
Integrating Electrocardiography and Vectorcardiography in the Differential Diagnosis of Wide Complex Tachycardia in a Patient with Left Ventricular Noncompaction: A Case Report and Brief Literature Review


Abstract
:1. Introduction
2. Case Presentation
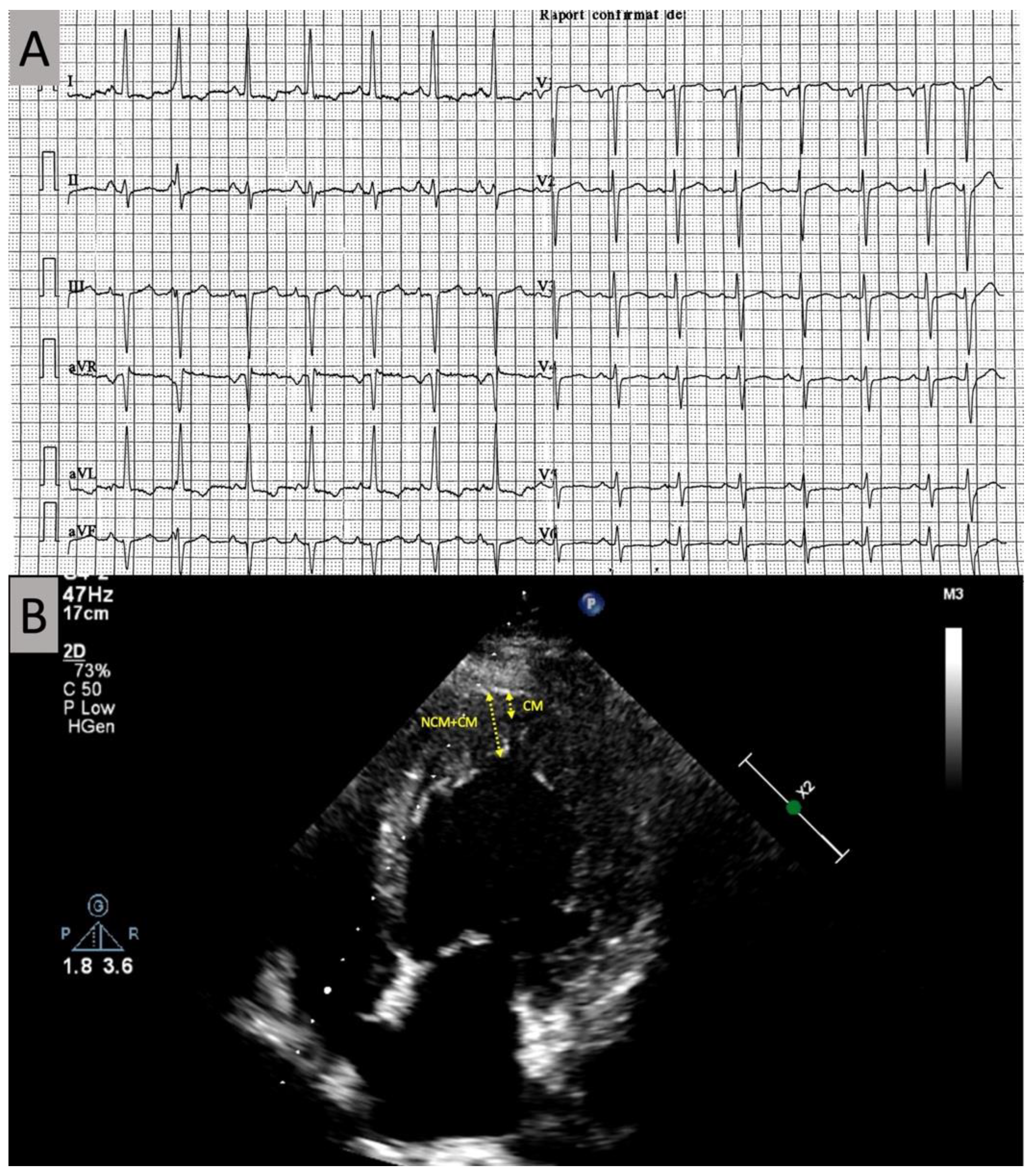
2.1. Investigations
2.2. Management
3. Discussion
3.1. Atrial and Ventricular Arrhythmias in LVNC
3.2. Established Algorithms for the Differential Diagnosis of WCT
3.3. Mode of Initiation of the WCT Episode
3.4. Vectorcardiographic Analysis of WCT: Differences in Ventricular Activation Velocity
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Finsterer, J.; Stöllberger, C.; Towbin, J.A. Left ventricular noncompaction cardiomyopathy: Cardiac, neuromuscular, and genetic factors. Nat. Rev. Cardiol. 2017, 14, 224–237. [Google Scholar] [CrossRef]
- Jenni, R.; Oechslin, E.N.; van der Loo, B. Isolated ventricular non-compaction of the myocardium in adults. Heart 2007, 93, 11–15. [Google Scholar] [CrossRef] [Green Version]
- Maron, B.J.; Towbin, J.A.; Thiene, G.; Antzelevitch, C.; Corrado, D.; Arnett, D.; Moss, A.J.; Seidman, C.E.; Young, J.B. American Heart Association. Contemporary definitions and classification of the cardiomyopathies: An American Heart Association Scientific Statement from the Council on Clinical Cardiology, Heart Failure and Transplantation Committee; Quality of Care and Outcomes Research and Functional Genomics and Translational Biology Interdisciplinary Working Groups; and Council on Epidemiology and Prevention. Circulation 2006, 113, 1807–1816. [Google Scholar]
- Arbustini, E.; Favalli, V.; Narula, N.; Serio, A.; Grasso, M. Left Ventricular Noncompaction: A Distinct Genetic Cardiomyopathy? J. Am. Coll. Cardiol. 2016, 68, 949–966. [Google Scholar] [CrossRef]
- Oechslin, E.; Jenni, R. Left Ventricular Noncompaction: From Physiologic Remodeling to Noncompaction Cardiomyopathy. J. Am. Coll. Cardiol. 2018, 71, 723–726. [Google Scholar] [CrossRef]
- Di Fusco, S.A.; Luca, F.; Madeo, A.; Massimiliano Rao, C.; Iorio, A.; Rizzo, M.; Dalila Luisella Delcre, S.; Colivicchi, F.; Gabrielli, D.; Paolo Pino, G.; et al. Left Ventricular Noncompaction: Diagnostic Approach, Prognostic Evaluation, and Man-agement Strategies. Cardiol. Rev. 2020, 28, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Mendoza, L.; Chan, W.; McFarlane, I.M. Non-Compaction Cardiomyopathy Presented with Atrial Fibrillation: A Case Report and Literature Review. Am. J. Med. Case Rep. 2020, 8, 281–283. [Google Scholar] [CrossRef]
- Munoz, J.J.S.; Munoz-Esparza, C.; Verdu, P.P.; Sanchez, J.M.; Almagro, F.G.; Ruiz, G.E.; Blanes, J.R.; Alberola, A.G. Catheter ablation of ventricular arrhythmias in left ventricular noncompaction cardiomyopathy. Heart Rhythm. 2021, 18, 545–552. [Google Scholar] [CrossRef] [PubMed]
