
Serum Wisteria Floribunda Agglutinin-Positive Mac-2 Binding Protein Could Not Always Predict Early Cirrhosis in Non-Viral Liver Diseases


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Subjects
2.2. Liver Biopsy and Evaluation of Biopsy Samples
2.3. Clinical and Biological Data
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
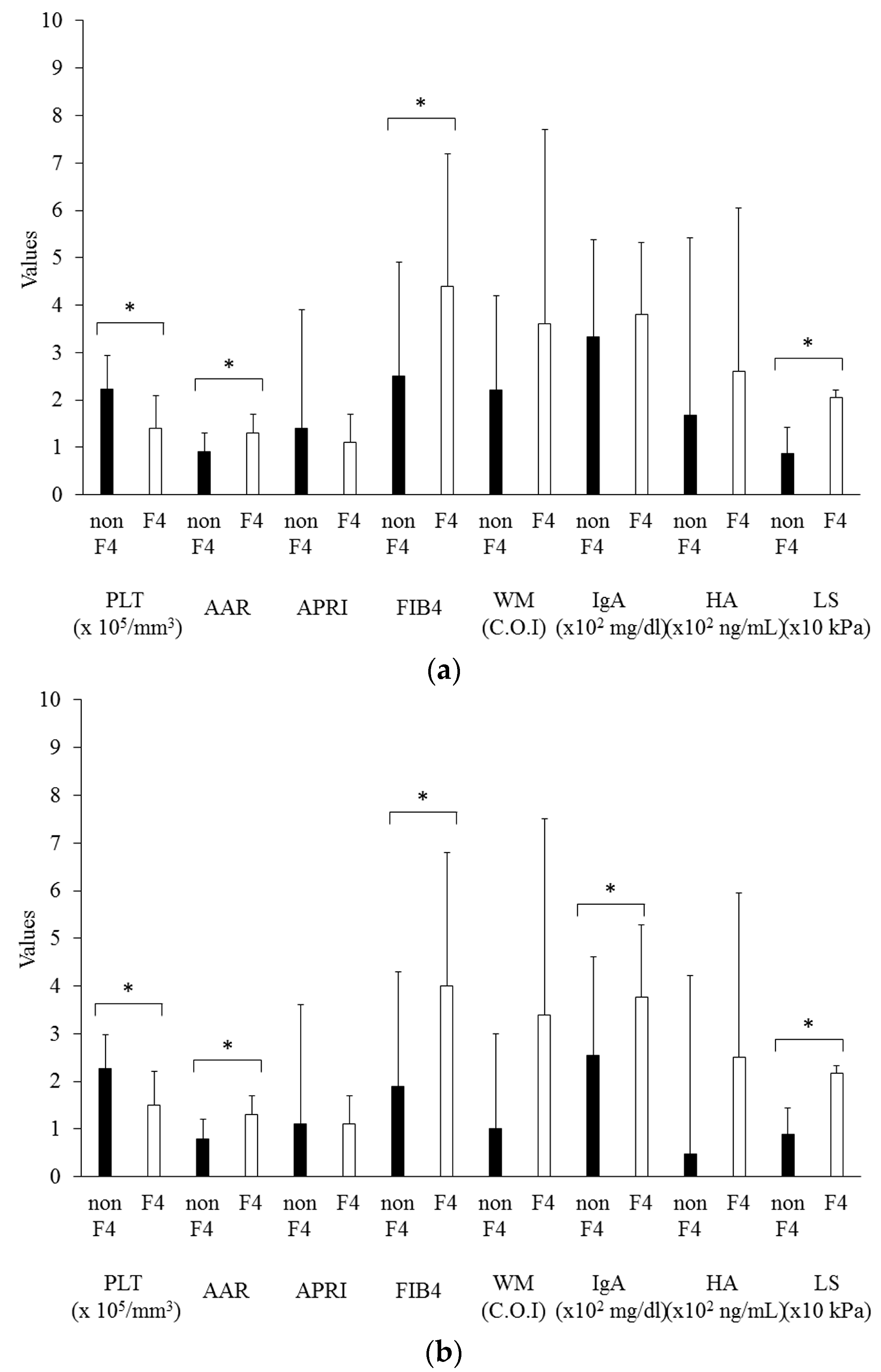
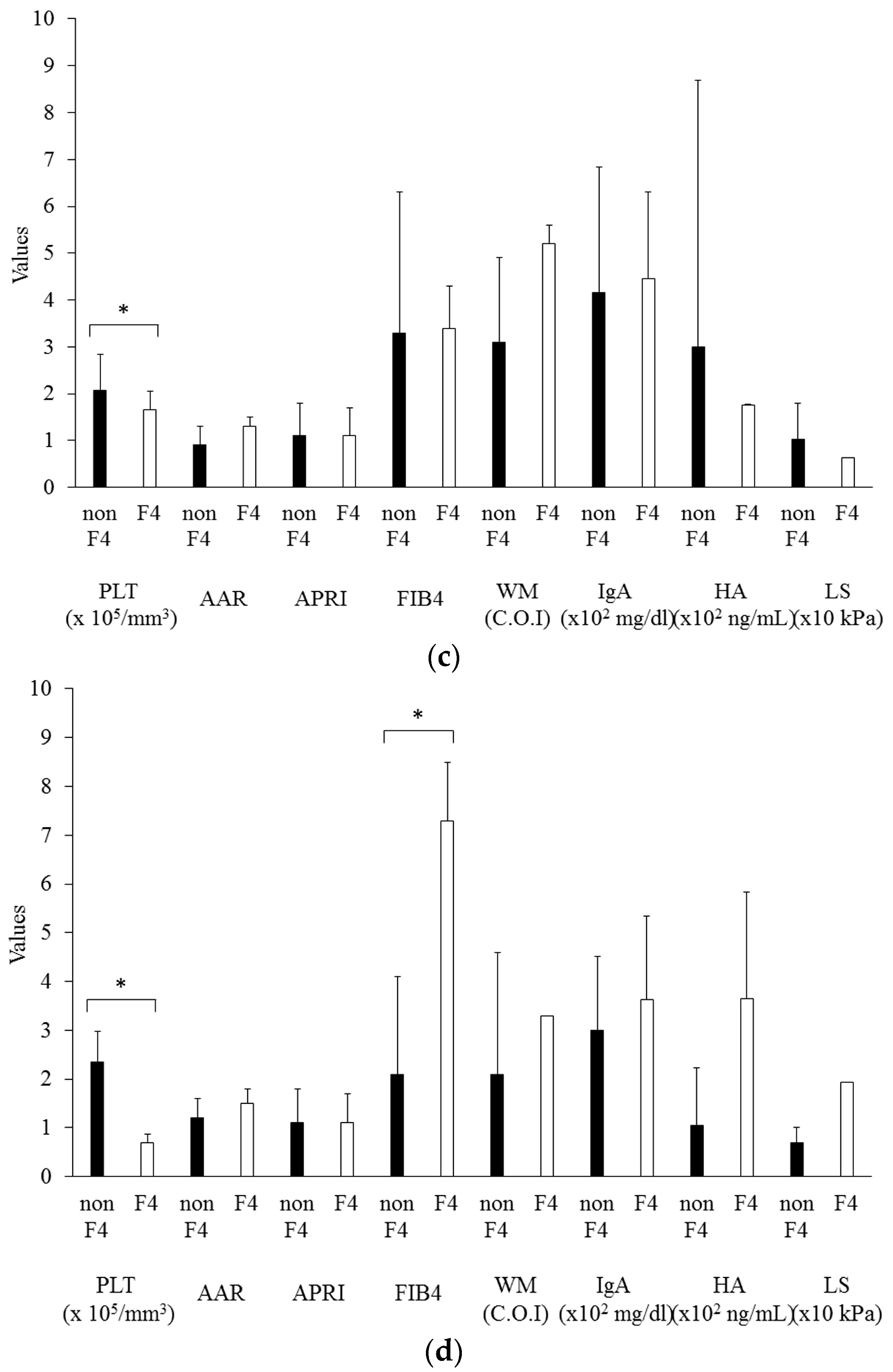
3.2. Diagnostic Performance of Noninvasive Fibrotic Markers in Comparison with Liver Biopsy
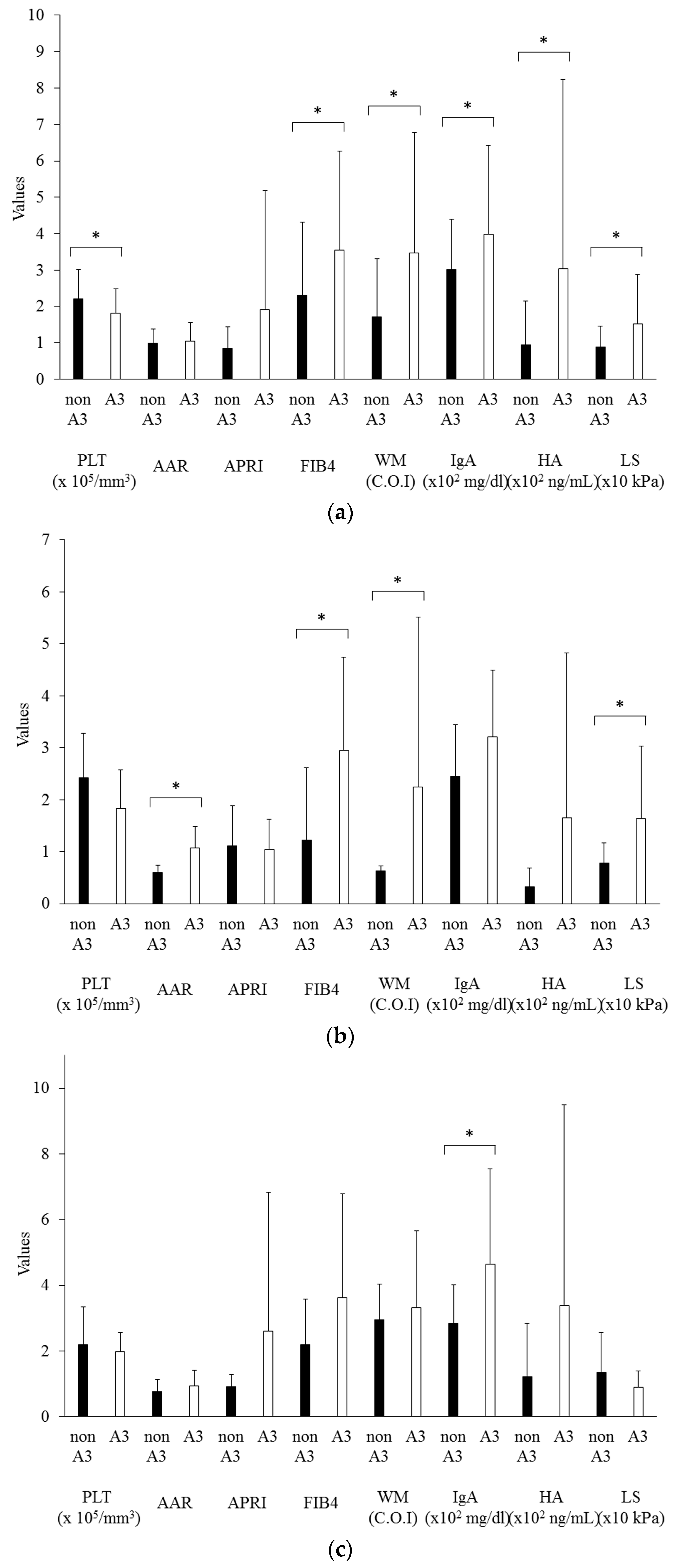
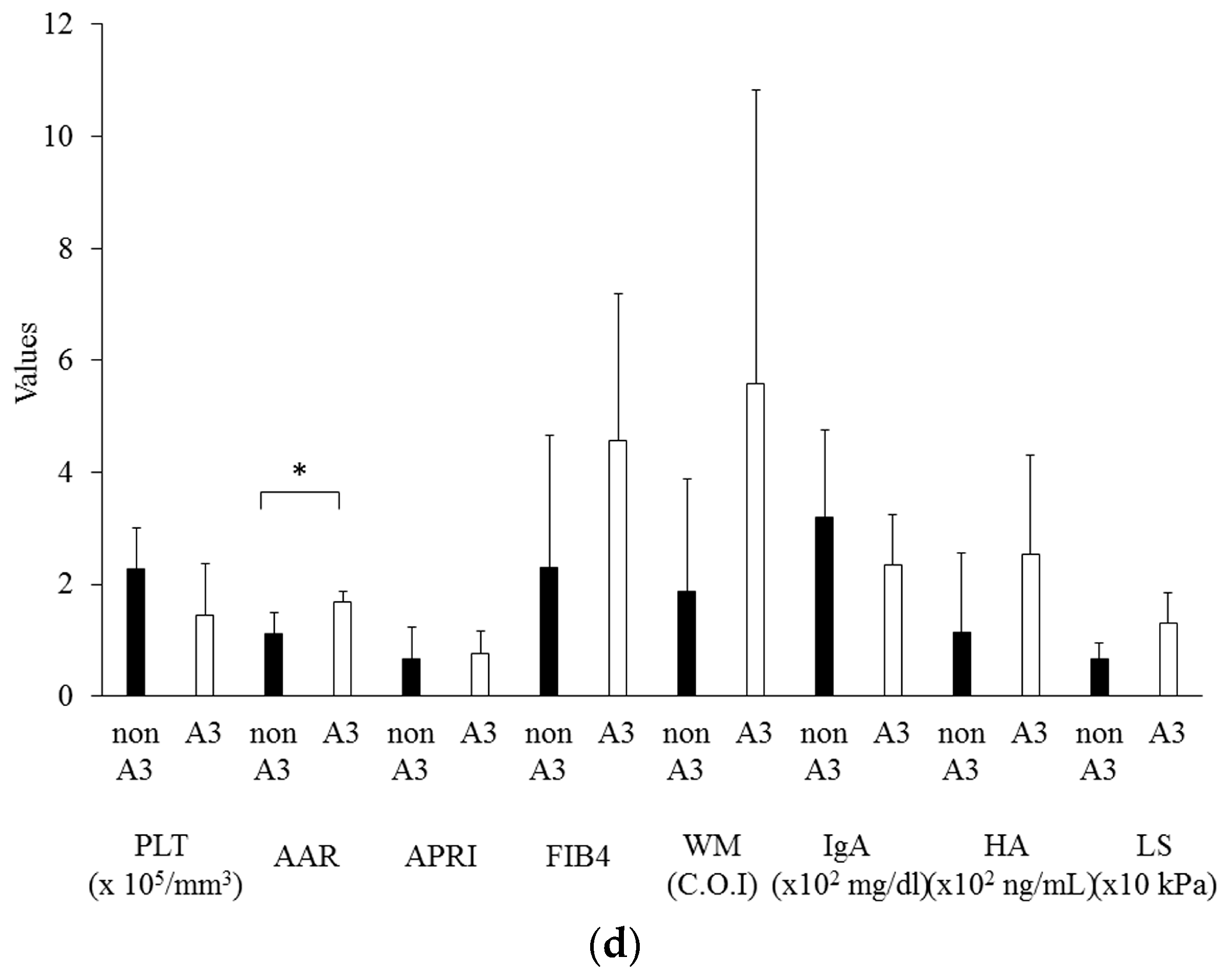
3.3. The Effects of Hepatic Inflammation on Noninvasive Fibrotic Markers
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Ratziu, V.; Bellentani, S.; Cortez-Pinto, H.; Day, C.; Marchesini, G. A position statement on NAFLD/NASH based on the EASL 2009 special conference. J. Hepatol. 2010, 53, 372–384. [Google Scholar] [CrossRef] [PubMed]
- Manns, M.P.; Czaja, A.J.; Gorham, J.D.; Krawitt, E.L.; Mieli-Vergani, G.; Vergani, D.; Vierling, J.M. Diagnosis and management of autoimmune hepatitis. Hepatology 2010, 51, 2193–2213. [Google Scholar] [CrossRef] [PubMed]
- Beuers, U.; Gershwin, M.E.; Gish, R.G.; Invernizzi, P.; Jones, D.E.; Lindor, K.; Ma, X.; Mackay, I.R.; Parés, A.; Tanaka, A.; et al. Changing nomenclature for PBC: from ‘Cirrhosis’ to ‘Cholangitis’. Am. J. Gastroenterol. 2015, 110, 1536–1538. [Google Scholar] [CrossRef] [PubMed]
