Management of a Facilitated Aesthetic Orthodontic Treatment with Clear Aligners and Minimally Invasive Corticotomy



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
1.1. Background
1.2. Aim
2. Case Reports
2.1. Subject Selection
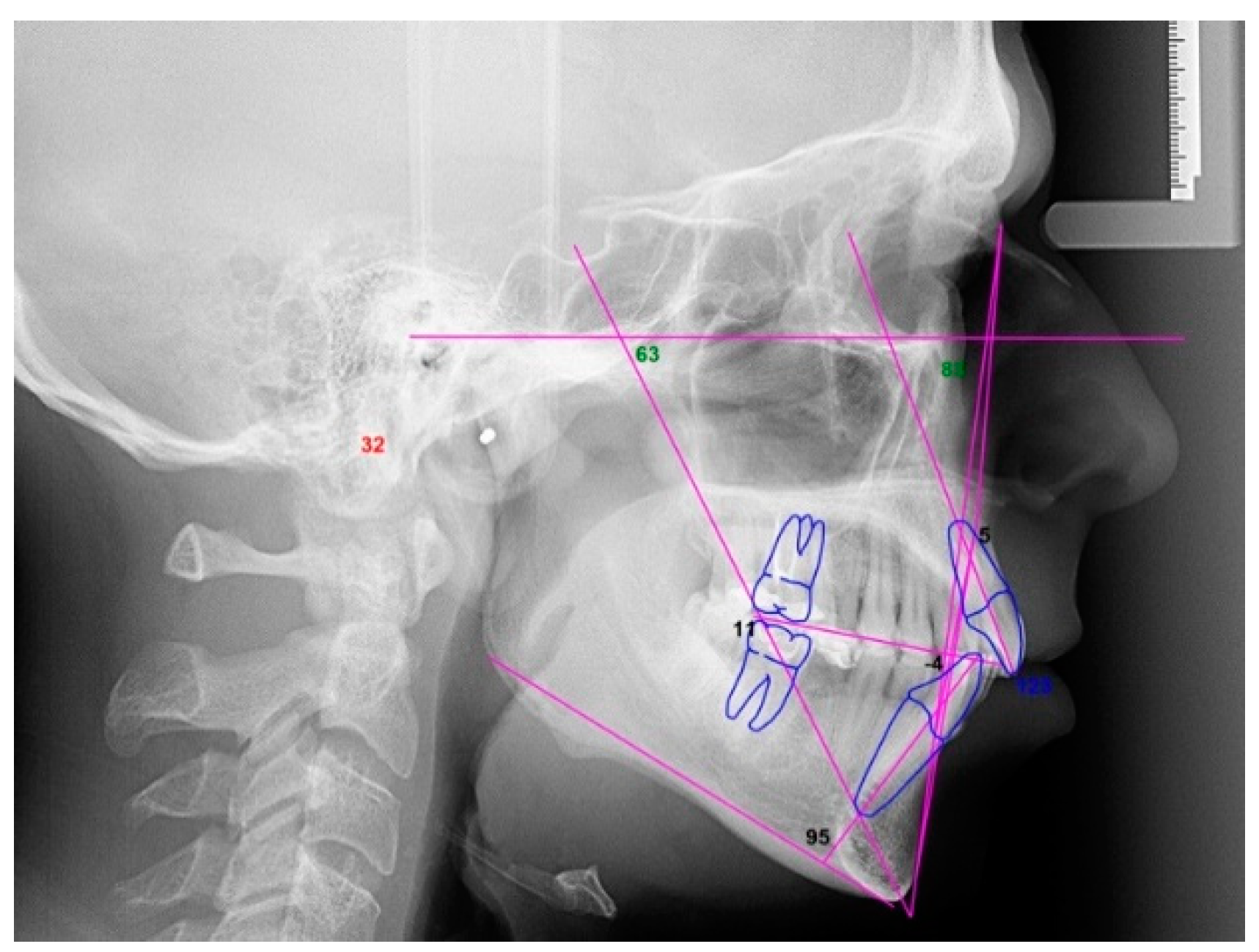
2.2. Orthodontic Planning
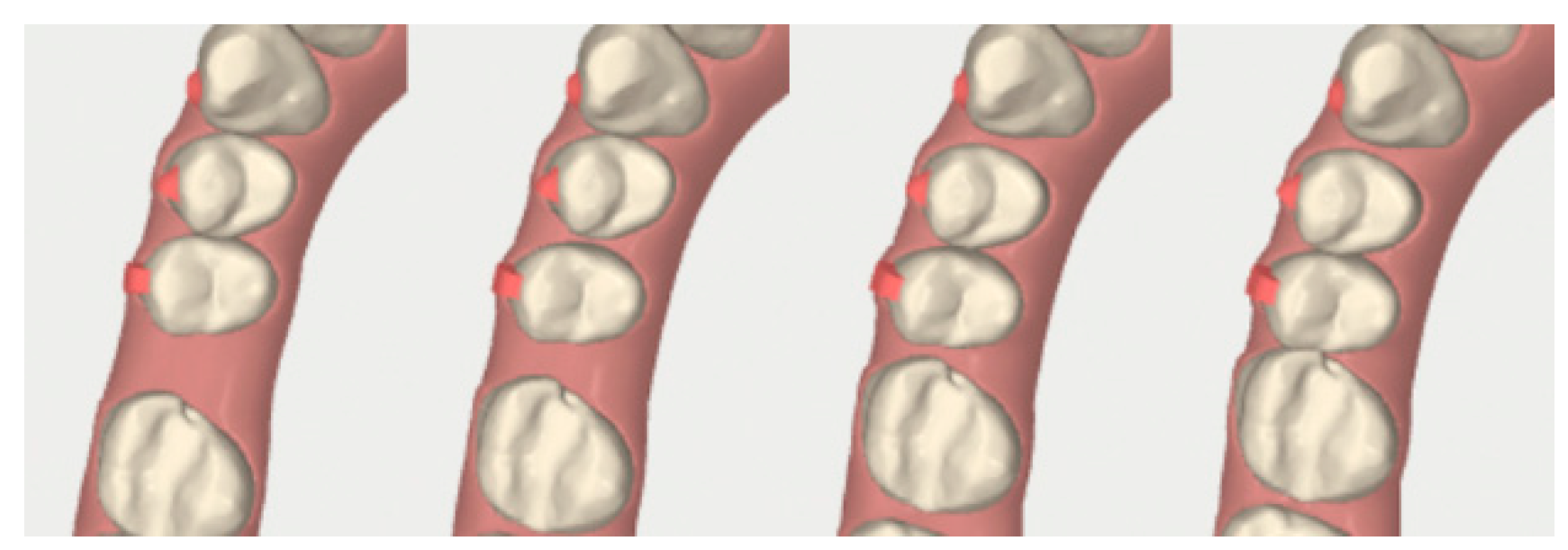
2.3. Surgical Procedure
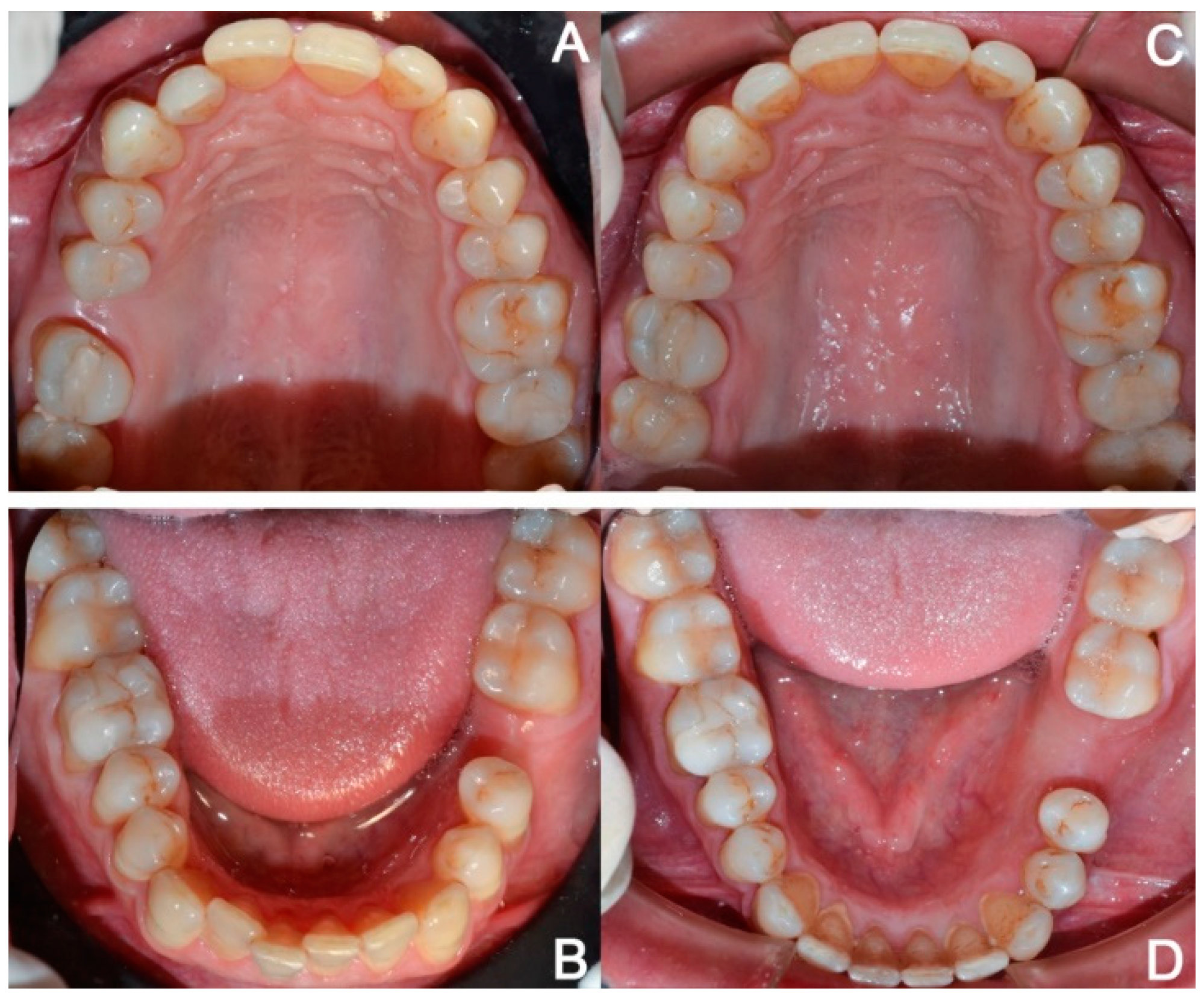
2.3.1. Example—Anterior Open-bite
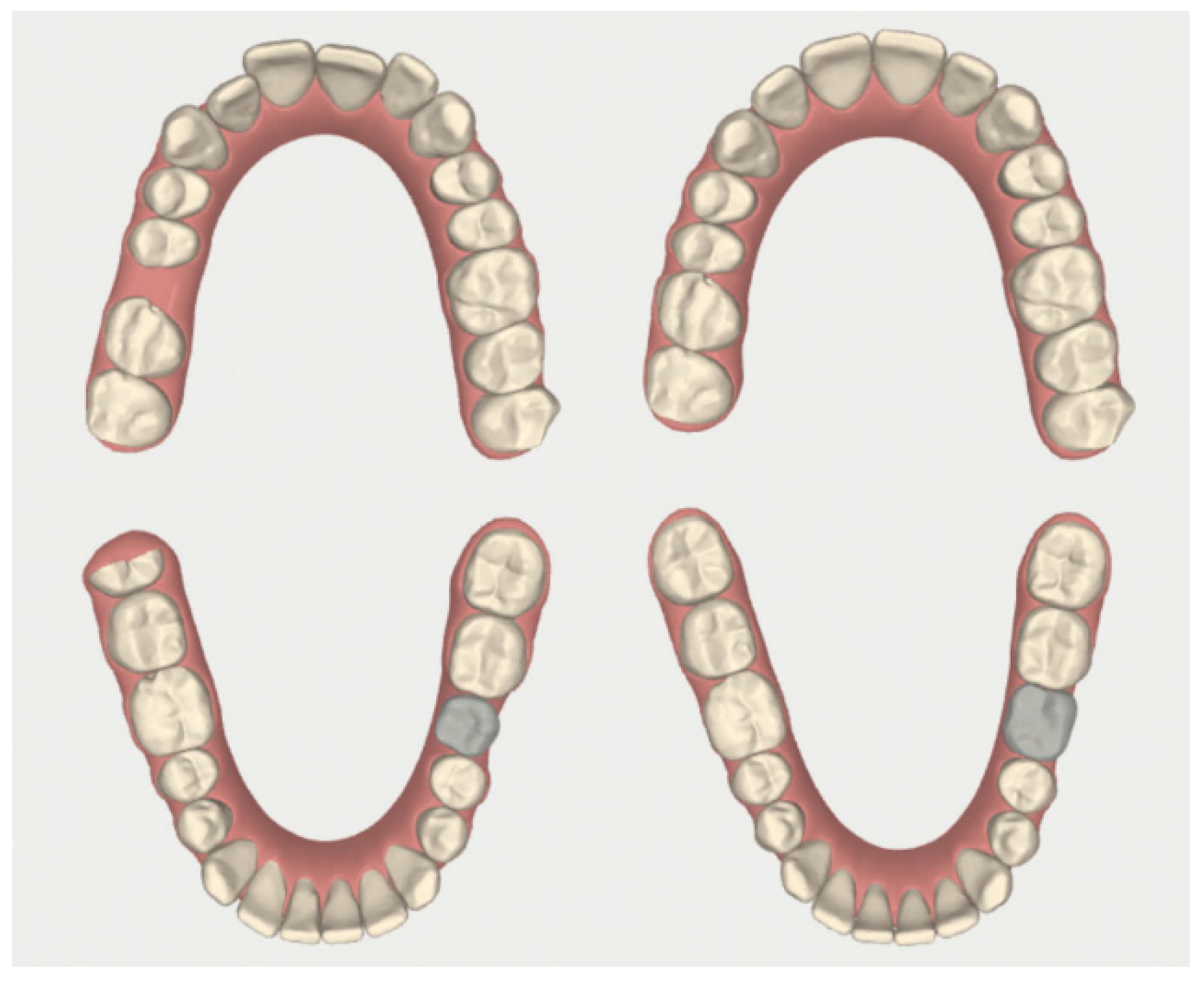
2.3.2. Example 2—Extraction Space Closure
3. Discussion
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Cassetta, M.; Pandolfi, S.; Giansanti, M. Minimally invasive corticotomy in orthodontics: A new technique using a CAD/CAM surgical template. Int. J. Oral Maxillofac. Surg. 2015, 44, 830–833. [Google Scholar] [CrossRef]
- Silvestrini Biavati, A.; Tecco, S.; Migliorati, M.; Festa, F.; Panza, G.; Marzo, G.; Gherlone, E.; Tetè, S. Three-dimensional tomographic mapping related to primary stability and structural miniscrew characteristics. Orthod. Craniofac. Res. 2011, 14, 88–99. [Google Scholar] [CrossRef] [PubMed]
- Liou, E.J.; Huang, C.S. Rapid canine retraction through distraction of the periodontal ligament. Am. J. Orthod. Dentofac. Orthop. 1998, 114, 372–382. [Google Scholar] [CrossRef]
- Collins, M.K.; Sinclair, P.M. The local use of vitamin D to increase the rate of orthodontic tooth movement. Am. J. Orthod. Dentofac. Orthop. 1988, 94, 278–284. [Google Scholar] [CrossRef]
- Kalra, A.; Jaggi, N.; Bansal, M.; Goel, S.; Medsinge, S.V.; Abraham, R.; Jasoria, G. Comparison of rate of canine retraction into recent extraction site with and without gingival fiberotomy: A clinical study. J. Contemp. Dent. Pract. 2013, 14, 419–426. [Google Scholar] [CrossRef] [PubMed]
- Long, H.; Pyakurel, U.; Wang, Y.; Liao, L.; Zhou, Y.; Lai, W. Interventions for accelerating orthodontic tooth movement: A systematic review. Angle Orthod. 2013, 83, 164–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keser, E.I.; Dibart, S. Sequential piezocision: A novel approach to accelerated orthodontic treatment. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 879–889. [Google Scholar] [CrossRef] [PubMed]
- Wilcko, W.; Wilcko, M.T. Accelerating tooth movement: The case for corticotomy-induced orthodontics. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 4–12. [Google Scholar] [CrossRef]
- Chung, K.R.; Oh, M.Y.; Ko, S.J. Corticotomy-assisted orthodontics. J. Clin. Orthod. 2001, 35, 331–339. [Google Scholar]
- Cassetta, M.; Altieri, F.; Barbato, E. The combined use of corticotomy and clear aligners: A case report. Angle Orthod. 2016, 86, 862–870. [Google Scholar] [CrossRef] [Green Version]
- Mathews, D.P.; Kokich, V.G. Accelerating tooth movement: The case against corticotomy-induced orthodontics. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Cassetta, M.; Di Carlo, S.; Giansanti, M.; Pompa, V.; Pompa, G.; Barbato, E. The impact of osteotomy technique for corticotomy-assisted orthodontic treatment (CAOT) on oral health-related quality of life. Eur. Rev. Med. Pharmacol. Sci. 2012, 16, 1735–1740. [Google Scholar] [PubMed]
- Dibart, S.; Surmenian, J.; Sebaoun, J.D.; Montesani, L. Rapid treatment of Class II malocclusion with piezocision: Two case reports. Int. J. Periodont. Restor. Dent. 2010, 30, 487–493. [Google Scholar]
- Milano, F.; Dibart, S.; Montesani, L.; Guerra, L. Computer-guided surgery using the piezocision technique. Int. J. Periodont. Restor. Dent. 2014, 34, 523–529. [Google Scholar] [CrossRef] [Green Version]
- Giancotti, A.; Mampieri, G.; Greco, M. Correction of deep bite in adults using the Invisalign system. J. Clin. Orthod. 2008, 42, 719–726. [Google Scholar]
- Miller, D.B. Invisalign in TMD treatment. Int. J. Orthod. Milwaukee 2009, 20, 15–19. [Google Scholar]
- Caruso, S.; Nota, A.; Ehsani, S.; Maddalone, E.; Ojima, K.; Tecco, S. Impact of molar teeth distalization with clear aligners on occlusal vertical dimension: A retrospective study. BMC Oral Health 2019, 19, 182. [Google Scholar] [CrossRef] [Green Version]
- Tecco, S.; Festa, F.; Salini, V.; Epifania, E.; D’Attilio, M. Treatment of joint pain and joint noises associated with a recent TMJ internal derangement: A comparison of an anterior repositioning splint, a full-arch maxillary stabilization splint, and an untreated control group. Cranio 2004, 22, 209–219. [Google Scholar] [CrossRef]
- Tecco, S.; Nota, A.; Caruso, S.; Primozic, J.; Marzo, G.; Baldini, A.; Gherlone, E.F. Temporomandibular clinical exploration in Italian adolescents. Cranio 2019, 37, 77–84. [Google Scholar] [CrossRef]
- Ciuffolo, F.; Manzoli, L.; Ferritto, A.L.; Tecco, S.; D’Attilio, M.; Festa, F. Surface electromyographic response of the neck muscles to maximal voluntary clenching of the teeth. J. Oral Rehabil. 2005, 32, 79–84. [Google Scholar] [CrossRef]
- Fietze, I.; Laharnar, N.; Obst, A.; Ewert, R.; Felix, S.B.; Garcia, C.; Gläser, S.; Glos, M.; Schmidt, C.O.; Stubbe, B.; et al. Prevalence and association analysis of obstructive sleep apnea with gender and age differences—Results of SHIP-Trend. J. Sleep Res. 2018, 28, e12770. [Google Scholar] [CrossRef] [PubMed]
- Silvestrini-Biavati, A.; Migliorati, M.; Demarziani, E.; Tecco, S.; Silvestrini-Biavati, P.; Polimeni, A.; