Liver Fibrosis Biomarkers Accurately Exclude Advanced Fibrosis and Are Associated with Higher Cardiovascular Risk Scores in Patients with NAFLD or Viral Chronic Liver Disease

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Results
2.1. Characteristics of Study Cohort
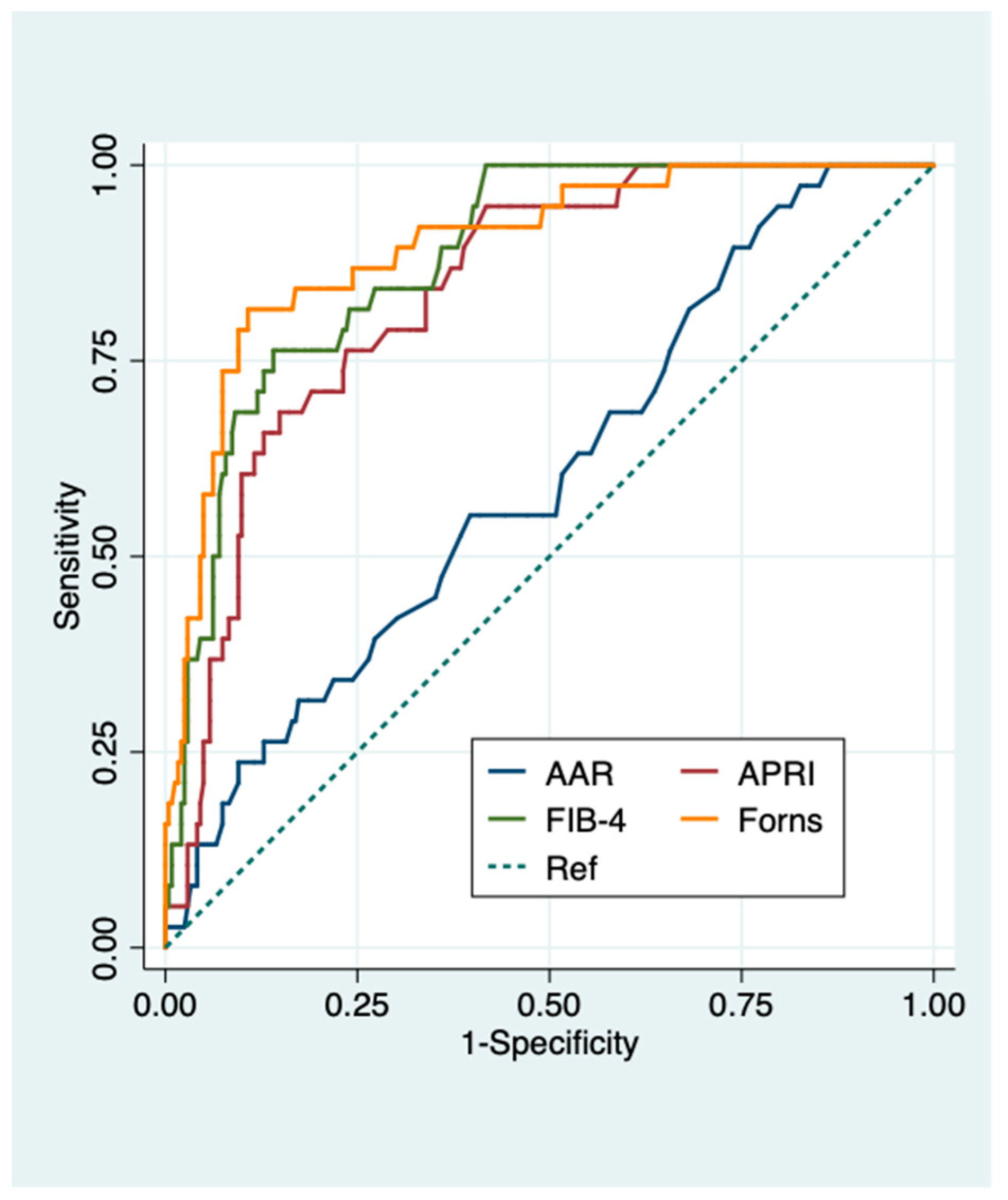
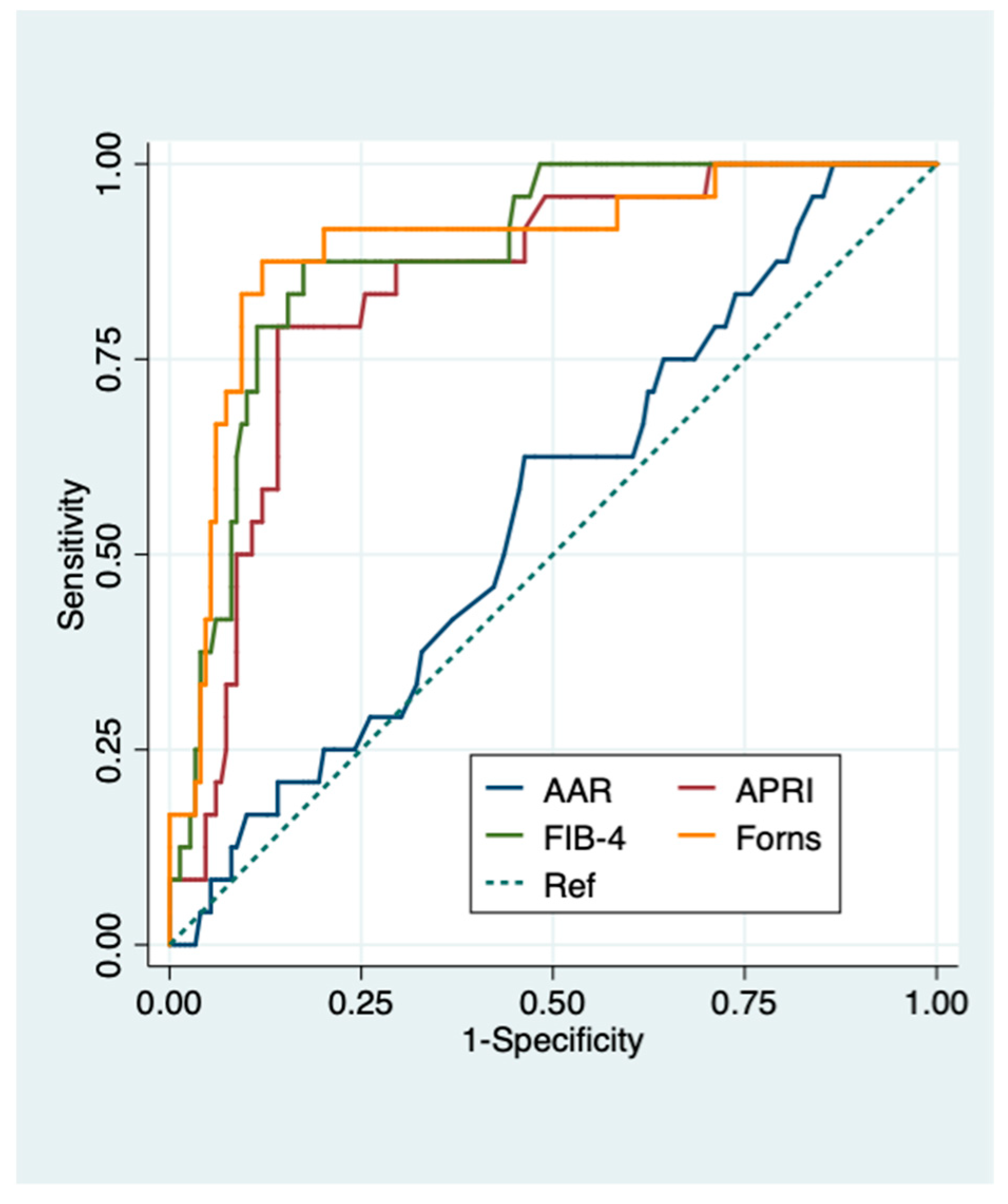
2.2. Diagnostic Performance of Liver Fibrosis Biomarkers
2.3. Associations of Liver Fibrosis Biomarkers with Cardiovascular Risk Scoring Systems
3. Discussion
3.1. Liver Fibrosis Biomarkers Accurately Exclude Advanced Fibrosis in Metabolic and Viral Chronic Liver Disease
3.2. Clinical Implications of Findings: Proportion of Spared Biopsies and NAFLD Screening
3.3. Liver Fibrosis Biomarkers are Correlated with CVR Scores
3.4. Clinical Implications of Findings: May Liver Fibrosis Biomarkers Be Used as an Adjunct to Traditional CVR Scoring Systems?