- Lindor, K.D.; Gershwin, M.E.; Poupon, R.; Kaplan, M.; Bergasa, N.V.; Heathcote, E.J. Primary biliary cirrhosis. Hepatology 2009, 50, 291–308. [Google Scholar] [CrossRef] [PubMed]
- Rockey, D.C.; Caldwell, S.H.; Goodman, Z.D.; Nelson, R.C.; Smith, A.D. Liver biopsy. Hepatology 2009, 49, 1017–1044. [Google Scholar] [CrossRef] [PubMed]
- Matsumura, H.; Moriyama, M.; Goto, I.; Tanaka, N.; Okubo, H.; Arakawa, Y. Natural course of progression of liver fibrosis in Japanese patients with chronic liver disease type C—A study of 527 patients at one establishment. J. Viral Hepat. 2000, 7, 268–275. [Google Scholar] [CrossRef] [PubMed]
- Neuman, M.G.; Cohen, L.B.; Nanau, R.M. Hyaluronic acid as a non-invasive biomarker of liver fibrosis. Clin. Biochem. 2016, 49, 302–315. [Google Scholar] [CrossRef] [PubMed]
- Wai, C.T.; Greenson, J.K.; Fontana, R.J.; Kalbfleisch, J.D.; Marrero, J.A.; Conjeevaram, H.S.; Lok, A.S. A simple noninvasive index can predict both significant fibrosis and cirrhosis in patients with chronic hepatitis C. Hepatology 2003, 38, 518–526. [Google Scholar] [CrossRef] [PubMed]
- Sterling, R.K.; Lissen, E.; Clumeck, N.; Sola, R.; Correa, M.C.; Montaner, J.; Sulkowski, M.S.; Torriani, F.J.; Dieterich, D.T.; Thomas, D.L.; et al. Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV coinfection. Hepatology 2006, 43, 1317–1325. [Google Scholar] [CrossRef] [PubMed]
