
A Nomogram for Predicting Laparoscopic and Endoscopic Cooperative Surgery during the Endoscopic Resection of Subepithelial Tumors of the Upper Gastrointestinal Tract

 and
and
Abstract
:1. Introduction
2. Materials & Methods
2.1. Inclusion Criteria and Exclusion Criteria of the Study Population
2.2. Equipment and Procedure
2.3. Ethical Considerations
2.4. Statistical Analysis
3. Results
3.1. Clinical Features of the Study Population
3.2. Analysis of Complication and Risk Factor Predictive for LECS
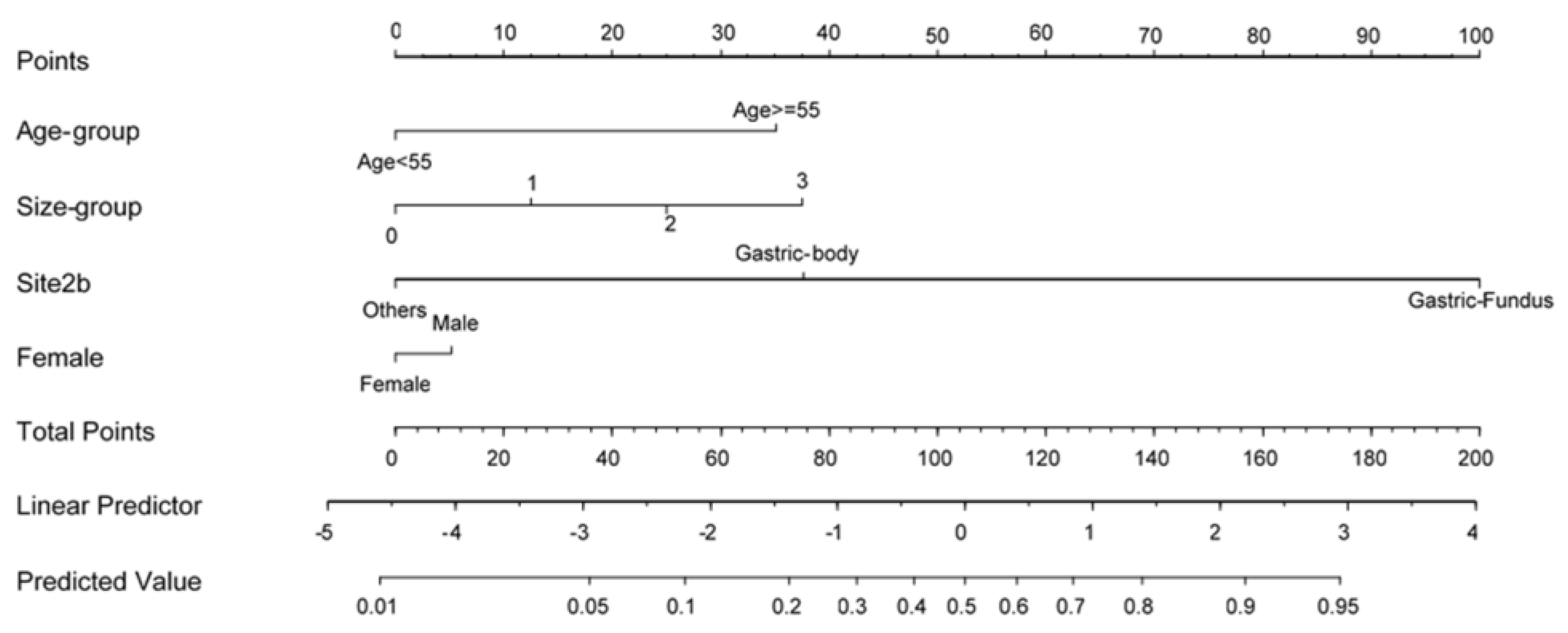
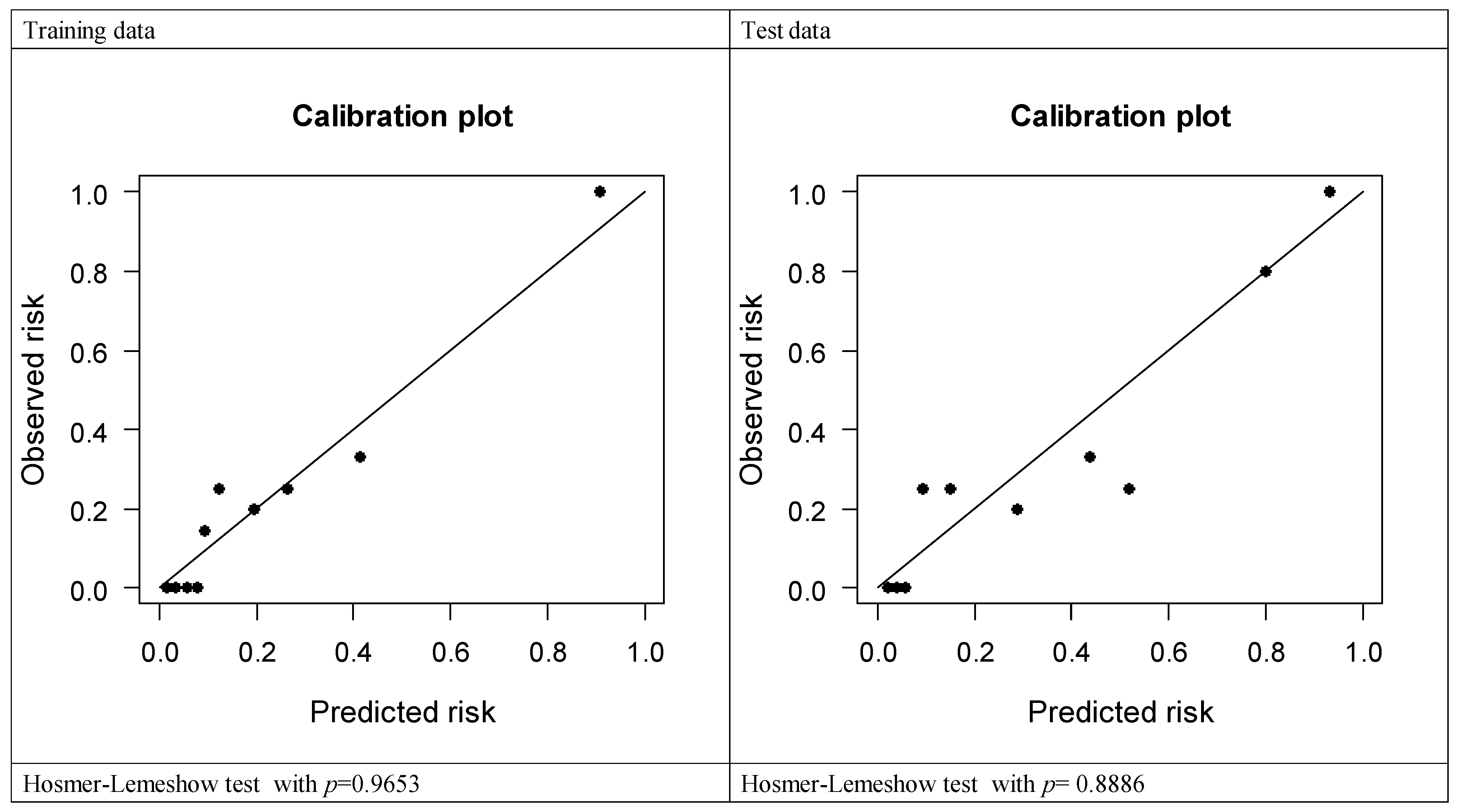
3.3. Development and Validation of the Nomogram
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Hedenbro, J.L.; Ekelund, M.; Wetterberg, P. Endoscopic diagnosis of submucosal gastric lesions. Surg. Endosc. 1991, 5, 20–23. [Google Scholar] [CrossRef]
- Lee, J.H.; Lee, H.L.; Ahn, Y.W.; Lee, K.N.; Jun, D.W.; Lee, O.Y.; Han, D.S.; Yoon, B.C.; Choi, H.S. Prevalence of Gastric Subepithelial Tumors in Korea: A Single Center Experience. Korean J. Gastroenterol. 2015, 66, 274–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hwang, J.H.; Saunders, M.D.; Rulyak, S.J.; Shaw, S.; Nietsch, H.; Kimmey, M.B. A prospective study comparing endoscopy and EUS in the evaluation of GI subepithelial masses. Gastrointest. Endosc. 2005, 62, 202–208. [Google Scholar] [CrossRef]
- Demetri, G.D.; Von Mehren, M.; Antonescu, C.R.; DeMatteo, R.P.; Ganjoo, K.N.; Maki, R.G.; Pisters, P.W.; Raut, C.P.; Riedel, R.F.; Schuetze, S.; et al. NCCN Task Force Report: Update on the Management of Patients with Gastrointestinal Stromal Tumors. J. Natl. Compr. Cancer Netw. 2010, 8, S1–S44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faulx, A.L.; Kothari, S.; Acosta, R.D.; Agrawal, D.; Bruining, D.H.; Chandrasekhara, V.; Eloubeidi, M.A.; Fanelli, R.D.; Gurudu, S.R.; Khashab, M.A.; et al. The role of endoscopy in subepithelial lesions of the GI tract. Gastrointest. Endosc. 2017, 85, 1117–1132. [Google Scholar] [CrossRef] [Green Version]
- Nishida, T.; Goto, O.; Raut, C.P.; Yahagi, N. Diagnostic and treatment strategy for small gastrointestinal stromal tumors. Cancer 2016, 122, 3110–3118. [Google Scholar] [CrossRef] [Green Version]
- Honda, M.; Hiki, N.; Nunobe, S.; Ohashi, M.; Kiyokawa, T.; Sano, T.; Yamaguchi, T. Long-term and surgical outcomes of laparoscopic surgery for gastric gastrointestinal stromal tumors. Surg. Endosc. 2014, 28, 2317–2322. [Google Scholar] [CrossRef]
