Long Term Real-World Outcomes of Trifluridine/Tipiracil in Metastatic Colorectal Cancer—A Single UK Centre Experience


Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Patient Demographics and Tumour Characteristics
3.2. Systemic Treatment Received Prior to Lonsurf
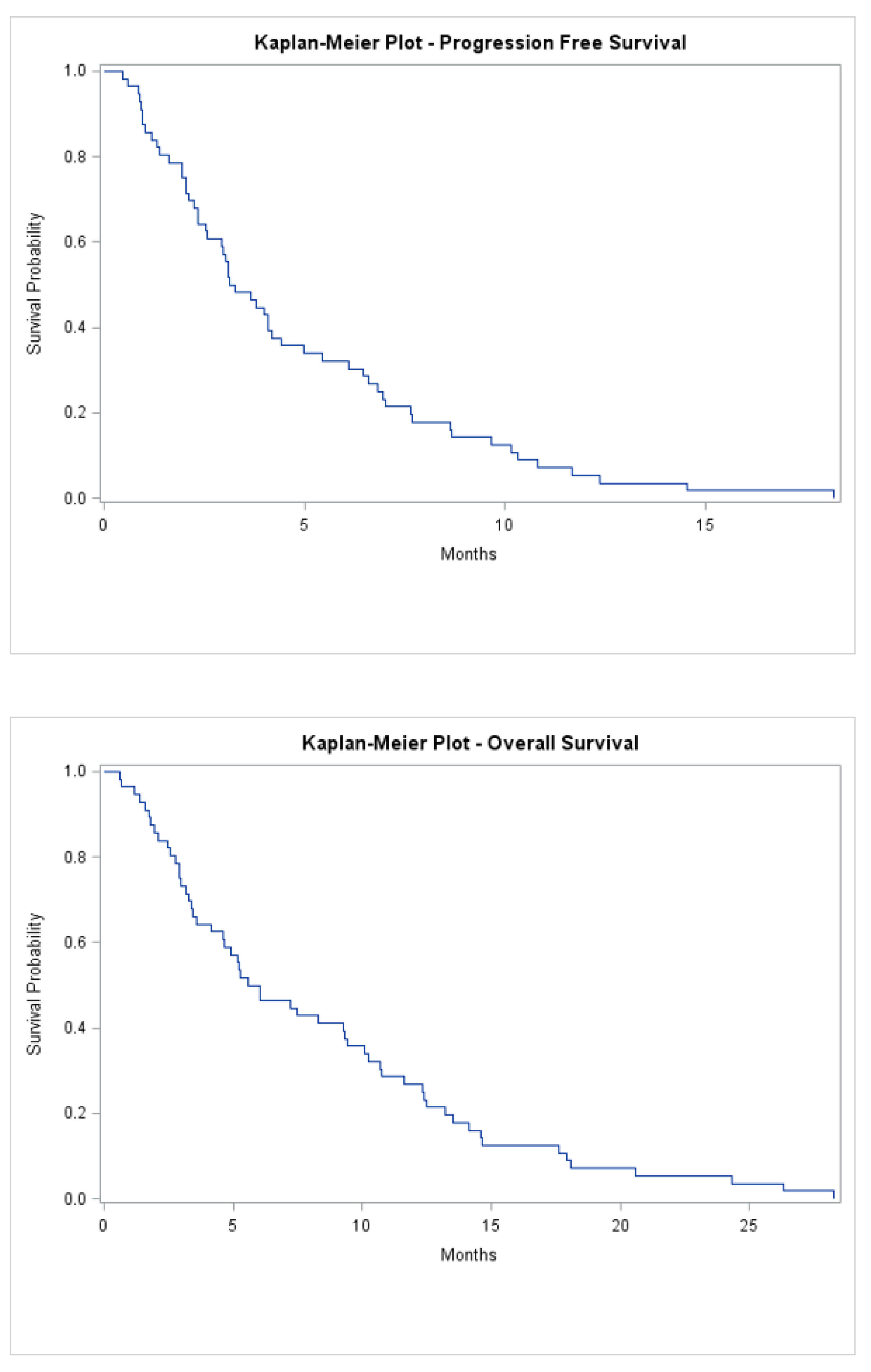
3.3. Lonsurf Treatment Details
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cancer Research UK. Cancer Mortality for Common Cancers. Available online: https://www.cancerresearchuk.org/health-professional/cancer-statistics/mortality/common-cancers-compared/ (accessed on 31 July 2020).