- Masuzaki, R.; Tateishi, R.; Yoshida, H.; Goto, E.; Sato, T.; Ohki, T.; Imamura, J.; Goto, T.; Kanai, F.; Kato, N.; et al. Prospective risk assessment for hepatocellular carcinoma development in patients with chronic hepatitis C by transient elastography. Hepatology 2009, 49, 1954–1961. [Google Scholar] [CrossRef] [PubMed]
- Inohara, H.; Akahani, S.; Koths, K.; Raz, A. Interactions between galectin-3 and Mac-2-binding protein mediate cell-cell adhesion. Cancer Res. 1996, 56, 4530–4534. [Google Scholar] [PubMed]
- Yamasaki, K.; Tateyama, M.; Abiru, S.; Komori, A.; Nagaoka, S.; Saeki, A.; Hashimoto, S.; Sasaki, R.; Bekki, S.; Kugiyama, Y.; et al. Elevated serum levels of Wisteria floribunda agglutinin-positive human Mac-2 binding protein predict the development of hepatocellular carcinoma in hepatitis C patients. Hepatology 2014, 60, 1563–1570. [Google Scholar] [CrossRef] [PubMed]
- Abe, M.; Miyake, T.; Kuno, A.; Imai, Y.; Sawai, Y.; Hino, K.; Hara, Y.; Hige, S.; Sakamoto, M.; Yamada, G.; et al. Association between Wisteria floribunda agglutinin-positive Mac-2 binding protein and the fibrosis stage of non-alcoholic fatty liver disease. J. Gastroenterol. 2015, 50, 776–784. [Google Scholar] [CrossRef] [PubMed]
