
Automated Detection of Pancreatic Cystic Lesions on CT Using Deep Learning

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
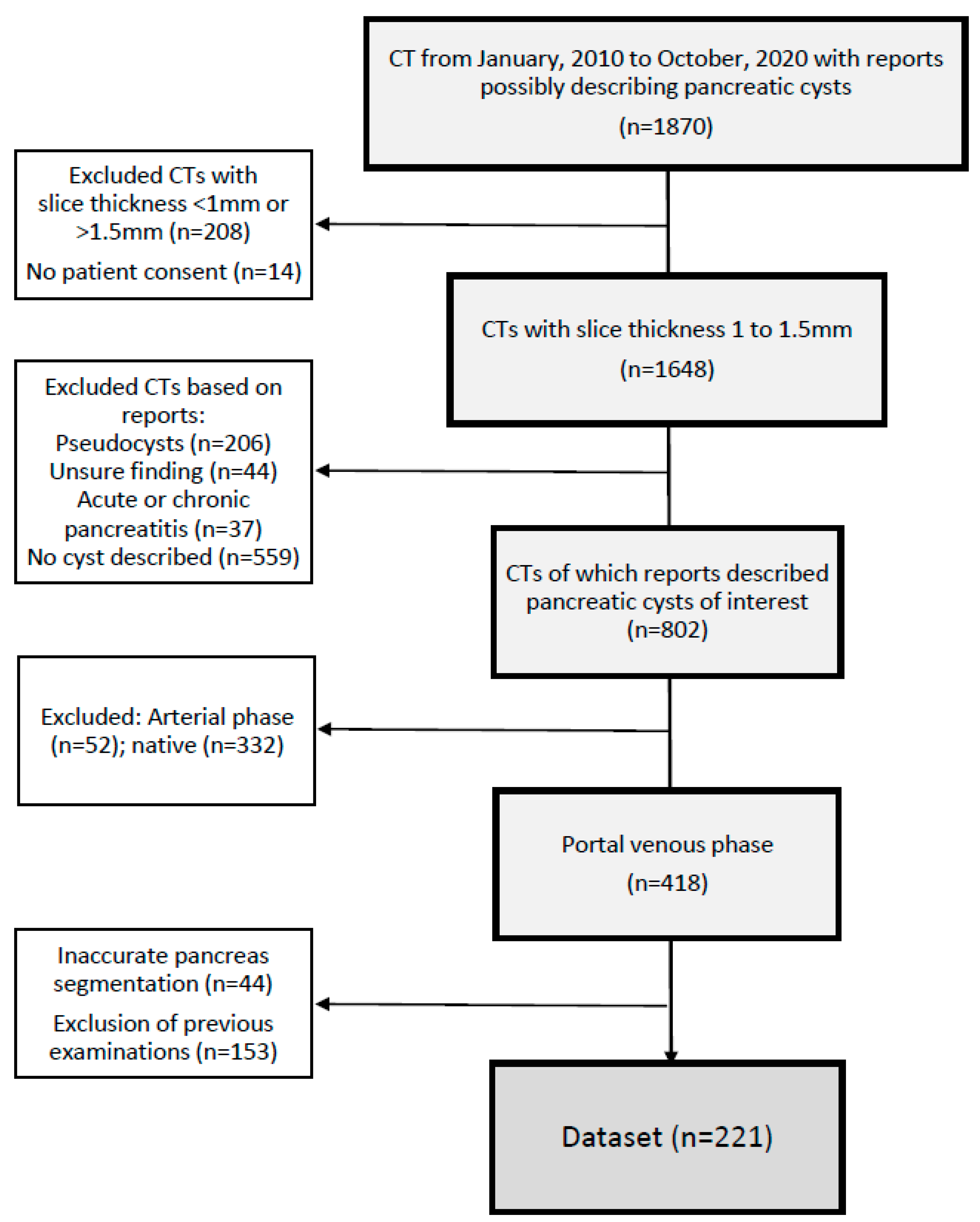
2.1. Data Selection
2.2. Patient Characteristics and Radiology Report Information
2.3. CT Protocols
2.4. Data Preprocessing: Cropping of CTs to the Region Showing the Pancreas
2.5. Ground-Truth Generation
2.5.1. Segmentation of PCLs
2.5.2. Segmentation of Main Pancreatic Ducts (MPD)
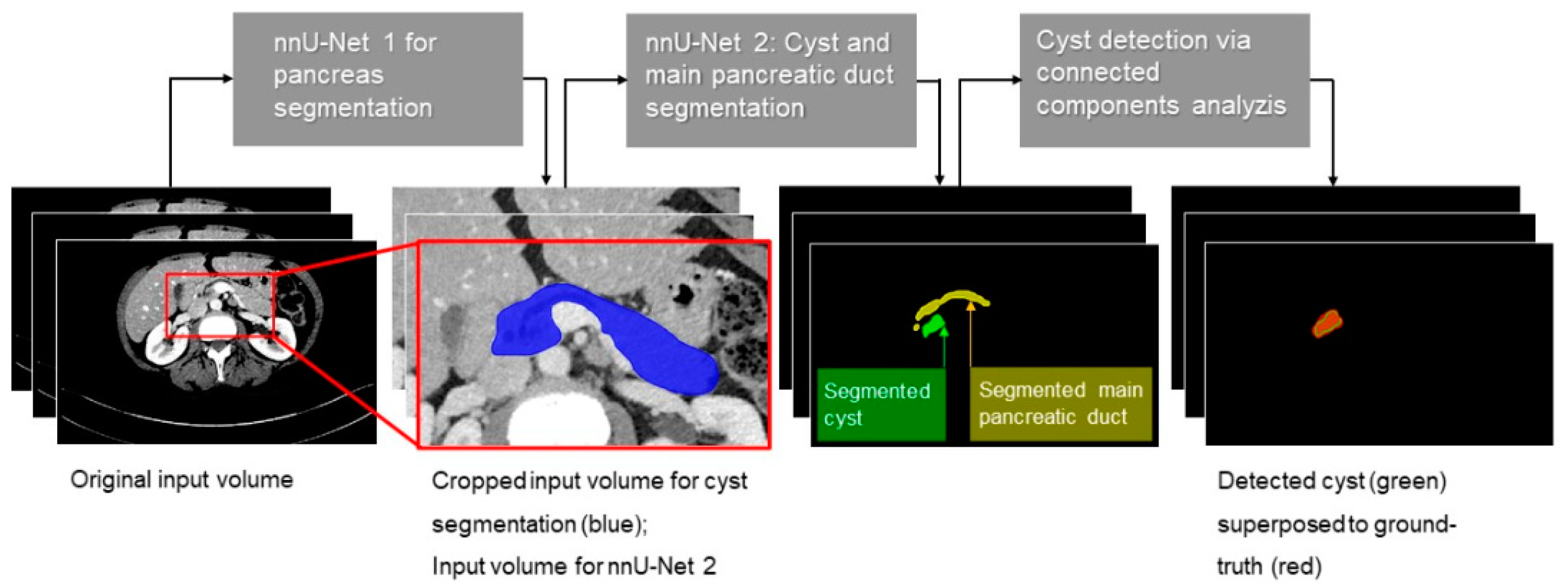
2.6. Algorithm
2.7. Performance Subanalyses Regarding PCL Size and Location within the Pancreas
2.8. Comparison of Model’s Performance with Human Readers
2.9. Statistical Analysis
3. Results
3.1. General Performance
3.2. Performance Sub-Analyses
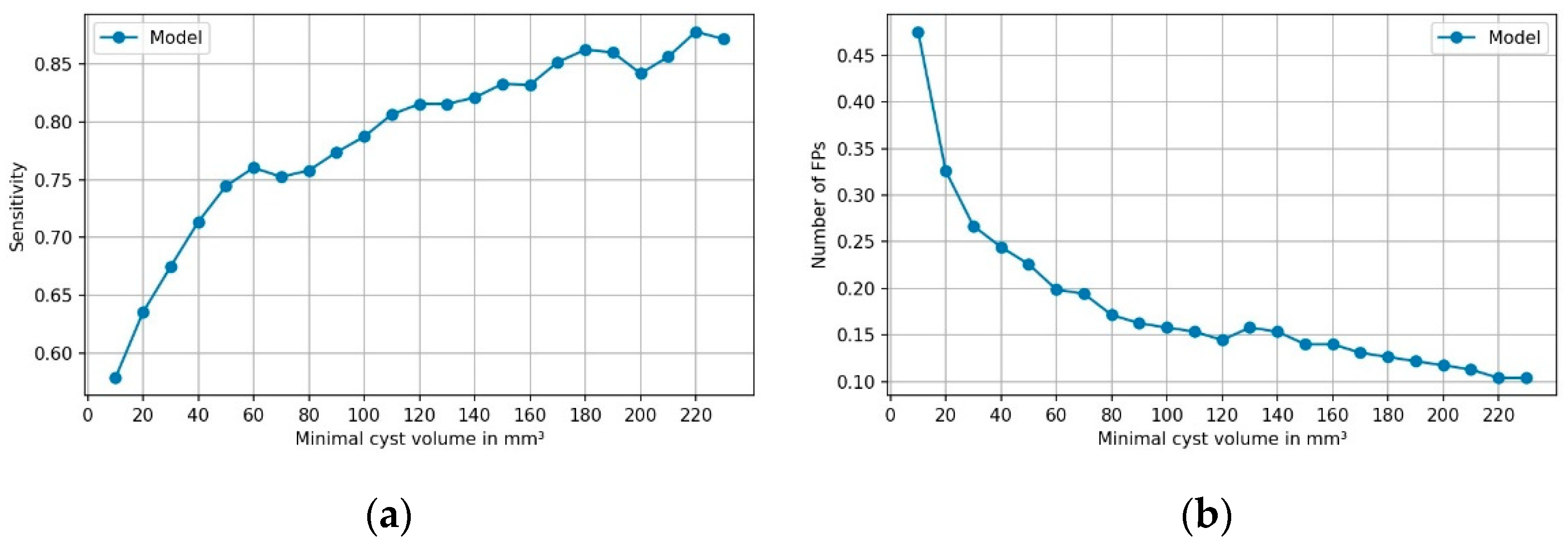
3.2.1. Performance Depending on Cyst Volume
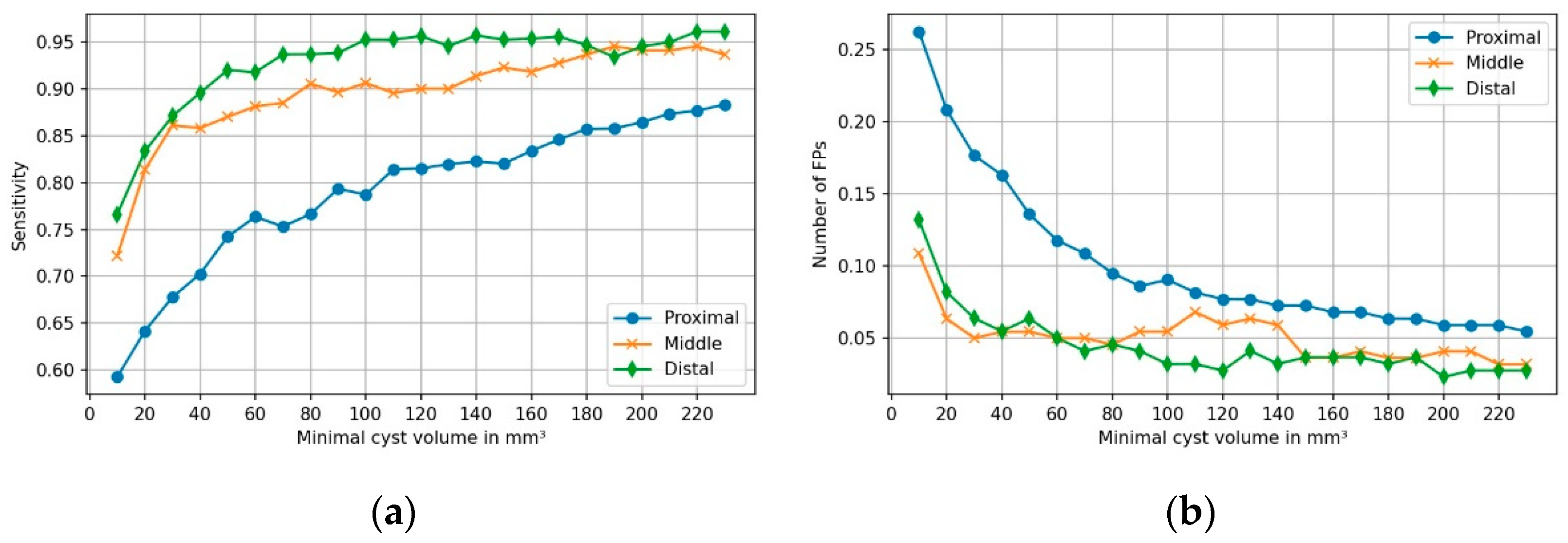
3.2.2. Performance Depending on Cysts’ Location within Pancreas
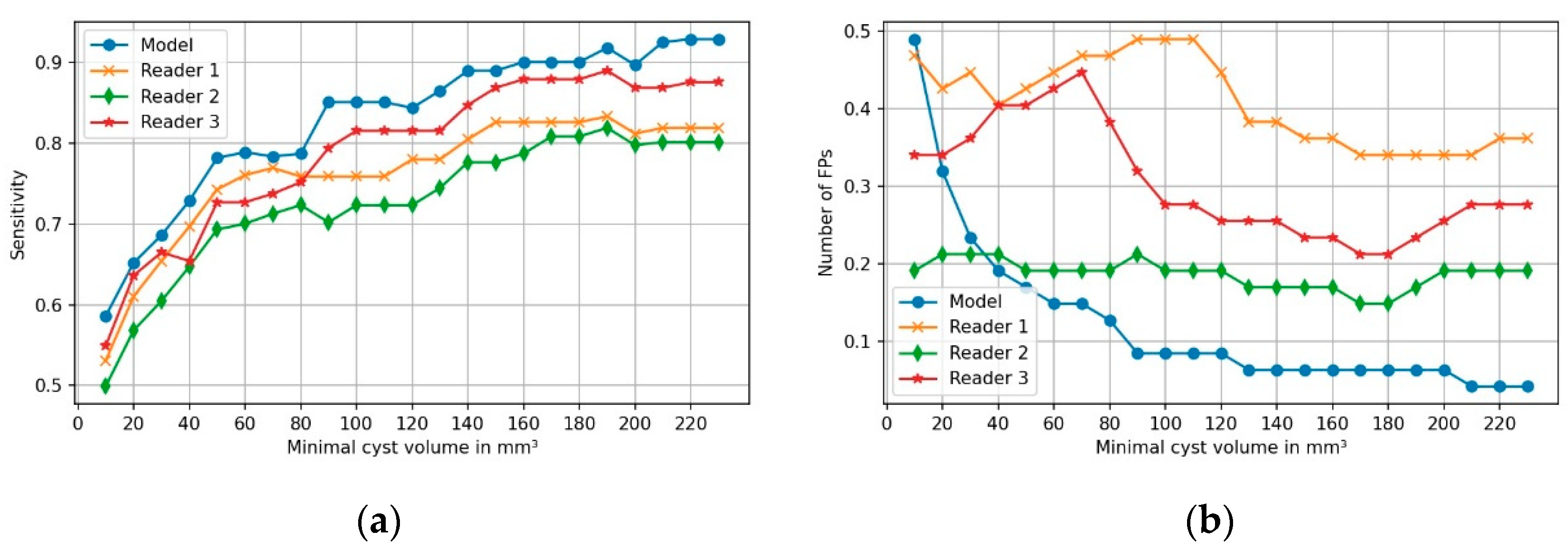
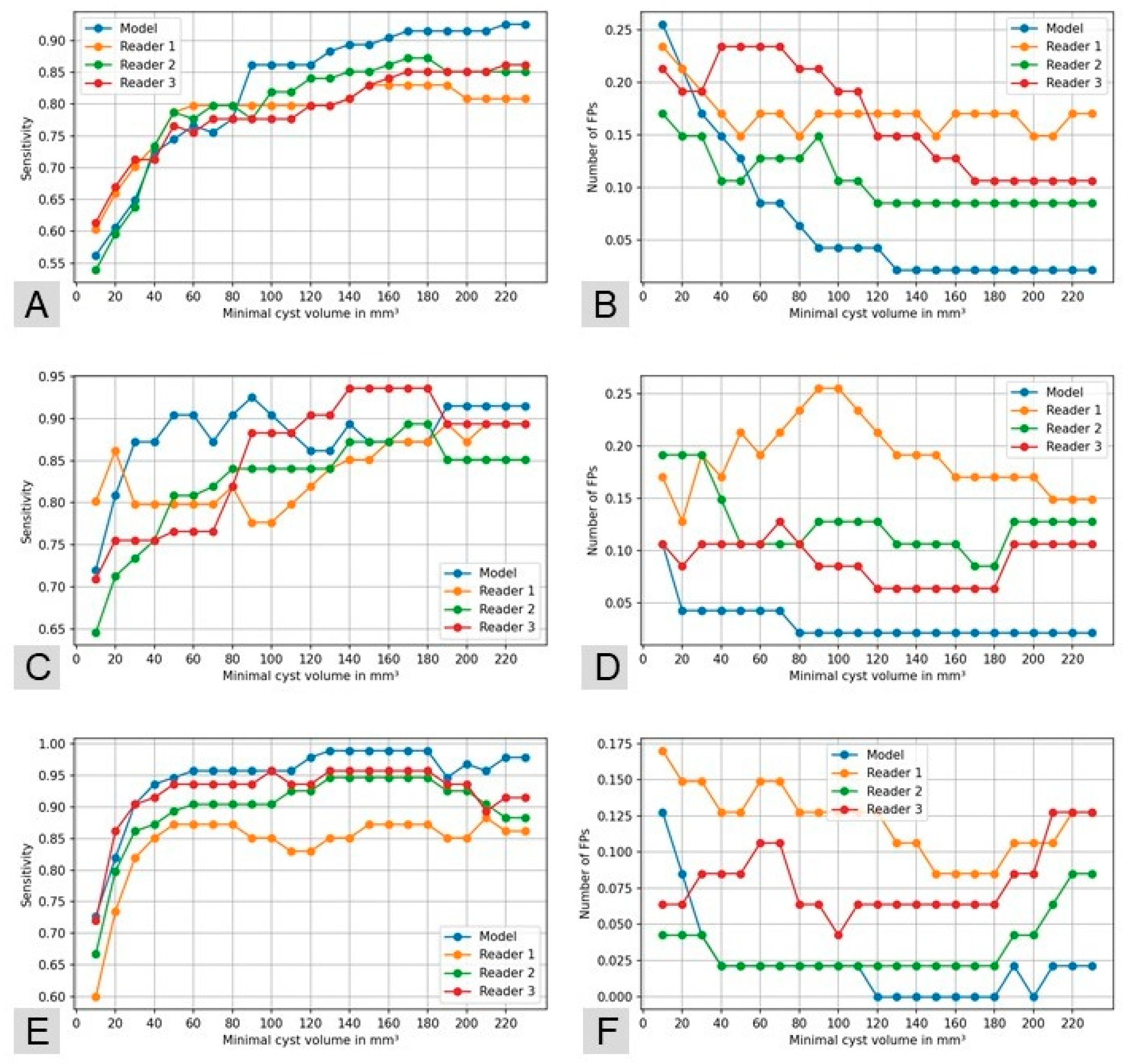
3.3. Comparison of Model’s Performance with Human Readers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix B

References
- Laffan, T.A.; Horton, K.M.; Klein, A.P.; Berlanstein, B.; Siegelman, S.S.; Kawamoto, S.; Johnson, P.T.; Fishman, E.K.; Hruban, R.H. Prevalence of Unsuspected Pancreatic Cysts on MDCT. AJR Am. J. Roentgenol. 2008, 191, 802–807. [Google Scholar] [CrossRef] [Green Version]
- Zanini, N.; Giordano, M.; Smerieri, E.; Cipolla d’Abruzzo, G.; Guidi, M.; Pazzaglini, G.; De Luca, F.; Chiaruzzi, G.; Vitullo, G.; Piva, P.; et al. Estimation of the Prevalence of Asymptomatic Pancreatic Cysts in the Population of San Marino. Pancreatology 2015, 15, 417–422. [Google Scholar] [CrossRef]