3.5. Strengths and Limitations
4. Materials and Methods
4.1. Histological Evaluation
4.2. Liver Fibrosis Biomarkers
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AAR | AST-to-ALT ratio |
| ALT | alanine aminotransferase |
| APRI | AST-to platelet ratio index |
| AST | aspartate aminotransferase |
| AUROC | area under the receiver operating characteristic |
| BMI | body mass index |
| CI | confidence intervals |
| CVD | cardiovascular disease |
| CVR | cardiovascular risk |
| FIB-4 | fibrosis-4 |
| FRS | Framingham risk score |
| GGT | gamma-glutamyltransferase |
| HBV | hepatitis B virus |
| HCC | hepatocellular carcinoma |
| HCV | hepatitis C virus |
| HDL | high-density lipopoprotein |
| HFS | hepamet fibrosis score |
| HOMA-IR | homeostasis model assessment of insulin resistance |
| IFG | impaired fasting glycemia |
| LDL | low-density lipopoprotein |
| NAFLD | nonalcoholic fatty liver disease |
| NASH | nonalcoholic steatohepatitis |
| NFS | NAFLD fibrosis score |
| NPV | negative predictive value |
| PPV | positive predictive value |
| ROC | receiver operating characteristic |
References
- Bataller, R.; Brenner, D.A. Liver fibrosis. J. Clin. Invest. 2005, 115, 209–218. [Google Scholar] [CrossRef] [PubMed]
- Udompap, P.; Kim, D.; Kim, W.R. Current and Future Burden of Chronic Nonmalignant Liver Disease. Clin. Gastroenterol. Hepatol. 2015, 13, 2031–2041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finelli, C.; Tarantino, G. What is the role of adiponectin in obesity related non-alcoholic fatty liver disease? World J. Gastroenterol. 2013, 19, 802–812. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Italian Association for the Study of the Liver (AISF). AISF position paper on nonalcoholic fatty liver disease (NAFLD): Updates and future directions. Dig. Liver Dis. 2017, 49, 471–483. [Google Scholar] [CrossRef] [PubMed]
- Duffell, E.F.; Hedrich, D.; Mardh, O.; Mozalevskis, A. Towards elimination of hepatitis B and C in European Union and European Economic Area countries: Monitoring the World Health Organization’s global health sector strategy core indicators and scaling up key interventions. Euro Surveill. 2017, 22, 30476. [Google Scholar] [CrossRef] [Green Version]
- Ekstedt, M.; Hagström, H.; Nasr, P.; Fredrikson, M.; Stål, P.; Kechagias, S.; Hultcrantz, R. Fibrosis stage is the strongest predictor for disease-specific mortality in NAFLD after up to 33 years of follow-up. Hepatology 2015, 61, 1547–1554. [Google Scholar] [CrossRef] [Green Version]
- Angulo, P.; Kleiner, D.E.; Dam-Larsen, S.; Adams, L.A.; Bjornsson, E.S.; Charatcharoenwitthaya, P.; Mills, P.R.; Keach, J.C.; Lafferty, H.D.; Stahler, A.; et al. Liver fibrosis, but no other histologic features, is associated with long-term outcomes of patients with nonalcoholic fatty liver disease. Gastroenterology 2015, 149, 389–397. [Google Scholar] [CrossRef] [Green Version]
- Ballestri, S.; Zona, S.; Targher, G.; Romagnoli, D.; Baldelli, E.; Nascimbeni, F.; Roverato, A.; Guaraldi, G.; Lonardo, A. Nonalcoholic fatty liver disease is associated with an almost two-fold increased risk of incident type 2 diabetes and metabolic syndrome. Evidence from a systematic review and meta-analysis. J. Gastroenterol. Hepatol. 2016, 31, 936–944. [Google Scholar] [CrossRef]
- Targher, G.; Byrne, C.D.; Lonardo, A.; Zoppini, G.; Barbui, C. Non-alcoholic fatty liver disease and risk of incident cardiovascular disease: A meta-analysis. J. Hepatol. 2016, 65, 589–600. [Google Scholar] [CrossRef] [Green Version]
- Hagström, H.; Nasr, P.; Ekstedt, M.; Hammar, U.; Stål, P.; Hultcrantz, R.; Kechagias, S. Fibrosis stage but not NASH predicts mortality and time to development of severe liver disease in biopsy-proven NAFLD. J. Hepatol. 2017, 67, 1265–1273. [Google Scholar] [CrossRef] [PubMed]
- Cai, J.; Zhang, X.J.; Ji, Y.X.; Zhang, P.; She, Z.G.; Li, H. Nonalcoholic Fatty Liver Disease Pandemic Fuels the Upsurge in Cardiovascular Diseases. Circ. Res. 2020, 126, 679–704. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.S.; Taylor, R.J.; Bayliss, S.; Hagström, H.; Nasr, P.; Schattenberg, J.M.; Ishigami, M.; Toyoda, H.; Wai-Sun Wong, V.; Peleg, N.; et al. Association Between Fibrosis Stage and Outcomes of Patients With Nonalcoholic Fatty Liver Disease: A Systematic Review and Meta-Analysis. Gastroenterology 2020, 158, 1611–1625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petta, S.; Valenti, L.; Bugianesi, E.; Targher, G.; Bellentani, S.; Bonino, F.; Special Interest Group on Personalised Hepatology of the Italian Association for the Study of the Liver (AISF); Special Interest Group on Personalised Hepatology of Italian Association for Study of Liver AISF. A “systems medicine” approach to the study of non-alcoholic fatty liver disease. Dig. Liver Dis. 2016, 48, 333–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ballestri, S.; Nascimbeni, F.; Romagnoli, D.; Baldelli, E.; Targher, G.; Lonardo, A. Type 2 Diabetes in Non-Alcoholic Fatty Liver Disease and Hepatitis C Virus Infection—Liver: The “Musketeer” in the Spotlight. Int. J. Mol. Sci. 2016, 17, 355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cotter, T.G.; Rinella, M. Nonalcoholic fatty liver disease 2020: The state of the disease. Gastroenterology 2020, 158, 1851–1864. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL Recommendations on Treatment of Hepatitis C 2018. J. Hepatol. 2018, 69, 461–511. [Google Scholar] [CrossRef] [Green Version]
