Comparative Efficacy and Safety of Immunotherapeutic Regimens with PD-1/PD-L1 Inhibitors for Previously Untreated Extensive-Stage Small Cell Lung Cancer: A Systematic Review and Network Meta-Analysis

 , ,
, , 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Systematic Review
2.2. Quality Evaluation
2.3. Inclusion and Exclusion Criteria (Predefined PICOS)
2.3.1. Patients
2.3.2. Interventions/Comparisons
2.3.3. Outcomes
2.3.4. Study Design
2.4. Statistical NMA Method
2.5. Sensitivity Analysis
2.6. Assessment of Heterogeneity and Inconsistency
2.7. Ethical Aspects
3. Results
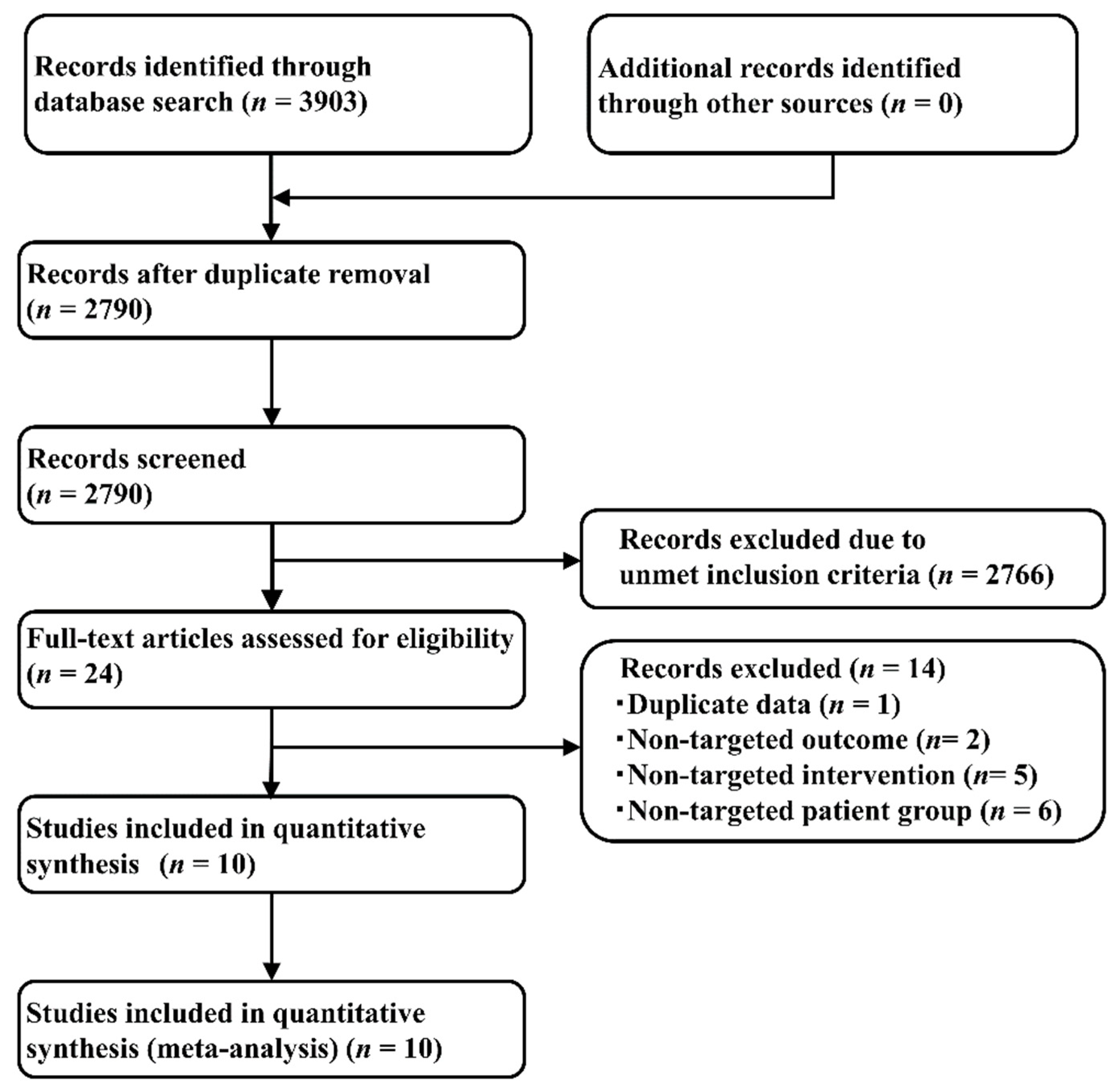
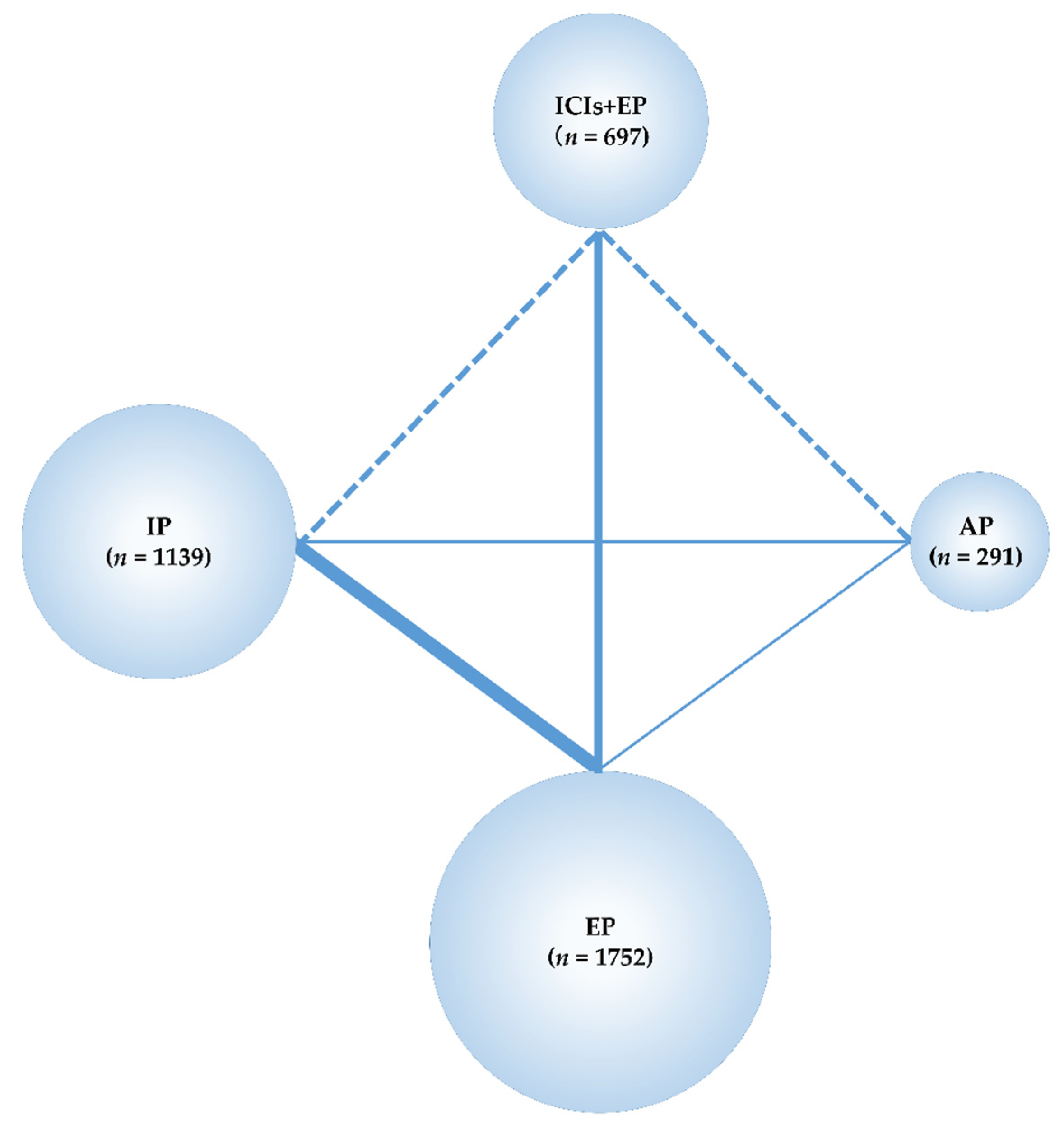
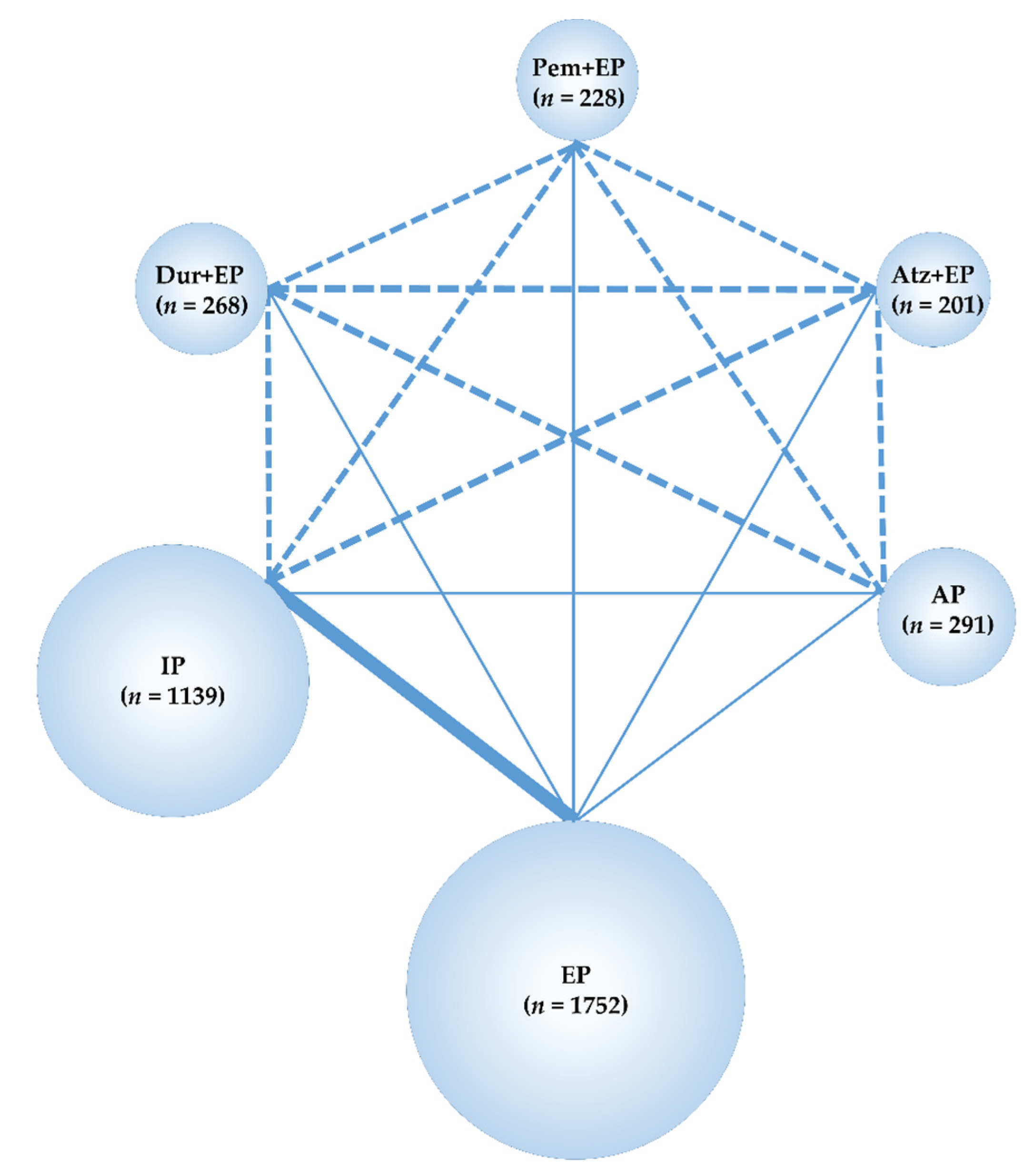
3.1. Systematic Review
3.2. Assessment of Risk of Bias and Heterogeneity/Inconsistency
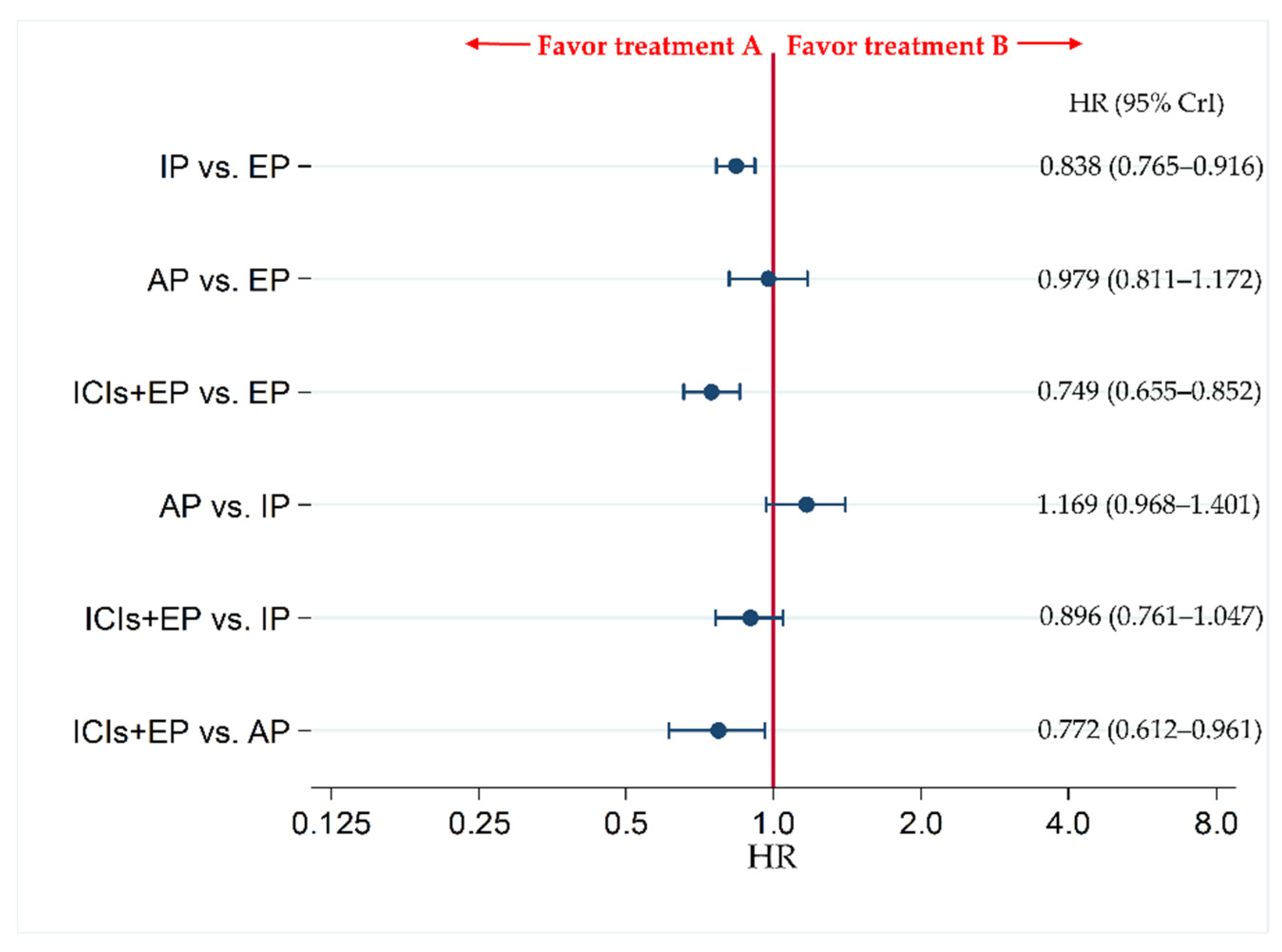
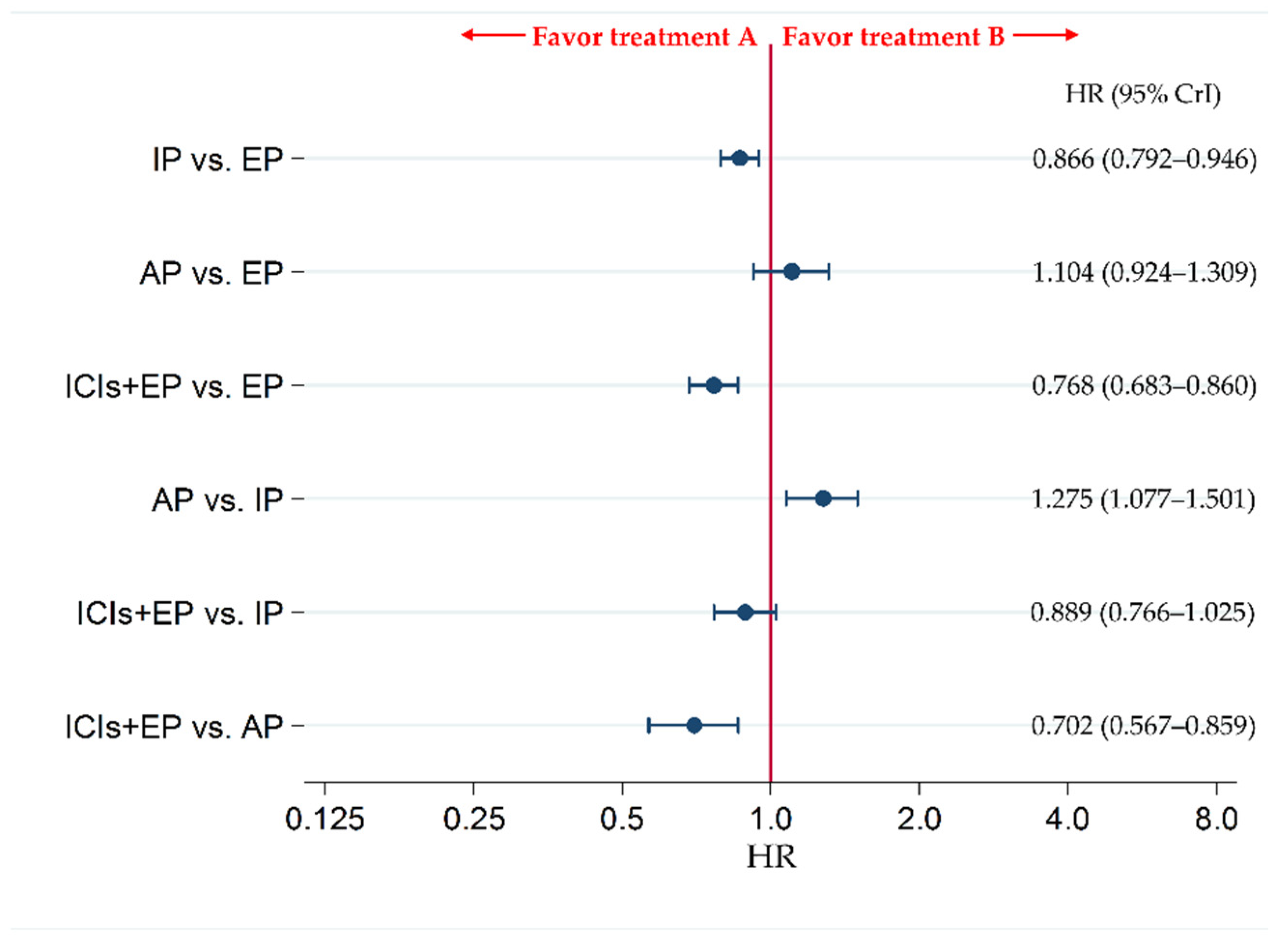
3.3. OS as the Primary Efficacy Endpoint
3.4. PFS as the Secondary Efficacy Endpoint
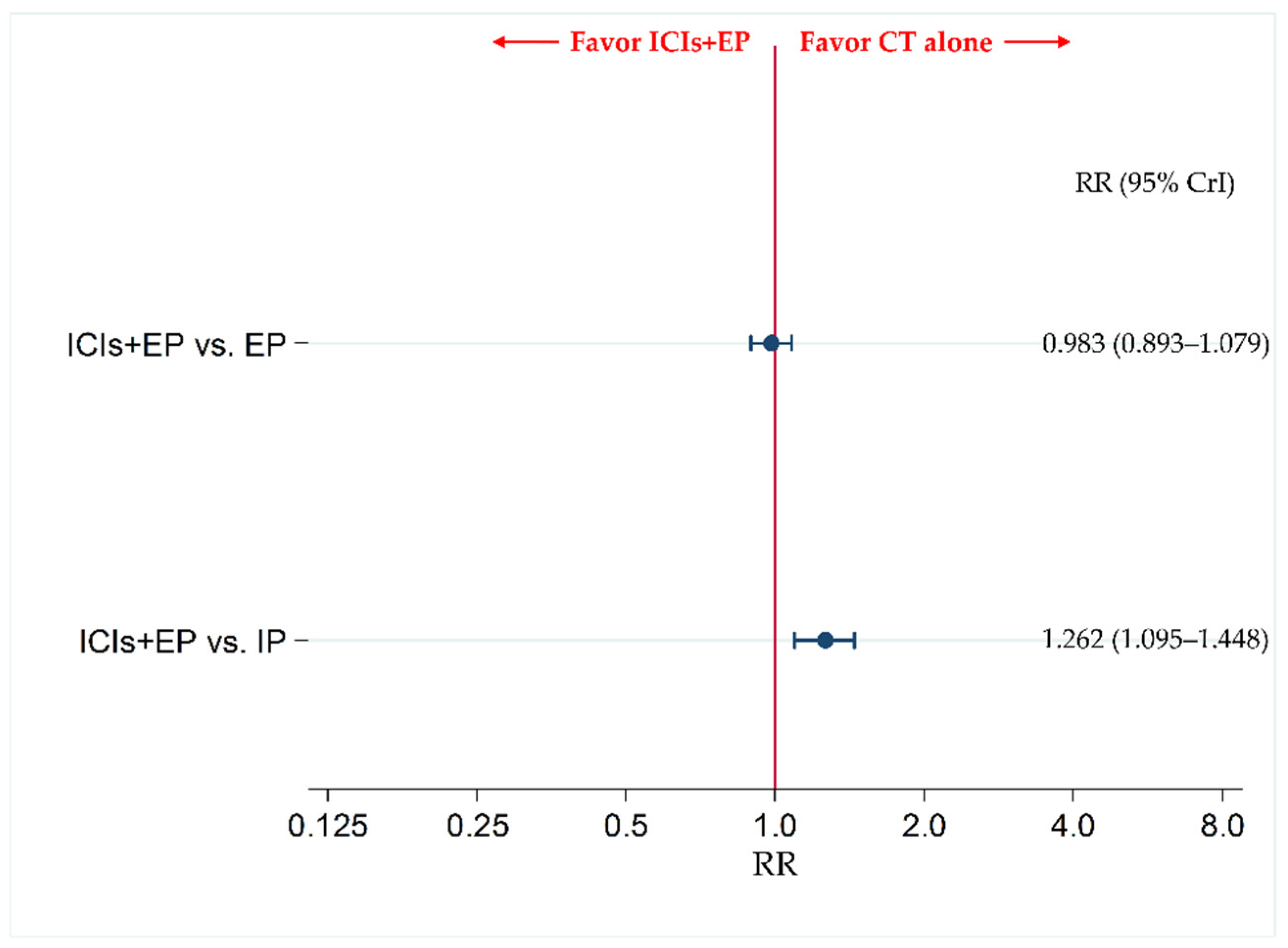
3.5. The Incidence of G3-AEs as a Primary Safety Endpoint
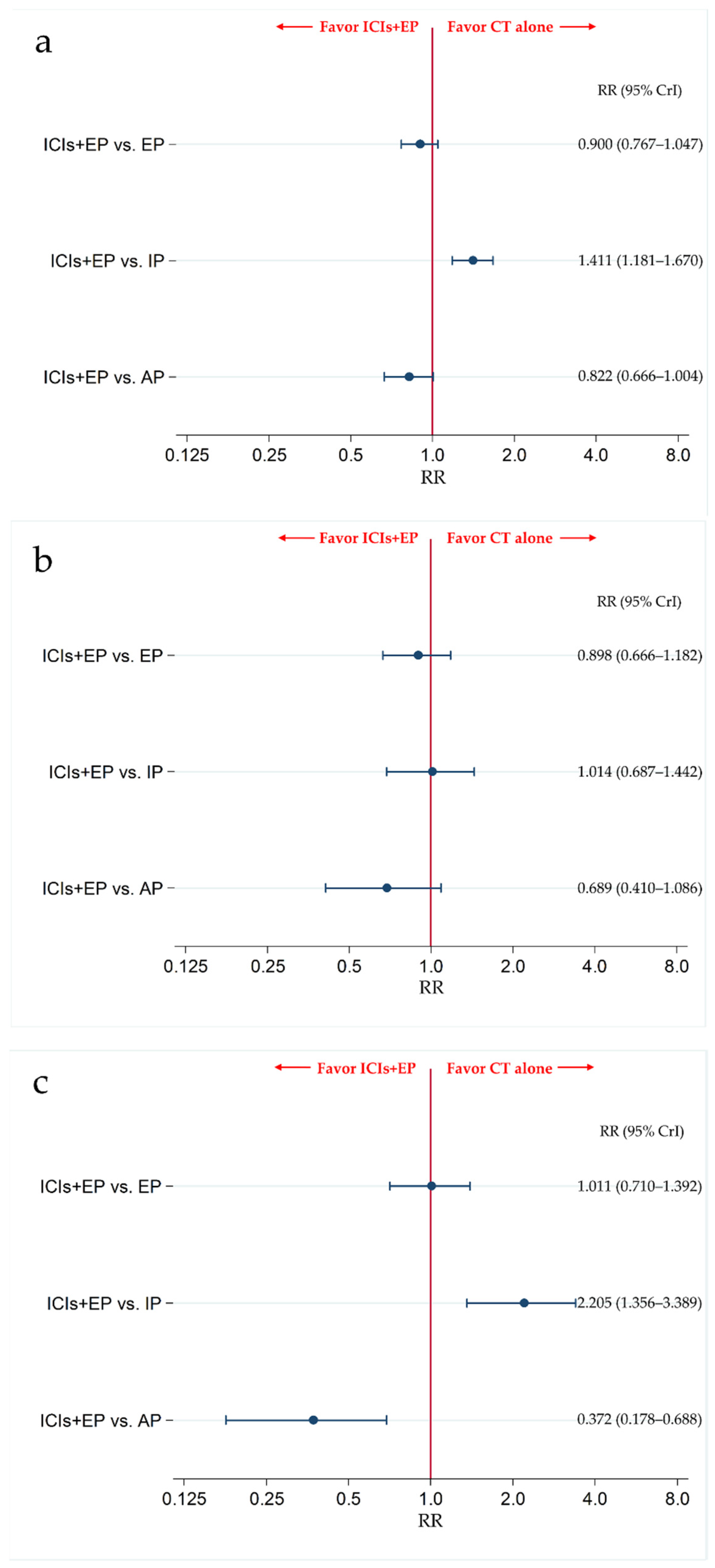
3.6. Secondary Safety Endpoint: The Incidence of G3-NP, G3-AN, and G3-TP
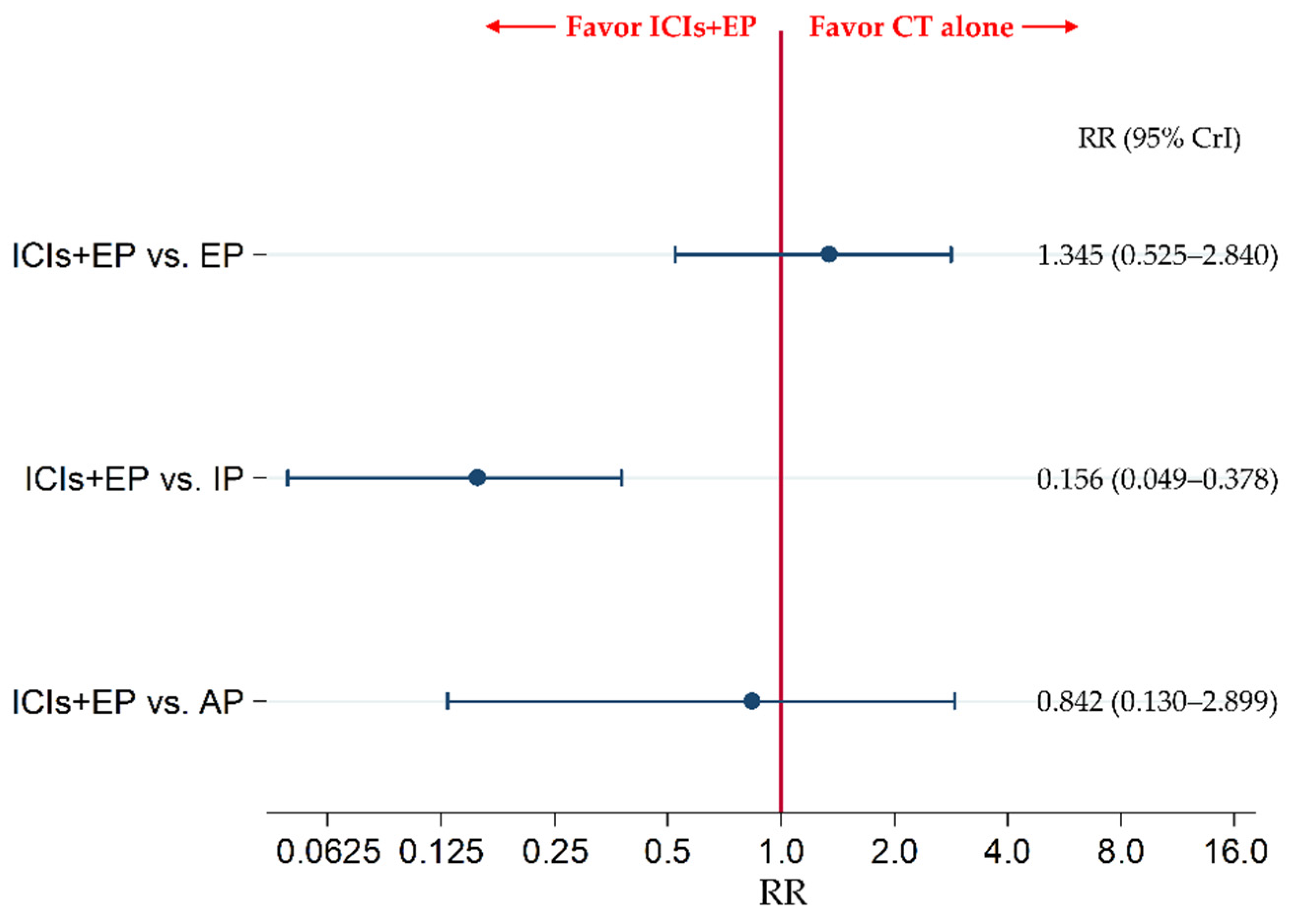
3.7. Secondary Safety Endpoint: The Incidence of G3-Diarrhea
3.8. Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A. Search Strategies in PubMed (Searched on 29 December 2020)
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef]
- Nasim, F.; Sabath, B.F.; Eapen, G.A. Lung Cancer. Med. Clin. N. Am. 2019, 103, 463–473. [Google Scholar] [CrossRef]
- Saltos, A.; Shafique, M.; Chiappori, A. Update on the biology, management, and treatment of small cell lung cancer (SCLC). Front. Oncol. 2020, 10, 1074. [Google Scholar] [CrossRef]
- Oronsky, B.; Reid, T.R.; Oronsky, A.; Carter, C.A. What’s New in SCLC? A Review. Neoplasia 2017, 19, 842–847. [Google Scholar] [CrossRef]
- Stahel, R.; Thatcher, N.; Früh, M.; Le Péchoux, C.; Postmus, P.E.; Sorensen, J.B.; Felip, E. Panel members. 1st ESMO Consensus Conference in lung cancer; Lugano 2010: Small-cell lung cancer. Ann. Oncol. 2011, 22, 1973–1980. [Google Scholar] [CrossRef] [PubMed]
- Rudin, C.M.; Awad, M.M.; Navarro, A.; Gottfried, M.; Peters, S.; Csőszi, T.; Cheema, P.C.; Rodriguez-Abreu, D.; Wollner, M.; Yang, J.C.-H.; et al. Pembrolizumab or placebo plus etoposide and platinum as first-line therapy for extensive-stage small-cell lung cancer: Randomized, double-blind, phase III KEYNOTE-604 study. J. Clin. Oncol. 2020, 38, 2369–2379. [Google Scholar] [CrossRef] [PubMed]