- Kromrey, M.-L.; Bülow, R.; Hübner, J.; Paperlein, C.; Lerch, M.M.; Ittermann, T.; Völzke, H.; Mayerle, J.; Kühn, J.-P. Prospective Study on the Incidence, Prevalence and 5-Year Pancreatic-Related Mortality of Pancreatic Cysts in a Population-Based Study. Gut 2018, 67, 138–145. [Google Scholar] [CrossRef] [Green Version]
- European Evidence-Based Guidelines on Pancreatic Cystic Neoplasms. Gut 2018, 67, 789–804. [CrossRef]
- Chakraborty, J.; Midya, A.; Gazit, L.; Attiyeh, M.; Langdon-Embry, L.; Allen, P.J.; Do, R.K.G.; Simpson, A.L. CT Radiomics to Predict High-Risk Intraductal Papillary Mucinous Neoplasms of the Pancreas. Med. Phys. 2018, 45, 5019–5029. [Google Scholar] [CrossRef]
- Barkin, J.A.; Barkin, J.S. Pancreatic Cysts: Controversies, Advances, Diagnoses, and Therapies. Pancreas 2017, 46, 735–741. [Google Scholar] [CrossRef] [PubMed]
- Ferrone, C.R.; Correa-Gallego, C.; Warshaw, A.L.; Brugge, W.R.; Forcione, D.G.; Thayer, S.P.; Castillo, C.F. Current Trends in Pancreatic Cystic Neoplasms. Arch. Surg. Chic. Ill 1960 2009, 144, 448–454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crippa, S.; Castillo, C.F.; Salivia, R.; Finkelstein, D.; BASSI, C.; Dominguez, I.; Muzikansky, A.; Thayer, S.P.; Falconi, M.; Mino–Kenudson, M.; et al. Mucin-Producing Neoplasms of the Pancreas: An Analysis of Distinguishing Clinical and Epidemiologic Characteristics. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2010, 8, 213–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodriguez, J.R.; Salivia, R.; Crippa, S.; Warshaw, A.L.; Bassi, C.; Falconi, M.; Thayer, S.P.; Lauwers, G.Y.; Capelli, P.; Mino–Kenudson, M.; et al. Branch-Duct Intraductal Papillary Mucinous Neoplasms: Observations in 145 Patients Who Underwent Resection. Gastroenterology 2007, 133, 72–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanno, A.; Satoh, K.; Hirota, M.; Hamada, S.; Umino, J.; Itoh, H.; Masamune, A.; Asakura, T.; Shimosegawa, T. Prediction of Invasive Carcinoma in Branch Type Intraductal Papillary Mucinous Neoplasms of the Pancreas. J. Gastroenterol. 2010, 45, 952–959. [Google Scholar] [CrossRef]