- Grothey, A.; Sargent, D.; Goldberg, R.M.; Schmoll, H.J. Survival of patients with advanced colorectal cancer improves with the availability of fluorouracil-leucovorin, irinotecan, and oxaliplatin in the course of treatment. J. Clin. Oncol. 2004, 22, 1209–1214. [Google Scholar] [CrossRef] [PubMed]
- Van Cutsem, E.; Cervantes, A.; Nordlinger, B.; Arnold, D. Metastatic colorectal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2014, 25, iii1–iii9. [Google Scholar] [CrossRef] [PubMed]
- Temmink, O.H.; Emura, T.; de Bruin, M.; Fukushima, M.; Peters, G.J. Therapeutic potential of the dual-targeted TAS-102 formulation in the treatment of gastrointestinal malignancies. Cancer Sci. 2007, 98, 779–789. [Google Scholar] [CrossRef] [PubMed]
- Yoshino, T.; Mizunuma, N.; Yamazaki, K.; Nishina, T.; Komatsu, Y.; Baba, H.; Tsuji, A.; Yamaguchi, K.; Muro, K.; Sugimoto, N.; et al. TAS-102 monotherapy for pretreated metastatic colorectal cancer: A double-blind, randomised, placebo-controlled phase 2 trial. Lancet Oncol. 2012, 13, 993–1001. [Google Scholar] [CrossRef]
- Mayer, R.J.; Van Cutsem, E.; Falcone, A.; Yoshino, T.; Garcia-Carbonero, R.; Mizunuma, N.; Yamazaki, K.; Shimada, Y.; Tabernero, J.; Komatsu, Y.; et al. Randomized trial of TAS-102 for refractory metastatic colorectal cancer. N. Engl. J. Med. 2015, 372, 1909–1919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- New Zealand: Drugsite Trust. FDA Approves Lonsurf. Available online: https://www.drugs.com/newdrugs/fda-approves-lonsurf-tipiracil-trifluridine-advanced-colorectal-cancer-4265.html/ (accessed on 31 July 2020).
- UK: National Institute for Health and Care Excellence. Trifluridine-Tipiracil for Previously Treated Metastatic Colorectal Cancer. Available online: https://www.nice.org.uk/guidance/TA405/chapter/1-Recommendations (accessed on 31 July 2020).
- Bachet, J.B.; Wyrwicz, L.; Price, T.; Cremolini, C.; Phelip, J.M.; Portales, F.; Ozet, A.; Cicin, I.; Atlan, D.; Becquart, M.; et al. Safety, efficacy and patient-reported outcomes with trifluridine/tipiracil in pretreated metastatic colorectal cancer: Results of the PRECONNECT study. ESMO Open 2020, 5, e000698. [Google Scholar] [CrossRef] [PubMed]
- Stavraka, C.; Pouptsis, A.; Synowiec, A.; Aggelis, V.; Satterthwaite, L.; Khan, S.; Chauhan, M.; Holden, C.E.; Young, S.; Karampera, C.; et al. Trifluridine/tipiracil in metastatic colorectal cancer: An updated multicentre real-world analysis on efficacy, safety and predictive factors. Ann. Oncol. 2019, 30, v198–v252. [Google Scholar] [CrossRef]
- Tilby, M.; Escola, C.; Ellison, C.; Narramneni, L.; King, M.; Grumett, S.; Jain, A. Trifluridine-tipiracil for the treatment of metastatic colorectal cancer patients: UK multicentre real-world experience. Ann. Oncol. 2019, 30, IV27. [Google Scholar] [CrossRef]
- Samawi, H.H.; Brezden-Masley, C.; Afzal, A.R.; Cheung, W.Y.; Dolley, A. Real-world use of trifluridine/tipiracil for patients with metastatic colorectal cancer in Canada. Curr. Oncol. 2019, 26, 319–329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andersen, S.E.; Andersen, I.B.; Jensen, B.V.; Pfeiffer, P.; Ota, T.; Larsen, J.S. A systematic review of observational studies of trifluridine/tipiracil (TAS-102) for metastatic colorectal cancer. Acta Oncol. 2019, 58, 1149–1157. [Google Scholar] [CrossRef] [PubMed]
- Wallander, M.; Rolander, B.; Åvall-Lundqvist, E.; Elander, N.O. Real world aspects of palliative trifluridine plus tiperacil (TAS-102) in refractory metastatic colorectal cancer. J. Gastrointest. Oncol. 2020, 11, 616–625. [Google Scholar] [CrossRef] [PubMed]
