The Role of Administrative and Secondary Data in Estimating the Costs and Effects of School and Workplace Closures due to the COVID-19 Pandemic

 , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Model
2.2. Epidemiological Parameters
2.3. Cost Parameters
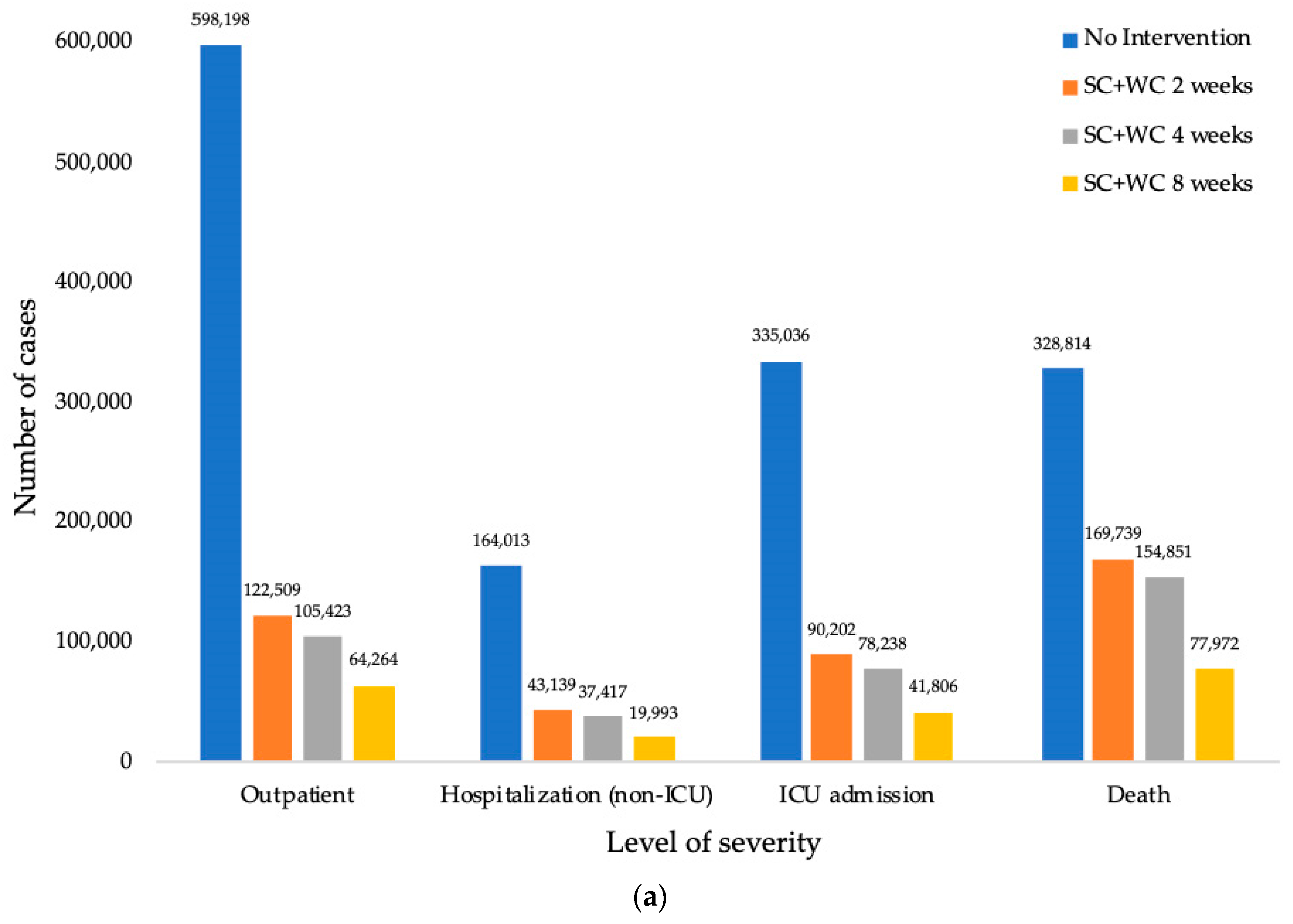
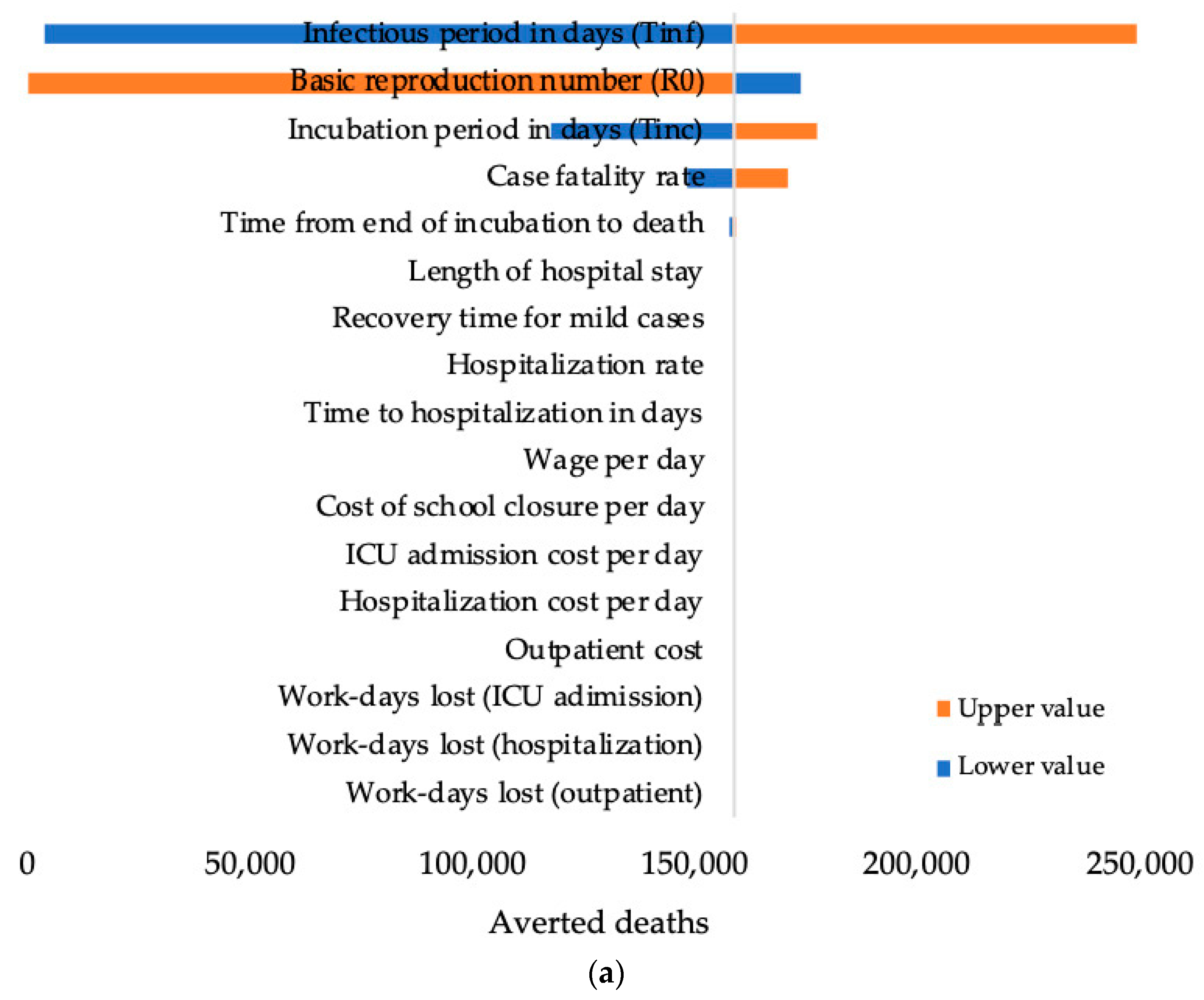
