Diet-Induced Rat Model of Gradual Development of Non-Alcoholic Fatty Liver Disease (NAFLD) with Lipopolysaccharides (LPS) Secretion

 ,
,  , , , , ,
, , , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Histological Evaluation
2.3. Biochemical Measurements
2.4. Statistical Analysis
3. Results
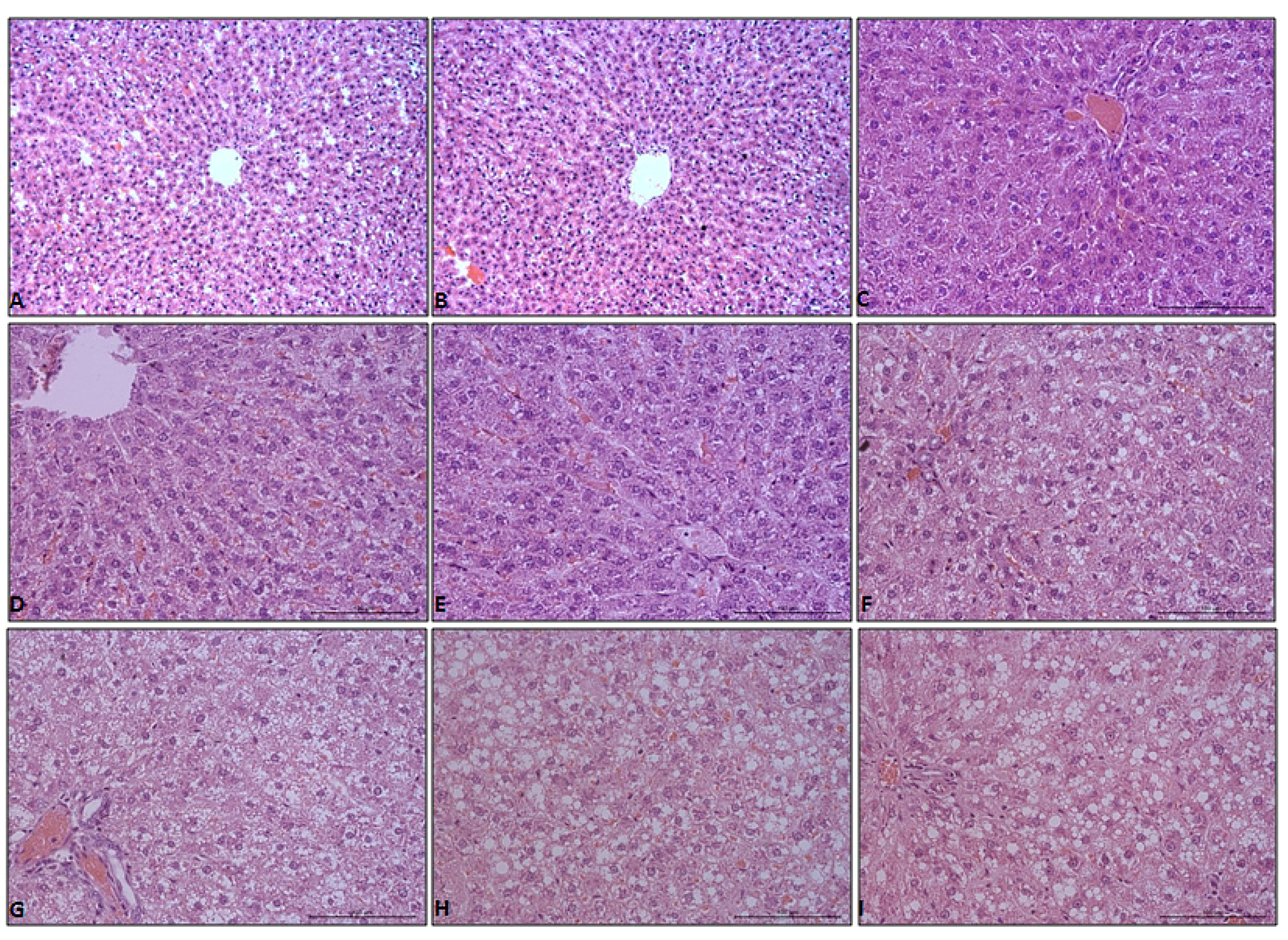
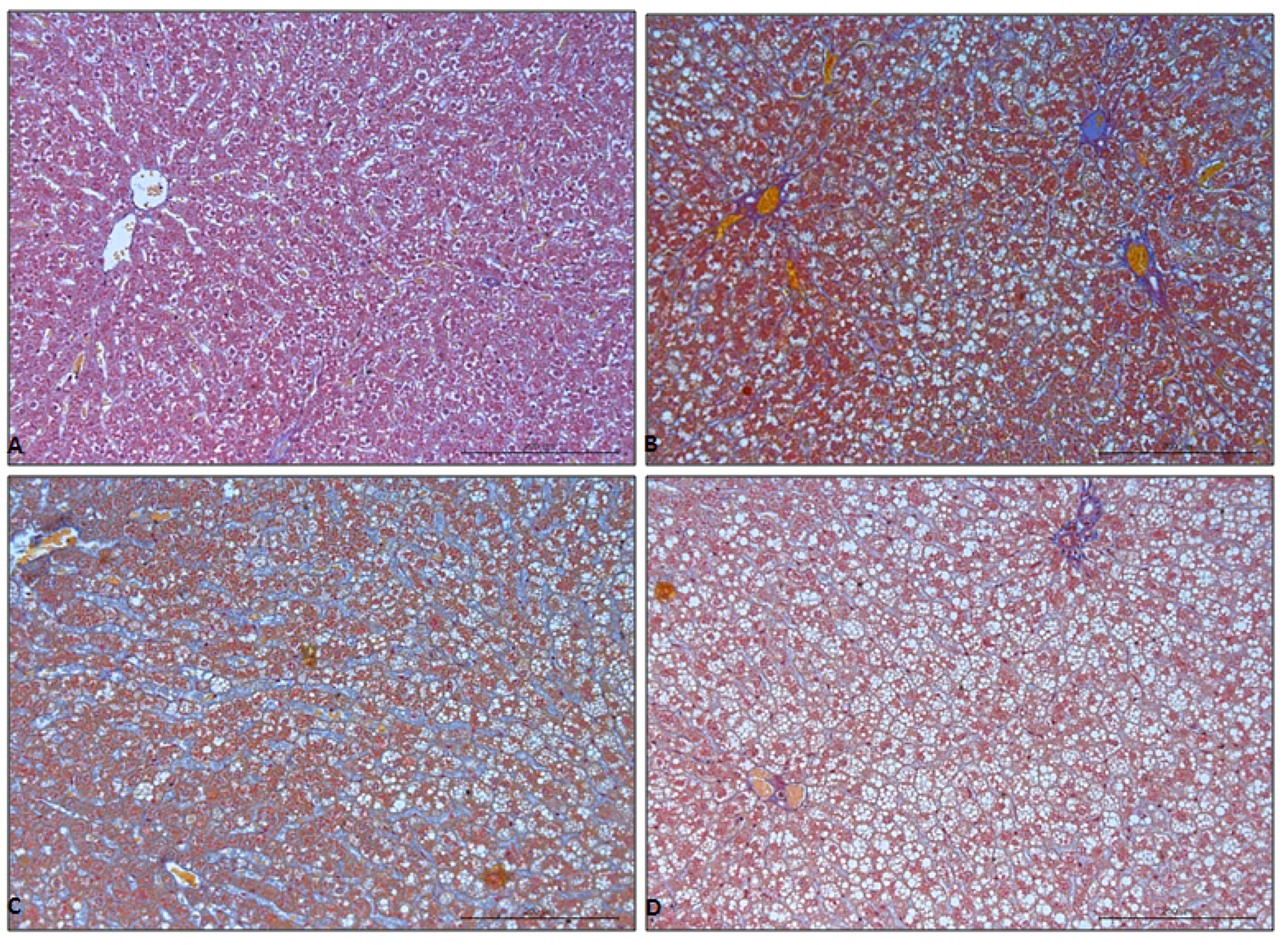
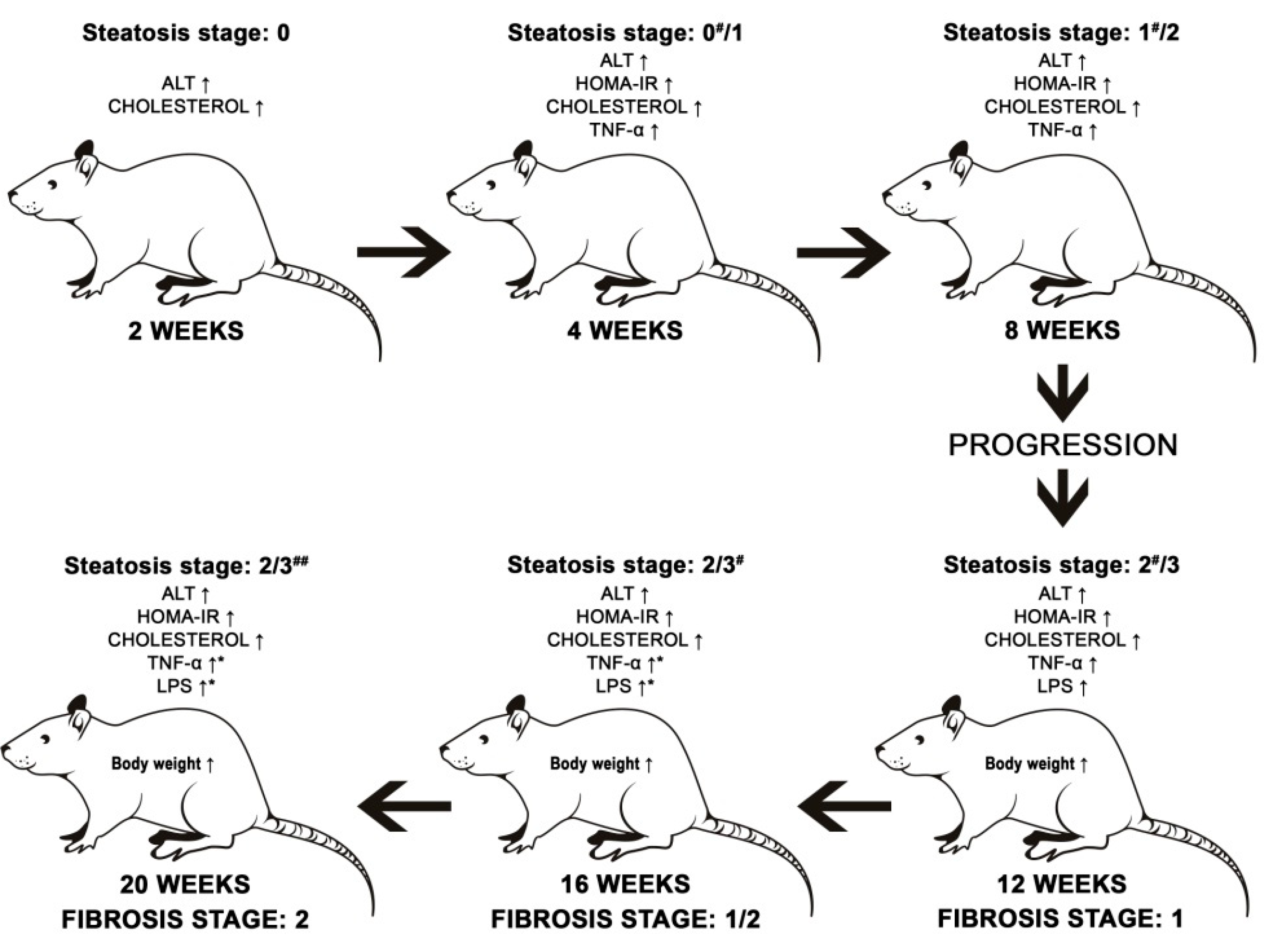
Hepatic Steatosis, Inflammation, and Fibrosis
4. Discussion
4.1. Selection of an Appropriate High Fat Dietary Model of NAFLD
4.2. Exposure for the HFHCh Diet
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Sherif, Z.A.; Saeed, A.; Ghavimi, S.; Nouraie, S.-M.; Laiyemo, A.O.; Brim, H.; Ashktorab, H. Global Epidemiology of Non-Alcoholic Fatty Liver Disease and Perspectives on US Minority Populations. Dig. Dis. Sci. 2016, 61, 1214–1225. [Google Scholar] [CrossRef] [PubMed]