- Chung, I.-K.; Lee, J.H.; Lee, S.-H.; Kim, S.-J.; Cho, J.Y.; Cho, W.Y.; Hwangbo, Y.; Keum, B.R.; Park, J.J.; Chun, H.-J.; et al. Therapeutic outcomes in 1000 cases of endoscopic submucosal dissection for early gastric neoplasms: Korean ESD Study Group multicenter study. Gastrointest. Endosc. 2009, 69, 1228–1235. [Google Scholar] [CrossRef]
- Białek, A.; Wiechowska-Kozłowska, A.; Pertkiewicz, J.; Polkowski, M.; Milkiewicz, P.; Karpińska, K.; Ławniczak, M.; Starzyńska, T. Endoscopic submucosal dissection for treatment of gastric subepithelial tumors (with video). Gastrointest. Endosc. 2012, 75, 276–286. [Google Scholar] [CrossRef] [PubMed]
- Aslanian, H.R.; Sethi, A.; Bhutani, M.S.; Goodman, A.; Krishnan, K.; Lichtenstein, D.R.; Melson, J.; Navaneethan, U.; Pannala, R.; Parsi, M.A.; et al. ASGE guideline for endoscopic full-thickness resection and submucosal tunnel endoscopic resection. VideoGIE 2019, 4, 343–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kushnir, V.M.; Keswani, R.N.; Hollander, T.G.; Kohlmeier, C.; Mullady, D.K.; Azar, R.R.; Murad, F.M.; Komanduri, S.; Edmundowicz, S.A.; Early, D.S. Compliance with surveillance recommendations for foregut subepithelial tumors is poor: Results of a prospective multicenter study. Gastrointest. Endosc. 2015, 81, 1378–1384. [Google Scholar] [CrossRef]
- Lee, I.-L.; Lin, P.Y.; Tung, S.-Y.; Shen, C.-H.; Wei, K.-L.; Wu, C.-S. Endoscopic submucosal dissection for the treatment of intraluminal gastric subepithelial tumors originating from the muscularis propria layer. Endoscopy 2006, 38, 1024–1028. [Google Scholar] [CrossRef] [PubMed]
- Chu, Y.-Y.; Lien, J.-M.; Tsai, M.-H.; Chiu, C.-T.; Chen, T.-C.; Yang, K.-C.; Ng, S.-C. Modified endoscopic submucosal dissection with enucleation for treatment of gastric subepithelial tumors originating from the muscularis propria layer. BMC Gastroenterol. 2012, 12, 124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, T.-H.; Hsu, C.-M.; Chu, Y.-Y.; Wu, C.-H.; Chen, T.-C.; Hsu, J.-T.; Yeh, T.-S.; Lin, C.-J.; Chiu, C.-T. Association of endoscopic ultrasonographic parameters and gastrointestinal stromal tumors (GISTs): Can endoscopic ultrasonography be used to screen gastric GISTs for potential malignancy? Scand. J. Gastroenterol. 2016, 51, 374–377. [Google Scholar] [CrossRef] [PubMed]