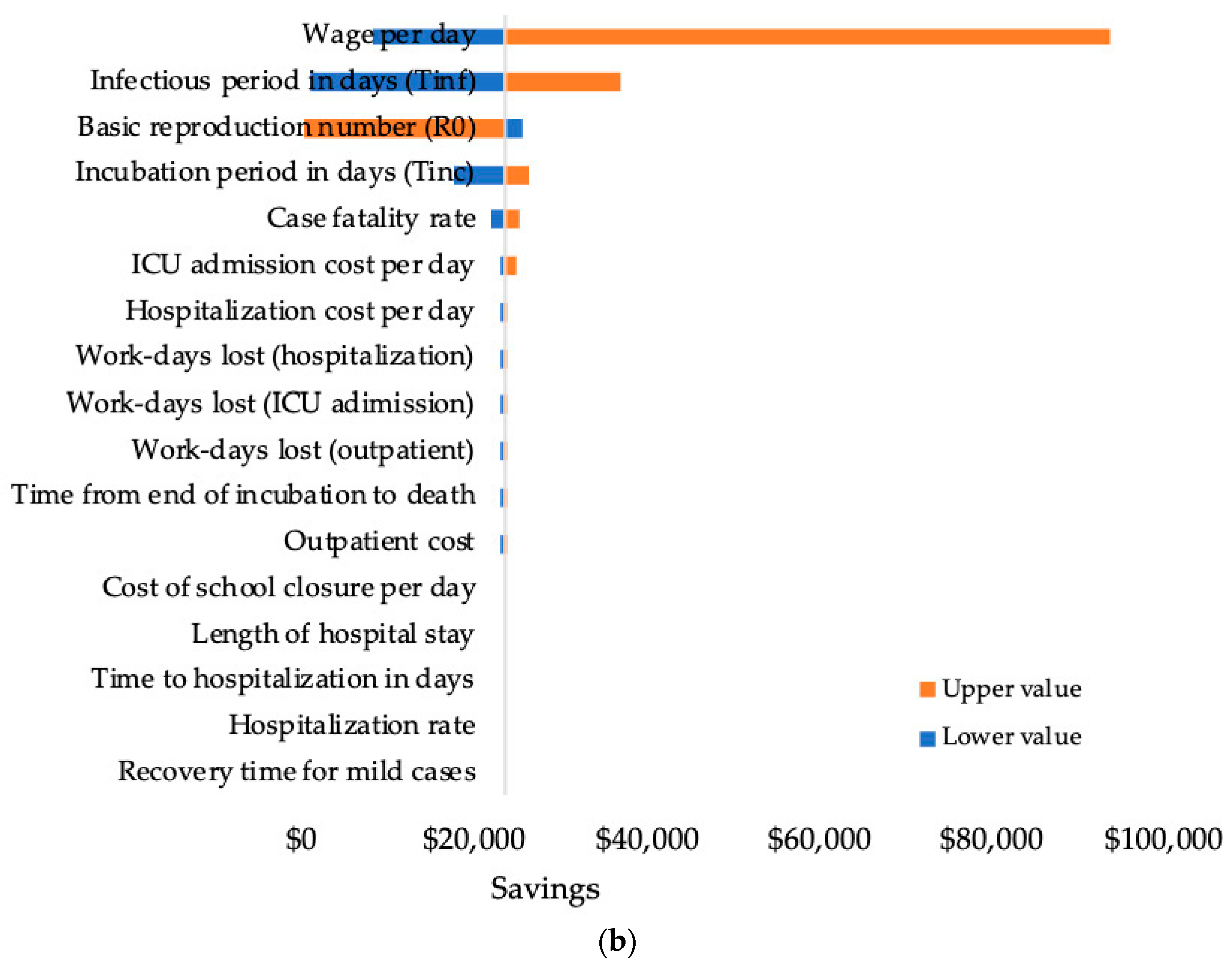
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- WHO. Coronavirus Disease 2019 (COVID-19) Situation Report—51. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200311-sitrep-51-covid-19.pdf?sfvrsn=1ba62e57_10 (accessed on 30 March 2020).
- WHO. Critical Preparedness, Readiness and Response Actions for COVID-19. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/critical-preparedness-readiness-and-response-actions-for-covid-19 (accessed on 30 March 2020).
- The Jakarta Administration. COVID-19 Monitoring Data. Available online: https://corona.jakarta.go.id/data (accessed on 30 March 2020).
