
Quality Indicators in Pediatric Palliative Care: Considerations for Latin America


 ,
,
Abstract
:
1. Introduction
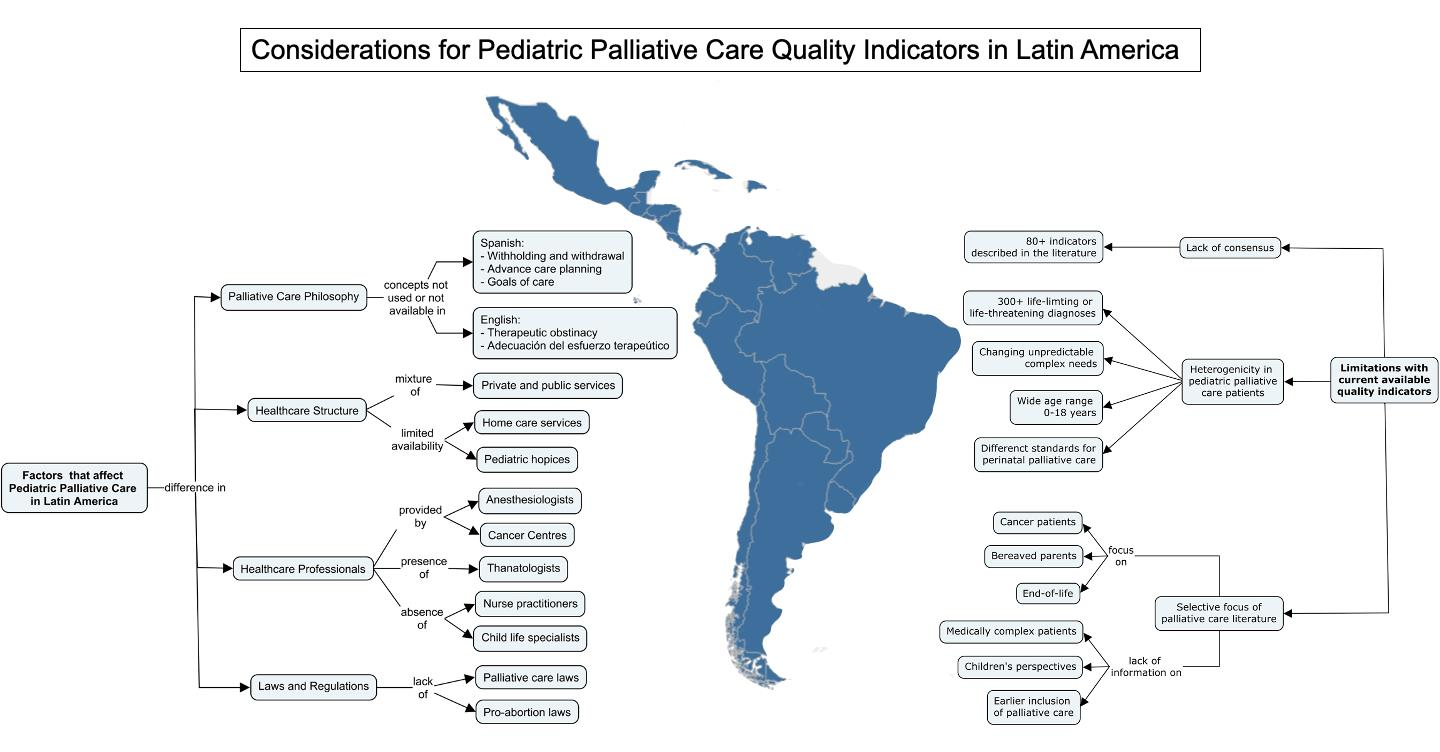
2. Contextual Factors That Influence PPC Development in LA
2.1. Palliative Care Philosophy
2.2. Healthcare Structure
2.3. Palliative Care Providers
2.4. Laws and Regulations in Palliative Care
3. Challenges of Implementing PPC Quality Indicators
3.1. Lack of Consensus
3.2. Heterogenicity in PPC Patients
3.3. Selective Focus of the PPC Literature
4. Pathway towards Developing Quality Indicators for PPC in LA
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chambers, L. A Guide to Children’s Palliative Care; Together for Short Lives: Bristol, UK, 2018. [Google Scholar]
- Connor, S.R. Global Atlas of Palliative Care, 2nd ed.; Worldwide Palliative Care Alliance: London, UK, 2020. [Google Scholar]
- Connor, S.R.; Downing, J.; Marston, J. Estimating the Global Need for Palliative Care for Children: A Cross-Sectional Analysis. J. Pain Symptom Manag. 2017, 53, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Knaul, F.M.; Farmer, P.E.; Krakauer, E.L.; De Lima, L.; Bhadelia, A.; Jiang Kwete, X.; Arreola-Ornelas, H.; Gómez-Dantés, O.; Rodriguez, N.M.; Alleyne, G.A.O.; et al. Alleviating the Access Abyss in Palliative Care and Pain Relief—an Imperative of Universal Health Coverage: The Lancet Commission Report. Lancet 2018, 391, 1391–1454. [Google Scholar] [CrossRef]
- Knapp, C.; Woodworth, L.; Wright, M.; Downing, J.; Drake, R.; Fowler-Kerry, S.; Hain, R.; Marston, J. Pediatric Palliative Care Provision around the World: A Systematic Review. Pediatr. Blood Cancer 2011, 57, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Pastrana, L.; De Lima, L.; Wenk, R.; Eisenchlas, J.; Monti, C.; Rocafort, J.; Centeno, C. Atlas de Cuidados Paliativos de Latinoamérica ALCP, 1st ed.; IAHPC Press: Houston, TX, USA, 2012. [Google Scholar]
- Garcia-Quintero, X.; Parra-Lara, L.G.; Claros-Hulbert, A.; Cuervo-Suarez, M.I.; Gomez-Garcia, W.; Desbrandes, F.; Arias-Casais, N. Advancing Pediatric Palliative Care in a Low-Middle Income Country: An Implementation Study, a Challenging but Not Impossible Task. BMC Palliat. Care 2020, 19, 170. [Google Scholar] [CrossRef] [PubMed]
- Feudtner, C. Perspectives on Quality at the End of Life. Arch. Pediatr. Adolesc. Med. 2004, 158, 415–417. [Google Scholar] [CrossRef]
- Charlebois, J.; Cyr, C. Quality Indicators for Paediatric Palliative Care. Paediatr. Child Health 2015, 20, 145–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Institute for Health Care Excellence (NICE). NICE Guideline NG61: End of Life Care for Infants, Children and Young People with Life-Limiting Conditions: Planning and Management; NICE: London, UK, 2016. [Google Scholar]
- National Hospice and Palliative Care Organization (NHPCO). Standards of Practice for Pediatric Palliative Care; NHPCO: Alexandria, VA, USA, 2019. [Google Scholar]
- European Association for Palliative Care TSG (last). IMPaCCT: Standards for Paediatric Palliative Care in Europe. Eur. J. Palliat. Care 2007, 14, 109–115. [Google Scholar]
- Friedel, M.; Aujoulat, I.; Dubois, A.-C.; Degryse, J.-M. Instruments to Measure Outcomes in Pediatric Palliative Care: A Systematic Review. Pediatrics 2019, 143, e20182379. [Google Scholar] [CrossRef] [Green Version]
- Widger, K.; Medeiros, C.; Trenholm, M.; Zuniga-Villanueva, G.; Streuli, J.C. Indicators Used to Assess the Impact of Specialized Pediatric Palliative Care: A Scoping Review. J. Palliat. Med. 2019, 22, 199–219. [Google Scholar] [CrossRef]