- Kuno, A.; Ikehara, Y.; Tanaka, Y.; Ito, K.; Matsuda, A.; Sekiya, S.; Hige, S.; Sakamoto, M.; Kage, M.; Mizokami, M.; et al. A serum “sweet-doughnut” protein facilitates fibrosis evaluation and therapy assessment in patients with viral hepatitis. Sci. Rep. 2013, 3, 1065. [Google Scholar] [CrossRef] [PubMed]
- Fujiyoshi, M.; Kuno, A.; Gotoh, M.; Fukai, M.; Yokoo, H.; Kamachi, H.; Kamiyama, T.; Korenaga, M.; Mizokami, M.; Narimatsu, H.; et al. Clinicopathological characteristics and diagnostic performance of Wisteria floribunda agglutinin positive Mac-2-binding protein as a preoperative serum marker of liver fibrosis in hepatocellular carcinoma. J. Gastroenterol. 2015, 50, 1134–1144. [Google Scholar] [CrossRef] [PubMed]
- Umemura, T.; Joshita, S.; Sekiguchi, T.; Usami, Y.; Shibata, S.; Kimura, T.; Komatsu, M.; Matsumoto, A.; Ota, M.; Tanaka, E. Serum Wisteria floribunda agglutinin-positive mac-2-binding protein level predicts liver fibrosis and prognosis in primary biliary cirrhosis. Am. J. Gastroenterol. 2015, 110, 857–864. [Google Scholar] [CrossRef] [PubMed]
- Goodman, Z.D. Grading and staging systems for inflammation and fibrosis in chronic liver diseases. J. Hepatol. 2007, 47, 598–607. [Google Scholar] [CrossRef] [PubMed]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Diehl, A.M.; Brunt, E.M.; Cusi, K.; Charlton, M.; Sanyal, A.J. The diagnosis and management of non-alcoholic fatty liver disease: Practice guideline by the American Association for the Study of Liver Diseases, American College of Gastroenterology, and the American Gastroenterological Association. Hepatology 2012, 55, 2005–2023. [Google Scholar] [CrossRef] [PubMed]