- Paz-Ares, L.; Dvorkin, M.; Chen, Y.; Reinmuth, N.; Hotta, K.; Trukhin, D.; Statsenko, G.; Hochmair, M.J.; Özgüroğlu, M.; Ji, J.H.; et al. Durvalumab plus platinum-etoposide versus platinum-etoposide in first-line treatment of extensive-stage small-cell lung cancer (CASPIAN): A randomised, controlled, open-label, phase 3 trial. Lancet 2019, 394, 1929–1939. [Google Scholar] [CrossRef]
- Horn, L.; Mansfield, A.S.; Szczęsna, A.; Havel, L.; Krzakowski, M.; Hochmair, M.J.; Huemer, F.; Losonczy, G.; Johnson, M.L.; Nishio, M.; et al. First-line atezolizumab plus chemotherapy in extensive-stage small-cell lung cancer. N. Engl. J. Med. 2018, 379, 2220–2229. [Google Scholar] [CrossRef]
- Iams, W.T.; Porter, J.; Horn, L. Immunotherapeutic approaches for small-cell lung cancer. Nat. Rev. Clin. Oncol. 2020, 17, 300–312. [Google Scholar] [CrossRef] [PubMed]
- Tsiouprou, I.; Zaharias, A.; Spyratos, D. The role of immunotherapy in extensive stage small-cell lung cancer: A review of the literature. Can. Respir. J. 2019, 2019, 6860432. [Google Scholar] [CrossRef]