- European Association for the Study of the Liver. EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J. Hepatol. 2017, 67, 370–398. [Google Scholar] [CrossRef] [Green Version]
- Tapper, E.B.; Lok, A.S. Use of Liver Imaging and Biopsy in Clinical Practice. N. Engl. J. Med. 2017, 377, 756–768. [Google Scholar] [CrossRef]
- Eguchi, Y.; Wong, G.; Akhtar, O.; Sumida, Y. Non-invasive diagnosis of non-alcoholic steatohepatitis and advanced fibrosis in Japan: A targeted literature review. Hepatol. Res. 2020, 50, 645–655. [Google Scholar] [CrossRef]
- Castera, L.; Friedrich-Rust, M.; Loomba, R. Noninvasive assessment of liver disease in patients with nonalcoholic fatty liver disease. Gastroenterology 2019, 156, 1264–1281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hou, W.; Janech, M.G.; Sobolesky, P.M.; Bland, A.M.; Samsuddin, S.; Alazawi, W.; Syn, W.K. Proteomic screening of plasma identifies potential noninvasive biomarkers associated with significant/advanced fibrosis in patients with nonalcoholic fatty liver disease. Biosci. Rep. 2020, 40, BSR20190395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Association for Study of Liver; Asociacion Latinoamericana para el Estudio del Higado. EASL-ALEH Clinical Practice Guidelines: Non-invasive tests for evaluation of liver disease severity and prognosis. J. Hepatol. 2015, 63, 237–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Carli, M.A.; De Carli, L.A.; Correa, M.B.; Junqueira, G., Jr.; Tovo, C.V.; Coral, G.P. Performance of noninvasive scores for the diagnosis of advanced liver fibrosis in morbidly obese with nonalcoholic fatty liver disease. Eur. J. Gastroenterol. Hepatol. 2020, 32, 420–425. [Google Scholar] [CrossRef] [PubMed]
- Nascimbeni, F.; Ballestri, S.; Machado, M.V.; Mantovani, A.; Cortez-Pinto, H.; Targher, G.; Lonardo, A. Clinical relevance of liver histopathology and different histological classifications of NASH in adults. Expert Rev. Gastroenterol. Hepatol. 2018, 12, 351–367. [Google Scholar] [CrossRef]
- Ampuero, J.; Pais, R.; Aller, R.; Gallego-Durán, R.; Crespo, J.; García-Monzón, C.; Boursier, J.; Vilar, E.; Petta, S.; Zheng, M.H.; et al. Development and Validation of Hepamet Fibrosis Scoring System-A Simple, Noninvasive Test to Identify Patients With Nonalcoholic Fatty Liver Disease With Advanced Fibrosis. Clin. Gastroenterol. Hepatol. 2020, 18, 216–225. [Google Scholar] [CrossRef]
- Brunt, E.M.; Janney, C.G.; Di Bisceglie, A.M.; Neuschwander-Tetri, B.A.; Bacon, B.R. Nonalcoholic steatohepatitis: A proposal for grading and staging the histological lesions. Am. J. Gastroenterol. 1999, 94, 2467–2474. [Google Scholar] [CrossRef]
- Kleiner, D.E.; Brunt, E.M.; Van Natta, M.; Behling, C.; Contos, M.J.; Cummings, O.W.; Ferrell, L.D.; Liu, Y.C.; Torbenson, M.S.; Unalp-Arida, A.; et al. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology 2005, 41, 1313–1321. [Google Scholar] [CrossRef]
- Ishak, K.; Baptista, A.; Bianchi, L.; Callea, F.; De Groote, J.; Gudat, F.; Denk, H.; Desmet, V.; Korb, G.; MacSween, R.N.; et al. Histological grading and staging of chronic hepatitis. J. Hepatol. 1995, 22, 696–699. [Google Scholar] [CrossRef]
- Xiao, G.; Zhu, S.; Xiao, X.; Yan, L.; Yang, J.; Wu, G. Comparison of laboratory tests, ultrasound, or magnetic resonance elastography to detect fibrosis in patients with nonalcoholic fatty liver disease: A meta-analysis. Hepatology 2017, 66, 1486–1501. [Google Scholar] [CrossRef]
- Vallet-Pichard, A.; Mallet, V.; Nalpas, B.; Verkarre, V.; Nalpas, A.; Dhalluin-Venier, V.; Fontaine, H.; Pol, S. FIB-4: An inexpensive and accurate marker of fibrosis in HCV infection: Comparison with liver biopsy and fibrotest. Hepatology 2007, 46, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Gordon, S.C.; Rupp, L.B.; Zhang, T.; Boscarino, J.A.; Vijayadeva, V.; Schmidt, M.A.; Lu, M.; Chronic Hepatitis Cohort Study (CHeCS) Investigators. The validity of serum markers for fibrosis staging in chronic hepatitis B and C. J. Viral Hepat. 2014, 21, 930–937. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.W.; Peng, C.Y.; Lai, H.C.; Su, W.P.; Lin, C.H.; Chuang, P.H.; Chen, S.H.; Chen, C.H.; Hsu, W.F.; Huang, G.T. New noninvasive index for predicting liver fibrosis in Asian patients with chronic viral hepatitis. Sci. Rep. 2017, 7, 3259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sebastiani, G.; Castera, L.; Halfon, P.; Pol, S.; Mangia, A.; Di Marco, V.; Pirisi, M.; Voiculescu, M.; Bourliere, M.; Alberti, A. The impact of liver disease aetiology and the stages of hepatic fibrosis on the performance of non-invasive fibrosis biomarkers: An international study of 2411 cases. Aliment. Pharmacol. Ther. 2011, 34, 1202–1216. [Google Scholar] [CrossRef] [PubMed]