- Marcus, K.L.; Santos, G.; Ciapponi, A.; Comandé, D.; Bilodeau, M.; Wolfe, J.; Dussel, V. Impact of Specialized Pediatric Palliative Care: A Systematic Review. J. Pain Symptom Manag. 2020, 59, 339–364.e10. [Google Scholar] [CrossRef]
- Wolff, S.L.; Christiansen, C.F.; Nielsen, M.K.; Johnsen, S.P.; Schroeder, H.; Neergaard, M.A. Predictors for Place of Death among Children:A Systematic Review and Meta-Analyses of Recent Literature. Eur. J. Pediatr. 2020, 179, 1227–1238. [Google Scholar] [CrossRef]
- Dosani, N.; Bhargava, R.; Arya, A.; Pang, C.; Tut, P.; Sharma, A.; Chasen, M. Perceptions of Palliative Care in a South Asian Community: Findings from an Observational Study. BMC Palliat. Care 2020, 19, 141. [Google Scholar] [CrossRef] [PubMed]
- Zurriaráin, R.G. Between Euthanasia and Therapeutic Obstinacy: Palliative Care. Hosp. Palliat. Med. Int. J. 2020, 4, 9–12. [Google Scholar] [CrossRef]
- Pérez Pérez, F.M. Adecuación del esfuerzo terapéutico, una estrategia al final de la vida. SEMERGEN Med. Fam. 2016, 42, 566–574. [Google Scholar] [CrossRef] [PubMed]
- Diestre Ortín, G.; González Sequero, V.; Collell Domènech, N.; Pérez López, F.; Hernando Robles, P. [Advance care planning and severe chronic diseases]. Rev. Espanola Geriatr. Gerontol. 2013, 48, 228–231. [Google Scholar] [CrossRef]
- Martínez Gimeno, M.L.; Cámara Escribano, C.; Honrubia Fernández, T.; Olmo García, M.C.; Tovar Benito, D.H.; Bilbao-Goyoaga Arenas, T.; Rodríguez Almagro, P.; en nombre del grupo PLAMOS. Knowledge and attitudes of health care professionals in advance healthcare directives. J. Healthc. Qual. Res. 2018, 33, 270–277. [Google Scholar] [CrossRef]
- Machado, K.K.; Hoff, P.M. Autonomy versus Paternalism in Latin America. Oncology (Williston Park NY) 2012, 26, 46–47. [Google Scholar]
- Bustamante, A.V.; Méndez, C.A. Health Care Privatization in Latin America: Comparing Divergent Privatization Approaches in Chile, Colombia, and Mexico. J. Health Polit. Policy Law 2014, 39, 841–886. [Google Scholar] [CrossRef]
- Smith, C.H.; Graham, C.A.; Herbert, A.R. Respite Needs of Families Receiving Palliative Care. J. Paediatr. Child Health 2017, 53, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Covarrubias-Gómez, A.; Otero-Lamas, M.; Templos-Esteban, L.A.; Soto-Pérez-de-Celis, E. Antecedentes de la medicina paliativa en México: Educación continua en cuidados paliativos. Rev. Mex. Anestesiol. 2019, 42, 7. [Google Scholar]
- Saunders, C. The Evolution of Palliative Care. J. R. Soc. Med. 2001, 94, 430–432. [Google Scholar] [CrossRef] [Green Version]
- Ramanayake, R.P.J.C.; Dilanka, G.V.A.; Premasiri, L.W.S.S. Palliative Care; Role of Family Physicians. J. Fam. Med. Prim. Care 2016, 5, 234–237. [Google Scholar] [CrossRef]
- Lohman, D.; Herrera García, A.; Amon, J.; Wilkinson, D.; Kippenberg, J.; Reidy, A.; Olugboji, B. Care When There Is No Cure: Ensuring the Right to Palliative Care in Mexico; Human Rights Watch: New York, NY, USA, 2014. [Google Scholar]
- Soto-Perez-de-Celis, E.; Chavarri-Guerra, Y.; Pastrana, T.; Ruiz-Mendoza, R.; Bukowski, A.; Goss, P.E. End-of-Life Care in Latin America. J. Glob. Oncol. 2017, 3, 261–270. [Google Scholar] [CrossRef]
- George, T. Role of the Advanced Practice Nurse in Palliative Care. Int. J. Palliat. Nurs. 2016, 22, 137–140. [Google Scholar] [CrossRef]
- Zug, K.E.; Cassiani, S.H.D.B.; Pulcini, J.; Garcia, A.B.; Aguirre-Boza, F.; Park, J. Advanced Practice Nursing in Latin America and the Caribbean: Regulation, Education and Practice. Rev. Lat. Am. Enfermagem 2016, 24, e2807. [Google Scholar] [CrossRef]