- Lara, P.N., Jr.; Natale, R.; Crowley, J.; Lenz, H.J.; Redman, M.W.; Carleton, J.E.; Jett, J.; Langer, C.J.; Kuebler, J.P.; Dakhil, S.R.; et al. Phase III trial of irinotecan/cisplatin compared with etopo-side/cisplatin in extensive-stage small-cell lung cancer: Clinical and pharmacogenomic results from SWOG S0124. J. Clin. Oncol. 2009, 27, 2530–2535. [Google Scholar] [CrossRef] [Green Version]
- Han, D.; Wang, G.; Sun, L.; Ren, X.; Shang, W.; Xu, L.; Li, S. Comparison of irinotecan/platinum versus etoposide/platinum chemotherapy for extensive-stage small cell lung cancer: A meta-analysis. Eur. J. Cancer Care (Engl.) 2017, 26, e12723. [Google Scholar] [CrossRef]
- Lima, J.P.; dos Santos, L.V.; Sasse, E.C.; Lima, C.S.; Sasse, A.D. Camptothecins compared with etoposide in combination with platinum analog in extensive stage small cell lung cancer: Systematic review with meta-analysis. J. Thorac. Oncol. 2010, 5, 1986–1993. [Google Scholar] [CrossRef] [Green Version]
- Jiang, J.; Liang, X.; Zhou, X.; Huang, L.; Huang, R.; Chu, Z.; Zhan, Q. A meta-analysis of randomized controlled trials comparing irinotecan/platinum with etoposide/platinum in patients with previously untreated extensive-stage small cell lung cancer. J. Thorac. Oncol. 2010, 5, 867–873. [Google Scholar] [CrossRef] [Green Version]