- Agaimy, A. Gastrointestinal stromal tumors (GIST) from risk stratification systems to the new TNM proposal: More questions than answers? A review emphasizing the need for a standardized GIST reporting. Int. J. Clin. Exp. Pathol. 2010, 3, 461–471. [Google Scholar] [PubMed]
- Kim, S.Y.; Shim, K.-N.; Lee, J.-H.; Lim, J.Y.; Kim, T.O.; Choe, A.R.; Tae, C.H.; Jung, H.-K.; Moon, C.M.; Kim, S.-E.; et al. Comparison of the Diagnostic Ability of Endoscopic Ultrasonography and Abdominopelvic Computed Tomography in the Diagnosis of Gastric Subepithelial Tumors. Clin. Endosc. 2019, 52, 565–573. [Google Scholar] [CrossRef] [Green Version]
- Koo, D.-H.; Ryu, M.-H.; Kim, K.-M.; Yang, H.-K.; Sawaki, A.; Hirota, S.; Zheng, J.; Zhang, B.; Tzen, C.-Y.; Yeh, C.-N.; et al. Asian Consensus Guidelines for the Diagnosis and Management of Gastrointestinal Stromal Tumor. Cancer Res. Treat. 2016, 48, 1155–1166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fang, Y.-J.; Cheng, T.-Y.; Sun, M.-S.; Yang, C.-S.; Chen, J.-H.; Liao, W.-C.; Wang, H.-P. Suggested cutoff tumor size for management of small EUS-suspected gastric gastrointestinal stromal tumors. J. Formos. Med. Assoc. 2012, 111, 88–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yen, H.-H.; Wu, P.-Y.; Su, P.-Y.; Yang, C.-W.; Chen, Y.-Y.; Chen, M.-F.; Lin, W.-C.; Tsai, C.-L.; Lin, K.-P. Performance Comparison of the Deep Learning and the Human Endoscopist for Bleeding Peptic Ulcer Disease. J. Med. Biol. Eng. 2021, 41, 504–513. [Google Scholar] [CrossRef]
- Yang, C.-W.; Yen, H.-H.; Chen, Y.-Y.; Soon, M.-S. Use of Dual Knife for Large Pedunculated Colorectal Polyps. Surg. Laparosc. Endosc. Percutaneous Tech. 2014, 24, 444–447. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.-W.; Yen, H.-H.; Chen, Y.-Y.; Soon, M.-S.; Chen, C.-J. Novel Use of the Tip of a Standard Diathermic Snare for Endoscopic Submucosal Dissection of a Large Gastric Adenomatous Polyp. J. Laparoendosc. Adv. Surg. Tech. 2012, 22, 910–912. [Google Scholar] [CrossRef]
- Lee, J.S.; Kim, G.H.; Park, Y.; Yoon, J.M.; Kim, T.W.; Seo, J.H.; Lee, B.E.; Song, G.A. Endoscopic Submucosal Dissection for Gastric Subepithelial Tumors: A Single-Center Experience. Gastroenterol. Res. Pract. 2015, 2015, 425469. [Google Scholar] [CrossRef] [PubMed]
- Du Jeong, I.; Jung, S.W.; Bang, S.-J.; Shin, J.W.; Park, N.H.; Kim, D.H. Endoscopic enucleation for gastric subepithelial tumors originating in the muscularis propria layer. Surg. Endosc. 2010, 25, 468–474. [Google Scholar] [CrossRef] [PubMed]
