Soluble ST2 as a Biomarker for Early Complications in Patients with Chronic Thromboembolic Pulmonary Hypertension Treated with Balloon Pulmonary Angioplasty

 , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Baseline Tests and Measurements
2.3. Balloon Pulmonary Angioplasty, Periprocedural Period and Complications
2.4. sST2 Measurements
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Delcroix, M.; Noordegraaf, A.V.; Fadel, E.; Lang, I.; Simonneau, G.; Naeije, R. Vascular and right ventricular remodelling in chronic thromboembolic pulmonary hypertension. Eur. Respir. J. 2012, 41, 224–232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simonneau, G.; Torbicki, A.; Dorfmüller, P.; Kim, N. The pathophysiology of chronic thromboembolic pulmonary hypertension. Eur. Respir. Rev. 2017, 26, 160112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galie, N.; Humbert, M.; Vachiery, J.L.; Gibbs, S.; Lang, I.; Torbicki, A.; Simonneau, G.; Peacock, A.; Vonk Noordegraaf, A.; Beghetti, M.; et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur. Respir. J. 2015, 46, 903–975. [Google Scholar] [PubMed]
- Kim, N.H.; Delcroix, M.; Jais, X.; Madani, M.M.; Matsubara, H.; Mayer, E.; Ogo, T.; Tapson, V.; Ghofrani, H.A.; Jenkins, D. Chronic thromboembolic pulmonary hypertension. Eur. Respir. J. 2018, 53, 1801915. [Google Scholar] [CrossRef]
- Dieplinger, B.; Januzzi, J.L.; Steinmair, M.; Gabriel, C.; Poelz, W.; Haltmayer, M.; Mueller, T. Analytical and clinical evaluation of a novel high-sensitivity assay for measurement of soluble ST2 in human plasma—The Presage™ ST2 assay. Clin. Chim. Acta 2009, 409, 33–40. [Google Scholar] [CrossRef]
- Dieplinger, B.; Mueller, T. Soluble ST2 in heart failure. Clin. Chim. Acta 2015, 443, 57–70. [Google Scholar] [CrossRef]
- Coglianese, E.E.; Larson, M.G.; Vasan, R.S.; Ho, J.E.; Ghorbani, A.; McCabe, E.L.; Cheng, S.; Fradley, M.G.; Kretschman, D.; Gao, W.; et al. Distribution and Clinical Correlates of the Interleukin Receptor Family Member Soluble ST2 in the Framingham Heart Study. Clin. Chem. 2012, 58, 1673–1681. [Google Scholar] [CrossRef]
- Luk, K.S.; Ip, C.; Gong, M.; Wong, S.H.; Wu, W.K.; Dong, M.; Li, G.; Chan, K.P.; Du, Y.; Liu, T.; et al. A meta-analysis of soluble suppression of tumorigenicity 2 (sST2) and clinical outcomes in pulmonary hypertension. J. Geriatr. Cardiol. 2017, 14, 766–771. [Google Scholar]
- Mueller, T.; Dieplinger, B. The Presage((R)) ST2 Assay: Analytical considerations and clinical applications for a high-sensitivity assay for measurement of soluble ST2. Expert Rev. Mol. Diagn. 2013, 13, 13–30. [Google Scholar] [CrossRef]
- Weinberg, E.O.; Shimpo, M.; De Keulenaer, G.W.; MacGillivray, C.; Tominaga, S.-I.; Solomon, S.D.; Rouleau, J.-L.; Lee, R.T. Expression and regulation of ST2, an interleukin-1 receptor family member, in cardiomyocytes and myocardial infarction. Circulation 2002, 106, 2961–2966. [Google Scholar] [CrossRef] [Green Version]
- Pei, C.; Barbour, M.; Fairlie-Clarke, K.J.; Allan, D.; Mu, R.; Jiang, H.-R. Emerging role of interleukin-33 in autoimmune diseases. Immunology 2013, 141, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Ky, B.; French, B.; McCloskey, K.; Rame, J.E.; McIntosh, E.; Shahi, P.; Dries, D.L.; Tang, W.W.; Wu, A.H.; Fang, J.C.; et al. High-Sensitivity ST2 for Prediction of Adverse Outcomes in Chronic Heart Failure. Circ. Hear. Fail. 2011, 4, 180–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pascual-Figal, D.A.; Manzano-Fernández, S.; Boronat, M.; Casas, T.; Garrido, I.P.; Bonaque, J.C.; Pastor-Perez, F.; Valdés, M.; Januzzi, J.L. Soluble ST2, high-sensitivity troponin T- and N-terminal pro-B-type natriuretic peptide: Complementary role for risk stratification in acutely decompensated heart failure. Eur. J. Hear. Fail. 2011, 13, 718–725. [Google Scholar] [CrossRef] [PubMed]
- Carlomagno, G.; Messalli, G.; Melillo, R.M.; Stanziola, A.A.; Visciano, C.; Mercurio, V.; Imbriaco, M.; Ghio, S.; Sofia, M.; Bonaduce, D.; et al. Serum soluble ST2 and interleukin-33 levels in patients with pulmonary arterial hypertension. Int. J. Cardiol. 2013, 168, 1545–1547. [Google Scholar] [CrossRef]
- Daniels, L.B.; Clopton, P.; Iqbal, N.; Tran, K.; Maisel, A.S. Association of ST2 levels with cardiac structure and function and mortality in outpatients. Am. Hear. J. 2010, 160, 721–728. [Google Scholar] [CrossRef]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E., Jr.; Colvin, M.M.; Drazner, M.H.; Filippatos, G.S.; Fonarow, G.C.; Givertz, M.M.; et al. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. Circulation 2017, 136, e137–e161. [Google Scholar] [CrossRef]
- Geenen, L.W.; Baggen, V.J.M.; Kauling, R.M.; Koudstaal, T.; Boomars, K.A.; Boersma, E.; Roos-Hesselink, J.W.; Bosch, A.E.V.D. The Prognostic Value of Soluble ST2 in Adults with Pulmonary Hypertension. J. Clin. Med. 2019, 8, 1517. [Google Scholar] [CrossRef] [Green Version]
- Zheng, Y.-G.; Yang, T.; He, J.-G.; Chen, G.; Liu, P.; Xiong, C.; Gu, Q.; Ni, X.; Zhao, Z.-H. Plasma Soluble ST2 Levels Correlate with Disease Severity and Predict Clinical Worsening in Patients With Pulmonary Arterial Hypertension. Clin. Cardiol. 2014, 37, 365–370. [Google Scholar] [CrossRef]
- Kurzyna, M.; Araszkiewicz, A.; Błaszczak, P.; Grabka, M.; Hawranek, M.; Kopeć, G.; Mroczek, E.; Zembala, M.; Kamiński, K.A.; Ochała, A. Summary of recommendations for the haemodynamic and angiographic assessment of the pulmonary circulation. Joint statement of the Polish Cardiac Society’s Working Group on Pulmonary Circulation and Association of Cardiovascular Interventions. Kardiol. Pol. 2015, 73, 63–68. [Google Scholar] [CrossRef] [Green Version]
