
Etiology of Carpal Tunnel Syndrome in a Large Cohort of Children

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Demographics
3.2. Etiology
3.3. Clinical Findings
3.4. Electrophysiological Examination
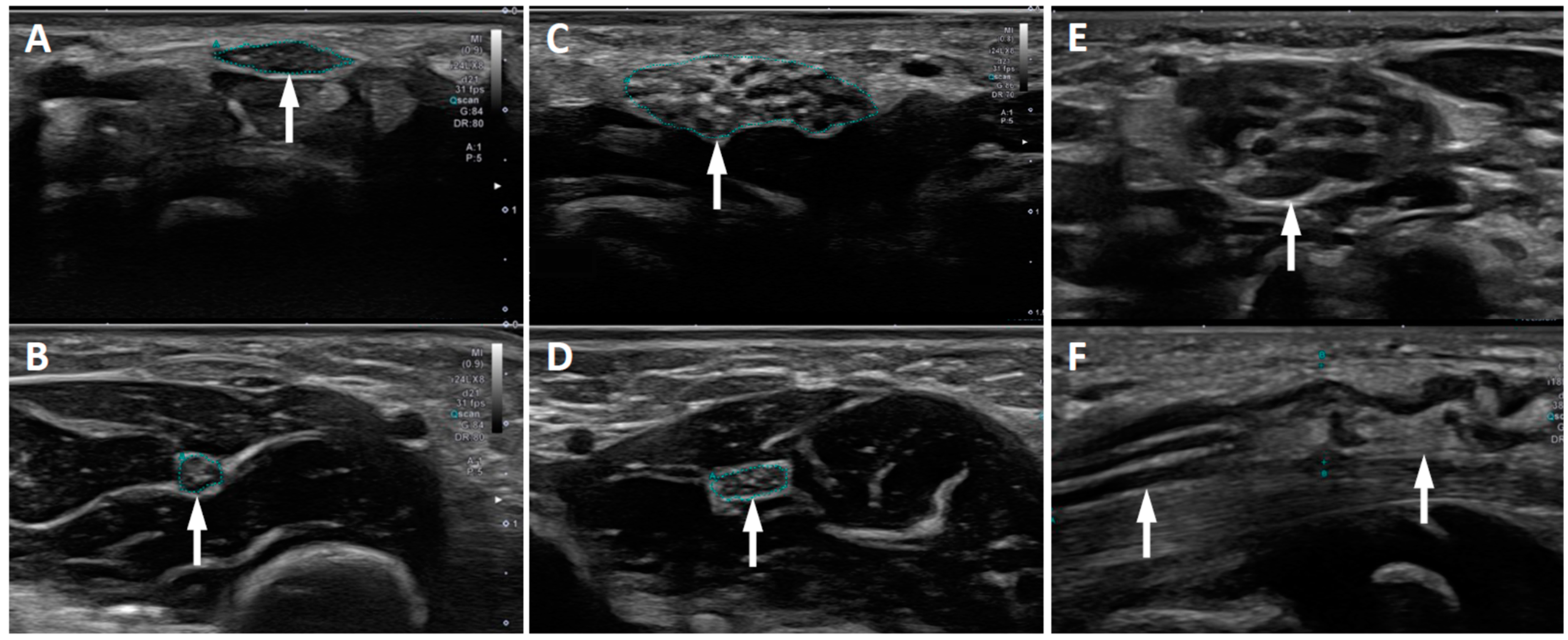
3.5. Ultrasound Imaging
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Martin, C.; Masse, P. Carpal tunnel syndrome in children. Arch. Fr. Pediatr. 1958, 15, 930–940. [Google Scholar] [PubMed]
- Poilvache, P.; Carlier, A.; Rombouts, J.J.; Partoune, E.; Lejeune, G. Carpal tunnel syndrome in childhood: Report of five new cases. J. Pediatr. Orthop. 1989, 9, 687–690. [Google Scholar] [CrossRef]
- Van Meir, N.; Smet, L. Carpal tunnel syndrome in children. Acta Orthop. Belg. 2003, 69, 387–395. [Google Scholar] [CrossRef]
- Van Meir, N.; Smet, L. Carpal tunnel syndrome in children. J. Pediatr. Orthop. B 2005, 14, 42–45. [Google Scholar] [CrossRef]
- Deymeer, F.; Jones, H.R., Jr. Pediatric median mononeuropathies: A clinical and electromyographic study. Muscle Nerve 1994, 17, 755–762. [Google Scholar] [CrossRef]
- Billakota, S.; Hobson-Webb, L.D. Standard median nerve ultrasound in carpal tunnel syndrome: A retrospective review of 1021 cases. Clin. Neurophysiol. Pract. 2017, 2, 188–191. [Google Scholar] [CrossRef]
- Dabaj, I.; Gitiaux, C.; Avila-Smirnow, D.; Ropers, J.; Desguerre, I.; Salon, A.; Pannier, S.; Tebani, A.; Valayannopoulos, V.; Quijano-Roy, S. Diagnosis and management of carpal tunnel syndrome in children with mucopolysaccharidosis: A 10 year experience. Diagnostics 2020, 10, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leti Acciaro, A.; Pilla, F.; Faldini, C.; Adani, R. The carpal tunnel syndrome in children. Musculoskelet. Surg. 2018, 102, 261–265. [Google Scholar] [CrossRef]
- Viskochil, D.; Muenzer, J.; Guffon, N.; Garin, C.; Munoz-Rojas, M.V.; Moy, K.A.; Hutchinson, D.T. Carpal tunnel syndrome in mucopolysaccharidosis I: A registry-based cohort study. Dev. Med. Child Neurol. 2017, 59, 1269–1275. [Google Scholar] [CrossRef] [Green Version]
- Werner, R.A.; Andary, M. Electrodiagnostic evaluation of carpal tunnel syndrome. Muscle Nerve 2011, 44, 597–607. [Google Scholar] [CrossRef] [Green Version]
- Druzhinin, D.; Naumova, E.; Nikitin, S. Nerve ultrasound normal values in children and young adults. Muscle Nerve 2019, 60, 757–761. [Google Scholar] [CrossRef] [PubMed]