- Lin, Z.H.; Xin, Y.N.; Dong, Q.J.; Wang, Q.; Jiang, X.J.; Zhan, S.H.; Sun, Y.; Xuan, S.Y. Performance of the aspartate aminotransferase-to-platelet ratio index for the staging of hepatitis C-related fibrosis: An updated meta-analysis. Hepatology 2011, 53, 726–736. [Google Scholar] [CrossRef]
- Chou, R.; Wasson, N. Blood tests to diagnose fibrosis or cirrhosis in patients with chronic hepatitis C virus infection: A systematic review. Ann. Intern. Med. 2013, 158, 807–820. [Google Scholar] [CrossRef] [Green Version]
- Adler, M.; Gulbis, B.; Moreno, C.; Evrard, S.; Verset, G.; Golstein, P.; Frotscher, B.; Nagy, N.; Thiry, P. The predictive value of FIB-4 versus FibroTest, APRI, FibroIndex and Forns index to noninvasively estimate fibrosis in hepatitis C and nonhepatitis C liver diseases. Hepatology 2008, 47, 762–763. [Google Scholar] [CrossRef]
- Siddiqui, M.S.; Yamada, G.; Vuppalanchi, R.; Van Natta, M.; Loomba, R.; Guy, C.; Brandman, D.; Tonascia, J.; Chalasani, N.; Neuschwander-Tetri, B.; et al. Diagnostic Accuracy of Noninvasive Fibrosis Models to Detect Change in Fibrosis Stage. Clin. Gastroenterol. Hepatol. 2019, 17, 1877–1885. [Google Scholar] [CrossRef]
- Newsome, P.N.; Sasso, M.; Deeks, J.J.; Paredes, A.; Boursier, J.; Chan, W.K.; Yilmaz, Y.; Czernichow, S.; Zheng, M.H.; Wong, V.W.; et al. FibroScan-AST (FAST) score for the non-invasive identification of patients with non-alcoholic steatohepatitis with significant activity and fibrosis: A prospective derivation and global validation study. Lancet Gastroenterol. Hepatol. 2020, 5, 362–373. [Google Scholar] [CrossRef] [Green Version]
- McPherson, S.; Hardy, T.; Dufour, J.F.; Petta, S.; Romero-Gomez, M.; Allison, M.; Oliveira, C.P.; Francque, S.; Van Gaal, L.; Schattenberg, J.M.; et al. Age as a Confounding Factor for the Accurate Non-Invasive Diagnosis of Advanced NAFLD Fibrosis. Am. J. Gastroenterol. 2017, 112, 740–751. [Google Scholar] [CrossRef] [Green Version]
- Ballestri, S.; Nascimbeni, F.; Romagnoli, D.; Lonardo, A. The independent predictors of non-alcoholic steatohepatitis and its individual histological features. Insulin resistance, serum uric acid, metabolic syndrome, alanine aminotransferase and serum total cholesterol are a clue to pathogenesis and candidate targets for treatment. Hepatol. Res. 2016, 46, 1074–1087. [Google Scholar] [CrossRef] [PubMed]
- Carulli, L.; Ballestri, S.; Lonardo, A.; Lami, F.; Violi, E.; Losi, L.; Bonilauri, L.; Verrone, A.M.; Odoardi, M.R.; Scaglioni, F.; et al. Is nonalcoholic steatohepatitis associated with a high-though-normal thyroid stimulating hormone level and lower cholesterol levels? Intern. Emerg. Med. 2013, 8, 297–305. [Google Scholar] [CrossRef] [PubMed]
- Loria, P.; Marchesini, G.; Nascimbeni, F.; Ballestri, S.; Maurantonio, M.; Carubbi, F.; Ratziu, V.; Lonardo, A. Cardiovascular risk, lipidemic phenotype and steatosis. A comparative analysis of cirrhotic and non-cirrhotic liver disease due to varying etiology. Atherosclerosis 2014, 232, 99–109. [Google Scholar] [CrossRef] [PubMed]
- McPherson, S.; Stewart, S.F.; Henderson, E.; Burt, A.D.; Day, C.P. Simple non-invasive fibrosis scoring systems can reliably exclude advanced fibrosis in patients with non-alcoholic fatty liver disease. Gut 2010, 59, 1265–1269. [Google Scholar] [CrossRef] [Green Version]
- Treeprasertsuk, S.; Piyachaturawat, P.; Soontornmanokul, T.; Wisedopas-Klaikaew, N.; Komolmit, P.; Tangkijavanich, P. Accuracy of noninvasive scoring systems to assess advanced liver fibrosis in Thai patients with nonalcoholic fatty liver disease. Asian Biomed. 2017, 10, s49–s55. [Google Scholar] [CrossRef]
- Sterling, R.K.; Lissen, E.; Clumeck, N.; Sola, R.; Correa, M.C.; Montaner, J.; Sulkowski, M.S.; Torriani, F.J.; Dieterich, D.T.; Thomas, D.L.; et al. Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV coinfection. Hepatology 2006, 43, 1317–1325. [Google Scholar] [CrossRef]
- Angulo, P.; Hui, J.M.; Marchesini, G.; Bugianesi, E.; George, J.; Farrell, G.C.; Enders, F.; Saksena, S.; Burt, A.D.; Bida, J.P.; et al. The NAFLD fibrosis score: A noninvasive system that identifies liver fibrosis in patients with NAFLD. Hepatology 2007, 45, 846–854. [Google Scholar] [CrossRef]
- Lonardo, A.; Ballestri, S. Perspectives of nonalcoholic fatty liver disease research: A personal point of view. Explor. Med. 2020, 1, 85–107. [Google Scholar] [CrossRef]
- Redman, J.; Sterling, R.K. Non-invasive Assessment of Liver Fibrosis. Curr. Treat. Options Gastroenterol. 2020, 18, 255–269. [Google Scholar] [CrossRef]