- Alvarez, F.; Berg, P.A.; Bianchi, F.B.; Bianchi, L.; Burroughs, A.K.; Cancado, E.L.; Chapman, R.W.; Cooksley, W.G.; Czaja, A.J.; Desmet, V.J.; et al. International Autoimmune Hepatitis Group Report: Review of criteria for diagnosis of autoimmune hepatitis. J. Hepatol. 1999, 31, 929–938. [Google Scholar] [CrossRef]
- Kanda, T.; Yokosuka, O.; Imazeki, F.; Saisho, H. Bezafibrate treatment: A new medical approach for PBC patients? J. Gastroenterol. 2003, 38, 573–578. [Google Scholar] [PubMed]
- Nakamura, M.; Kanda, T.; Nakamoto, S.; Miyamura, T.; Jiang, X.; Wu, S.; Yokosuka, O. No correlation between PNPLA3 rs738409 genotype and fatty liver and hepatic cirrhosis in Japanese patients with HCV. PLoS ONE 2013, 8, e81312. [Google Scholar] [CrossRef] [PubMed]
- Angulo, P.; Hui, J.M.; Marchesini, G.; Bugianesi, E.; George, J.; Farrell, G.C.; Enders, F.; Saksena, S.; Burt, A.D.; Bida, J.P.; et al. The NAFLD fibrosis score: A noninvasive system that identifies liver fibrosis in patients with NAFLD. Hepatology 2007, 45, 846–854. [Google Scholar] [CrossRef] [PubMed]
- Pelliccia, P.; Natoli, C.; Petitti, M.T.; Verrotti, A.; Chiarelli, F.; Iacobelli, S. Elevated levels of circulating immunostimulatory 90K in Henoch-Schoenlein purpura. J. Clin. Immunol. 1999, 19, 143–147. [Google Scholar] [CrossRef] [PubMed]