- Sahora, K.; Crippa, S.; Zamboni, G.; Ferrone, C.; Warshaw, A.L.; Lillemoe, K.; Mino-Kenudson, M.; Falconi, M.; Fernandez-del Castillo, C. Intraductal Papillary Mucinous Neoplasms of the Pancreas with Concurrent Pancreatic and Periampullary Neoplasms. Eur. J. Surg. Oncol. EJSO 2016, 42, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Ideno, N.; Ohtsuka, T.; Kono, H.; Fujiwara, K.; Oda, Y.; Aishima, S.; Ito, T.; Ishigami, K.; Tokunaga, S.; Ohuchida, K.; et al. Intraductal Papillary Mucinous Neoplasms of the Pancreas With Distinct Pancreatic Ductal Adenocarcinomas Are Frequently of Gastric Subtype. Ann. Surg. 2013, 258, 141–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vosshenrich, J.; Brantner, P.; Cyriac, J.; Boll, D.T.; Merkle, E.M.; Heye, T. Quantifying Radiology Resident Fatigue: Analysis of Preliminary Reports. Radiology 2021, 298, 8. [Google Scholar] [CrossRef] [PubMed]
- Ruutiainen, A.T.; Durand, D.J.; Scanlon, M.H.; Itri, J.N. Increased Error Rates in Preliminary Reports Issued by Radiology Residents Working More Than 10 Consecutive Hours Overnight. Acad. Radiol. 2013, 20, 305–311. [Google Scholar] [CrossRef]
- Stec, N.; Arje, D.; Moody, A.R.; Krupinski, E.A.; Tyrrell, P.N. A Systematic Review of Fatigue in Radiology: Is It a Problem? Am. J. Roentgenol. 2018, 210, 799–806. [Google Scholar] [CrossRef] [PubMed]
- Giger, M.L. Machine Learning in Medical Imaging. J. Am. Coll. Radiol. 2018, 15, 512–520. [Google Scholar] [CrossRef]
- Waite, S.; Kolla, S.; Jeudy, J.; Legasto, A.; Macknik, S.L.; Martinez-Conde, S.; Krupinski, E.A.; Reede, D.L. Tired in the Reading Room: The Influence of Fatigue in Radiology. J. Am. Coll. Radiol. 2017, 14, 191–197. [Google Scholar] [CrossRef]