- Jackson, C.; Vynnycky, E.; Hawker, J.; Olowokure, B.; Mangtani, P. School closures and influenza: Systematic review of epidemiological studies. BMJ Open 2013, 3, e002149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perlroth, D.J.; Glass, R.J.; Davey, V.J.; Cannon, D.; Garber, A.M.; Owens, D.K. Health outcomes and costs of community mitigation strategies for an influenza pandemic in the United States. Clin. Infect. Dis. 2010, 50, 165–174. [Google Scholar] [CrossRef] [PubMed]
- Halder, N.; Kelso, J.K.; Milne, G.J. Cost-Effective Strategies for Mitigating a Future Influenza Pandemic with H1N1 2009 Characteristics. PLoS ONE 2011, 6, e22087. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goh, G. Epidemic Calculator. Available online: http://gabgoh.github.io/COVID/index.html (accessed on 30 March 2020).
- Statistics of Jakarta. Population by Age and Sex in 2018. Available online: https://jakarta.bps.go.id/dynamictable/2019/09/16/58/jumlah-penduduk-provinsi-dki-jakarta-menurut-kelompok-umur-dan-jenis-kelamin-2018-.html (accessed on 30 March 2020).
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.S.M.; Lau, E.H.Y.; Wong, J.Y.; et al. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N. Engl. J. Med. 2020, 382, 1199–1207. [Google Scholar] [CrossRef] [PubMed]
- Verity, R.; Okell, L.C.; Dorigatti, I.; Winskill, P.; Whittaker, C.; Imai, N.; Cuomo-Dannenburg, G.; Thompson, H.; Walker, P.G.T.; Fu, H.; et al. Estimates of the severity of coronavirus disease 2019: A model-based analysis. Lancet Infect. Dis. 2020, 20, 669–677. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Imperial College COVID-19 Response Team. Impact of Non-Pharmaceutical Interventions (NPIs) to Reduce COVID- 19 Mortality and Healthcare Demand. Available online: https://www.imperial.ac.uk/media/imperial-college/medicine/sph/ide/gida-fellowships/Imperial-College-COVID19-NPI-modelling-16-03-2020.pdf (accessed on 30 March 2020).
- Hilfi, L.; Setiawati, E.P.; Djuhaeni, H.; Paramita, S.A.; Komara, R. The Differences of Unit Cost Calculation by Activity Based Costing (ABC) Method and Double Distribution (DD) Method for Category 2 of Pulmonary TB Patients in Outpatient and Inpatient of Lung Hospital. JKKI 2015, 4, 109–116. [Google Scholar]
- Statistics of Jakarta. Life Expectancy Years. Available online: https://ipm.bps.go.id/data/provinsi/metode/baru/3100 (accessed on 30 March 2020).
- Statistics of Indonesia. GDP Per Capita. Available online: https://www.bps.go.id/dynamictable/2015/10/07/957/-seri-2010-produk-domestik-regional-bruto-per-kapita-atas-dasar-harga-berlaku-menurut-provinsi-2010-2018-ribu-rupiah-.html (accessed on 30 March 2020).
- The Jakarta Administration. Kartu Jakarta Pintar Plus. Available online: https://kjp.jakarta.go.id/kjp2/public/informasi_umum (accessed on 30 March 2020).
- The Central Bank of Indonesia. Exchange Rate Information. Available online: https://www.bi.go.id/id/moneter/informasi-kurs/transaksi-bi/Default.aspx (accessed on 30 March 2020).