- Araszkiewicz, A.; DaRocha, S.; Pietrasik, A.; Pietura, R.; Jankiewicz, S.; Banaszkiewicz, M.; Sławek-Szmyt, S.; Biederman, A.; Mularek-Kubzdela, T.; Lesiak, M.; et al. Balloon pulmonary angioplasty for the treatment of residual or recurrent pulmonary hypertension after pulmonary endarterectomy. Int. J. Cardiol. 2019, 278, 232–237. [Google Scholar] [CrossRef]
- DaRocha, S.; Kurzyna, M.; Pietura, R.; Kamiński, K.A. Balloon pulmonary angioplasty for inoperable chronic thromboembolic pulmonary hypertension. Kardiol. Pol. 2013, 71, 1331. [Google Scholar] [CrossRef] [PubMed]
- DaRocha, S.; Pietura, R.; Pietrasik, A.; Norwa, J.; Dobosiewicz, A.; Piłka, M.; Florczyk, M.; Biederman, A.; Kamiński, K.A.; Kurzyna, M. Improvement in Quality of Life and Hemodynamics in Chronic Thromboembolic Pulmonary Hypertension Treated with Balloon Pulmonary Angioplasty. Circ. J. 2017, 81, 552–557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurzyna, M.; DaRocha, S.; Pietura, R.; Pietrasik, A.; Norwa, J.; Mańczak, R.; Wieteska, M.; Biederman, A.; Matsubara, H.; Torbicki, A. Changing the strategy of balloon pulmonary angioplasty resulted in a reduced complication rate in patients with chronic thromboembolic pulmonary hypertension. A single-centre European experience. Kardiol. Pol. 2017, 75, 645–654. [Google Scholar] [CrossRef] [PubMed]
- Inami, T.; Kataoka, M.; Shimura, N.; Ishiguro, H.; Yanagisawa, R.; Taguchi, H.; Fukuda, K.; Yoshino, H.; Satoh, T. Pulmonary Edema Predictive Scoring Index (PEPSI), a New Index to Predict Risk of Reperfusion Pulmonary Edema and Improvement of Hemodynamics in Percutaneous Transluminal Pulmonary Angioplasty. JACC Cardiovasc. Interv. 2013, 6, 725–736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robin, X.A.; Turck, N.; Hainard, A.; Tiberti, N.; Lisacek, F.; Sanchez, J.-C.; Müller, M. pROC: An open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinf. 2011, 12, 77. [Google Scholar] [CrossRef]
- Pascual-Figal, D.A.; Januzzi, J.L. The Biology of ST2: The International ST2 Consensus Panel. Am. J. Cardiol. 2015, 115, 3B–7B. [Google Scholar] [CrossRef]
- Lu, J.; Snider, J.V.; Grenache, D.G. Establishment of reference intervals for soluble ST2 from a United States population. Clin. Chim. Acta 2010, 411, 1825–1826. [Google Scholar] [CrossRef]
- Kohli, P.; Bonaca, M.P.; Kakkar, R.; Kudinova, A.Y.; Scirica, B.M.; Sabatine, M.S.; Murphy, S.A.; Braunwald, E.; Lee, R.T.; Morrow, D.A. Role of ST2 in Non–ST-Elevation Acute Coronary Syndrome in the MERLIN-TIMI 36 Trial. Clin. Chem. 2012, 58, 257–266. [Google Scholar] [CrossRef] [Green Version]
- Lassus, J.; Gayat, E.; Mueller, C.; Peacock, W.; Spinar, J.; Harjola, V.-P.; Van Kimmenade, R.; Pathak, A.; Mueller, T.; DiSomma, S.; et al. Incremental value of biomarkers to clinical variables for mortality prediction in acutely decompensated heart failure: The Multinational Observational Cohort on Acute Heart Failure (MOCA) study. Int. J. Cardiol. 2013, 168, 2186–2194. [Google Scholar] [CrossRef]