- Basak, R.B.; Momaya, R.; Guo, J.; Rathi, P. Role of Child Life Specialists in Pediatric Palliative Care. J. Pain Symptom Manag. 2019, 58, 735–737. [Google Scholar] [CrossRef]
- Sutter, C.; Reid, T. How Do We Talk to the Children? Child Life Consultation to Support the Children of Seriously Ill Adult Inpatients. J. Palliat. Med. 2012, 15, 1362–1368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Färber, S.S. Tanatologia clínica e cuidados paliativos: Facilitadores do luto oncológico pediátrico. Cad. Saúde Coletiva 2013, 21, 267–271. [Google Scholar] [CrossRef] [Green Version]
- Zuniga-Villanueva, G.; Ramirez-GarciaLuna, J.L.; Weingarten, K. Factors Associated With Knowledge and Comfort Providing Palliative Care: A Survey of Pediatricians in Mexico. J. Palliat. Care 2019, 34, 132–138. [Google Scholar] [CrossRef]
- Zúñiga-Fajuri, A. Human Rights and the Right to Abortion in Latin America. Cienc. Saude Coletiva 2014, 19, 841–846. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wool, C. Instrument Development: Parental Satisfaction and Quality Indicators of Perinatal Palliative Care. J. Hosp. Palliat. Nurs. 2015, 17, 301–308. [Google Scholar] [CrossRef]
- Organisation for Economic Co-operation and Development; World Health Organization; World Bank Group. Delivering Quality Health Services: A Global Imperative for Universal Health Coverage; OECD Publishing: Paris, France, 2018. [Google Scholar]
- Donabedian, A. The Quality of Care. How Can It Be Assessed? JAMA 1988, 260, 1743–1748. [Google Scholar] [CrossRef]
- Coombes, L.H.; Wiseman, T.; Lucas, G.; Sangha, A.; Murtagh, F.E. Health-Related Quality-of-Life Outcome Measures in Paediatric Palliative Care: A Systematic Review of Psychometric Properties and Feasibility of Use. Palliat. Med. 2016, 30, 935–949. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, S.; Morris, A.; Bennett, K.; Sajid, L.; Dale, J. Specialist Paediatric Palliative Care Services: What Are the Benefits? Arch. Dis. Child. 2017, 102, 923–929. [Google Scholar] [CrossRef] [Green Version]
- Zuniga-Villanueva, G.; Widger, K.; Medeiros, C.; Trenholm, M.; Streuli, J.C. Specialized Pediatric Palliative Care in Neonates with Life-Limiting Illness: A Systematic Review. Am. J. Perinatol. 2020. [Google Scholar] [CrossRef]
- Widger, K.A.; Wilkins, K. What Are the Key Components of Quality Perinatal and Pediatric End-of-Life Care? A Literature Review. J. Palliat. Care 2004, 20, 105–112. [Google Scholar] [CrossRef]
- Together for Short Lives. Standards Framework for Children’s Palliative Care; Together for Short Lives: Bristol, UK, 2015. [Google Scholar]
- National Instituce for Health and Care Excellence. NICE Quality Standard QS160: End of Life Care for Infants, Children and Young People; NICE: London, UK, 2017. [Google Scholar]
- Gans, D.; Kominski, G.F.; Roby, D.H.; Diamant, A.L.; Chen, X.; Lin, W.; Hohe, N. Better Outcomes, Lower Costs: Palliative Care Program Reduces Stress, Costs of Care for Children with Life-Threatening Conditions; UCLA Center for Health Policy Research: Los Angeles, CA, USA, 2012. [Google Scholar]
- Bergstraesser, E.; Zimmermann, K.; Eskola, K.; Luck, P.; Ramelet, A.-S.; Cignacco, E. Paediatric End-of-Life Care Needs in Switzerland: Current Practices, and Perspectives from Parents and Professionals. A Study Protocol. J. Adv. Nurs. 2015, 71, 1940–1947. [Google Scholar] [CrossRef]
