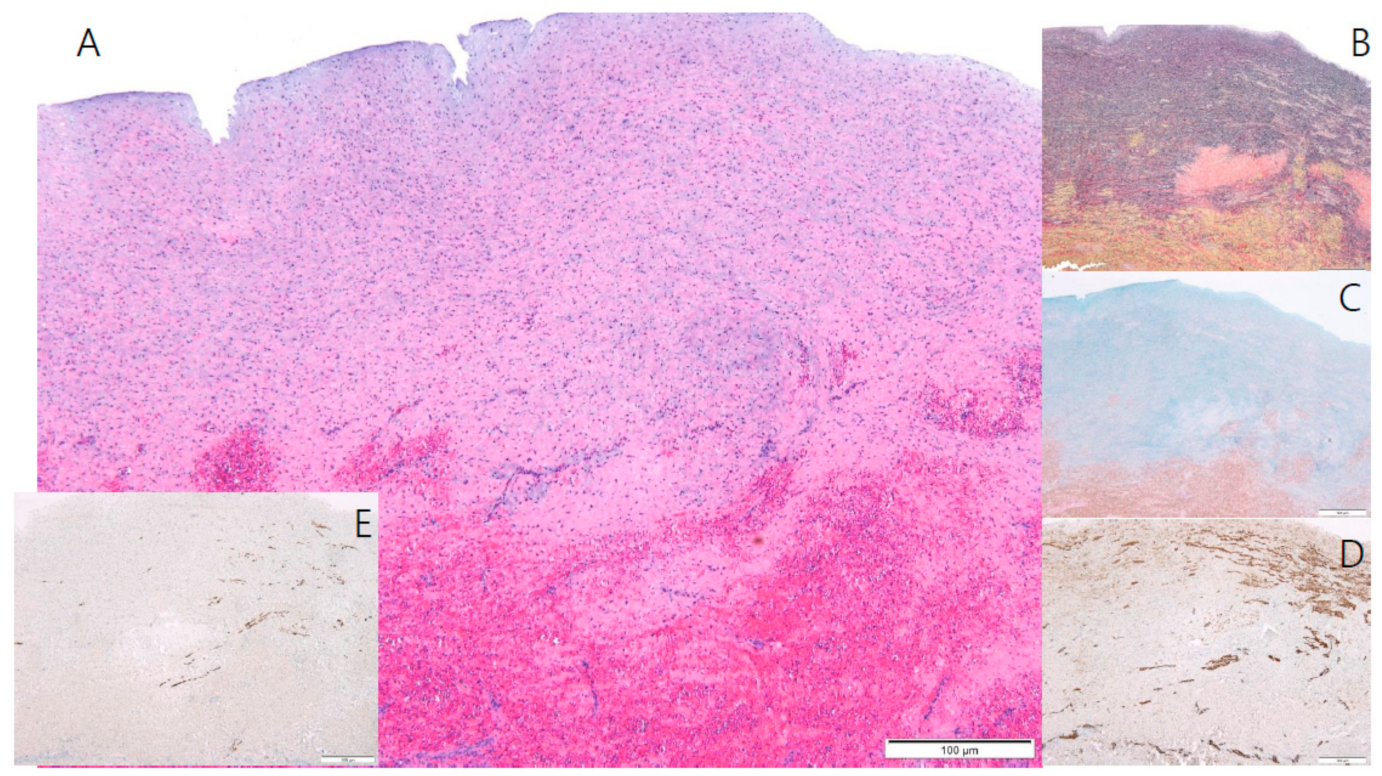
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Uhl, H.S. A previously undescribed congenital malformation of the heart: Almost total absence of the myocardium of the right ventricle. Bull. Johns Hopkins Hosp. 1952, 91, 197–209. [Google Scholar]
- Uhl, H.S. Uhl’s anomaly revisited. Circulation 1996, 93, 1483–1484. [Google Scholar] [CrossRef]
- Van der Palen, R.L.; van der Wal, A.C.; Robles de Medina, P.G.; Blom, N.A.; Clur, S.A. Uhl’s anomaly: Clinical spectrum and pathophysiology. Int. J. Cardiol. 2016, 209, 118–121. [Google Scholar] [CrossRef]
- Osler, W.M. The Principles and Practice of Medicine, 6th ed.; D. Appleton: New York, NY, USA, 1905; p. 280. [Google Scholar]
- Gerlis, L.M.; Schmidt-Ott, S.C.; Ho, S.Y.; Anderson, R.A. Dysplastic conditions of the right ventricular myocardium: Uhl’s anomaly vs arrhythmogenic right ventricular dysplasia. Br. Heart J. 1993, 69, 142–150. [Google Scholar] [CrossRef] [PubMed]
- Mihos, C.G.; Larrauri-Reyes, M.; Yucel, E.; Santana, O. Clinical presentation and echocardiographic characteristics of Uhl’s anomaly. Echocardiography 2017, 34, 299–302. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.F.; Mohammed, T.L.; Griffith, B.P.; White, C.S. CT of Uhl’s anomaly in an adult. Int. J. Cardiovasc. Imaging 2005, 21, 663–666. [Google Scholar] [CrossRef] [PubMed]
- Feucht, M.; Christ, B.; Wilting, J. VEGF induces cardiovascular malformation and embryonic lethality. Am. J. Pathol. 1997, 151, 1407–1416. [Google Scholar] [PubMed]
- Greer, M.L.; MacDonald, C.; Adatia, I. MRI of Uhl’s anomaly. Circulation 2000, 101, e230–e232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kilinc, M.; Akademir, I.; Sivasli, E. A case of Uhl’s anomaly presenting with severe right heart failure. Acta Cardiol. 2000, 55, 367–369. [Google Scholar] [CrossRef] [PubMed]
- Cammalleri, V.; Forcina, M.; Pugliese, L.; Romeo, F.; Floris, R.; Chiochi, M. Uhl anomaly in asymptomatic adult woman. Circ. Cardiovasc. Imaging 2019, 12, e008277. [Google Scholar] [CrossRef] [PubMed]