- Felker, G.M.; Fiuzat, M.; Thompson, V.; Shaw, L.K.; Neely, M.L.; Adams, K.F.; Whellan, D.J.; Donahue, M.P.; Ahmad, T.; Kitzman, D.W.; et al. Soluble ST2 in ambulatory patients with heart failure: Association with functional capacity and long-term outcomes. Circ. Heart Fail. 2013, 6, 1172–1179. [Google Scholar] [CrossRef] [Green Version]
- Banaszkiewicz, M.; Pietrasik, A.; DaRocha, S.; Piłka, M.; Florczyk, M.; Dobosiewicz, A.; Kędzierski, P.; Pędzich-Placha, E.; Kochman, J.; Opolski, G.; et al. Soluble ST2 protein as a new biomarker in patientswith precapillary pulmonary hypertension. Arch. Med. Sci. 2020, 16. [Google Scholar] [CrossRef]
- Haeck, M.L.; Scherptong, R.W.; Marsan, N.A.; Holman, E.R.; Schalij, M.J.; Bax, J.J.; Vliegen, H.W.; Delgado, V. Prognostic Value of Right Ventricular Longitudinal Peak Systolic Strain in Patients with Pulmonary Hypertension. Circ. Cardiovasc. Imaging 2012, 5, 628–636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fine, N.M.; Chen, L.; Bastiansen, P.M.; Frantz, R.P.; Pellikka, P.A.; Oh, J.K.; Kane, G.C. Outcome Prediction by Quantitative Right Ventricular Function Assessment in 575 Subjects Evaluated for Pulmonary Hypertension. Circ. Cardiovasc. Imaging 2013, 6, 711–721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siennicka, A.; DaRocha, S.; Banaszkiewicz, M.; Kędzierski, P.; Dobosiewicz, A.; Błaszczak, P.; Peregud-Pogorzelska, M.; Kasprzak, J.D.; Tomaszewski, M.; Mroczek, E.; et al. Treatment of chronic thromboembolic pulmonary hypertension in a multidisciplinary team. Ther. Adv. Respir. Dis. 2018, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plácido, R.; Cortez-Dias, N.; Martins, S.R.; Almeida, A.G.; Calisto, C.; Gonçalves, S.; Sadoune, M.; Diogo, A.N.; Mebazaa, A.; Pinto, F.J. Prognostic stratification in pulmonary hypertension: A multi-biomarker approach. Rev. Port. Cardiol. 2017, 36, 111–125. [Google Scholar] [CrossRef] [PubMed]
- Manzano-Fernández, S.; Januzzi, J.; Pastor-Pérez, F.; Bonaque-González, J.; Boronat-Garcia, M.; Pascual-Figal, D.; Montalban-Larrea, S.; Navarro-Peñalver, M.; Andreu-Cayuelas, J.; Valdés, M. Serial Monitoring of Soluble Interleukin Family Member ST2 in Patients with Acutely Decompensated Heart Failure. Cardiology 2012, 122, 158–166. [Google Scholar] [CrossRef] [PubMed]
- Gaggin, H.K.; Motiwala, S.; Bhardwaj, A.; Parks, K.A.; Januzzi, J.L., Jr. Soluble concentrations of the interleukin receptor family member ST2 and beta-blocker therapy in chronic heart failure. Circ. Heart Fail. 2013, 6, 1206–1213. [Google Scholar] [CrossRef] [Green Version]
- Kriechbaum, S.D.; Wiedenroth, C.B.; Keller, T.; Wolter, J.S.; Ajnwojner, R.; Peters, K.; Haas, M.A.; Roller, F.C.; Breithecker, A.; Rieth, A.J.; et al. Dynamics of high-sensitivity cardiac troponin T during therapy with balloon pulmonary angioplasty for chronic thromboembolic pulmonary hypertension. PLoS ONE 2018, 13, e0204683. [Google Scholar] [CrossRef]