- Kim, H.Y.; Lee, K.; Chang, W.; Kim, Y.; Lee, S.; Oh, D.Y.; Sunwoo, L.; Lee, Y.J.; Kim, Y.H. Robustness of Deep Learning Algorithm to Varying Imaging Conditions in Detecting Low Contrast Objects in Computed Tomography Phantom Images: In Comparison to 12 Radiologists. Diagnostics 2021, 11, 410. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Hatipoglu, S.; Alonso-Álvarez, D.; Gatehouse, P.; Li, B.; Gao, Y.; Firmin, D.; Keegan, J.; Yang, G. Fast and Automated Segmentation for the Three-Directional Multi-Slice Cine Myocardial Velocity Mapping. Diagnostics 2021, 11, 346. [Google Scholar] [CrossRef]
- Weikert, T.; Winkel, D.J.; Bremerich, J.; Stieltjes, B.; Parmar, V.; Sauter, A.W.; Sommer, G. Automated Detection of Pulmonary Embolism in CT Pulmonary Angiograms Using an AI-Powered Algorithm. Eur. Radiol. 2020, 30, 6545–6553. [Google Scholar] [CrossRef]
- Winkel, D.J.; Weikert, T.J.; Breit, H.-C.; Chabin, G.; Gibson, E.; Heye, T.J.; Comaniciu, D.; Boll, D.T. Validation of a Fully Automated Liver Segmentation Algorithm Using Multi-Scale Deep Reinforcement Learning and Comparison versus Manual Segmentation. Eur. J. Radiol. 2020, 126, 108918. [Google Scholar] [CrossRef] [PubMed]
- Winkel, D.J.; Breit, H.-C.; Shi, B.; Boll, D.T.; Seifert, H.-H.; Wetterauer, C. Predicting Clinically Significant Prostate Cancer from Quantitative Image Features Including Compressed Sensing Radial MRI of Prostate Perfusion Using Machine Learning: Comparison with PI-RADS v2 Assessment Scores. Quant. Imaging Med. Surg. 2020, 10, 808–823. [Google Scholar] [CrossRef]
- Zheng, Q.; Yang, L.; Zeng, B.; Li, J.; Guo, K.; Liang, Y.; Liao, G. Artificial Intelligence Performance in Detecting Tumor Metastasis from Medical Radiology Imaging: A Systematic Review and Meta-Analysis. EClinicalMedicine 2021, 31, 100669. [Google Scholar] [CrossRef]