- Chun, S.Y.; Kim, K.O.; Park, D.S.; Lee, I.J.; Park, J.W.; Moon, S.-H.; Baek, I.H.; Kim, J.H.; Park, C.K.; Kwon, M.J. Endoscopic submucosal dissection as a treatment for gastric subepithelial tumors that originate from the muscularis propria layer: A preliminary analysis of appropriate indications. Surg. Endosc. 2013, 27, 3271–3279. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Wang, F.; Wu, B.; Wang, Q.; Wang, C.; Liu, J. Endoscopic submucosal dissection of gastric fundus subepithelial tumors originating from the muscularis propria. Exp. Ther. Med. 2013, 6, 391–395. [Google Scholar] [CrossRef] [Green Version]
- Catalano, F.; Rodella, L.; Lombardo, F.; Silano, M.; Tomezzoli, A.; Fuini, A.; Di Cosmo, M.A.; de Manzoni, G.; Trecca, A. Endoscopic submucosal dissection in the treatment of gastric submucosal tumors: Results from a retrospective cohort study. Gastric Cancer 2013, 16, 563–570. [Google Scholar] [CrossRef]
- Zhang, Y.; Ye, L.-P.; Zhou, X.-B.; Mao, X.-L.; Zhu, L.-H.; He, B.-L.; Huang, Q. Safety and Efficacy of Endoscopic Excavation for Gastric Subepithelial Tumors Originating From the Muscularis Propria Layer. J. Clin. Gastroenterol. 2013, 47, 689–694. [Google Scholar] [CrossRef]
- Ye, L.-P.; Zhu, L.-H.; Zhou, X.-B.; Mao, X.-L.; Zhang, Y. Endoscopic excavation for the treatment of small esophageal subepithelial tumors originating from the muscularis propria. Hepatogastroenterology 2015, 62, 65–68. [Google Scholar]
- Inoue, H.; Minami, H.; Kobayashi, Y.; Sato, Y.; Kaga, M.; Suzuki, M.; Satodate, H.; Odaka, N.; Itoh, H.; Kudo, S. Peroral endoscopic myotomy (POEM) for esophageal achalasia. Endoscopy 2010, 42, 265–271. [Google Scholar] [CrossRef]
- Inoue, H.; Ikeda, H.; Hosoya, T.; Onimaru, M.; Yoshida, A.; Eleftheriadis, N.; Maselli, R.; Kudo, S. Submucosal endoscopic tumor resection for subepithelial tumors in the esophagus and cardia. Endoscopy 2012, 44, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Xu, M.-D.; Cai, M.-Y.; Zhou, P.-H.; Qin, X.-Y.; Zhong, Y.-S.; Chen, W.-F.; Hu, J.-W.; Zhang, Y.-Q.; Ma, L.-L.; Qin, W.-Z.; et al. Submucosal tunneling endoscopic resection: A new technique for treating upper GI submucosal tumors originating from the muscularis propria layer (with videos). Gastrointest. Endosc. 2012, 75, 195–199. [Google Scholar] [CrossRef] [PubMed]