- Cremolini, C.; Rossini, D.; Martinelli, E.; Pietrantonio, F.; Lonardi, S.; Noventa, S.; Tamburini, E.; Frassineti, G.L.; Mosconi, S.; Nichetti, F.; et al. Trifluridine/Tipiracil (TAS-102) in Refractory Metastatic Colorectal Cancer: A Multicenter Register in the Frame of the Italian Compassionate Use Program. Oncologist 2018, 23, 1178–1187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tabernero, J.; Argiles, G.; Sobrero, A.F.; Borg, C.; Ohtsu, A.; Mayer, R.J.; Vidot, L.; Moreno Vera, S.R.; Van Cutsem, E. Effect of trifluridine/tipiracil in patients treated in RECOURSE by prognostic factors at baseline: An exploratory analysis. ESMO Open. 2020, 5, e000752. [Google Scholar] [CrossRef] [PubMed]
- Pfeiffer, P.; Yilmaz, M.; Möller, S.; Zitnjak, D.; Krogh, M.; Petersen, L.N.; Poulsen, L.Ø.; Winther, S.B.; Thomsen, K.G.; Qvortrup, C. TAS-102 with or without bevacizumab in patients with chemorefractory metastatic colorectal cancer: An investigator-initiated, open-label, randomised, phase 2 trial. Lancet Oncol. 2020, 21, 412–420. [Google Scholar] [CrossRef]
- Yoshida, Y.; Yamada, T.; Kamiyama, H.; Kosugi, C.; Ishibashi, K.; Yoshida, H.; Ishida, H.; Yamaguchi, S.; Kuramochi, H.; Fukazawa, A.; et al. Combination of TAS-102 and bevacizumab as third-line treatment for metastatic colorectal cancer: TAS-CC3 study. Int. J. Clin. Oncol. 2021, 26, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Yoshino, T.; Oki, E.; Nozawa, H.; Eguchi-Nakajima, T.; Taniguchi, H.; Morita, S.; Takenaka, N.; Ozawa, D.; Shirao, K. Rationale and design of the TRUSTY study: A randomized, multicentre, open-label phase II/III study of tri- fluridine/tipiracil plus bevacizumab versus irinotecan fluoropyrimidine plus bevacizumab as second-line treatment in patients with metastatic colorectal cancer progressive during or following first-line oxapliplatin- based chemotherapy. ESMO Open 2018, 3, e0000411. [Google Scholar] [CrossRef] [Green Version]
- Van Cutsem, E.; Danielewicz, I.; Saunders, M.P.; Pfeiffer, P.; Argilés, G.; Borg, C.; Glynne-Jones, R.; Punt, C.J.A.; Van de Wouw, A.J.; Fedyanin, M.; et al. Trifluridine/tipiracil plus bevacizumab in patients with untreated metastatic colorectal cancer ineligible for intensive therapy: The randomized TASCO1 study. Ann. Oncol. 2020, 31, 1160–1168. [Google Scholar] [CrossRef] [PubMed]
- André, T.; Saunders, M.; Kanehisa, A.; Gandossi, E.; Fougeray, R.; Amellal, N.C.; Falcone, A. First-line trifluridine/tipiracil plus bevacizumab for unresectable metastatic colorectal cancer: SOLSTICE study design. Future Oncol. 2020, 16, 21–29. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study [Reference] | Country | Study Type | Number of Patients | Performance Status | RAS Mutant (%) | Previous Lines of Treatment | Median Duration of Treatment (months) | Median PFS (months) | Median OS (months) |
|---|---|---|---|---|---|---|---|---|---|
| RECOURSE [6] | International | Phase III trial | 800 | 0–1 | 51 | ≥2 | 1.5 | 2 | 7.1 |
| PRECONNECT [9] | International | Phase IIIb trial | 798 | 0–1 in 97% | 52.6 | 36.1% ≤2 30.6% 3 32.8% ≥4 | 2.8 | 3 | Not reported |
| Stavraka et al. [10] | UK | Abstract (retrospective) | 236 | 0–1 in 90% | Not reported | ≥2 | 3 | 3.3 | 7.6 |
| Tilby et al. [11] | UK | Abstract (retrospective) | 91 | 0–1 in 96% | 53 | Not reported | 4.3 | 4.1 | 8.7 |
| Samawi et al. [12] | Canada | Retrospective study | 717 | Not stated | 60 | Not reported | 2.5 | Not reported | Not reported |
