Fertility and Reproduction after Recovery from Anorexia Nervosa: A Systematic Review and Meta-Analysis of Long-Term Follow-Up Studies


Abstract
:1. Introduction
Is the Impairment of Reproductive Function during AN Reversible after Recovery?
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
2.2. Information Source and Search Strategy
2.3. Study Selection
2.4. Data Collection Process and Data Items
2.5. Data Synthesis
3. Results
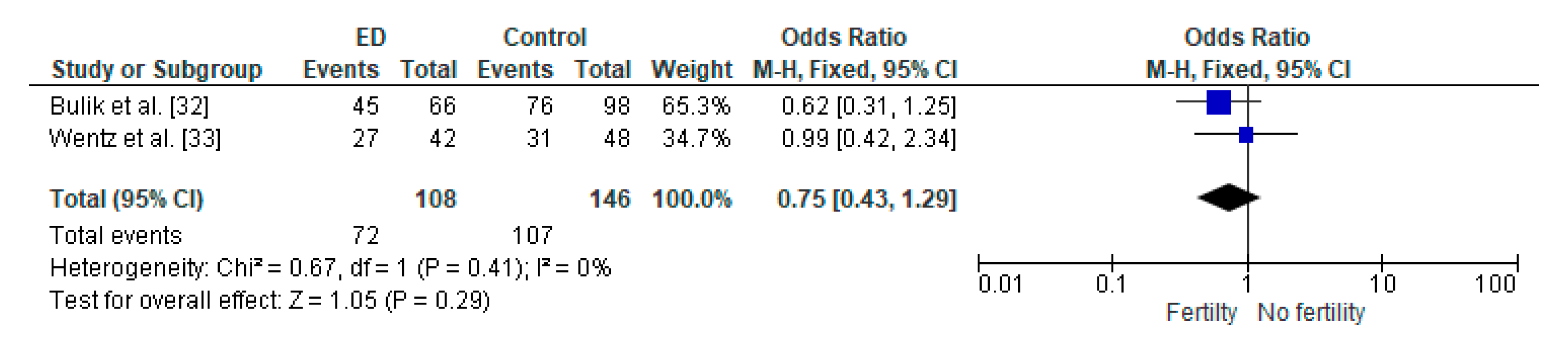
Meta-Analysis
4. Discussion
4.1. Clinical Implications
4.2. Strengths and Limitations
5. Conclusions and Areas for Future Research
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Dalle Grave, R.; Sartirana, M.; El Ghoch, M.; Calugi, S. DSM-5 severity specifiers for anorexia nervosa and treatment outcomes in adult females. Eat. Behav. 2018, 31, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Hudson, J.I.; Hiripi, E.; Pope, H.G., Jr.; Kessler, R.C. The prevalence and correlates of eating disorders in the national comorbidity survey replication. Biol. Psychiatry 2007, 61, 348–358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitchell, J.E.; Crow, S. Medical complications of anorexia nervosa and bulimia nervosa. Curr. Opin. Psychiatry 2006, 19, 438–443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El Ghoch, M.; Gatti, D.; Calugi, S.; Viapiana, O.; Bazzani, P.V.; Dalle Grave, R. The Association between Weight Gain/Restoration and Bone Mineral Density in Adolescents with Anorexia Nervosa: A Systematic Review. Nutrients 2016, 8, 769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calugi, S.; El Ghoch, M.; Conti, M.; Dalle Grave, R. Depression and treatment outcome in anorexia nervosa. Psychiatry Res. 2014, 218, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Calugi, S.; Franchini, C.; Pivari, S.; Conti, M.; El Ghoch, M.; Dalle Grave, R. Anorexia nervosa and childhood sexual abuse: Treatment outcomes of intensive enhanced cognitive behavioural therapy. Psychiatry Res. 2018, 262, 477–481. [Google Scholar] [CrossRef]
- Birmingham, C.; Su, J.; Hlynsky, J.; Goldner, E.; Gao, M. The mortality rate from anorexia nervosa. Int. J. Eat. Disord 2005, 38, 143–146. [Google Scholar] [CrossRef]
- Jayasinghe, Y.; Grover, S.R.; Zacharin, S.M. Current concepts in bone and reproductive health in adolescents with anorexia nervosa. BJOG 2008, 115, 304–315. [Google Scholar] [CrossRef]
- Kimmel, M.C.; Ferguson, E.H.; Zerwas, S.C.; Bulik, C.M.; Meltzer-Brody, S. Obstetric and Gynecologic Problems Associa ted withEating Disorders. Int. J. Eat. Disord. 2016, 49, 260–275. [Google Scholar] [CrossRef]
- Boutari, C.; Pappas, P.D.; Mintziori, G.; Nigdelis, M.P.; Athanasiadis, L.; Goulis, D.G.; Mantzoros, C.S. The effect of underweight on female and male reproduction. Metabolism 2020, 107, 154229. [Google Scholar] [CrossRef]
- Golden, N.H.; Shenker, I.R. Amenorrhea in anorexia nervosa. Neuroendocrine control of hypothalamic dysfunction. Int J. Eat. Disord. 1994, 16, 53–60. [Google Scholar] [CrossRef]
- Gnoth, C.; Godehardt, E.; Frank-Herrmann, P.; Friol, K.; Tigges, J.; Freundl, G. Definition and prevalence of subfertility and infertility. Hum. Reprod. 2005, 20, 1144–1147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffman, E.R.; Zerwas, S.C.; Bulik, C.M. Reproductive issues in anorexia nervosa. Expert Rev. Obs. Gynecol. 2011, 6, 403–414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Méquinion, M.; Chauveau, C.; Viltart, O. The use of animal models to decipher physiological and neurobiological alterations of anorexia nervosa patients. Front. Endocrinol. 2015, 6, 68. [Google Scholar]
- Tabler, J.; Utz, R.L.; Smith, K.R.; Hanson, H.A.; Geist, C. Variation in reproductive outcomes of women with histories of bulimia nervosa, anorexia nervosa, or eating disorder not otherwise specified relative to the general population and closest-aged sisters. Int. J. Eat. Disord. 2018, 51, 102–111. [Google Scholar] [CrossRef]
- Linna, M.S.; Raevuori, A.; Haukka, J.; Suvisaari, J.M.; Suokas, J.T.; Gissler, M. Reproductive Health Outcomes in Eating Disorders. Int J. Eat. Disord. 2013, 46, 826–833. [Google Scholar] [CrossRef]
- Richardson, W.S.; Wilson, M.C.; Nishikawa, J.; Hayward, R.S. The well-built clinical question: A key to evidence-based decisions. ACP J. Club. 1995, 123, A12–A13. [Google Scholar]
- Attia, E.; Roberto, C.A. Should amenorrhea be a diagnostic criterion for anorexia nervosa? Int. J. Eat. Disord. 2009, 42, 581–589. [Google Scholar] [CrossRef]
- Fairburn, C.G.; Cooper, Z. Eating disorders, DSM-5 and clinical reality. Br. J. Psychiatry 2011, 198, 8–10. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. Ann. Intern. Med. 2009, 151, W65–W94. [Google Scholar] [CrossRef] [Green Version]
- Age limits and adolescents. Paediatr Child. Health 2003, 8, 577–578. [CrossRef] [PubMed] [Green Version]
- PubMed, National Library of Medicine. Available online: https://pubmed.ncbi.nlm.nih.gov/ (accessed on 14 September 2020).
- Cochrane Library. Available online: https://www.cochranelibrary.com/ (accessed on 14 September 2020).
- ScienceDirect. Available online: https://0-www-sciencedirect-com.brum.beds.ac.uk/ (accessed on 14 September 2020).
- El Ghoch, M.; Soave, F.; Calugi, S.; Dalle Grave, R. Eating disorders, physical fitness and sport performance: A systematic review. Nutrients 2013, 5, 5140–5160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Popay, J.; Roberts, H.; Sowden, A.; Petticrew, M.; Britten, N.; Arai, L.; Rodgers, M.; Britten, N.; Roen, K.; Duffy, S. Developing guidance on the conduct of narrative synthesis in systematic reviews. J. Epidemiol. Community Health 2005, 59, A7. [Google Scholar]
- Review Manager (RevMan) [Computer Software] Version 5.1; Copenhagen D, Cochrane Collaboration: London, UK, 2011.
- Kohmura, H.; Miyake, A.; Aono, T.; Tanizawa, O. Recovery of reproductive function in patients with anorexia nervosa: A 10-year follow-up study. Eur. J. Obs. Gynecol. Reprod. Biol. 1986, 22, 293–296. [Google Scholar] [CrossRef]
- Brinch, M.; Isager, T.; Tolstrup, K. Anorexia nervosa and motherhood: Reproduction pattern and mothering behavior of 50 women. Acta Psychiatr. Scand. 1988, 77, 611–617. [Google Scholar] [CrossRef]
- Shomento, S.H.; Kreipe, R.E. Menstruation and Fertility Following Anorexia Nervosa. Adolesc. Pediatr. Gynecol. 1994, 7, 142–146. [Google Scholar] [CrossRef]
- Bulik, C.M.; Sullivan, P.F.; Fear, J.L.; Pickering, A.; Dawn, A.; McCullin, M. Fertility and Reproduction in Women with Anorexia Nervosa: A Controlled Study. J. Clin. Psychiatry 1999, 60, 130–135. [Google Scholar] [CrossRef]
- Wentz, E.; Gillberg, I.C.; Anckarsater, H.; Gillberg, C.; Rastam, M. Reproduction and Offspring Status 18 years After Teenage-Onset Anorexia Nervosa—A Controlled Community-Based Study. Int. J. Eat. Disord. 2009, 42, 483–491. [Google Scholar] [CrossRef]
- Bassoe, H.H.; Eseland, I. A prospective study of 133 patients with anorexia nervosa: Treatment and outcome. Acta Psychiatry Stand. 1982, 65, 127–133. [Google Scholar] [CrossRef]
- Beck, J.C.; Brechner-Mortensen, K. Observations on the prognosis in anorexia nervosa. Acta Med. Scand. 1954, 149, 409–430. [Google Scholar] [CrossRef] [PubMed]
- Niskanen, P.; Jaaskelainen, J.; Acte, K. Anorexia nervosa, treatment results and prognosis. Psychiatr. Fenn. 1974, 257–263. [Google Scholar]
- Traboulsi, S.; Itani, L.; Tannir, H.; Kreidieh, D.; El Masri, D.; El Ghoch, M. Is body fat percentage a good predictor of menstrual recovery in females with anorexia nervosa after weight restoration? A systematic review and exploratory and selective meta-analysis. J. Popul. Ther. Clin. Pharmacol. 2019, 26, e25–e37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El Ghoch, M.; Bazzani, P.V.; Dalle Grave, R. Management of ischiopubic stress fracture in patients with anorexia nervosa and excessive compulsive exercising. BMJ Case Rep. 2014. [Google Scholar] [CrossRef] [Green Version]
- Tan, Q. Epigenetic Consequences of Low Birth-Weight and Preterm Birth in Adult Twins. In Handbook of Nutrition, Diet, and Epigenetics; Patel, V., Preedy, V., Eds.; Springer: Cham, Switzerland, 2017. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| First Author | Year | Study Design | Sample | Follow-Up | Finding |
|---|---|---|---|---|---|
| Kohmura et al. [29] | 1986 | Non-controlled study | N = 21 | 8–13 years (Average 10.2 years) |
|
| Brinch et al. [30] | 1988 | Non-controlled study | N = 141 | 4–22 years (Average 12.5 years) |
|
| Shomento et al. [31] | 1994 | Non-controlled study | N = 83 | 6 years |
|
| Bulik et al. [32] | 1999 | Controlled study | N = 66 (AN patients) N = 98 (Controls) | >10 years |
|
| Wentz et al. [33] | 2009 | Controlled study | N = 42 (AN patients) N = 48 (Controls) | 18 years |
|
| Author | Kohmura et al. (1986) [29] | Brinch et al. (1988) [30] | Shomento et al. (1994) [31] |
|---|---|---|---|
| Case series collected in more than one center, i.e., multi-center study | 0 | 0 | 0 |
| Is the hypothesis/aim/objective of the study clearly described? | 1 | 1 | 1 |
| Are the inclusion and exclusion criteria (case definition) clearly reported? | 0 | 0 | 0 |
| Is there a clear definition of the outcomes reported? | 1 | 1 | 1 |
| Were data collected prospectively? | 1 | 1 | 0 |
| Is there an explicit statement that patients were recruited consecutively? | 0 | 0 | 1 |
| Are the main findings of the study clearly described? | 1 | 1 | 1 |
| Are outcomes stratified? | 1 | 1 | 1 |
| Total Score | 5 | 5 | 5 |
| Author | Bulik et al. (1999) [32] | Wentz et al. (2009) [33] |
|---|---|---|
| Selection | ||
| Represents cases with independent validation | 1 | 0 |
| Cases are consecutive | 0 | 0 |
| Controls are from the community | 1 | 1 |
| Controls have no history of anorexia nervosa | 1 | 1 |
| Comparability | ||
| Controls are comparable for the most important factors | 1 | 1 |
| Control for any additional factor | 0 | 0 |
| Ascertainment of exposure | ||
| Same method of ascertainment for cases and controls | 1 | 1 |
| Cases and controls have completed follow up | 0 | 0 |
| Total Score | 5 | 4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chaer, R.; Nakouzi, N.; Itani, L.; Tannir, H.; Kreidieh, D.; El Masri, D.; El Ghoch, M. Fertility and Reproduction after Recovery from Anorexia Nervosa: A Systematic Review and Meta-Analysis of Long-Term Follow-Up Studies. Diseases 2020, 8, 46. https://0-doi-org.brum.beds.ac.uk/10.3390/diseases8040046
Chaer R, Nakouzi N, Itani L, Tannir H, Kreidieh D, El Masri D, El Ghoch M. Fertility and Reproduction after Recovery from Anorexia Nervosa: A Systematic Review and Meta-Analysis of Long-Term Follow-Up Studies. Diseases. 2020; 8(4):46. https://0-doi-org.brum.beds.ac.uk/10.3390/diseases8040046
Chicago/Turabian StyleChaer, Rayane, Nour Nakouzi, Leila Itani, Hana Tannir, Dima Kreidieh, Dana El Masri, and Marwan El Ghoch. 2020. "Fertility and Reproduction after Recovery from Anorexia Nervosa: A Systematic Review and Meta-Analysis of Long-Term Follow-Up Studies" Diseases 8, no. 4: 46. https://0-doi-org.brum.beds.ac.uk/10.3390/diseases8040046