- Saba, L.; Biswas, M.; Kuppili, V.; Cuadrado Godia, E.; Suri, H.S.; Edla, D.R.; Omerzu, T.; Laird, J.R.; Khanna, N.N.; Mavrogeni, S.; et al. The Present and Future of Deep Learning in Radiology. Eur. J. Radiol. 2019, 114, 14–24. [Google Scholar] [CrossRef] [PubMed]
- McBee, M.P.; Awan, O.A.; Colucci, A.T.; Ghobadi, C.W.; Kadom, N.; Kansagra, A.P.; Tridandapani, S.; Auffermann, W.F. Deep Learning in Radiology. Acad. Radiol. 2018, 25, 1472–1480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, Y.; Xie, L.; Fishman, E.K.; Yuille, A.L. Deep Supervision for Pancreatic Cyst Segmentation in Abdominal CT Scans. In Proceedings of the Medical Image Computing and Computer Assisted Intervention—MICCAI 2017, Quebec City, QC, Canada, 11–13 September 2017; Descoteaux, M., Maier-Hein, L., Franz, A., Jannin, P., Collins, D.L., Duchesne, S., Eds.; Springer International Publishing: Cham, Germany, 2017; pp. 222–230. [Google Scholar]
- Chu, L.C.; Park, S.; Kawamoto, S.; Wang, Y.; Zhou, Y.; Shen, W.; Zhu, Z.; Xia, Y.; Xie, L.; Liu, F.; et al. Application of Deep Learning to Pancreatic Cancer Detection: Lessons Learned From Our Initial Experience. J. Am. Coll. Radiol. 2019, 16, 1338–1342. [Google Scholar] [CrossRef] [PubMed]
- Xie, L.; Yu, Q.; Zhou, Y.; Wang, Y.; Fishman, E.K.; Yuille, A.L. Recurrent Saliency Transformation Network for Tiny Target Segmentation in Abdominal CT Scans. IEEE Trans. Med. Imaging 2020, 39, 514–525. [Google Scholar] [CrossRef]
- Weikert, T.; Cyriac, J.; Yang, S.; Nesic, I.; Parmar, V.; Stieltjes, B. A Practical Guide to Artificial Intelligence–Based Image Analysis in Radiology. Investig. Radiol. 2020, 55, 1–7. [Google Scholar] [CrossRef]