- Ferrell, B.R.; Twaddle, M.L.; Melnick, A.; Meier, D.E. National Consensus Project Clinical Practice Guidelines for Quality Palliative Care Guidelines, 4th Edition. J. Palliat. Med. 2018, 21, 1684–1689. [Google Scholar] [CrossRef]
- Constantinou, G.; Garcia, R.; Cook, E.; Randhawa, G. Children’s Unmet Palliative Care Needs: A Scoping Review of Parents’ Perspectives. BMJ Support. Palliat. Care 2019. [Google Scholar] [CrossRef] [PubMed]
- Leemann, T.; Bergstraesser, E.; Cignacco, E.; Zimmermann, K. Differing Needs of Mothers and Fathers during Their Child’s End-of-Life Care: Secondary Analysis of the “Paediatric End-of-Life Care Needs” (PELICAN) Study. BMC Palliat. Care 2020, 19, 118. [Google Scholar] [CrossRef]
- Huang, I.-C.; Shenkman, E.A.; Madden, V.L.; Vadaparampil, S.; Quinn, G.; Knapp, C.A. Measuring Quality of Life in Pediatric Palliative Care: Challenges and Potential Solutions. Palliat. Med. 2010, 24, 175–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiener, L.; McConnell, D.G.; Latella, L.; Ludi, E. Cultural and Religious Considerations in Pediatric Palliative Care. Palliat. Support. Care 2013, 11, 47–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marston, J.; Boucher, S.; Downing, J. International Children’s Palliative Care Network: A Global Action Network for Children With Life-Limiting Conditions. J. Pain Symptom Manag. 2018, 55, S104–S111. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| Available Resources | Achievable Standards of Care | Description of Quality Indicators |
|---|---|---|
| Perinatal and PPC 1 champion or specialist | Child’s quality of life | Offers specialized pain and symptom management to achieve comfort and minimize total pain and suffering. |
| Offers age-appropriate care during all disease stages. | ||
| Uses patient-reported outcomes to guide care (when possible). | ||
| Offers services to children with life-limiting and life-threatening conditions, which includes chronic-complex conditions, cancer and perinatal diagnosis. | ||
| Family Support | Offers family-centered care by supporting the family unit. | |
| Helps families identify their goals. | ||
| Encourages parents to be part of the care of the child. | ||
| Communication | Offers clear and honest information to the child and family. | |
| Ensures communication with other healthcare providers who follow the patient. | ||
| Advanced care planning | Promotes shared decision-making. | |
| Involves patients and families in developing treatment goals and plans. | ||
| Helps families in difficult decision-making, including end-of-life care plans. | ||
| End-of-life care | Provides care for the imminently dying patient. | |
| Assures that the intensity of treatment is in accordance with the goals of care and the child’s best interest. | ||
| Helps families prepare for the death of the child. | ||
| Referrals | Provides information about emotional and psychosocial support and how to access it. | |
| Provides information on bereavement support and how to access it. | ||
| Education | Offers education to the family. | |
| Offers education to other healthcare professionals. | ||
| Specialized PPC team (it may include a combination of physicians, nursing, social worker, mental health specialist, child life specialist, spiritual support, grief counselling and other allied health professionals) | Holistic support | Offers multidisciplinary assessment and support of patient and family needs. |
| Offers support to siblings and extended family. | ||
| Offers psychological support to patient and family. | ||
| Offers social support for patient and family. | ||
| Offers spiritual support for patient and family. | ||
| Offers expressive therapies including art, music, play and massage. | ||
| Coordination of care | Designates a keyworker to the patient and family who leads and coordinates the care. | |
| Offers flexible delivery of care across settings to ensure continuity of care. | ||
| Grief and bereavement support | Offers grief support before, during and after death. | |
| Offers continuing bereavement support for families during their grief process. | ||
| Offers active grief support of siblings and extended family. | ||
| Helps families make funeral arrangements. | ||
| Availability | Offers access to PPC 24 h a day, seven days a week, 365 days a year. | |
| Healthcare professionals support | Promotes continuous training and self-care for all team members. | |
| Supports other healthcare professionals. | ||
| Community healthcare providers with PPC knowledge | Community provision of PPC | Provides palliative care and follow-up at home. |
| Provides end-of-life care at home for families who desire it. | ||
| Offers a seamless transition between the hospital and home. | ||
| Hospice | Respite | Offers respite for care providers to obtain brakes. |
| End-of-life care | Offers end-of-life care outside of the hospital and in the community other than at home. | |
| National Council, Association or College | Advocacy | Active lobbying for PPC development. |
| Advocates for the compliance of laws and regulations. | ||
| Research and publications | Development of national guidelines, standards or norms. | |
| Encourages local PPC providers to engage in research and academic activities. | ||
| Education | Endorses perinatal and PPC training programs. | |
| Regulation | Assesses performance to ensure the quality of care provision. | |
| Regulates the professional activities of PPC providers. | ||
| Collaboration | Creates a network that fosters collaboration between PPC providers. | |
| Creates partnerships between PPC and other specialties. | ||
| Engages with international palliative care associations. | ||
| Health system | National law | Existence of law that protects PPC practice and recognizes specific pediatric needs in palliative care. |
| Equity | Inclusive and equitable access to PPC across settings and institutions. | |
| Existence of specific pediatric formulations available in the national essential medicine list. | ||
| Funding | Funding of palliative care services. | |
| Assessment of healthcare utilization and costs. | ||
| Offer financial support to families with PPC needs. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zuniga-Villanueva, G.; Ramos-Guerrero, J.A.; Osio-Saldaña, M.; Casas, J.A.; Marston, J.; Okhuysen-Cawley, R. Quality Indicators in Pediatric Palliative Care: Considerations for Latin America. Children 2021, 8, 250. https://0-doi-org.brum.beds.ac.uk/10.3390/children8030250
Zuniga-Villanueva G, Ramos-Guerrero JA, Osio-Saldaña M, Casas JA, Marston J, Okhuysen-Cawley R. Quality Indicators in Pediatric Palliative Care: Considerations for Latin America. Children. 2021; 8(3):250. https://0-doi-org.brum.beds.ac.uk/10.3390/children8030250
Chicago/Turabian StyleZuniga-Villanueva, Gregorio, Jorge Alberto Ramos-Guerrero, Monica Osio-Saldaña, Jessica A. Casas, Joan Marston, and Regina Okhuysen-Cawley. 2021. "Quality Indicators in Pediatric Palliative Care: Considerations for Latin America" Children 8, no. 3: 250. https://0-doi-org.brum.beds.ac.uk/10.3390/children8030250