- Kriechbaum, S.D.; Wiedenroth, C.B.; Wolter, J.S.; Hütz, R.; Haas, M.; Breithecker, A.; Roller, F.C.; Kriechbaum, S.; Guth, S.; Rolf, A.; et al. N-terminal pro–B-type natriuretic peptide for monitoring after balloon pulmonary angioplasty for chronic thromboembolic pulmonary hypertension. J. Heart Lung Transplant. 2018, 37, 639–646. [Google Scholar] [CrossRef]
- Kriechbaum, S.D.; Wiedenroth, C.B.; Peters, K.; Barde, M.A.; Ajnwojner, R.; Wolter, J.-S.; Haas, M.; Roller, F.C.; Guth, S.; Rieth, A.J.; et al. Galectin-3, GDF-15, and sST2 for the assessment of disease severity and therapy response in patients suffering from inoperable chronic thromboembolic pulmonary hypertension. Biomarkers 2020, 25, 578–586. [Google Scholar] [CrossRef]
- de Boer, R.A.; Nayor, M.; de Filippi, C.R.; Enserro, D.; Bhambhani, V.; Kizer, J.R.; Blaha, M.J.; Brouwers, F.P.; Cushman, M.; Lima, J.A.; et al. Association of Cardiovascular Biomarkers with Incident Heart Failure With Preserved and Reduced Ejection Fraction. JAMA Cardiol. 2018, 3, 215–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Willems, S.; Sels, J.-W.; Flier, S.; Versteeg, D.; Buhre, W.F.; De Kleijn, D.P.; Hoefer, I.E.; Pasterkamp, G. Temporal changes of soluble ST2 after cardiovascular interventions. Eur. J. Clin. Investig. 2013, 43, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Ejiri, K.; Ogawa, A.; Fujii, S.; Ito, H.; Matsubara, H. Vascular Injury Is a Major Cause of Lung Injury After Balloon Pulmonary Angioplasty in Patients with Chronic Thromboembolic Pulmonary Hypertension. Circ. Cardiovasc. Interv. 2018, 11, e005884. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bayés-Genis, A.; González, A.; Lupón, J. ST2 in Heart Failure. Circ. Hear. Fail. 2018, 11, e005582. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | All Study Population |
|---|---|
| Procedures, n | 57 |
| Age (years) | 52 ± 19 |
| WHO FC, n (%) | |
| I | 4 (7%) |
| II | 24 (42%) |
| III | 28 (49%) |
| IV | 1(2%) |
| mRAP (mmHg) | 6.9 ± 3.9 |
| mPAP (mmHg) | 43.9 ± 10.9 |
| PVR (Wood Unit) | 7.6 ± 3.8 |
| CO (L/min) | 5.0 ± 1.2 |
| CI (L/min × m2) | 2.8 ± 0.6 |
| MVsatO2 (%) | 67.7 ± 6.3 |
| AOsatO2 (%) | 95.6 ± 2.9 |
| sST2 (ng/mL) | 26.56 (16.66–40.83) |
| NT-proBNP (pg/mL) | 451 (178–1293) |
| TnT (ng/mL) | 0.009 (0.006–0.017) |
| Variables | Admission Day | 24 h after Procedure | 48 h after Procedure | Discharge Day | p1 Value | p2 Value | p3 Value |
|---|---|---|---|---|---|---|---|
| sST2 (ng/mL) | 26.56 (16.66–40.83) | 33.31 (20.81–62.56) | 27.45 (17.66–54.45) | 21.59 (12.50–33.48) | 0.048 | <0.001 | 0.028 |
| NT-proBNP (pg/mL) | 451 (178–1293) | 368 (147–996) | 317 (129–851) | 240 (132–1077) | 0.010 | 0.006 | 0.013 |
| TnT (ng/mL) | 0.009 (0.006–0.017) | 0.01 (0.006–0.019) | 0.009 (0.006–0.017) | 0.011 (0.006–0.014) | 0.44 | 0.006 | 0.078 |