- Isensee, F.; Jäger, P.F.; Kohl, S.A.A.; Petersen, J.; Maier-Hein, K.H. Automated Design of Deep Learning Methods for Biomedical Image Segmentation. Nat. Methods 2020, 18, 203–211. [Google Scholar] [CrossRef]
- NORA-Medical Imaging Platform. Available online: Https://Www.Nora-Imaging.Com/ (accessed on 23 March 2021).
- Vilas-Boas, F.; Macedo, G. Management Guidelines for Pancreatic Cystic Lesions: Should We Adopt or Adapt the Current Roadmaps? J. Gastrointestin. Liver Dis. 2019, 28, 495–501. [Google Scholar] [CrossRef]
- Stutchfield, B.M.; Nayar, M.; Penman, I.D. Pancreatic Cystic Lesions: Risk Stratification and Management Based on Recent Guidelines. Frontline Gastroenterol. 2019, 10, 182–187. [Google Scholar] [CrossRef]
- Bai, H.X.; Wang, R.; Xiong, Z.; Hsieh, B.; Chang, K.; Halsey, K.; Tran, T.M.L.; Choi, J.W.; Wang, D.-C.; Shi, L.-B.; et al. Artificial Intelligence Augmentation of Radiologist Performance in Distinguishing COVID-19 from Pneumonia of Other Origin at Chest CT. Radiology 2020, 296, E156–E165. [Google Scholar] [CrossRef]
- Summers, R.M. Progress in Fully Automated Abdominal CT Interpretation. AJR Am. J. Roentgenol. 2016, 207, 67–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pandey, P.; Pandey, A.; Luo, Y.; Aliyari Ghasabeh, M.; Khoshpouri, P.; Ameli, S.; O’Broin-Lennon, A.M.; Canto, M.; Hruban, R.H.; Goggins, M.S.; et al. Follow-up of Incidentally Detected Pancreatic Cystic Neoplasms: Do Baseline MRI and CT Features Predict Cyst Growth? Radiology 2019, 292, 647–654. [Google Scholar] [CrossRef]
- Tanaka, M.; Fernández-del Castillo, C.; Kamisawa, T.; Jang, J.Y.; Levy, P.; Ohtsuka, T.; Salvia, R.; Shimizu, Y.; Tada, M.; Wolfgang, C.L. Revisions of International Consensus Fukuoka Guidelines for the Management of IPMN of the Pancreas. Pancreatology 2017, 17, 738–753. [Google Scholar] [CrossRef]