- Grassadonia, A.; Tinari, N.; Iurisci, I.; Piccolo, E.; Cumashi, A.; Innominato, P.; D’Egidio, M.; Natoli, C.; Piantelli, M.; Iacobelli, S. 90K (Mac-2 BP) and galectins in tumor progression and metastasis. Glycoconj. J. 2004, 19, 551–556. [Google Scholar] [CrossRef] [PubMed]
- Artini, M.; Natoli, C.; Tinari, N.; Costanzo, A.; Marinelli, R.; Balsano, C.; Porcari, P.; Angelucci, D.; D’Egidio, M.; Levrero, M.; et al. Elevated serum levels of 90K/MAC-2 BP predict unresponsiveness to alpha-interferon therapy in chronic HCV hepatitis patients. J. Hepatol. 1996, 25, 212–217. [Google Scholar] [CrossRef]
- Natoli, C.; Dianzani, F.; Mazzotta, F.; Balocchini, E.; Pierotti, P.; Antonelli, G.; Iacobelli, S. 90K protein: A new predictor marker of disease progression in human immunodeficiency virus infection. J. Acquir. Immune Defic. Syndr. 1993, 6, 370–375. [Google Scholar] [PubMed]
- Kamada, Y.; Fujii, H.; Fujii, H.; Sawai, Y.; Doi, Y.; Uozumi, N.; Mizutani, K.; Akita, M.; Sato, M.; Kida, S.; et al. Serum Mac-2 binding protein levels as a novel diagnostic biomarker for prediction of disease severity and nonalcoholic steatohepatitis. Proteom. Clin. Appl. 2013, 7, 648–656. [Google Scholar] [CrossRef] [PubMed]
- Kamada, Y.; Ono, M.; Hyogo, H.; Fujii, H.; Sumida, Y.; Mori, K.; Tanaka, S.; Yamada, M.; Akita, M.; Mizutani, K.; et al. A novel noninvasive diagnostic method for nonalcoholic steatohepatitis using two glycobiomarkers. Hepatology 2015, 62, 1433–1443. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total Patients | NASH | AIH | PBC | |