- Noda, K.; Nishiwaki, Y.; Kawahara, M.; Negoro, S.; Sugiura, T.; Yokoyama, A.; Fukuoka, M.; Mori, K.; Watanabe, K.; Tamura, T.; et al. Irinotecan plus cisplatin compared with etoposide plus cisplatin for extensive small-cell lung cancer. N. Engl. J. Med. 2002, 346, 85–91. [Google Scholar] [CrossRef]
- White, I.R. Network meta-analysis. Stata J. 2015, 15, 951–985. [Google Scholar] [CrossRef] [Green Version]
- Tonin, F.S.; Rotta, I.; Mendes, A.M.; Pontarolo, R. Network meta-analysis: A technique to gather evidence from direct and indirect comparisons. Pharm. Pract. (Granada) 2017, 15, 943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lhermusier, T.; Lipinski, M.J.; Tantry, U.S.; Escarcega, R.O.; Baker, N.; Bliden, K.P.; Magalhaes, M.A.; Ota, H.; Tian, W.; Pendyala, L.; et al. Meta-analysis of direct and indirect comparison of ticagrelor and prasugrel effects on platelet reactivity. Am. J. Cardiol. 2015, 115, 716–723. [Google Scholar] [CrossRef]
- Miladinovic, B.; Chaimani, A.; Hozo, I.; Djulbegovic, B. Indirect treatment comparison. Stata J. 2014, 14, 76–86. [Google Scholar] [CrossRef] [Green Version]