- Ballestri, S.; Nascimbeni, F.; Lugari, S.; Lonardo, A.; Francica, G. A critical appraisal of the use of ultrasound in hepatic steatosis. Expert Rev. Gastroenterol. Hepatol. 2019, 13, 667–681. [Google Scholar] [CrossRef]
- Ballestri, S.; Tana, C.; Di Girolamo, M.; Fontana, M.C.; Capitelli, M.; Lonardo, A.; Cioni, G. Semi-quantitative Ultrasonographic Evaluation of NAFLD. Curr. Pharm. Des. 2020, 26, 3915–3927. [Google Scholar] [CrossRef] [PubMed]
- Lonardo, A.; Nascimbeni, F.; Mantovani, A.; Targher, G. Hypertension, diabetes, atherosclerosis and NASH: Cause or consequence? J. Hepatol. 2018, 68, 335–352. [Google Scholar] [CrossRef] [PubMed]
- Barone, M.; Viggiani, M.T.; Amoruso, A.; Schiraldi, S.; Zito, A.; Devito, F.; Cortese, F.; Gesualdo, M.; Brunetti, N.; Di Leo, A.; et al. Endothelial dysfunction correlates with liver fibrosis in chronic HCV infection. Gastroenterol. Res. Pr. 2015, 2015, 682174. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.K.; Stelzle, D.; Bing, R.; Anwar, M.; Strachan, F.; Bashir, S.; Newby, D.E.; Shah, J.S.; Chung, M.H.; Bloomfield, G.S.; et al. Global burden of atherosclerotic cardiovascular disease in people with hepatitis C virus infection: A systematic review, meta-analysis, and modelling study. Lancet Gastroenterol. Hepatol. 2019, 4, 794–804. [Google Scholar] [CrossRef] [Green Version]
- Adinolfi, L.E.; Petta, S.; Fracanzani, A.L.; Coppola, C.; Narciso, V.; Nevola, R.; Rinaldi, L.; Calvaruso, V.; Staiano, L.; Di Marco, V.; et al. Impact of hepatitis C virus clearance by direct-acting antiviral treatment on the incidence of major cardiovascular events: A prospective multicentre study. Atherosclerosis 2020, 296, 40–47. [Google Scholar] [CrossRef] [Green Version]
- Chen, Q.; Li, Q.; Li, D.; Chen, X.; Liu, Z.; Hu, G.; Wang, J.; Ling, W. Association between liver fibrosis scores and the risk of mortality among patients with coronary artery disease. Atherosclerosis 2020, 299, 45–52. [Google Scholar] [CrossRef]
- Lee, J.; Kim, H.S.; Cho, Y.K.; Kim, E.H.; Lee, M.J.; Bae, I.Y.; Jung, C.H.; Park, J.-Y.; Kim, H.-K.; Lee, W.J. Association between noninvasive assessment of liver fibrosis and coronary artery calcification progression in patients with nonalcoholic fatty liver disease. Sci. Rep. 2020, 10, 18323. [Google Scholar] [CrossRef]
- Schonmann, Y.; Yeshua, H.; Bentov, I.; Zelber-Sagi, S. Liver fibrosis marker is an independent predictor of cardiovascular morbidity and mortality in the general population. Dig. Liver Dis. 2021, 53, 79–85. [Google Scholar] [CrossRef]
- Tsochatzis, E.A.; Srivastava, A.; Rosenberg, W. Reply to: “FIB-4 cut off of 1.3 may be inappropriate in a primary care referral pathway for patients with non-alcoholic fatty liver disease”. J. Hepatol. 2020, 73, 217–218. [Google Scholar] [CrossRef]
- Salomone, F.; Micek, A.; Godos, J. Simple Scores of Fibrosis and Mortality in Patients with NAFLD: A Systematic Review with Meta-Analysis. J. Clin. Med. 2018, 7, 219. [Google Scholar] [CrossRef] [Green Version]
- Simon, T.G.; Corey, K.E.; Cannon, C.P.; Blazing, M.; Park, J.G.; O’Donoghue, M.L.; Chung, R.T.; Giugliano, R.P. The nonalcoholic fatty liver disease (NAFLD) fibrosis score, cardiovascular risk stratification and a strategy for secondary prevention with ezetimibe. Int. J. Cardiol. 2018, 270, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Hagström, H.; Nasr, P.; Ekstedt, M.; Stål, P.; Hultcrantz, R.; Kechagias, S. Accuracy of Noninvasive Scoring Systems in Assessing Risk of Death and Liver-Related Endpoints in Patients With Nonalcoholic Fatty Liver Disease. Clin. Gastroenterol. Hepatol. 2019, 17, 1148–1156.e4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baratta, F.; Pastori, D.; Angelico, F.; Balla, A.; Paganini, A.M.; Cocomello, N.; Ferro, D.; Violi, F.; Sanyal, A.J.; Del Ben, M. Nonalcoholic Fatty Liver Disease and Fibrosis Associated With Increased Risk of Cardiovascular Events in a Prospective Study. Clin. Gastroenterol. Hepatol. 2020, 18, 2324–2331.e4. [Google Scholar] [CrossRef] [PubMed]
- Henson, J.B.; Simon, T.G.; Kaplan, A.; Osganian, S.; Masia, R.; Corey, K.E. Advanced fibrosis is associated with incident cardiovascular disease in patients with non-alcoholic fatty liver disease. Aliment. Pharmacol. Ther. 2020, 51, 728–736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spinosa, M.; Stine, J.G. Nonalcoholic Fatty Liver Disease-Evidence for a Thrombophilic State? Curr. Pharm. Des. 2020, 26, 1036–1044. [Google Scholar] [CrossRef]
- Ballestri, S.; Capitelli, M.; Fontana, M.C.; Arioli, D.; Romagnoli, E.; Graziosi, C.; Lonardo, A.; Marietta, M.; Dentali, F.; Cioni, G. Direct Oral Anticoagulants in Patients with Liver Disease in the Era of Non-Alcoholic Fatty Liver Disease Global Epidemic: A Narrative Review. Adv. Ther. 2020, 37, 1910–1932. [Google Scholar] [CrossRef] [Green Version]
- Dogan, S.; Celikbilek, M.; Yilmaz, Y.K.; Sarikaya, S.; Zararsiz, G.; Serin, H.I.; Borekci, E.; Akyol, L.; Pirti, I.; Davarci, S.E. Association between liver fibrosis and coronary heart disease risk in patients with nonalcoholic fatty liver disease. Eur. J. Gastroenterol. Hepatol. 2015, 27, 298–304. [Google Scholar] [CrossRef]