- Vernon, G.; Baranova, A.; Younossi, Z.M. Systematic review: The epidemiology and natural history of non-alcoholic fatty liver disease and non-alcoholic steatohepatitis in adults. Aliment. Pharmacol. Ther. 2011, 34, 274–285. [Google Scholar] [CrossRef] [PubMed]
- Cioboata, R.; Gaman, A.; Trasca, D.; Ungureanu, A.; Docea, A.O.; Tomescu, P.; Gherghina, F.; Arsene, A.L.; Badiu, C.; Tsatsakis, A.M.; et al. Pharmacological management of non-alcoholic fatty liver disease: Atorvastatin versus pentoxifylline. Exp. Ther. Med. 2017, 13, 2375–2381. [Google Scholar] [CrossRef] [PubMed]
- Cobbina, E.; Akhlaghi, F. Non-alcoholic fatty liver disease (NAFLD)—Pathogenesis, classification, and effect on drug metabolizing enzymes and transporters. Drug Metab. Rev. 2017, 49, 197–211. [Google Scholar] [CrossRef] [PubMed]
- Engin, A. Non-Alcoholic Fatty Liver Disease. Adv. Exp. Med. Biol. 2017, 960, 443–467. [Google Scholar] [CrossRef]
- Buzzetti, E.; Pinzani, M.; Tsochatzis, E.A. The multiple-hit pathogenesis of non-alcoholic fatty liver disease (NAFLD). Metabolism 2016, 65, 1038–1048. [Google Scholar] [CrossRef]