|---|---|---|---|---|
| n (Male/Female) | 94 (21/73) | 34 (14/20) | 31 (2/29) | 29 (5/24) |
| Age | 58.0 ± 13.6 | 53.9 ± 16.4 | 60.1 ± 11.0 | 60.5 ± 11.4 |
| BMI (kg/m2) | 25.0 ± 4.4 | 27.9 ± 3.7 | 22.9 ± 3.6 | 23.9 ± 4.1 |
| A grade (A1/A2/A3) | 17/34/37 | 6/14/12 | 1/6/21 | 10/14/4 |
| F stage (F1/F2/F3/F4) | 42/10/16/21 | 14/2/1/16 | 12/4/10/2 | 16/4/5/3 |
| Platelet counts (×104/mm3) | 20.2 ± 7.9 | 19.1 ± 8.1 | 20.0 ± 7.9 | 21.9 ± 8.0 |
| AST (IU/L) | 82.2 ± 141.5 | 66.0 ± 39.0 | 139.4 ± 233.8 | 40.1 ± 19.0 |
| ALT (IU/L) | 98.6 ± 154.8 | 84.1 ± 62.6 | 170.6 ± 245.4 | 38.4 ± 27.2 |
| ALP (IU/L) | 381.8 ± 232.0 | 301.4 ± 155.3 | 369.6 ± 154.7 | 488.9 ± 323.8 |
| ALB (g/dL) | 4.1 ± 0.4 | 4.3 ± 0.4 | 3.9 ± 0.4 | 4.0 ± 0.4 |
| T-Chol (mg/dL) | 186.2 ± 43.9 | 176.4 ± 45.9 | 182.1 ± 41.5 | 203.4 ± 40.5 |
| LDL-Chol (mg/dL) | 110.6 ± 36.7 | 106.7 ± 34.1 | 109.3 ± 41.0 | 117.7 ± 34.8 |
| TG (mg/dL) | 133.1 ± 66.6 | 152.8 ± 83.8 | 118.7 ± 45.8 | 124.7 ± 58.1 |
| HbA1c (%) | 5.2 ± 0.7 | 5.6 ± 0.7 | 5.1 ± 0.7 | 5.0 ± 0.5 |
| Ferritin (ng/mL) | 308.4 ± 520.3 | 346.1 ± 454.0 | 459.4 ± 724.6 | 95.9 ± 98.6 |
| ANA (-fold) | 325.7 ± 434.7 | 56.5 ± 63.9 | 457.3 ± 462.8 | 518.5 ± 506.5 |