- Jenny, C.; Lütschg, J.; Broser, P.J. Change in cross-sectional area of the median nerve with age in neonates, infants and children analyzed by high-resolution ultrasound imaging. Eur. J. Paediatr. Neurol. 2020, 29, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Algahtani, H.; Watson, B.V.; Thomson, J.; Al-Rabia, M.W. Idiopathic bilateral carpal tunnel syndrome in a 9-month-old infant presenting as a pseudo-dystonia. Pediatr. Neurol. 2014, 51, 147–150. [Google Scholar] [CrossRef] [PubMed]
- Bland, J.D.P.; Rudolfer, S.M. Clinical surveillance of carpal tunnel syndrome in two areas of the United Kingdom, 1991–2001. J. Neurol. Neurosurg. Psychiatry 2003, 74, 1674–1679. [Google Scholar] [CrossRef] [Green Version]
- Lamberti, P.M.; Light, T.R. Carpal tunnel syndrome in children. Hand Clin. 2002, 18, 331–337. [Google Scholar] [CrossRef]
- Kwon, J.Y.; Ko, K.; Sohn, Y.B.; Kim, S.J.; Park, S.W.; Kim, S.H.; Cho, S.Y.; Jin, D.K. High prevalence of carpal tunnel syndrome in children with mucopolysaccharidosis type II (Hunter syndrome). Am. J. Med. Genet. Part A 2011, 155, 1329–1335. [Google Scholar] [CrossRef]
- Patel, P.; Antoniou, G.; Clark, D.; Ketteridge, D.; Williams, N. Screening for Carpal Tunnel Syndrome in Patients with Mucopolysaccharidosis. J. Child Neurol. 2020, 35, 410–417. [Google Scholar] [CrossRef] [Green Version]
- White, K.; Kim, T.; Neufeld, J.A. Clinical assessment and treatment of carpal tunnel syndrome in the mucopolysaccharidoses. J. Pediatr. Rehabil. Med. 2010, 3, 57–62. [Google Scholar] [CrossRef] [Green Version]
- Del Colle, R.; Fabrizi, G.M.; Turazzini, M.; Cavallaro, T.; Silvestri, M.; Rizzuto, N. Hereditary neuropathy with liability to pressure palsies: Electrophysiological and genetic study of a family with carpal tunnel syndrome as only clinical manifestation. Neurol. Sci. 2003, 24, 57–60. [Google Scholar] [CrossRef]
- Leguern, E.; Gugenheim, M.; Maisonobe, T.; Léger, J.M.; Vallat, J.M.; Agid, Y.; Bouche, P.; Brice, A. Clinical, electrophysiologic, and molecular correlations in 13 families with hereditary neuropathy with liability to pressure palsies and a chromosome 17~11.2 deletion. Neurology 1995, 45, 2018–2023. [Google Scholar]
- Abdullah, S.; Nor, N.F.M.; Haflah, N.H.M. Melorheostosis of the hand affecting the c6 sclerotome and presenting with carpal tunnel syndrome. Singap. Med. J. 2014, 55, 54–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ameen, S.; Nagy, L.; Gerich, U.; Anderson, S.E. Melorheostosis of the hand with complicating bony spur formation and bursal inflammation: Diagnosis and treatment. Skelet. Radiol. 2002, 31, 467–470. [Google Scholar] [CrossRef]
- Suresh, S.; Muthukumar, T.; Saifuddin, A. Classical and unusual imaging appearances of melorheostosis. Clin. Radiol. 2010, 65, 593–600. [Google Scholar] [CrossRef]