- Peng, W.; Tan, S.; Huang, S.; Ren, Y.; Li, H.; Peng, Y.; Fu, X.; Tang, X. Efficacy and safety of submucosal tunneling endoscopic resection for upper gastrointestinal submucosal tumors with more than 1-year’ follow-up: A systematic review and meta-analysis. Scand. J. Gastroenterol. 2019, 54, 397–406. [Google Scholar] [CrossRef]
- Schmidt, A.; Bauder, M.; Riecken, B.; Von Renteln, D.; Muehleisen, H.; Caca, K. Endoscopic full-thickness resection of gastric subepithelial tumors: A single-center series. Endoscopy 2014, 47, 154–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarker, S.; Gutierrez, J.P.; Council, L.; Brazelton, J.D.; Baig, K.R.K.K.; Mönkemüller, K. Over-the-scope clip-assisted method for resection of full-thickness submucosal lesions of the gastrointestinal tract. Endoscopy 2014, 46, 758–761. [Google Scholar] [CrossRef] [PubMed]
- Azzolini, F.; Cecinato, P.; Iori, V.; De Marco, L.; Sassatelli, R. Endoscopic full-thickness resection for suspected residual rectal neuroendocrine tumor and closure of the defect with a new suturing system. Endoscopy 2015, 47, E556–E557. [Google Scholar] [CrossRef] [Green Version]
- Hiki, N.; Yamamoto, Y.; Fukunaga, T.; Yamaguchi, T.; Nunobe, S.; Tokunaga, M.; Miki, A.; Ohyama, S.; Seto, Y. Laparoscopic and endoscopic cooperative surgery for gastrointestinal stromal tumor dissection. Surg. Endosc. 2008, 22, 1729–1735. [Google Scholar] [CrossRef] [PubMed]
- Hoteya, S.; Haruta, S.; Shinohara, H.; Yamada, A.; Furuhata, T.; Yamashita, S.; Kikuchi, D.; Mitani, T.; Ogawa, O.; Matsui, A.; et al. Feasibility and safety of laparoscopic and endoscopic cooperative surgery for gastric submucosal tumors, including esophagogastric junction tumors. Dig. Endosc. 2014, 26, 538–544. [Google Scholar] [CrossRef]
- Aoyama, J.; Kawakubo, H.; Matsuda, S.; Mayanagi, S.; Fukuda, K.; Irino, T.; Nakamura, R.; Wada, N.; Kitagawa, Y. Clinical outcomes of laparoscopic and endoscopic cooperative surgery for submucosal tumors on the esophagogastric junction: A retrospective single-center analysis. Gastric Cancer 2020, 23, 1084–1090. [Google Scholar] [CrossRef]
- Yen, H.H.; Su, P.Y.; Huang, S.P.; Wu, L.; Hsu, T.C.; Zeng, Y.H.; Chen, Y.Y. Evaluation of non-alcoholic fatty liver disease in patients with inflammatory bowel disease using controlled attenuation parameter technology: A Taiwanese retrospective cohort study. PLoS ONE 2021, 16, e0252286. [Google Scholar] [CrossRef]