- Bellentani, S. The epidemiology of non-alcoholic fatty liver disease. Liver Int. Off. J. Int. Assoc. Study Liver 2017, 37 (Suppl. 1), 81–84. [Google Scholar] [CrossRef]
- Petrakis, D.; Vassilopoulou, L.; Mamoulakis, C.; Psycharakis, C.; Anifantaki, A.; Sifakis, S.; Docea, A.O.; Tsiaoussis, J.; Makrigiannakis, A.; Tsatsakis, A.M. Endocrine Disruptors Leading to Obesity and Related Diseases. Int. J. Environ. Res. Public Health 2017, 14, 1282. [Google Scholar] [CrossRef]
- Hu, M.; Phan, F.; Bourron, O.; Ferré, P.; Foufelle, F. Steatosis and NASH in type 2 diabetes. Biochimie 2017, 143, 37–41. [Google Scholar] [CrossRef]
- Nakajima, T.; Naito, H. Mechanism Analysis and Prevention of Pathogenesis of Nonalcoholic Steatohepatitis. Nihon Eiseigaku Zasshi Jpn. J. Hyg. 2015, 70, 197–204. [Google Scholar] [CrossRef]
- Caligiuri, A.; Gentilini, A.; Marra, F. Molecular Pathogenesis of NASH. Int. J. Mol. Sci. 2016, 17, 1575. [Google Scholar] [CrossRef] [PubMed]