- Hasan, A.; Visrodia, K.; Farrell, J.J.; Gonda, T.A. Overview and Comparison of Guidelines for Management of Pancreatic Cystic Neoplasms. World J. Gastroenterol. 2019, 25, 4405–4413. [Google Scholar] [CrossRef]
- Tanaka, M. Clinical Management and Surgical Decision-Making of IPMN of the Pancreas. In Pancreatic Cancer; Su, G.H., Ed.; Springer: New York, NY, USA, 2019; Volume 1882, pp. 9–22. ISBN 978-1-4939-8878-5. [Google Scholar]
- van Huijgevoort, N.C.M.; del Chiaro, M.; Wolfgang, C.L.; van Hooft, J.E.; Besselink, M.G. Diagnosis and Management of Pancreatic Cystic Neoplasms: Current Evidence and Guidelines. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 676–689. [Google Scholar] [CrossRef]
- Lee, J.E.; Choi, S.-Y.; Min, J.H.; Yi, B.H.; Lee, M.H.; Kim, S.S.; Hwang, J.A.; Kim, J.H. Determining Malignant Potential of Intraductal Papillary Mucinous Neoplasm of the Pancreas: CT versus MRI by Using Revised 2017 International Consensus Guidelines. Radiology 2019, 293, 134–143. [Google Scholar] [CrossRef]
- Tobaly, D.; Santinha, J.; Sartoris, R.; Burgio, M.D.; Matos, C.; Cros, J.; Couvelard, A.; Rebours, V.; Sauvanet, A.; Ronot, M.; et al. CT-Based Radiomics Analysis to Predict Malignancy in Patients with Intraductal Papillary Mucinous Neoplasm (IPMN) of the Pancreas. Cancers 2020, 12, 3089. [Google Scholar] [CrossRef]
- Sun, Y.; Yang, S.; Qi, E.; Liu, F.; Zhou, F.; Lu, Y.; Liang, P.; Ye, H.; Yu, X. Comparative Diagnostic Evaluation with Contrast-Enhanced Ultrasound, Computed Tomography and Magnetic Resonance Imaging in Patients with Pancreatic Cystic Neoplasms. Cancer Manag. Res. 2020, 12, 2889–2898. [Google Scholar] [CrossRef]