- König, J.; Krahn, U.; Binder, H. Visualizing the flow of evidence in network meta-analysis and characterizing mixed treatment comparisons. Stat. Med. 2013, 32, 5414–5429. [Google Scholar] [CrossRef] [PubMed]
- Jansen, J.P.; Fleurence, R.; Devine, B.; Itzler, R.; Barrett, A.; Hawkins, N.; Lee, K.; Boersma, C.; Annemans, L.; Cappelleri, J.C. Interpreting indirect treatment comparisons and network meta-analysis for health-care decision making: Report of the ISPOR Task Force on Indirect Treatment Comparisons Good Research Practices: Part 1. Value Health 2011, 14, 417–428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, G.; Ades, A.E. Combination of direct and indirect evidence in mixed treatment comparisons. Stat. Med. 2004, 23, 3105–3124. [Google Scholar] [CrossRef] [PubMed]
- Lumley, T. Network meta-analysis for indirect treatment comparisons. Stat. Med. 2002, 21, 2313–2324. [Google Scholar] [CrossRef]
- Bucher, H.C.; Guyatt, G.H.; Griffith, L.E.; Walter, S.D. The results of direct and indirect treatment comparisons in meta-analysis of randomized controlled trials. J. Clin. Epidemiol. 1997, 50, 683–691. [Google Scholar] [CrossRef]
- PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/ (accessed on 29 December 2020).