- Starley, B.Q.; Calcagno, C.J.; Harrison, S.A. Nonalcoholic fatty liver disease and hepatocellular carcinoma: A weighty connection. Hepatology 2010, 51, 1820–1832. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.-J.; Fan, J.-G.; Ding, X.-D.; Qiao, L.; Wang, G.-L. Characterization of high-fat, diet-induced, non-alcoholic steatohepatitis with fibrosis in rats. Dig. Dis. Sci. 2010, 5, 931–940. [Google Scholar] [CrossRef] [PubMed]
- Kleiner, D.E.; Brunt, E.M.; Van Natta, M.; Behling, C.; Contos, M.J.; Cummings, O.W.; Ferrell, L.D.; Liu, Y.-C.; Torbenson, M.S.; Unalp-Arida, A.; et al. Nonalcoholic Steatohepatitis Clinical Research Network. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology 2005, 41, 1313–1321. [Google Scholar] [CrossRef]
- Statistics with Confidence: Confidence Intervals and Statistical Guidelines, 2nd ed.; Wiley, 2000; Available online: https://0-www-wiley-com.brum.beds.ac.uk/en-us/Statistics+with+Confidence%3A+Confidence+Intervals+and+Statistical+Guidelines%2C+2nd+Edition-p-9780727913753 (accessed on 21 January 2019).