| Variables | No Complications in Postprocedural Period | Complications in Postprocedural Period | p Value |
|---|---|---|---|
| Procedures, n | 42 | 15 | - |
| mRAP (mmHg) | 6.6 ± 3.6 | 7.6 ± 4.0 | 0.379 |
| mPAP (mmHg) | 41.6 ± 10.1 | 50.3 ± 10.7 | 0.009 |
| PVR (Wood Unit) | 7.0 ± 3.6 | 9.5 ± 4.1 | 0.025 |
| CO (L/min) | 5.1 ± 1.3 | 4.72 ± 1.1 | 0.285 |
| CI (L/min·m2) | 2.8 ± 0.6 | 2.64 ± 0.5 | 0.320 |
| MVsatO2 (%) | 69.1 ± 5.4 | 63.7 ± 7.1 | 0.009 |
| AOsatO2 (%) | 96.3 ± 2.6 | 93.7 ± 2.9 | 0.005 |
| Variabes | No Complications in Postprocedural Period | Complications in Postprocedural Period | p | |
|---|---|---|---|---|
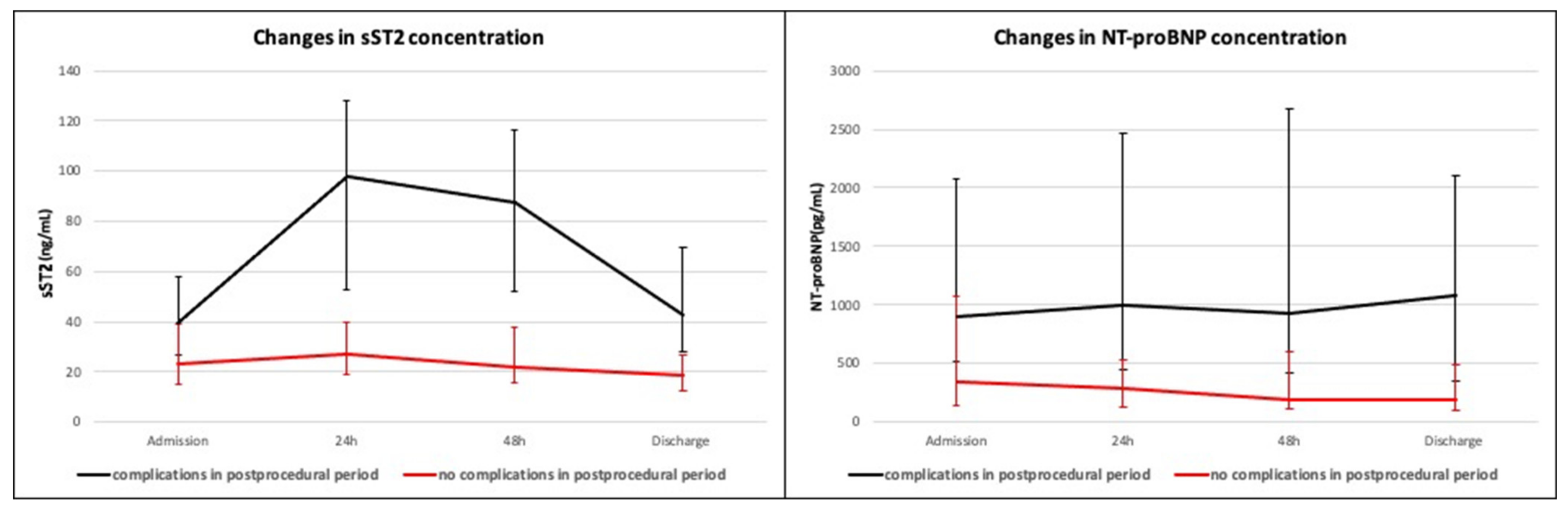
| Admission day | sST2 (ng/mL) | 23.25 (15.35–38.69) | 39.73 (24.03–47.57) | 0.044 |
| NT-proBNP (pg/mL) | 348 (139–1081) | 894 (514–2081) | 0.003 | |
| TnT (ng/mL) | 0.008 (0.00–0.01) | 0.014 (0.007–0.04) | 0.08 | |
| 24 h after procedure | sST2 (ng/mL) | 26.86 (19.10–40.12) | 97.66 (53.07–126.18) | <0.001 |
| NT-proBNP (pg/mL) | 284 (123–530) | 996 (445–2466) | 0.004 | |
| TnT (ng/mL) | 0.009 (0.01–0.014) | 0.017 (0.01–0.04) | 0.09 | |
| 48 h after procedure | sST2 (ng/mL) | 21.58 (15.73–37.67) | 87.35 (52.07–116.41) | <0.001 |
| NT-proBNP (pg/mL) | 185 (114–601) | 931 (423–2680) | 0.002 | |
| TnT (ng/mL) | 0.008 (0.01–0.02) | 0.012 (0.01–0.04) | 0.08 | |
| Discharge day | sST2 (ng/mL) | 18.64 (12.50–27.25) | 42.97 (28.18–70.20) | <0.001 |
| NT-proBNP (pg/mL) | 195 (103–487) | 1077 (348–2099) | 0.004 | |
| TnT (ng/mL) | 0.01 (0.004–0.014) | 0.014 (0.008–0.05) | 0.09 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Banaszkiewicz, M.; Pietrasik, A.; Florczyk, M.; Kędzierski, P.; Piłka, M.; Mańczak, R.; Kochman, J.; Opolski, G.; Torbicki, A.; Kurzyna, M.; et al. Soluble ST2 as a Biomarker for Early Complications in Patients with Chronic Thromboembolic Pulmonary Hypertension Treated with Balloon Pulmonary Angioplasty. Diagnostics 2021, 11, 133. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11010133
Banaszkiewicz M, Pietrasik A, Florczyk M, Kędzierski P, Piłka M, Mańczak R, Kochman J, Opolski G, Torbicki A, Kurzyna M, et al. Soluble ST2 as a Biomarker for Early Complications in Patients with Chronic Thromboembolic Pulmonary Hypertension Treated with Balloon Pulmonary Angioplasty. Diagnostics. 2021; 11(1):133. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11010133
Chicago/Turabian StyleBanaszkiewicz, Marta, Arkadiusz Pietrasik, Michał Florczyk, Piotr Kędzierski, Michał Piłka, Rafał Mańczak, Janusz Kochman, Grzegorz Opolski, Adam Torbicki, Marcin Kurzyna, and et al. 2021. "Soluble ST2 as a Biomarker for Early Complications in Patients with Chronic Thromboembolic Pulmonary Hypertension Treated with Balloon Pulmonary Angioplasty" Diagnostics 11, no. 1: 133. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11010133