- Jenni, R.; Oechslin, E.; Schneider, J.; Jost, C.A.; A Kaufmann, P. Echocardiographic and pathoanatomical characteristics of isolated left ventricular non-compaction: A step towards classification as a distinct cardiomyopathy. Heart 2001, 86, 666–671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steffel, J.; Kobza, R.; Oechslin, E.; Jenni, R.; Duru, F. Electrocardiographic characteristics at initial diagnosis in patients with isolated left ventricular noncompaction. Am. J. Cardiol. 2009, 104, 984–989. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Urooj, F.; Khan, M.E.; Choudhary, G.; Kulkarni, A.; Singh, M.; Dwight, S. An Uncommon Presentation of Broad Complex Tachycardia with Aberrant Conduction in Patient With Ventricular Noncompaction Cardiomyopathy. Chest 2014, 146. [Google Scholar] [CrossRef]
- Stöllberger, C.; Hasun, M.; Winkler-Dworak, M.; Finsterer, J. Usefulness of Neuromuscular Co-morbidity, Left Bundle Branch Block, and Atrial Fibrillation to Predict the Long-Term Prognosis of Left Ventricular Hypertrabeculation/Noncompaction. Am. J. Cardiol. 2020, 128, 168–173. [Google Scholar] [CrossRef] [PubMed]
- Aung, N.; Doimo, S.; Ricci, F.; Sanghvi, M.M.; Pedrosa, C.; Woodbridge, S.P.; Al-Balah, A.; Zemrak, F.; Khanji, M.Y.; Munroe, P.B.; et al. Prognostic Significance of Left Ventricular Noncompaction: Systematic Review and Meta-Analysis of Observational Studies. Circ. Cardiovasc. Imaging. 2020, 13, 009712. [Google Scholar] [CrossRef] [PubMed]
- Elliott, P.; Andersson, B.; Arbustini, E.; Bilinska, Z.; Cecchi, F.; Charron, P.; Dubourg, O.; Kuhl, U.; Maisch, B.; McKenna, W.J.; et al. Classification of the cardiomyopathies: A position statement from the European Society Of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur. Heart J. 2008, 29, 270–276. [Google Scholar] [CrossRef] [Green Version]
- Towbin, J.A.; McKenna, W.J.; Abrams, D.J.; Ackerman, M.J.; Calkins, H.; Darrieux, F.C.; Daubert, J.P.; de Chillou, C.; DePasquale, E.C.; Desai, M.Y.; et al. HRS expert consensus statement on evaluation, risk stratification, and management of arrhythmogenic cardiomyopathy. Heart Rhythm. 2019, 16, e301–e372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brugada, P.; Brugada, J.; Mont, L.; Smeets, J.; Andries, E.W. A new approach to the differential diagnosis of a regular tachycardia with a wide QRS complex. Circulation 1991, 83, 1649–1659. [Google Scholar] [CrossRef] [Green Version]
- Vereckei, A. Current algorithms for the diagnosis of wide QRS complex tachycardias. Curr. Cardiol. Rev. 2014, 10, 262–276. [Google Scholar] [CrossRef] [Green Version]
- Kashou, A.H.; Noseworthy, P.A.; DeSimone, C.V.; Deshmukh, A.J.; Asirvatham, S.J.; May, A.M. Wide Complex Tachycardia Dif-ferentiation: A Reappraisal of the State-of-the-Art. J. Am. Heart Assoc. 2020, 9, e016598. [Google Scholar] [CrossRef] [PubMed]
- McGill, T.D.; Kashou, A.H.; Deshmukh, A.J.; LoCoco, S.; May, A.M.; De Simone, C.V. Wide complex tachycardia differentiation: An examination of traditional and contemporary approaches. J. Electrocardiol. 2020, 60, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Padala, S.K.; Sidhu, M.S.; Brown, J.R.; Zipursky, J.S.; Steckman, D.A.; Parikh, D.R.; Greenberg, M.L. Non-sustained wide complex tachycardia: An underappreciated sign to aid in diagnosis. Europace 2016, 18, 1069–1076. [Google Scholar] [CrossRef] [PubMed]