- Takahashi, Y.; Soejima, Y.; Fukusato, T. Animal models of nonalcoholic fatty liver disease/nonalcoholic steatohepatitis. World J. Gastroenterol. 2012, 18, 2300–2308. [Google Scholar] [CrossRef]
- Larter, C.Z.; Yeh, M.M. Animal models of NASH: Getting both pathology and metabolic context right. J. Gastroenterol. Hepatol. 2008, 23, 1635–1648. [Google Scholar] [CrossRef]
- Romestaing, C.; Piquet, M.-A.; Bedu, E.; Rouleau, V.; Dautresme, M.; Hourmand-Ollivier, I.; Filippi, C.; Duchamp, C.; Sibille, B. Long term highly saturated fat diet does not induce NASH in Wistar rats. Nutr. Metab. 2007, 4, 4. [Google Scholar] [CrossRef]
- Savard, C.; Tartaglione, E.V.; Kuver, R.; Haigh, W.G.; Farrell, G.C.; Subramanian, S.; Chait, A.; Yeh, M.M.; Quinn, L.S.; Ioannou, G.N. Synergistic interaction of dietary cholesterol and dietary fat in inducing experimental steatohepatitis. Hepatology 2013, 57, 81–92. [Google Scholar] [CrossRef]
- Kitamori, K.; Naito, H.; Tamada, H.; Kobayashi, M.; Miyazawa, D.; Yasui, Y.; Sonoda, K.; Tsuchikura, S.; Yasui, N.; Ikeda, K.; et al. Development of novel rat model for high-fat and high-cholesterol diet-induced steatohepatitis and severe fibrosis progression in SHRSP5/Dmcr. Environ. Health Prev. Med. 2012, 17, 173–182. [Google Scholar] [CrossRef]
- Tirosh, O. Hypoxic Signaling and Cholesterol Lipotoxicity in Fatty Liver Disease Progression. Oxidative Med. Cell. Longev. 2018, 2018, 2548154. [Google Scholar] [CrossRef]
- Brotherton, C.S.; Taylor, A.G.; Bourguignon, C.; Anderson, J.G. A High Fiber Diet May Improve Bowel Function and Health-Related Quality of Life in Patients with Crohn’s Disease. Gastroenterol. Nurs. Off. J. Soc. Gastroenterol. Nurses Assoc. 2014, 37, 206–216. [Google Scholar] [CrossRef] [PubMed]
- Roychowdhury, S.; Selvakumar, P.C.; Cresci, G.A.M. The Role of the Gut Microbiome in Nonalcoholic Fatty Liver Disease. Med. Sci. 2018, 6, 47. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, C.P.; de Lima Sanches, P.; de Abreu-Silva, E.O.; Marcadenti, A. Nutrition and Physical Activity in Nonalcoholic Fatty Liver Disease. J. Diabetes Res. 2016, 2016, 4597246. [Google Scholar] [CrossRef] [PubMed]
- Marshall, J.C.; Walker, P.M.; Foster, D.M.; Harris, D.; Ribeiro, M.; Paice, J.; Romaschin, A.D.; Derzko, A.N. Measurement of endotoxin activity in critically ill patients using whole blood neutrophil dependent chemiluminescence. Crit. Care 2002, 6, 342–348. [Google Scholar] [CrossRef]
- Guo, S.; Al-Sadi, R.; Said, H.M.; Ma, T.Y. Lipopolysaccharide Causes an Increase in Intestinal Tight Junction Permeability In Vitro and In Vivo by Inducing Enterocyte Membrane Expression and Localization of TLR-4 and CD14. Am. J. Pathol. 2013, 182, 375–387. [Google Scholar] [CrossRef]