| IgG (mg/dL) | 1864.8 ± 902.1 | 1390.0 ± 347.0 | 2423.5 ± 1243.4 | 1824.2 ± 532.2 |
| IgA (mg/dL) | 344.8 ± 195.7 | 310.9 ± 128.5 | 413.5 ± 268.2 | 311.1 ± 151.2 |
| IgM (mg/dL) | 187.5 ± 131.7 | 121.4 ± 55.9 | 165.3 ± 111.3 | 288.6 ± 155.6 |
| r | P-Value | |
|---|---|---|
| NASH | 0.65 | <0.01 |
| AIH | 0.30 | 0.12 |
| PBC | 0.64 | <0.01 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haga, Y.; Kanda, T.; Sasaki, R.; Nakamura, M.; Takahashi, K.; Wu, S.; Yasui, S.; Arai, M.; Nakamoto, S.; Yokosuka, O. Serum Wisteria Floribunda Agglutinin-Positive Mac-2 Binding Protein Could Not Always Predict Early Cirrhosis in Non-Viral Liver Diseases. Diseases 2016, 4, 38. https://0-doi-org.brum.beds.ac.uk/10.3390/diseases4040038
Haga Y, Kanda T, Sasaki R, Nakamura M, Takahashi K, Wu S, Yasui S, Arai M, Nakamoto S, Yokosuka O. Serum Wisteria Floribunda Agglutinin-Positive Mac-2 Binding Protein Could Not Always Predict Early Cirrhosis in Non-Viral Liver Diseases. Diseases. 2016; 4(4):38. https://0-doi-org.brum.beds.ac.uk/10.3390/diseases4040038
Chicago/Turabian StyleHaga, Yuki, Tatsuo Kanda, Reina Sasaki, Masato Nakamura, Koji Takahashi, Shuang Wu, Shin Yasui, Makoto Arai, Shingo Nakamoto, and Osamu Yokosuka. 2016. "Serum Wisteria Floribunda Agglutinin-Positive Mac-2 Binding Protein Could Not Always Predict Early Cirrhosis in Non-Viral Liver Diseases" Diseases 4, no. 4: 38. https://0-doi-org.brum.beds.ac.uk/10.3390/diseases4040038