- Earn, D.J.; He, D.; Loeb, M.B.; Fonseca, K.; Lee, B.E.; Dushoff, J. Effects of school closure on incidence of pandemic influenza in Alberta, Canada. Ann. Intern. Med. 2012, 156, 173–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cauchemez, S.; Valleron, A.-J.; Boelle, P.-Y.; Flahault, A.; Ferguson, N.M. Estimating the impact of school closure on influenza transmission from sentinel data. Nature 2008, 452, 750–754. [Google Scholar] [CrossRef] [PubMed]
- Eames, K.T.; Tilston, N.L.; Brooks-Pollock, E.; Edmunds, W.J. Measured Dynamic Social Contact Patterns Explain the Spread of H1N1v Influenza. PLoS Comput. Biol. 2012, 8, e1002425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jackson, C.; Mangtani, P.; Hawker, J.; Olowokure, B.; Vynnycky, E. The Effects of School Closures on Influenza Outbreaks and Pandemics: Systematic Review of Simulation Studies. PLoS ONE 2014, 9, e97297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sadique, M.S.; Adams, E.J.; Edmunds, W.J. Estimating the costs of school closure for mitigating an influenza pandemic. BMC Public Health. 2008, 8, 135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loayza, N.V.; Pennings, S. Macroeconomic Policy in the Time of COVID-19: A Primer for Developing Countries. Available online: https://openknowledge.worldbank.org/bitstream/handle/10986/33540/Macroeconomic-Policy-in-the-Time-of-COVID-19-A-Primer-for-Developing-Countries.pdf?sequence=1&isAllowed=y (accessed on 8 October 2020).
- Mao, L. Cost-effectiveness of workplace closure and travel restriction for mitigating influenza outbreaks: A network-based simulation. In Proceedings of the Second ACM SIGSPATIAL International Workshop on Use of GIS in Public Health, HealthGIS 2013, Orlando, FL, USA, 5–8 November 2013; pp. 77–84. [Google Scholar]
- Milne, G.J.; Halder, N.; Kelso, J.K. The Cost Effectiveness of Pandemic Influenza Interventions: A Pandemic Severity Based Analysis. PLoS ONE 2013, 8, e61504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nsoesie, E.O.; Beckman, R.J.; Marathe, M.V. Sensitivity Analysis of an Individual-Based Model for Simulation of Influenza Epidemics. PLoS ONE 2012, 7, e45414. [Google Scholar] [CrossRef] [PubMed]
- Cabinet Secretariat of the Republic of Indonesia. BPOM Head: Indonesia Owns Two Options in COVID-19 Vaccine Development. Available online: https://setkab.go.id/en/bpom-head-indonesia-owns-two-options-in-covid-19-vaccine-development/ (accessed on 8 October 2020).
- Baker, S.R.; Bloom, N.; Davis, S.J.; Terry, S.J. COVID-Induced Economic Uncertainty. Available online: https://www.nber.org/papers/w26983.pdf (accessed on 8 October 2020).
- World Bank. East Asia and Pacific in the Time of COVID-19 East Asia and Pacific Economic Update (April); World Bank: Washington, DC, USA, 2020. [Google Scholar] [CrossRef]
- Akhtaruzzaman, M.; Boubaker, S.; Sensoy, A. Financial contagion during COVID–19 crisis. Financ. Res. Lett. 2020, 101604. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Hu, M.; Ji, Q. Financial markets under the global pandemic of COVID-19. Financ. Res. Lett. 2020, 101528. [Google Scholar] [CrossRef] [PubMed]
- Coibion, O.; Gorodnichenko, Y.; Weber, M. Labor Markets during the COVID-19 Crisis: A Preliminary View. Available online: https://www.nber.org/papers/w27017.pdf (accessed on 8 October 2020).
- Corbet, S.; Hou, Y.; Hu, Y.; Lucey, B.; Oxley, L. Aye Corona! The contagion effects of being named Corona during the COVID-19 pandemic. Financ. Res. Lett. 2020, 101591. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Value | Ref. |
|---|---|---|
| Basic reproduction number (R0) | 2.2 (95% CI; 1.4–3.9) | [9] |
| Incubation period (Tinc) | 5.2 days (95% CI; 4.1–7.0 days) | [9] |
| Infectious period (Tinf) | 2.3 days (95% CI; 0–14.9 days) | [9] |
| Time from end of incubation to death | 21 days (95% CI; 17–25 days) | [11] |
| Length of hospital stay | 11 days (95% CI; 7–14 days) | [11] |
| Recovery time for mild cases | 24.7 days (95% CI; 22.9–28.1 days) | [11] |
| Time to hospitalization in days | 7 days (95% CI; 4–9 days) | [11] |
| Case fatality rate | 3.7% (95% CI; 3.6%–3.8%) | [10] |
| Hospitalization rate | 18.4% (95% CI; 11.0%–37.6%) | [10] |
| Illness attack rate reduction (SC + WC 2 weeks) | 42% (Rt = 1.28) | [6] |
| Illness attack rate reduction (SC + WC 4 weeks) | 44% (Rt = 1.23) | [6] |
| Illness attack rate reduction (SC + WC 8 weeks) | 54% (Rt = 1.01) | [6] |
| Wage per day | Average wage = $11.00 (Min wage = $3.39; Max wage = $45.68) | [15] |
| Cost for school closure per day | Average cost = $1.26 (Min cost = $0.85; Max cost = $1.59) | [16] |
| Outpatient cost | Average tariff = $24.20 (Min tariff = $16.01; Max tariff = $28.80) | [13] |
| Hospitalization cost per day | Average tariff = $162.11 (Min tariff = $81.57; Max tariff = $364.29) | [13] |
| ICU admission cost per day | Average tariff = $219.15 (Min tariff = $110.27; Max tariff = $492.46) | [13] |
| Workdays lost (outpatient) | 25 (95% CI; 23–28) | [10,11] |
| Workdays lost (hospitalization) | 36 (95% CI; 30–42) | [10,11] |
| Workdays lost (ICU admission) | 44 (95% CI; 34–54) | [10,11] |
| Number of people | 10.5 million | [8] |
| Life expectancy | 7267 years | [14] |
| Time horizon | 1 year | [7] |
| (a) Cost Analysis Results | ||||||||
| Intervention | Costs (Million $) | Savings (Million $) | Averted Deaths | |||||
| Healthcare Cost | Cost of SC | Productivity Loss due to WC | Productivity Loss due to Illness | Total Pandemic Cost | ||||
| No Intervention | $1701.99 | - | - | $48,215.89 | $49,917.88 | - | - | |
| SC + WC 2 weeks | $455.48 | $20.95 | $1102.61 | $24,782.81 | $26,361.85 | $23,556.03 | 159,075 | |
| SC + WC 4 weeks | $395.04 | $41.90 | $2205.22 | $22,604.64 | $25,246.80 | $24,671.08 | 173,963 | |
| SC + WC 8 weeks | $211.28 | $83.80 | $4410.43 | $11,386.75 | $16,092.27 | $33,825.61 | 250,842 | |
| (b) Percentage Change in the Cost due to Intervention | ||||||||
| Intervention | Healthcare Cost | Cost of SC | Productivity Loss due to WC | Productivity Loss due to Illness | ||||
| % | ↓ | % | ↑ | % | ↑ | % | ↓ | |
| No Intervention | 3.41% | 0.00% | 0.00% | 96.59% | ||||
| SC + WC 2 weeks | 1.73% | 1.68% | 0.08% | 0.08% | 4.18% | 4.18% | 94.01% | 2.58% |
| SC + WC 4 weeks | 1.56% | 1.85% | 0.17% | 0.17% | 8.73% | 8.73% | 89.53% | 7.06% |
| SC + WC 8 weeks | 1.31% | 2.10% | 0.52% | 0.52% | 27.41% | 27.41% | 70.76% | 25.83% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suwantika, A.A.; Zakiyah, N.; Diantini, A.; Abdulah, R.; Postma, M.J. The Role of Administrative and Secondary Data in Estimating the Costs and Effects of School and Workplace Closures due to the COVID-19 Pandemic. Data 2020, 5, 98. https://0-doi-org.brum.beds.ac.uk/10.3390/data5040098
Suwantika AA, Zakiyah N, Diantini A, Abdulah R, Postma MJ. The Role of Administrative and Secondary Data in Estimating the Costs and Effects of School and Workplace Closures due to the COVID-19 Pandemic. Data. 2020; 5(4):98. https://0-doi-org.brum.beds.ac.uk/10.3390/data5040098
Chicago/Turabian StyleSuwantika, Auliya A., Neily Zakiyah, Ajeng Diantini, Rizky Abdulah, and Maarten J. Postma. 2020. "The Role of Administrative and Secondary Data in Estimating the Costs and Effects of School and Workplace Closures due to the COVID-19 Pandemic" Data 5, no. 4: 98. https://0-doi-org.brum.beds.ac.uk/10.3390/data5040098