
Early Adoption of Checkpoint Inhibitors in Patients with Metastatic Gastric Adenocarcinoma—A Case Series of Non-Operative Long-Term Survivors


Abstract
:1. Introduction
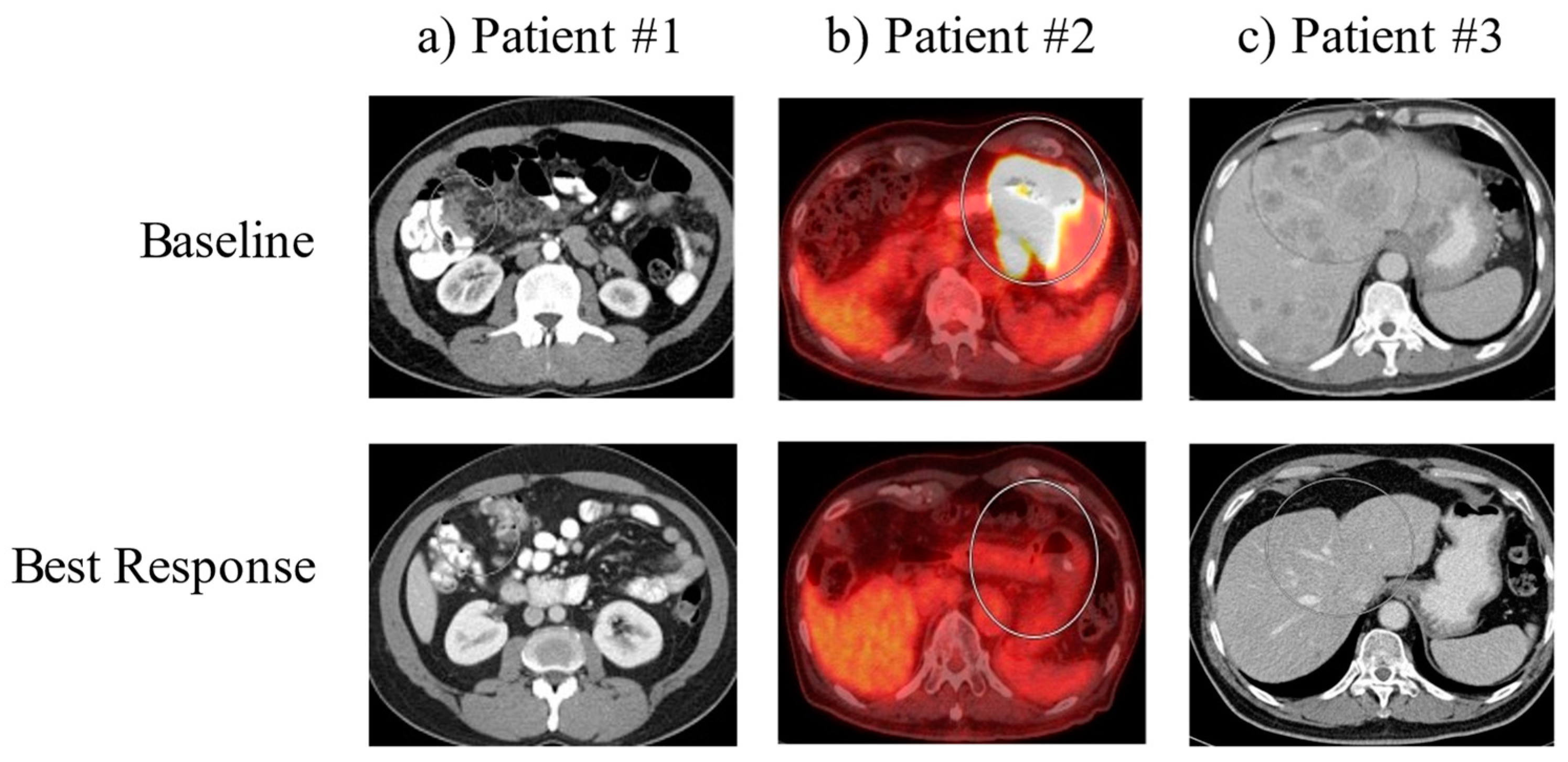
2. Case Series
2.1. Case 1
2.2. Case 2
2.3. Case 3
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Kyi, C.; A Postow, M. Immune checkpoint inhibitor combinations in solid tumors: Opportunities and challenges. Immunother. 2016, 8, 821–837. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janjigian, Y.Y.; Bang, Y.-J.; Fuchs, C.S.; Qin, S.; Satoh, T.; Shitara, K.; Tabernero, J.; Van Cutsem, E.; Cao, Z.A.; Chen, X.; et al. KEYNOTE-811 pembrolizumab plus trastuzumab and chemotherapy for HER2+ metastatic gastric or gastroesophageal junction cancer (mG/GEJC): A double-blind, randomized, placebo-controlled phase 3 study. J. Clin. Oncol. 2019, 37, TPS4146. [Google Scholar] [CrossRef]
- Janjigian, Y.Y.; Shitara, K.; Moehler, M.; Garrido, M.; Salman, P.; Shen, L.; Wyrwicz, L.; Yamaguchi, K.; Skoczylas, T.; Bragagnoli, A.C.; et al. First-line nivolumab plus chemotherapy versus chemotherapy alone for advanced gastric, gastro-oesophageal junction, and oesophageal adenocarcinoma (CheckMate 649): A randomised, open-label, phase 3 trial. Lancet 2021, 398, 27–40. [Google Scholar] [CrossRef]
- Fuchs, C.S.; Doi, T.; Jang, R.W.; Muro, K.; Satoh, T.; Machado, M.; Sun, W.; Jalal, S.I.; Shah, M.A.; Metges, J.-P.; et al. Safety and Efficacy of Pembrolizumab Monotherapy in Patients With Previously Treated Advanced Gastric and Gastroesophageal Junction Cancer. JAMA Oncol. 2018, 4, e180013. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.-T.; Satoh, T.; Ryu, M.-H.; Chao, Y.; Kato, K.; Chung, H.C.; Chen, J.-S.; Muro, K.; Kang, W.K.; Yeh, K.-H.; et al. A phase 3 study of nivolumab in previously treated advanced gastric or gastroesophageal junction cancer (ATTRACTION-2): 2-year update data. Gastric Cancer 2020, 23, 510–519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shitara, K.; Özgüroglu, M.; Bang, Y.-J.; Di Bartolomeo, M.; Mandalà, M.; Ryu, M.-H.; Fornaro, L.; Olesinski, T.; Caglevic, C.; Chung, H.; et al. Pembrolizumab versus paclitaxel for previously treated, advanced gastric or gastro-oesophageal junction cancer (KEYNOTE-061): A randomised, open-label, controlled, phase 3 trial. Lancet 2018, 392, 123–133. [Google Scholar] [CrossRef]
- Kang, Y.-K.; Chen, L.-T.; Ryu, M.-H.; Oh, D.-Y.; Oh, S.C.; Chung, H.C.; Lee, K.-W.; Omori, T.; Shitara, K.; Sakuramoto, S.; et al. Nivolumab plus chemotherapy versus placebo plus chemotherapy in patients with HER2-negative, untreated, unresectable advanced or recurrent gastric or gastro-oesophageal junction cancer (ATTRACTION-4): A randomised, multicentre, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2022, 23, 234–247. [Google Scholar] [CrossRef]