- Embase. Available online: https://www.embase.com/login (accessed on 29 December 2020).
- Cochrane Central Register of Controlled Trials [CENTRAL]. Available online: https://www.cochranelibrary.com/ (accessed on 29 December 2020).
- SCOPUS. Available online: https://0-www-scopus-com.brum.beds.ac.uk/home.uri (accessed on 29 December 2020).
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, M. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [Green Version]
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.A.; Straus, S.; Thorlund, K.; Jansen, J.P.; et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: Checklist and explanations. Ann. Intern. Med. 2015, 162, 777–784. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019. [Google Scholar]
- Hoaglin, D.C.; Hawkins, N.; Jansen, J.P.; Scott, D.A.; Itzler, R.; Cappelleri, J.C.; Boersma, C.; Thompson, D.; Larholt, K.M.; Diaz, M.; et al. Conducting indirect-treatment-comparison and network-meta-analysis studies: Report of the ISPOR Task Force on Indirect Treatment Comparisons Good Research Practices: Part 2. Value Health 2011, 14, 429–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jansen, J.P.; Crawford, B.; Bergman, G.; Stam, W. Bayesian meta-analysis of multiple treatment comparisons: An introduction to mixed treatment comparisons. Value Health 2008, 11, 956–964. [Google Scholar] [CrossRef] [Green Version]
- Dias, S.; Welton, N.J.; Sutton, A.J.; Caldwell, D.M.; Lu, G.; Ades, A. Evidence synthesis for decision making 4: Inconsistency in networks of evidence based on randomized controlled trials. Med. Decis. Mak. 2013, 33, 641–656. [Google Scholar] [CrossRef] [Green Version]
- Dias, S.; Sutton, A.J.; Welton, N.J.; Ades, A. Evidence synthesis for decision making 3: Heterogenei-ty—subgroups, meta-regression, bias, and bias-adjustment. Med. Decis. Mak. 2013, 33, 618–640. [Google Scholar] [CrossRef] [Green Version]
- Dias, S.; Sutton, A.J.; Ades, A.; Welton, N.J. Evidence synthesis for decision making 2: A generalized linear modeling framework for pairwise and network meta-analysis of randomized controlled trials. Med. Decis. Mak. 2013, 33, 607–617. [Google Scholar] [CrossRef] [Green Version]
- Salanti, G.; Ades, A.E.; Ioannidis, J.P. Graphical methods and numerical summaries for presenting results from multiple-treatment meta-analysis: An overview and tutorial. J. Clin. Epidemiol. 2011, 64, 163–171. [Google Scholar] [CrossRef]
- Brooks, S.P.; Roberts, G.O. Convergence assessment techniques for Markov chain Monte Carlo. Stat. Comput. 1998, 8, 319–335. [Google Scholar] [CrossRef]
- Brooks, S.P.; Gelman, A. General methods for monitoring convergence of iterative simulations. J. Comput. Graph. Stat. 1998, 7, 434–455. [Google Scholar]
- Sun, Y.; Cheng, Y.; Hao, X.; Wang, J.; Hu, C.; Han, B.; Liu, X.; Zhang, L.; Wan, H.; Xia, Z.; et al. Randomized phase III trial of amrubicin/cisplatin versus etoposide/cisplatin as first-line treatment for extensive small-cell lung cancer. BMC Cancer 2016, 16, 265. [Google Scholar] [CrossRef] [Green Version]
- Satouchi, M.; Kotani, Y.; Shibata, T.; Ando, M.; Nakagawa, K.; Yamamoto, N.; Ichinose, Y.; Ohe, Y.; Nishio, M.; Hida, T.; et al. Phase III study comparing amrubicin plus cisplatin with irinotecan plus cisplatin in the treatment of extensive-disease small-cell lung cancer: JCOG 0509. J. Clin. Oncol. 2014, 32, 1262–1268. [Google Scholar] [CrossRef]
- Hanna, N.; Bunn, P.A., Jr.; Langer, C.; Einhorn, L.; Guthrie, T., Jr.; Beck, T.; Ansari, R.; Ellis, P.; Byrne, M.; Morrison, M.; et al. Randomized phase III trial comparing irinotecan/cisplatin with etoposide/cisplatin in patients with previously untreated extensive-stage disease small-cell lung cancer. J. Clin. Oncol. 2006, 24, 2038–2043. [Google Scholar] [CrossRef]
- Zatloukal, P.; Cardenal, F.; Szczesna, A.; Gorbunova, V.; Moiseyenko, V.; Zhang, X.; Cisar, L.; Soria, J.-C.; Domine, M.; Thomas, M. A multicenter international randomized phase III study comparing cisplatin in combination with irinotecan or etoposide in previously untreated small-cell lung cancer patients with extensive disease. Ann. Oncol. 2010, 21, 1810–1816. [Google Scholar] [CrossRef]
- Kim, D.W.; Kim, H.G.; Kim, J.H.; Park, K.; Kim, H.K.; Jang, J.S.; Kim, B.-S.; Kang, J.-H.; Lee, K.H.; Kim, S.-W.; et al. Randomized phase III trial of irinotecan plus cisplatin versus etoposide plus cisplatin in chemotherapy-naïve Korean patients with extensive-disease small cell lung cancer. Cancer Res. Treat. 2019, 51, 119–127. [Google Scholar] [CrossRef] [Green Version]
- Zhou, F.; Zhao, W.; Gong, X.; Ren, S.; Su, C.; Jiang, T.; Zhou, C. Immune-checkpoint inhibitors plus chemotherapy versus chemotherapy as first-line treatment for patients with extensive-stage small cell lung cancer. J. Immunother. Cancer 2020, 8, e001300. [Google Scholar] [CrossRef]