- Chang, Y.-Y.; Li, P.-C.; Chang, R.-F.; Yao, C.-D.; Chen, Y.-Y.; Chang, W.-Y.; Yen, H.-H. Deep learning-based endoscopic anatomy classification: An accelerated approach for data preparation and model validation. Surg. Endoscopy 2021. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Number | |
|---|---|---|
| Median age, years (Median, IQR) | 55 (48–60.75) | |
| Sex, n (%) | ||
| Male | 61 (49.6%) | |
| Female | 62 (50.4%) | |
| Hospital day, days (Median, IQR) | 6 (5–8) | |
| Procedure time, minutes (Median, IQR) | 60 (30–90) | |
| Tumor location | ||
| Esophagus | 30 | |
| Gastric fundus | 21 | |
| Gastric cardia | 21 | |
| Gastric body | 35 | |
| Gastric antrum | 14 | |
| Duodenum | 2 | |
| Tumor size, cm (Median, IQR) | 1.5 (1–2.5) | |
| Layer of tumor origin, n (%) | ||
| Submucosa | 38 (30.9%) | |
| Muscularis propria | 85 (69.1%) | |
| Complications, n (%) | ||
| Perforation | 47 (38.2%) | |
| Perforation with laparoscopic cooperative surgery | 30 (24.4%) | |
| Delayed perforation | 1 (0.8%) | |
| Delayed bleeding | 1 (0.8%) | |
| Pathology report, n (%) | ||
| Leiomyoma | 56 (45.5%) | |
| GIST | 42 (34.1%) | |
| Aberrant pancreas | 8 (6.5%) | |
| Neuroendocrine tumor | 3 (2.4%) | |
| Others * | 14 (11.4%) | |
| En bloc resection rate | 114 (92.7%) | |
| Follow-up days, day (Median, IQR) | 242 (69–774) | |
| Esophagus | Gastric Fundus | Gastric Cardia | Gastric Body | Gastric Antrum | DuodenuSm | |
|---|---|---|---|---|---|---|
| GIST | 1 | 17 | 7 | 14 | 3 | 0 |
| Leiomyoma | 25 | 2 | 13 | 16 | 0 | 0 |
| Aberrant pancreas | 0 | 0 | 0 | 1 | 6 | 1 |
| Neuroendocrine tumor | 0 | 0 | 0 | 2 | 0 | 1 |
| Others | 4 | 2 | 1 | 2 | 5 | 0 |
| Without LECS | With LECS | p-Value | |
|---|---|---|---|
| Sex (M/F) | 47/46 | 14/16 | 0.7134 |
| Age, year (mean, SD) | 51.79 (13.09) | 58.16 (11.06) | 0.0018 |
| Size, cm (mean, SD) | 1.61 (0.89) | 2.20 (1.10) | 0.0003 |
| Site (E/Antrum/Body/Cardia/Fundus/D) | 30/13/26/17/5/2 | 0/1/9/4/16/0 | <0.0001 |
| Pathology (GIST/Leiomyoma/Others) | 22/49/22 | 20/7/3 | 0.0001 |
| Resection method (ESD/STER) | 78/15 | 29/1 | 0.0712 |
| Univariable Analysis | Multivariable Analysis | |||||
|---|---|---|---|---|---|---|
| cOR (95% CI) | p-value | AUC | Coef. | adj. OR (95% CI) | p-value | |
| Site | 0.820 | |||||
| Others | 1 | 1 | ||||
| Gastric body | 3.57 (0.68, 18.65) | 0.132 | 1.60 | 4.95 (0.78, 31.62) | 0.091 | |
| Gastric fundus | 100.8 (6.36, 1598.31) | 0.001 | 4.25 | 70.32 (3.74, 1320.99) | 0.005 | |