- Riera, A.R.P.; Uchida, A.H.; Ferreira Filho, C.; Meneghini, A.; Ferreira, C.; Schapacknik, E.; Dubner, S.; Moffa, P. Significance of vectorcardiogram in the cardiological diagnosis of the 21st century. Clin. Cardiol. 2007, 30, 319–323. [Google Scholar] [CrossRef] [PubMed]
- Eliot, R.S.; Everhart, F.J.; Sterns, L.P. Loops for the lost. An introductory lesson for vector-electrocardiographic enjoyment (if not proficiency and accuracy). Arch. Intern. Med. 1967, 120, 293–297. [Google Scholar] [CrossRef]
- Talbot, S.; Kilpatrick, D.; Weeks, B. Vectorcardiographic features of ventricular extrasystoles correlated with conventional scalar electrocardiographic interpretation. Heart 1978, 40, 883–890. [Google Scholar] [CrossRef] [PubMed]
- Talbot, S.; Kilpatrick, D.; Weeks, B. Vectorcardiographic analysis of ventricular tachycardia. Cardiovasc. Res. 1980, 14, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Kulbertus, H.E.; De Laval-Rutten, F.; Casters, P. Vectorcardiographic study of aberrant conduction anterior displacement of QRS: Another form of intraventricular block. Br. Heart J. 1976, 38, 549–557. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Brugada Criteria for VT | Vereckei Criteria for VT | ||
|---|---|---|---|
| Chest lead concordance | Not present (very small r waves) | AV dissociation present | Probably absent (P-QRS association at WCT onset and termination, but not all P waves seen) |
| RS interval >100 ms | Absent | Initial R wave in aVR | Absent |
| AV dissociation | Probably absent (P-QRS association at WCT onset and termination, but not all P waves seen) | QRS morphology unlike bundle branch block or fascicular block | Absent |
| VT morphology criteria in V1–V2, V6 | Absent | Vi/Vt ≤ 1 | Absent |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Țentea, C.-P.; Eötvös, C.-A.; Lazar, R.-D.; Zehan, I.-G.; Paștiu, G.; Porca, A.; Jelnean, M.; Pop, S.; Blendea, D. Integrating Electrocardiography and Vectorcardiography in the Differential Diagnosis of Wide Complex Tachycardia in a Patient with Left Ventricular Noncompaction: A Case Report and Brief Literature Review. Diagnostics 2021, 11, 1152. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11071152
Țentea C-P, Eötvös C-A, Lazar R-D, Zehan I-G, Paștiu G, Porca A, Jelnean M, Pop S, Blendea D. Integrating Electrocardiography and Vectorcardiography in the Differential Diagnosis of Wide Complex Tachycardia in a Patient with Left Ventricular Noncompaction: A Case Report and Brief Literature Review. Diagnostics. 2021; 11(7):1152. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11071152
Chicago/Turabian StyleȚentea, Călina-Patricia, Csilla-Andrea Eötvös, Roxana-Daiana Lazar, Iulia-Georgiana Zehan, Giorgia Paștiu, Adriana Porca, Mihaela Jelnean, Sorin Pop, and Dan Blendea. 2021. "Integrating Electrocardiography and Vectorcardiography in the Differential Diagnosis of Wide Complex Tachycardia in a Patient with Left Ventricular Noncompaction: A Case Report and Brief Literature Review" Diagnostics 11, no. 7: 1152. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11071152