- Marzin, P.; Thierry, B.; Dancasius, A.; Cavau, A.; Michot, C.; Rondeau, S.; Baujat, G.; Phan, G.; Bonnière, M.; Le Bourgeois, M.; et al. Geleophysic and acromicric dysplasias: Natural history, genotype–phenotype correlations, and management guidelines from 38 cases. Genet. Med. 2021, 23, 331–340. [Google Scholar] [CrossRef]
- Scheller, C.; Richter, H.P.; Scheuerle, A.; Kretschmer, T.; König, R.W.; Antoniadis, G. Intraneural perineuriomas; a rare entity. Clinical, surgical and neuropathological details in the management of these lesions. Zentralbl. Neurochir. 2008, 69, 134–138. [Google Scholar] [CrossRef]
- Koutlas, I.G.; Anbinder, A.-L.; Alshagroud, R.; Rodrigues Cavalcante, A.S.; Al Kindi, M.; Crenshaw, M.M.; Sapp, J.C.; Kondolf, H.; Lindhurst, M.J.; Dudley, J.N.; et al. Orofacial overgrowth with peripheral nerve enlargement and perineuriomatous pseudo-onion bulb proliferations is part of the PIK3CA-related overgrowth spectrum. Hum. Genet. Genom. Adv. 2020, 1, 100009. [Google Scholar] [CrossRef]
- Blackburn, P.R.; Milosevic, D.; Marek, T.; Folpe, A.L.; Howe, B.M.; Spinner, R.J.; Carter, J.M. PIK3CA mutations in lipomatosis of nerve with or without nerve territory overgrowth. Mod. Pathol. 2020, 33, 420–430. [Google Scholar] [CrossRef] [PubMed]
- Dailiana, Z.H.; Bougioukli, S.; Varitimidis, S.; Kontogeorgakos, V.; Togia, E.; Vlychou, M.; Malizos, K.N. Tumors and tumor-like lesions mimicking carpal tunnel syndrome. Arch. Orthop. Trauma Surg. 2014, 134, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Işikay, S.; Yilmaz, K.; Yiǧiter, R.; Balat, A.; Büyükçelik, M. Colchicine treatment in children with familial Mediterranean fever: Is it a risk factor for neuromyopathy? Pediatr. Neurol. 2013, 49, 417–419. [Google Scholar] [CrossRef]
- Bademci, G.; Erdemoglu, A.K.; Evliyaoglu, C.; Atasoy, P.; Keskil, S. Bilateral carpal tunnel syndrome associated to familial Mediterranean fever. Clin. Neurol. Neurosurg. 2005, 108, 77–79. [Google Scholar] [CrossRef]
- Balcl-Peynircioǧlu, B.; Kaya-Akça, Ü.; Arlcl, Z.S.; Avcl, E.; Yeliz Akkaya-Ulum, Z.; Karadaǧ, Ö.; Kalyoncu, U.; Bilginer, Y.; Yllmaz, E.; Özen, S. Comorbidities in familial Mediterranean fever: Analysis of 2000 genetically confirmed patients. Rheumatology 2020, 59, 1372–1380. [Google Scholar] [CrossRef] [PubMed]
- Beekman, R.; Visser, L.H. Sonography in the diagnosis of carpal tunnel syndrome: A critical review of the literature. Muscle Nerve 2003, 27, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Duncan, I.; Sullivan, P.; Lomas, F. Sonography in the diagnosis of carpal tunnel syndrome. AJR Am. J. Roentgenol. 1999, 3, 681–684. [Google Scholar] [CrossRef]