| Size (per 1 unit increase) | 1.84 (0.94, 3.60) | 0.076 | 0.658 | 0.53 | 1.70 (0.68, 4.27) | 0.257 |
| Age ≥ 55 | 3.91 (0.82, 18.56) | 0.086 | 0.653 | 1.49 | 4.45 (0.61, 32.22) | 0.140 |
| Female | 1.14 (0.31, 4.17) | 0.845 | 0.517 | −0.22 | 0.80 (0.15, 4.35) | 0.800 |
| Training Data | Validation Data | Test Data | p-Value | |
|---|---|---|---|---|
| Sample size | 54 | 28 | 41 | |
| Age, years | 54.89 ± 10.55 | 50.07 ± 12.57 | 53.56 ± 15.51 | 0.275 |
| <55 | 23 (42.59%) | 16 (57.14%) | 20 (48.78%) | 0.454 |
| ≥55 | 31 (57.41%) | 12 (42.86%) | 21 (51.22%) | |
| Sex | ||||
| Female | 28 (51.85%) | 15 (53.57%) | 19 (46.34%) | 0.807 |
| Male | 26 (48.15%) | 13 (46.43%) | 22 (53.66%) | |
| Site | ||||
| Gastric fundus | 5 (9.26%) | 3 (10.71%) | 13 (31.71%) | 0.041 |
| Gastric body | 18 (33.33%) | 7 (25%) | 10 (24.39%) | |
| Others | 31 (57.41%) | 18 (64.29%) | 18 (43.9%) | |
| Size, cm | 1.87 ± 1.04 | 1.67 ± 0.94 | 1.66 ± 0.92 | 0.516 |
| <1 | 10 (18.52%) | 6 (21.43%) | 10 (24.39%) | 0.811 |
| ≥1 to <2 | 23 (42.59%) | 14 (50%) | 18 (43.9%) | |
| ≥2 to <3 | 10 (18.52%) | 5 (17.86%) | 9 (21.95%) | |
| 3 | 11 (20.37%) | 3 (10.71%) | 4 (9.76%) | |
| LCES | ||||
| No | 43 (79.63%) | 21 (75%) | 29 (70.73%) | 0.604 |
| Yes | 11 (20.37%) | 7 (25%) | 12(29.27%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsiao, S.-W.; Chen, M.-W.; Yang, C.-W.; Lin, K.-H.; Chen, Y.-Y.; Kor, C.-T.; Huang, S.-P.; Yen, H.-H. A Nomogram for Predicting Laparoscopic and Endoscopic Cooperative Surgery during the Endoscopic Resection of Subepithelial Tumors of the Upper Gastrointestinal Tract. Diagnostics 2021, 11, 2160. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11112160
Hsiao S-W, Chen M-W, Yang C-W, Lin K-H, Chen Y-Y, Kor C-T, Huang S-P, Yen H-H. A Nomogram for Predicting Laparoscopic and Endoscopic Cooperative Surgery during the Endoscopic Resection of Subepithelial Tumors of the Upper Gastrointestinal Tract. Diagnostics. 2021; 11(11):2160. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11112160
Chicago/Turabian StyleHsiao, Shun-Wen, Mei-Wen Chen, Chia-Wei Yang, Kuo-Hua Lin, Yang-Yuan Chen, Chew-Teng Kor, Siou-Ping Huang, and Hsu-Heng Yen. 2021. "A Nomogram for Predicting Laparoscopic and Endoscopic Cooperative Surgery during the Endoscopic Resection of Subepithelial Tumors of the Upper Gastrointestinal Tract" Diagnostics 11, no. 11: 2160. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics11112160