- Fukunishi, S.; Sujishi, T.; Takeshita, A.; Ohama, H.; Tsuchimoto, Y.; Asai, A.; Tsuda, Y.; Higuchi, K. Lipopolysaccharides accelerate hepatic steatosis in the development of nonalcoholic fatty liver disease in Zucker rats. J. Clin. Biochem. Nutr. 2014, 54, 39–44. [Google Scholar] [CrossRef]
- Aagaard-Tillery, K.M.; Grove, K.; Bishop, J.; Ke, X.; Fu, Q.; McKnight, R.; Lane, R.H. Developmental origins of disease and determinants of chromatin structure: Maternal diet modifies the primate fetal epigenome. J. Mol. Endocrinol. 2008, 41, 91–102. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Component | HFHCh | Control |
|---|---|---|
| Carbohydrates [%E] | 50 | 65 |
| Fat [%E] | 30 | 10 |
| Protein [%E] | 20 | 25 |
| Fiber [%] | 3.5 | 3.5 |
| Cholesterol [g/100g] | 2 | 0 |
| Methionine [g/100g] | 0.65 | 0.65 |
| Choline [g/100g] | 0.2 | 0.2 |
| Group | Week | N (n) | Histological Grades of Steatosis Number of Evaluated Histological Fields (Percentage of Grade of Steatosis) | Fibrosis Stage (N) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | 0 | 1 | 2 | 3 | 4 | |||
| Control | 2–20 | 36 (360) | 360 (100) | 0 (0) | 0 (0) | 0 (0) | 36 | 0 | 0 | 0 | 0 |
| HFHCh | 2 | 6 (60) | 360 (100) | 0 (0) | 0 (0) | 0 (0) | 6 | 0 | 0 | 0 | 0 |
| 4 | 6 (60) | 45 (75) *,a | 15 (25) *,a | 0 (0) | 0 (0) | 6 | 0 | 0 | 0 | 0 | |
| 8 | 6 (60) | 0 (0) *,a,b | 47 (78.3) *,a,b | 13 (21.7) *,a,b | 0 (0) | 6 | 0 | 0 | 0 | 0 | |
| 12 | 6 (60) | 0 (0) *,a,b | 0 (0) b,c | 38 (63.33) *,a,b,c | 22 (36.67) *,a,b,c | 1 | 4 | 1 | 0 | 0 | |
| 16 | 6 (60) | 0 (0) *,a,b | 0 (0) b,c | 26 (43.33) *,a,b,c,d | 34 (56.67) *,a,b,c,d | 1 | 3 | 2 | 0 | 0 | |
| 20 | 6 (60) | 0 (0) *,a,b | 0 (0) b,c | 15 (25) *,b,d,e | 45 (75) *,a,b,c,d,e | 1 | 1 | 4 | 0 | 0 | |
| Group | Week | N (n) | Inflammation ScoreNumber of Evaluated Histological Fields (Percentage of Grade of Inflammation) | |||
|---|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | |||
| Control | 2–20 | 36 (360) | 360 (100) | 0 (0) | 0 (0) | 0 (0) |
| HFD | 2 | 6 (60) | 360 (100) | 0 (0) | 0 (0) | 0 (0) |
| 4 | 6 (60) | 48 (80) ** | 12 (20) ** | 0 (0) | 0 (0) | |
| 8 | 6 (60) | 41 (68.33) ***,a | 18 (30) ***,a | 1 (1,67) | 0 (0) | |
| 12 | 6 (60) | 38 (63.33) ***,a,f | 18 (30) ***,a | 4 (6.67) *,c,f | 0 (0) | |
| 16 | 6 (60) | 28 (46.66) ***,a,d,h | 25 (41.67) ***,a,f | 7 (11.67) **,b,e,h | 0 (0) | |
| 20 | 6 (60) | 26 (43.34) ***,a,d,g,i | 26 (43.33) ***,a,e | 8 (11.33) **,b,e,h | 0 (0) | |
| Time Points | Weight [g] | ALT [U/L] | HOMA-IR | |||
| CONTROL | HFHCh | CONTROL | HFHCh | CONTROL | HFHCh | |
| 2 weeks | 401.66 ± 10.57 | 400 ± 14.14 | 18.8 * ± 0.06 | 26.6 * ± 0.73 | 0.69 ± 0.25 | 1.02 5,6 ± 0.46 |