- Fábrega-Foster, K.; Kamel, I.R.; Horowitz, J.M.; Arif-Tiwari, H.; Bashir, M.R.; Chernyak, V.; Goldstein, A.; Grajo, J.R.; Hindman, N.M.; Kamaya, A.; et al. ACR Appropriateness Criteria® Pancreatic Cyst. J. Am. Coll. Radiol. 2020, 17, S198–S206. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | n (%) | Mean (±SD 1) in mm | Median in mm |
|---|---|---|---|
| Reported number of cysts per patient | 1.2 (0.4) | ||
| Size: | |||
| Maximal diameter | 12.8 (7.7) | 12.0 | |
| Minimal diameter | 11.6 (7.3) | 10.0 | |
| Mean diameter | 13.3 (7.4) | 11.5 | |
| Radiologically suspected diagnosis: | |||
| IPMN | 173 (78.3) | ||
| Indeterminate | 36 (16.2) | ||
| SCN 2 | 5 (2.3) | ||
| MCN 3 | 5 (2.3) | ||
| Others (lymphangioma, ontogenetic cyst) | 2 (0.9) |
| Cyst Volume Group [mm3] | Sensitivity (%) | FPs/Case | F1-Score |
|---|---|---|---|
| 10–50 | 40.1 | 0.33 | 0.40 |
| >50–200 | 65.5 | 0.19 | 0.66 |
| >200–600 | 75.9 | 0.11 | 0.76 |
| >600 | 91.9 | 0.08 | 0.91 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abel, L.; Wasserthal, J.; Weikert, T.; Sauter, A.W.; Nesic, I.; Obradovic, M.; Yang, S.; Manneck, S.; Glessgen, C.; Ospel, J.M.; et al. Automated Detection of Pancreatic Cystic Lesions on CT Using Deep Learning. Diagnostics 2021, 11, 901. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11050901
Abel L, Wasserthal J, Weikert T, Sauter AW, Nesic I, Obradovic M, Yang S, Manneck S, Glessgen C, Ospel JM, et al. Automated Detection of Pancreatic Cystic Lesions on CT Using Deep Learning. Diagnostics. 2021; 11(5):901. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11050901
Chicago/Turabian StyleAbel, Lorraine, Jakob Wasserthal, Thomas Weikert, Alexander W. Sauter, Ivan Nesic, Marko Obradovic, Shan Yang, Sebastian Manneck, Carl Glessgen, Johanna M. Ospel, and et al. 2021. "Automated Detection of Pancreatic Cystic Lesions on CT Using Deep Learning" Diagnostics 11, no. 5: 901. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11050901