| Anderson et al. [13] | Japan, Europe | Meta-analysis | 1008 | 0–1 in 93% | 62 | 34% ≤2 35% 3 31% ≥4 | Pooled data not reported, individual studies ranged 1–3 | 2.2 | 6.6 |
| Wallander et al. [14] | Sweden | Retrospective study | 48 | 0–1 in 94% | 60 | 73% ≤2 23% 3 2% ≥4 | Not reported | 2.3 | 6.4 |
| Cremolini et al. [15] | Italy | Retrospective study | 341 | 0–1 in 98% | 59 | 33.4% ≤2 28.1% 3 38.4% ≥4 | Not reported | 2.4 | 6.2 |
| Variable | Value (n) | (%) |
|---|---|---|
| Baseline characteristics | ||
| Gender | ||
| Male | 33 | 59 |
| Female | 23 | 41 |
| Median age at diagnosis | 61 | Range 37–79 |
| Location of tumour | ||
| Left-sided | 40 | 71.4 |
| Right-sided | 15 | 26.8 |
| Other | 1 | 1.8 |
| Staging at diagnosis | ||
| T | ||
| 1 | 0 | 0 |
| 2 | 2 | 3.6 |
| 3 | 22 | 39.3 |
| 4 | 16 | 28.6 |
| N | ||
| 0 | 2 | 3.6 |
| 1 | 13 | 23.2 |
| 2 | 25 | 44.6 |
| M | ||
| 0 | 16 | 30.8 |
| 1 | 36 | 69.2 |
| Median interval until metastasis (months) | 11 | Range 2–108 |
| Site of metastasis | ||
| Lung | 21 | 37.5 |
| Liver | 39 | 69.6 |
| Peritoneum | 8 | 14.2 |
| Nodal | 8 | 14.2 |
| Ovary | 2 | 3.6 |
| Multiple sites of metastases? | ||
| Yes | 16 | 28.6 |
| No | 40 | 71.4 |
| Histology | ||
| Median number of positive nodes | 4 | Range 0–18 |
| Grade of tumour | ||
| 1 | 0 | 0 |
| 2 | 32 | 57.1 |
| 3 | 6 | 10.7 |
| Not stated or not operated | 18 | 32.1 |
| Extramural vascular invasion | ||
| Positive | 16 | 28.6 |
| Negative | 15 | 26.8 |
| Not stated | 25 | 44.6 |
| RAS mutation | ||
| Mutant | 23 | 41.4 |
| Wildtype | 25 | 44.6 |
| Not tested | 8 | 14.2 |
| BRAF mutation | ||
| Mutant | 1 | 1.8 |
| Wildtype | 14 | 25 |
| Not tested | 41 | 73.2 |
| Systemic treatment details | ||
| Adjuvant chemo received | ||
| Yes | 22 | 39.3 |
| No | 34 | 60.7 |
| Regimen | ||
| FOLFOX | 12 | 54.5 |
| FOLFIRI | 1 | 1.8 |
| CAPOX | 2 | 3.6 |
| 5′FU | 1 | 1.8 |
| Capecitabine | 1 | 1.8 |
| Not stated | 5 | 8.9 |
| Median number of cycles received | 12 | Range 2–14 |
| Lines received prior to LONSURF | ||
| 1 | 0 | 0 |
| 2 | 52 | 92.9 |
| 3 | 3 | 5.4 |
| Not stated | 1 | 1.8 |
| Median FOLFOX received | 12 | Range 4–31 |
| Median FOLFIRI received | 12 | Range 3–43 |
| Parameters | PFS | OS | ||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Age at diagnosis (≥65 vs. <65) | 0.9 (0.4–1.7) | 0.78 | 2.1 (1.1–4.2) | 0.03 |
| Tumour location (right vs. left) | 1.5 (0.6–3.7) | 0.43 | 0.9 (0.4–2.3) | 0.86 |
| Metastatic at diagnosis (yes vs. no) | 2.7 (1.3–5.9) | 0.009 | 2 (1–4) | 0.05 |
| RAS status (wildtype vs. mutant) | 0.7 (0.3–1.4) | 0.31 | 1.7 (0.8–3.4) | 0.14 |
| Lung only metastasis (yes vs. no) | 0.8 (0.2–3.1) | 0.81 | 0.7 (0.2–2.6) | 0.64 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tong, D.; Wang, L.; Mendis, J.; Essapen, S. Long Term Real-World Outcomes of Trifluridine/Tipiracil in Metastatic Colorectal Cancer—A Single UK Centre Experience. Curr. Oncol. 2021, 28, 2260-2269. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28030208
Tong D, Wang L, Mendis J, Essapen S. Long Term Real-World Outcomes of Trifluridine/Tipiracil in Metastatic Colorectal Cancer—A Single UK Centre Experience. Current Oncology. 2021; 28(3):2260-2269. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28030208
Chicago/Turabian StyleTong, Daniel, Lei Wang, Jeewaka Mendis, and Sharadah Essapen. 2021. "Long Term Real-World Outcomes of Trifluridine/Tipiracil in Metastatic Colorectal Cancer—A Single UK Centre Experience" Current Oncology 28, no. 3: 2260-2269. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28030208