- Niederseer, D.; Wernly, S.; Bachmayer, S.; Wernly, B.; Bakula, A.; Huber-Schönauer, U.; Semmler, G.; Schmied, C.; Aigner, E.; Datz, C. Diagnosis of Non-Alcoholic Fatty Liver Disease (NAFLD) Is Independently Associated with Cardiovascular Risk in a Large Austrian Screening Cohort. J. Clin. Med. 2020, 9, 1065. [Google Scholar] [CrossRef] [Green Version]
- Pisetta, C.; Chillè, C.; Pelizzari, G.; Pigozzi, M.G.; Salvetti, M.; Paini, A.; Muiesan, M.L.; De Ciuceis, C.; Ricci, C.; Rizzoni, D. Evaluation of Cardiovascular Risk in Patient with Primary Non-alcoholic Fatty Liver Disease. High Blood Press. Cardiovasc. Prev. 2020, 27, 321–330. [Google Scholar] [CrossRef]
- Lonardo, A.; Ballestri, S.; Targher, G.; Loria, P. Diagnosis and management of cardiovascular risk in nonalcoholic fatty liver disease. Expert Rev. Gastroenterol. Hepatol. 2015, 9, 629–650. [Google Scholar] [CrossRef]
- Lonardo, A.; Nascimbeni, F.; Ballestri, S. NAFLD, Hepatotropic Viruses, and Cardiometabolic Risk. Hepatology 2017, 65, 2122–2123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.C.; Cheng, P.N.; Kao, J.H. Systematic review: Chronic viral hepatitis and metabolic derangement. Aliment. Pharmacol. Ther. 2020, 51, 216–230. [Google Scholar] [CrossRef] [PubMed]
- Poynard, T.; Peta, V.; Deckmyn, O.; Pais, R.; Ngo, Y.; Charlotte, F.; Ngo, A.; Munteanu, M.; Imbert-Bismut, F.; Monneret, D.; et al. Performance of liver biomarkers, in patients at risk of nonalcoholic steato-hepatitis, according to presence of type-2 diabetes. Eur. J. Gastroenterol. Hepatol. 2020, 32, 998–1007. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Gosai, F.; Siddiqui, M.T.; Gupta, M.; Lopez, R.; Lawitz, E.; Poordad, F.; Carey, W.; McCullough, A.; Alkhouri, N. Accuracy of Noninvasive Fibrosis Scores to Detect Advanced Fibrosis in Patients With Type-2 Diabetes With Biopsy-proven Nonalcoholic Fatty Liver Disease. Clin. Gastroenterol. 2020, 54, 891–897. [Google Scholar] [CrossRef] [PubMed]
- Lemoine, M.; Nayagam, S.; Thursz, M. Viral hepatitis in resource-limited countries and access to antiviral therapies: Current and future challenges. Future Virol. 2013, 8, 371–380. [Google Scholar] [CrossRef] [Green Version]
- Gayam, V.; Gill, A.; Garlapati, P.; Mohanty, S. Direct-Acting Antivirals in Chronic Hepatitis C Infection with Liver Cirrhosis, Hepatitis B and C. IntechOpen 2019, 6, 83–98. [Google Scholar] [CrossRef] [Green Version]
- Edwards, D.J.; Coppens, D.G.; Prasad, T.L.; Rook, L.A.; Iyer, J.K. Access to hepatitis C medicines. Bull. World Health Organ. 2015, 93, 799–805. [Google Scholar] [CrossRef]
- Kondili, L.A.; Gaeta, G.B.; Brunetto, M.R.; Di Leo, A.; Iannone, A.; Santantonio, T.A.; Giammario, A.; Raimondo, G.; Filomia, R.; Coppola, C.; et al. Incidence of DAA failure and the clinical impact of retreatment in real-life patients treated in the advanced stage of liver disease: Interim evaluations from the PITER network. PLoS ONE 2017, 12, e0185728. [Google Scholar] [CrossRef] [Green Version]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2004, 27, S5–S10. [Google Scholar] [CrossRef] [Green Version]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [PubMed]
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.; Loria, C.M.; Smith, S.C., Jr.; et al. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conroy, R.M.; Pyörälä, K.; Fitzgerald, A.P.; Sans, S.; Menotti, A.; De Backer, G.; De Bacquer, D.; Ducimetière, P.; Jousilahti, P.; Keil, U.; et al. Estimation of ten-year risk of fatal cardiovascular disease in Europe: The SCORE project. Eur. Heart J. 2003, 24, 987–1003. [Google Scholar] [CrossRef]
- Palmieri, L.; Panico, S.; Vanuzzo, D.; Ferrario, M.; Pilotto, L.; Sega, R.; Cesana, G.; Giampaoli, S.; Gruppo di Ricerca del Progetto CUORE. Evaluation of the global cardiovascular absolute risk: The Progetto CUORE individual score. Ann. Ist. Super. Sanita 2004, 40, 393–399. [Google Scholar] [PubMed]
- D’Agostino, R.B.; Vasan, R.S.; Pencina, M.J.; Wolf, P.A.; Cobain, M.; Massaro, J.M.; Kannel, W.B. General cardiovascular risk profile for use in primary care. Circulation 2008, 117, 743–753. [Google Scholar] [CrossRef] [Green Version]
- Eichler, K.; Puhan, M.A.; Steurer, J.; Bachmann, L.M. Prediction of first coronary events with the Framingham score: A systematic review. Am. Heart J. 2007, 153, 722–731.e7318. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver (EASL); European Association for the Study of Diabetes (EASD); European Association for the Study of Obesity (EASO). EASL-EASD-EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. J. Hepatol. 2016, 64, 1388–1402. [Google Scholar] [CrossRef]
- Gupta, E.; Bajpai, M.; Choudhary, A. Hepatitis C virus: Screening, diagnosis, and interpretation of laboratory assays. Asian J. Transfus. Sci. 2014, 8, 19–25. [Google Scholar] [CrossRef]