- Shitara, K.; Van Cutsem, E.; Bang, Y.-J.; Fuchs, C.; Wyrwicz, L.; Lee, K.-W.; Kudaba, I.; Garrido, M.; Chung, H.C.; Lee, J.; et al. Efficacy and Safety of Pembrolizumab or Pembrolizumab Plus Chemotherapy vs Chemotherapy Alone for Patients with First-line, Advanced Gastric Cancer: The KEYNOTE-062 Phase 3 Randomized Clinical Trial. JAMA Oncol. 2020, 6, 1571–1580. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Case | Age (Years) | Gender | Primary | Site of Metastasis | Agent Type | Number of Cycles | Months of CPI | Response |
|---|---|---|---|---|---|---|---|---|
| 1 | 59 | Male | poorly diff gastric adenocarcinoma | peritoneal carcinomatosis | pembrolizumab | 23 | 21 | No evidence of Disease |
| 2 | 79 | Male | poorly diff gastric adenocarcinoma | intrathoracic and intraabdominal nodal metastases | nivolumab pembrolizumab | 6 26 (200 mg) + 16 (400 mg) = 42 | 4.5 18 + 21 = 39 | No evidence of Disease |
| 3 | 61 | Male | poorly diff gastric adenocarcinoma | innumerable hepatic lesions | pembrolizumab | 16 (200 mg) + 11 (400 mg) = 27 | 18.5 + 20.5 = 39 | Continued partial response |
| Case | HER2 | IHC | MSI | PDL1 (CPS) | NGS |
|---|---|---|---|---|---|
| 1 | negative | Strongly + CK7 +CDX2 (40%) Negative CK20 Negative H pylori | Cannot be determined | +(35%) | ATR L1707I PIK3R1 T576del TMB cannot be determined |
| 2 | negative | Negative CK7 +CDX2 Negative CK20 Positive AE1/AE3 Positive H pylori | MS-stable | +(50%) | MET amplification CDK6 amplification—equivocal EP300 S1476fs*1 FUBP1 I436fs*7 MAP2K4 loss TP53 E287* |
| 3 | negative | Patchy + CK7 Diffuse positive CDX2 Negative CK20 Weak rare positive HCC Negative SALL4 PAS positive PAS-D negative | MS-stable | +(10%) | PTEN N340fs 0.4% Temsirolimus, Copanlisib, Everolimus TP53 P316fs 0.9% Negative for MUC17 or CLDN18.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaakour, D.; Ward, G.; Dayyani, F. Early Adoption of Checkpoint Inhibitors in Patients with Metastatic Gastric Adenocarcinoma—A Case Series of Non-Operative Long-Term Survivors. Diseases 2022, 10, 24. https://0-doi-org.brum.beds.ac.uk/10.3390/diseases10020024
Kaakour D, Ward G, Dayyani F. Early Adoption of Checkpoint Inhibitors in Patients with Metastatic Gastric Adenocarcinoma—A Case Series of Non-Operative Long-Term Survivors. Diseases. 2022; 10(2):24. https://0-doi-org.brum.beds.ac.uk/10.3390/diseases10020024
Chicago/Turabian StyleKaakour, Dalia, Garrett Ward, and Farshid Dayyani. 2022. "Early Adoption of Checkpoint Inhibitors in Patients with Metastatic Gastric Adenocarcinoma—A Case Series of Non-Operative Long-Term Survivors" Diseases 10, no. 2: 24. https://0-doi-org.brum.beds.ac.uk/10.3390/diseases10020024