- Mhoon, J.T.; Juel, V.C.; Hobson-Webb, L.D. Median nerve ultrasound as a screening tool in carpal tunnel syndrome: Correlation of cross-sectional area measures with electrodiagnostic abnormality. Muscle Nerve 2012, 46, 871–878. [Google Scholar] [CrossRef] [PubMed]
- Bäumer, T.; Bühring, N.; Schelle, T.; Münchau, A.; Muschol, N. Nerve ultrasound in clinical management of carpal tunnel syndrome in mucopolysaccharidosis. Dev. Med. Child Neurol. 2016, 58, 1172–1179. [Google Scholar] [CrossRef]


{kind=link}
| Gender [n (%)] | female | 22 (58%) |
| male | 16 (42%) | |
| Age at diagnosis [years] | mean | 9.8 |
| range | 2.5–17 | |
| Location [n (%)] | unilateral | 9 (24%) |
| bilateral | 29 (76%) | |
| Positive family history for CTS [n (%)] | 8 (21%) | |
| Treatment [n (%)] | conservative | 11 (29%) |
| surgical | 27 (71%) |
| Number of Patients (n) | Unilateral vs. Bilateral | ||
|---|---|---|---|
| Lysosomal storage diseases | MPS Type 1 | 4 | bilateral |
| MPS Type 2 | 7 | bilateral | |
| MPS Type 3 | 1 | bilateral | |
| MPS Type 6 | 2 | bilateral | |
| Mucolipidosis Type 3 | 1 | bilateral | |
| Neuropathy | HNPP (assumed) | 3 | bilateral |
| CMT1A | 1 | bilateral | |
| associated with ARSACS | 1 | bilateral | |
| Congenital malformation | Geleophysic dysplasia | 2 | bilateral |
| Melorheostosis | 1 | unilateral | |
| Hemihypertrophia | 1 | bilateral | |
| Tumor | Intraneural Perineurioma | 2 | unilateral |
| Traumatic lesion | 2 | unilateral | |
| Rheumatoid arthritis | 1 | bilateral | |
| Idiopathic | 9 | 4 unilateral, 5 bilateral |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rüsch, C.T.; Knirsch, U.; Weber, D.M.; Rohrbach, M.; Eichenberger, A.; Lütschg, J.; Weber, K.; Broser, P.J.; Stettner, G.M. Etiology of Carpal Tunnel Syndrome in a Large Cohort of Children. Children 2021, 8, 624. https://0-doi-org.brum.beds.ac.uk/10.3390/children8080624
Rüsch CT, Knirsch U, Weber DM, Rohrbach M, Eichenberger A, Lütschg J, Weber K, Broser PJ, Stettner GM. Etiology of Carpal Tunnel Syndrome in a Large Cohort of Children. Children. 2021; 8(8):624. https://0-doi-org.brum.beds.ac.uk/10.3390/children8080624
Chicago/Turabian StyleRüsch, Christina T., Ursula Knirsch, Daniel M. Weber, Marianne Rohrbach, André Eichenberger, Jürg Lütschg, Kirsten Weber, Philip J. Broser, and Georg M. Stettner. 2021. "Etiology of Carpal Tunnel Syndrome in a Large Cohort of Children" Children 8, no. 8: 624. https://0-doi-org.brum.beds.ac.uk/10.3390/children8080624