- Facchinetti, F.; Di Maio, M.; Tiseo, M. Adding PD-1/PD-L1 inhibitors to chemotherapy for the first-line treatment of extensive stage small cell lung cancer (SCLC): A meta-analysis of randomized trials. Cancers (Basel) 2020, 12, 2645. [Google Scholar] [CrossRef]
- Zhou, T.; Zhang, Z.; Luo, F.; Zhao, Y.; Hou, X.; Liu, T.; Wang, K.; Zhao, H.; Huang, Y.; Zhang, L. Comparison of first-line treatments for patients with extensive-stage small cell lung cancer: A sys-tematic review and network meta-analysis. JAMA Netw. Open. 2020, 3, e2015748. [Google Scholar] [CrossRef]
- Wang, B.C.; Xiao, B.Y.; Li, P.C.; Kuang, B.H.; Chen, W.B.; Li, P.D.; Lin, G.H.; Liu, Q. Efficacy and safety of first-line immunotherapy in combination with chemotherapy for patients with extensive-stage small cell lung cancer: A systematic review and network meta-analysis. J. Oncol. 2020, 2020, 2368164. [Google Scholar] [CrossRef]
- Chen, H.-L.; Tu, Y.-K.; Chang, H.-M.; Lee, T.-H.; Wu, K.-L.; Tsai, Y.-C.; Lee, M.-H.; Yang, C.-J.; Hung, J.-Y.; Chong, I.-W. Systematic Review and Network Meta-Analysis of Immune Checkpoint Inhibitors in Combination with Chemotherapy as a First-Line Therapy for Extensive-Stage Small Cell Carcinoma. Cancers 2020, 12, 3629. [Google Scholar] [CrossRef]
- Sage, P.T.; Schildberg, F.A.; Sobel, R.A.; Kuchroo, V.K.; Freeman, G.J.; Sharpe, A.H. Dendritic cell PD-L1 limits autoimmunity and follicular T cell differentiation and function. J. Immunol. 2018, 200, 2592–2602. [Google Scholar] [CrossRef]
- Sistigu, A.; Yamazaki, T.; Vacchelli, E.; Chaba, K.; Enot, D.P.; Adam, J.; Vitale, I.; Goubar, A.; Baracco, E.E.; Romedios, C.; et al. Cancer cell-autonomous contribution of type I interferon signaling to the efficacy of chemotherapy. Nat. Med. 2014, 20, 1301–1309. [Google Scholar] [CrossRef]
- Benedict, C.A.; Loewendorf, A.; Garcia, Z.; Blazar, B.R.; Janssen, E.M. Dendritic cell programming by cytomegalovirus stunts naive T cell responses via the PD-L1/PD-1 pathway. J. Immunol. 2008, 180, 4836–4847. [Google Scholar] [CrossRef] [Green Version]
- Sholl, L.M.; Hirsch, F.R.; Hwang, D.; Botling, J.; Lopez-Rios, F.; Bubendorf, L.; Mino-Kenudson, M.; Roden, A.C.; Beasley, M.B.; Borczuk, A.; et al. The promises and challenges of tumor mutation burden as an immunotherapy biomarker: A perspective from the International Association for the Study of Lung Cancer Pathology Committee. J. Thorac. Oncol. 2020, 15, 1409–1424. [Google Scholar] [CrossRef]
- Schmid, S.; Früh, M. Immune checkpoint inhibitors and small cell lung cancer: What’s new? J. Thorac. Dis. 2018, 10, S1503–S1508. [Google Scholar] [CrossRef] [PubMed]
- Mok, T.S.K.; Wu, Y.L.; Kudaba, I.; Kowalski, D.M.; Cho, B.C.; Turna, H.Z.; Castro, G.; Srimuninnimit, V.; Laktionov, K.K.; Bondarenko, I.; et al. KEYNOTE-042 Investigators Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): A randomised, open-label, controlled, phase 3 trial. Lancet 2019, 393, 1819–1830. [Google Scholar] [CrossRef]
- Hellmann, M.D.; Paz-Ares, L.; Bernabe Caro, R.; Zurawski, B.; Kim, S.W.; Carcereny Costa, E.; Park, K.; Alexandru, A.; Lupinacci, L.; de la Mora Jimenez, E.; et al. Nivolumab plus ipilimumab in advanced non-small-cell lung cancer. N. Engl. J. Med. 2019, 381, 2020–2031. [Google Scholar] [CrossRef] [PubMed]
- Socinski, M.A.; Jotte, R.M.; Cappuzzo, F.; Orlandi, F.; Stroyakovskiy, D.; Nogami, N.; Rodríguez-Abreu, D.; Moro-Sibilot, D.; Thomas, C.A.; Barlesi, F.; et al. Atezolizumab for first-line treatment of metastatic nonsquamous NSCLC. N. Engl. J. Med. 2018, 378, 2288–2301. [Google Scholar] [CrossRef] [PubMed]









Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ando, K.; Manabe, R.; Kishino, Y.; Kusumoto, S.; Yamaoka, T.; Tanaka, A.; Ohmori, T.; Ohnishi, T.; Sagara, H. Comparative Efficacy and Safety of Immunotherapeutic Regimens with PD-1/PD-L1 Inhibitors for Previously Untreated Extensive-Stage Small Cell Lung Cancer: A Systematic Review and Network Meta-Analysis. Curr. Oncol. 2021, 28, 1094-1113. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28020106
Ando K, Manabe R, Kishino Y, Kusumoto S, Yamaoka T, Tanaka A, Ohmori T, Ohnishi T, Sagara H. Comparative Efficacy and Safety of Immunotherapeutic Regimens with PD-1/PD-L1 Inhibitors for Previously Untreated Extensive-Stage Small Cell Lung Cancer: A Systematic Review and Network Meta-Analysis. Current Oncology. 2021; 28(2):1094-1113. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28020106
Chicago/Turabian StyleAndo, Koichi, Ryo Manabe, Yasunari Kishino, Sojiro Kusumoto, Toshimitsu Yamaoka, Akihiko Tanaka, Tohru Ohmori, Tsukasa Ohnishi, and Hironori Sagara. 2021. "Comparative Efficacy and Safety of Immunotherapeutic Regimens with PD-1/PD-L1 Inhibitors for Previously Untreated Extensive-Stage Small Cell Lung Cancer: A Systematic Review and Network Meta-Analysis" Current Oncology 28, no. 2: 1094-1113. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28020106