| 4 weeks | 380.83 ± 17.89 | 424.16 ± 32.07 | 19.4 * ± 0.09 | 24.8 * ± 0.18 | 0.95 * ± 0.31 | 1.30 * ± 0.41 |
| 8 weeks | 408.33 ± 10.67 | 420.83 ± 16.69 | 18.2 * ± 0.04 | 23.6 * ± 0.26 | 0.48 * ± 0.10 | 1.48 * ± 0.53 |
| 12 weeks | 420.00 * ± 12.90 | 463.33 *1,2,3 ± 11.05 | 19.0 * ± 0.05 | 22.7 * ± 0.29 | 0.73 * ± 0.215 | 1.30 * ± 0.70 |
| 16 weeks | 418.33 * ± 13.44 | 477.50 *1,2,3 ± 19.09 | 18.4 * ± 0.07 | 30.4 * ± 0.57 | 0.66 * ± 0.32 | 1.71 * ± 0.48 |
| 20 weeks | 420.00 * ± 16.33 | 496.67 *1,2,3 ± 17.95 | 18.3 * ± 0.92 | 27.9 * ± 0.49 | 0.69 * ± 0.38 | 2.07 * ± 0.72 |
| Time Points | CHOLESTEROL [mg/dL] | TNF-α [pg/mL] | LPS [ng/mL] | |||
| CONTROL | HFHCh | CONTROL | HFHCh | CONTROL | HFHCh | |
| 2 weeks | 60.47 * ± 17.65 | 101.24 *,5,6 ± 19.77 | 122.34 ± 9.49 | 149.51 5,6 ± 17.62 | 1.47 ± 1.88 | 2.62 5,6 ± 2.59 |
| 4 weeks | 64.77 * ± 6.07 | 111.31 *,5,6 ± 14.66 | 118.6 * ± 6.19 | 142.53 5,6 * ± 20.57 | 2.17 ± 1.61 | 2.57 5,6 ± 2.00 |
| 8 weeks | 46.13 * ± 22.79 | 112.38 *,5,6 ± 16.54 | 124.30 * ± 7.12 | 136.74 *,5,6 ± 10.41 | 1.48 ± 1.84 | 2.71 5,6 ± 0.98 |
| 12 weeks | 49.10 * ± 12.41 | 121.52 *,5,6 ± 19.77 | 125.41 * ± 13.26 | 141.11 *,5,6 ±16.51 | 2.03 * ± 2.84 | 3.37 *6 ± 3.32 |
| 16 weeks | 68.48 * ± 15.60 | 185.79 *,1,2,3,4 ± 29.92 | 124.14 * ± 17.40 | 165.34 *,1,2,3,4,6 ± 16.12 | 1.77 * ± 1.47 | 3.97 *,1,2,3,6 ± 2.17 |
| 20 weeks | 72.63 * ± 11.66 | 203.16 *,1,2,3,4 ± 64.42 | 129.13 * ± 18.12 | 241.58 *,1,2,3,4,5 ± 98.49 | 2.33 * ± 1.91 | 8.82 *,1,2,3,4,5,6 ± 3.25 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maciejewska, D.; Łukomska, A.; Dec, K.; Skonieczna-Żydecka, K.; Gutowska, I.; Skórka-Majewicz, M.; Styburski, D.; Misiakiewicz-Has, K.; Pilutin, A.; Palma, J.; et al. Diet-Induced Rat Model of Gradual Development of Non-Alcoholic Fatty Liver Disease (NAFLD) with Lipopolysaccharides (LPS) Secretion. Diagnostics 2019, 9, 205. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics9040205
Maciejewska D, Łukomska A, Dec K, Skonieczna-Żydecka K, Gutowska I, Skórka-Majewicz M, Styburski D, Misiakiewicz-Has K, Pilutin A, Palma J, et al. Diet-Induced Rat Model of Gradual Development of Non-Alcoholic Fatty Liver Disease (NAFLD) with Lipopolysaccharides (LPS) Secretion. Diagnostics. 2019; 9(4):205. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics9040205
Chicago/Turabian StyleMaciejewska, Dominika, Agnieszka Łukomska, Karolina Dec, Karolina Skonieczna-Żydecka, Izabela Gutowska, Marta Skórka-Majewicz, Daniel Styburski, Kamila Misiakiewicz-Has, Anna Pilutin, Joanna Palma, and et al. 2019. "Diet-Induced Rat Model of Gradual Development of Non-Alcoholic Fatty Liver Disease (NAFLD) with Lipopolysaccharides (LPS) Secretion" Diagnostics 9, no. 4: 205. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics9040205