- Otmani, A.; Leborgne, L.; Renard, C.; Bakkour, H.; Quenum, S.; Tribouilloy, C.; Rey, J.L. Images in cardiovascular medicine. Electrocardiogram, Echocardiography, and Magnetic resonance imaging characteristics in Uhl’s disease. Circulation 2007, 115, e11–e12. [Google Scholar] [CrossRef] [Green Version]
- Taksande, A.; Gautami, V. Uhl’s anomaly with absent tricuspid valve in an infant. J. Cardiovasc. Echogr. 2015, 25, 90–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azhari, N.; Assaqqat, M.; Bulbul, Z. Successful surgical repair of Uhl’s anomaly. Cardiol. Young 2002, 12, 192–195. [Google Scholar] [CrossRef] [PubMed]
- Yoshii, S.; Suzuki, S.; Hosaka, S.; Osawa, H.; Takahashi, W.; Takizawa, K.; Abraham, S.J.K.; Tada, Y.; Sugiyama, H.; Tan, T.; et al. A case of Uhl anomaly treated with one and a half ventricle repair combined with partial right ventriculectomy in infancy. J. Thorac. Cardiovasc. Surg. 2001, 122, 1026–1028. [Google Scholar] [CrossRef] [Green Version]
- Ikari, N.M.; Azeka, E.; Aiello, V.D.; Atik, E.; Barbero-Marcial, M.; Ebaid, M. Uhl’s anomaly. Differential diagnosis and indications for cardiac transplantation in an infant. Arq. Bras. Cardiol. 2001, 77, 69–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, T.; Ko, H.; Byun, J.-H.; Lee, H.D.; Kim, H.; Choi, K.; Na, J.-Y. A Case of Prenatally Diagnosed Uhl’s Anomaly with Absent Pulmonary Valve Leaflets and Dysplastic Tricuspid Valve. Children 2021, 8, 190. https://0-doi-org.brum.beds.ac.uk/10.3390/children8030190
Kim T, Ko H, Byun J-H, Lee HD, Kim H, Choi K, Na J-Y. A Case of Prenatally Diagnosed Uhl’s Anomaly with Absent Pulmonary Valve Leaflets and Dysplastic Tricuspid Valve. Children. 2021; 8(3):190. https://0-doi-org.brum.beds.ac.uk/10.3390/children8030190
Chicago/Turabian StyleKim, Taehong, Hoon Ko, Joung-Hee Byun, Hyoung Doo Lee, Hyungtae Kim, Kwangho Choi, and Joo-Young Na. 2021. "A Case of Prenatally Diagnosed Uhl’s Anomaly with Absent Pulmonary Valve Leaflets and Dysplastic Tricuspid Valve" Children 8, no. 3: 190. https://0-doi-org.brum.beds.ac.uk/10.3390/children8030190