- Krajden, M.; McNabb, G.; Petric, M. The laboratory diagnosis of hepatitis B virus. Can. J. Infect. Dis. Med. Microbiol. 2005, 16, 65–72. [Google Scholar] [CrossRef] [Green Version]
- Williams, A.L.; Hoofnagle, J.H. Ratio of serum aspartate to alanine aminotransferase in chronic hepatitis. Relationship to cirrhosis. Gastroenterology 1988, 95, 734–739. [Google Scholar] [CrossRef]
- Wai, C.T.; Greenson, J.K.; Fontana, R.J.; Kalbfleisch, J.D.; Marrero, J.A.; Conjeevaram, H.S.; Lok, A.S. A simple noninvasive index can predict both significant fibrosis and cirrhosis in patients with chronic hepatitis C. Hepatology 2003, 38, 518–526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forns, X.; Ampurdanès, S.; Llovet, J.M.; Aponte, J.; Quintó, L.; Martínez-Bauer, E.; Bruguera, M.; Sánchez-Tapias, J.M.; Rodés, J. Identification of chronic hepatitis C patients without hepatic fibrosis by a simple predictive model. Hepatology 2002, 36, 986–992. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrison, S.A.; Oliver, D.; Arnold, H.L.; Gogia, S.; Neuschwander-Tetri, B.A. Development and validation of a simple NAFLD clinical scoring system for identifying patients without advanced disease. Gut 2008, 57, 1441–1447. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| All (n = 280) | Viral CLD * (n = 173) | NAFLD (n = 107) | p† | |
|---|---|---|---|---|
| Biometrics | ||||
| Age (years) | 47.6 ± 11.5 | 47.7 ± 11.3 | 47.6 ± 11.9 | 0.983 |
| Male/Female ratio (n, %) | 185/95 (66/34) | 108/65 (62/38) | 77/30 (72/28) | 0.119 |
| BMI (kg/m2) | 27.5 ± 4.5 | 26.0 ± 3.9 | 29.5 ± 4.5 | <0.001 |
| Waist Circumference (cm) | 97.1 ± 12.3 | 91.0 ± 9.9 | 101.8 ± 11.9 | <0.001 |
| Hypertension (n, %) | 82 (29) | 44 (26) | 38 (36) | 0.081 |
| Type 2 diabetes (n, %) | 46 (16) | 13 (8) | 33 (31) | <0.001 |
| Metabolic syndrome (n, %) | 77 (28) | 21 (12) | 56 (52) | <0.001 |
| CVR scores | ||||
| SCORE | 0.5 (0.1 ÷ 1.4) | 0.4 (0.1 ÷ 1.4) | 0.7 (0.2 ÷ 1.7) | 0.052 |
| FRS | 7.3 (3.6 ÷ 14.8) | 6.7 (3.6 ÷ 13.4) | 8.7 (4.0 ÷ 19.9) | 0.026 |
| Progetto CUORE | 1.9 (0.8 ÷ 4.8) | 1.5 (0.6 ÷ 4.1) | 2.5 (1.1 ÷ 6.0) | 0.002 |
| Laboratory | ||||
| Platelet count (×103/mm3) | 212.6 ± 61.4 | 206.2 ± 61.3 | 223.0 ± 60.2 | 0.025 |
| Fasting glucose (mg/dL) | 95.0 (87.0 ÷ 103.0) | 93.5 (85.0 ÷ 100.0) | 98.0 (91.0 ÷ 116.0) | <0.001 |
| Fasting insulin (mIU/L) | 10.7 (7.2 ÷ 15.8) | 9.6 (7.1 ÷ 15.7) | 11.5 (8.0 ÷ 15.9) | 0.244 |
| HOMA-IR score | 2.6 (1.6 ÷ 4.0) | 2.4 (1.5 ÷ 3.8) | 2.9 (1.9 ÷ 4.3) | 0.148 |
| AST (U/L) | 39.7 (28.0 ÷ 58.9) | 43.0 (32.0 ÷ 69.7) | 33.0 (26.0 ÷ 49.0) | <0.001 |
| ALT (U/L) | 41.5 (64.5 ÷ 119.7) | 71.0 (44.0 ÷ 130.2) | 58.0 (40.0 ÷ 91.0) | 0.019 |
| GGT (U/L) | 41.0 (27.4 ÷ 76.8) | 40.0 (24.0 ÷ 62.1) | 49.0 (33.0 ÷ 109.0) | 0.003 |
| Albumin (g/dL) | 4.4 ± 0.5 | 4.4 ± 0.4 | 4.5 ± 0.5 | 0.052 |
| γ-globulin (mg/dL) | 1.3 ± 0.4 | 1.4 ± 0.4 | 1.1 ± 0.3 | <0.001 |
| Total Cholesterol (mg/dL) | 186.7 ± 44.8 | 171.8 ± 37.6 | 210.8 ± 45.1 | <0.001 |
| HDL-Cholesterol (mg/dL) | 46.4 ± 13.9 | 48.3 ± 14.2 | 44.4 ± 13.5 | 0.049 |
| LDL-Cholesterol (mg/dL) | 118.9 ± 39.5 | 102.3 ± 32.5 | 135.2 ± 39.1 | <0.001 |
| Triglycerides (mg/dL) | 69.0 (97.0 ÷ 147.0) | 82.0 (62.0 ÷ 113.0) | 146.0 (92.0 ÷ 228.0) | <0.001 |
| Serum uric acid (mg/dL) | 5.3 ± 1.4 | 4.8 ± 1.2 | 6.0 ± 1.5 | <0.001 |
| Ferritin (mg/dL) | 150.0 (79.0 ÷ 252.5) | 134.0(64.0 ÷ 252.5) | 178.0 (98.5 ÷ 258.3) | 0.036 |
| Liver histology | ||||
| Steatosis ≥ 5% (n, %) | 184 (66) | 75 (43) | 107 (100) | <0.001 |
| Significant fibrosis (n, %) | 100 (36) | 55 (32) | 45 (42) | 0.095 |
| Advanced fibrosis (n, %) | 38 (14) | 24 (14) | 14 (13) | 1.000 |
| Cirrhosis (n, %) | 10 (4) | 5 (3) | 5 (5) | 0.513 |
| Liver fibrosis biomarkers | ||||
| AAR | 0.62 (0.49 ÷ 0.73) | 0.64 (0.52 ÷ 0.74) | 0.56 (0.46 ÷ 0.69) | 0.002 |
| APRI | 0.57 (0.35 ÷ 0.88) | 0.64 (0.40 ÷ 1.08) | 0.43 (0.30 ÷ 0.69) | <0.001 |
| FIB-4 | 1.05 (0.72 ÷ 1.65) | 1.21 (0.82 ÷ 1.92) | 0.84 (0.63 ÷ 1.29) | <0.001 |
| Forns | 4.9 ± 1.8 | 5.1 ± 1.8 | 4.5 ± 1.8 | 0.019 |
| Cut-Offs | SE | SP | PPV | NPV | ACC | LR+ | LR− | AUROC (95% CI) | |
|---|---|---|---|---|---|---|---|---|---|
| AAR | ≥0.8 | 26.3 | 84.3 | 20.8 | 87.9 | 76.4 | 1.68 | 0.87 | 0.60 (0.51–0.70) |
| >1 | 13.2 | 93.8 | 25.0 | 87.3 | 82.9 | 2.12 | 0.93 | ||
| APRI | >0.5 | 94.7 | 49.2 | 22.6 | 98.4 | 55.4 | 1.86 | 0.11 | 0.84 (0.78–0.90) |
| >1 | 63.2 | 87.2 | 43.6 | 93.8 | 83.9 | 4.93 | 0.42 | ||
| >1.5 | 36.8 | 93.8 | 48.3 | 90.4 | 86.1 | 5.94 | 0.67 | ||
| FIB-4 | ≥1.45 | 81.6 | 74.4 | 33.3 | 96.3 | 75.4 | 3.18 | 0.25 | 0.88 (0.83–0.93) |
| >3.25 | 36.8 | 96.7 | 63.6 | 90.7 | 88.6 | 11.15 | 0.65 | ||
| Forns | ≥4.2 | 97.4 | 43.8 | 21.4 | 99.1 | 51.1 | 1.73 | 0.06 | 0.90 (0.84–0.95) |
| >6.9 | 40.6 | 95.7 | 75.7 | 83.1 | 82.1 | 9.51 | 0.62 |
| Cut-Offs | SE | SP | PPV | NPV | ACC | LR+ | LR− | AUROC (95% CI) | |
|---|---|---|---|---|---|---|---|---|---|
| AAR | ≥0.8 | 20.8 | 81.9 | 15.6 | 86.5 | 73.4 | 1.15 | 0.97 | 0.56 (0.44–0.68) |
| >1 | 8.3 | 92.6 | 15.4 | 86.3 | 80.9 | 1.13 | 0.99 | ||
| APRI | >0.5 | 95.8 | 38.9 | 20.2 | 98.3 | 46.8 | 1.57 | 0.11 | 0.84 (0.76–0.92) |
| >1 | 79.2 | 82.6 | 42.2 | 96.1 | 82.1 | 4.54 | 0.25 | ||
| >1.5 | 50.0 | 90.6 | 46.2 | 91.8 | 85.0 | 5.32 | 0.55 | ||
| FIB-4 | ≥1.45 | 87.5 | 67.1 | 30.0 | 97.1 | 69.9 | 2.66 | 0.19 | 0.88 (0.82–0.95) |
| >3.25 | 37.5 | 96.0 | 60.0 | 90.5 | 87.9 | 9.31 | 0.65 | ||
| Forns | ≥4.2 | 95.8 | 36.9 | 19.7 | 98.2 | 45.1 | 1.52 | 0.11 | 0.89 (0.82–0.97) |
| >6.9 | 66.7 | 92.6 | 59.3 | 94.5 | 89.0 | 9.03 | 0.36 |
| Cut-Offs | SE | SP | PPV | NPV | ACC | LR+ | LR− | AUROC (95% CI) | |
|---|---|---|---|---|---|---|---|---|---|
| AAR | ≥0.8 | 35.7 | 88.2 | 31.3 | 90.1 | 81.3 | 3.02 | 0.73 | 0.66 (0.50–0.82) |
| >1 | 21.4 | 95.7 | 42.9 | 89.0 | 86.0 | 4.98 | 0.82 | ||
| APRI | >0.5 | 92.9 | 65.6 | 28.9 | 98.4 | 69.2 | 2.70 | 0.11 | 0.87 (0.79–0.95) |
| >1 | 35.7 | 94.6 | 50.0 | 90.7 | 86.9 | 6.64 | 0.68 | ||
| >1.5 | 14.3 | 98.9 | 66.7 | 88.5 | 87.9 | 13.29 | 0.87 | ||
| Fib-4 | ≥1.3 | 78.6 | 83.9 | 42.3 | 96.3 | 83.2 | 4.87 | 0.26 | 0.91 (0.84–0.97) |
| ≥1.45 | 71.4 | 86.0 | 43.5 | 95.2 | 84.1 | 5.11 | 0.33 | ||
| >2.67 | 35.7 | 96.8 | 62.5 | 90.9 | 88.8 | 11.07 | 0.66 | ||
| >3.25 | 35.7 | 97.9 | 71.4 | 91.0 | 89.7 | 16.61 | 0.66 | ||
| Forns | ≥4.2 | 100.0 | 54.8 | 25.0 | 100.0 | 60.8 | 2.21 | 0.00 | 0.92 (0.85–0.99) |
| >6.9 | 42.9 | 95.7 | 60.0 | 91.8 | 88.8 | 9.96 | 0.60 | ||
| NFS | ≥−1.455 | 85.7 | 64.5 | 26.7 | 96.8 | 67.3 | 2.42 | 0.22 | 0.89 (0.81–0.97) |
| >0.675 | 42.9 | 96.8 | 66.7 | 91.8 | 89.7 | 13.29 | 0.59 | ||
| BARD | ≥2 | 78.6 | 75.3 | 32.4 | 95.9 | 75.7 | 3.18 | 0.29 | 0.79 (0.66–0.93) |
| HFS | ≥0.12 | 78.6 | 89.3 | 52.4 | 96.5 | 87.9 | 7.31 | 0.24 | 0.94 (0.90–0.99) |
| >0.47 | 50.0 | 96.8 | 70.0 | 92.8 | 90.7 | 15.5 | 0.52 |
| All | Viral CLD | NAFLD | |||||
|---|---|---|---|---|---|---|---|
| Cut-Offs | Patients, n (%) | FN, n (%) | Patients, n (%) | FN, n (%) | Patients, n (%) | FN, n (%) | |
| AAR | <0.8 | 232/280 (83) | 28 (12) | 141/173 (82) | 19 (14) | 91/107 (85) | 9 (10) |
| ≤1 | 260/280 (93) | 33 (13) | 160/173 (93) | 22 (14) | 100/107 (94) | 11 (11) | |
| APRI | <0.5 | 121/280 (52) | 2 (2) | 59/173 (34) | 1 (2) | 62/107 (58) | 1 (2) |
| <0.7 | 177/280 (63) | 8 (5) | 93/173 (54) | 3 (3) | 84/107 (79) | 5 (6) | |
| <1 | 225/280 (80) | 14 (6) | 128/173 (74) | 5 (4) | 97/107 (91) | 9 (9) | |
| FIB-4 | <1.3 | 173/280 (62) | 6 (4) | 92/173 (53) | 3 (3) | 81/107 (76) | 3 (4) |
| <1.45 | 187/280 (67) | 7 (4) | 103/173 (60) | 3 (3) | 84/107 (79) | 4 (5) | |
| Forns | <4.2 | 107/280 (38) | 1 (1) | 56/173 (32) | 1 (2) | 51/107 (48) | 0 (0) |
| NFS | <−1.455 | _ | _ | _ | _ | 62/107 (58) | 2 (3) |
| BARD | <2 | _ | _ | _ | _ | 73/107 (68) | 3 (4) |
| HFS | <0.12 | _ | _ | _ | _ | 86/107 (80) | 3 (4) |
| SCORE | Progetto CUORE | FRS | |||||||
|---|---|---|---|---|---|---|---|---|---|
| All | Viral CLD | NAFLD | All | Viral CLD | NAFLD | All | Viral CLD | NAFLD | |
| AAR | 0.302 * | 0.261 † | 0.406 * | 0.302 * | 0.340 * | 0.325 † | 0.252 * | 0.166 § | 0.401 * |
| APRI | 0.208 * | 0.234 † | 0.260 * | 0.145 § | 0.156 | 0.375 * | 0.114 | 0.124 | 0.407 * |
| FIB-4 | 0.462 * | 0.476 * | 0.499 * | 0.402 * | 0.399 * | 0.560 * | 0.342 * | 0.319 * | 0.584 * |
| Forns | 0.468 * | 0.454 * | 0.544 * | 0.437 * | 0.370 * | 0.568 * | 0.445 * | 0.453 * | 0.532 * |
| NFS | _ | _ | 0.593 * | _ | _ | 0.658 * | _ | _ | 0.702 * |
| BARD | _ | _ | 0.449 * | _ | _ | 0.471 * | _ | _ | 0.540 * |
| HFS | _ | _ | 0.509 * | _ | _ | 0.643 * | _ | _ | 0.679 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ballestri, S.; Mantovani, A.; Baldelli, E.; Lugari, S.; Maurantonio, M.; Nascimbeni, F.; Marrazzo, A.; Romagnoli, D.; Targher, G.; Lonardo, A. Liver Fibrosis Biomarkers Accurately Exclude Advanced Fibrosis and Are Associated with Higher Cardiovascular Risk Scores in Patients with NAFLD or Viral Chronic Liver Disease. Diagnostics 2021, 11, 98. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11010098
Ballestri S, Mantovani A, Baldelli E, Lugari S, Maurantonio M, Nascimbeni F, Marrazzo A, Romagnoli D, Targher G, Lonardo A. Liver Fibrosis Biomarkers Accurately Exclude Advanced Fibrosis and Are Associated with Higher Cardiovascular Risk Scores in Patients with NAFLD or Viral Chronic Liver Disease. Diagnostics. 2021; 11(1):98. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11010098
Chicago/Turabian StyleBallestri, Stefano, Alessandro Mantovani, Enrica Baldelli, Simonetta Lugari, Mauro Maurantonio, Fabio Nascimbeni, Alessandra Marrazzo, Dante Romagnoli, Giovanni Targher, and Amedeo Lonardo. 2021. "Liver Fibrosis Biomarkers Accurately Exclude Advanced Fibrosis and Are Associated with Higher Cardiovascular Risk Scores in Patients with NAFLD or Viral Chronic Liver Disease" Diagnostics 11, no. 1: 98. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11010098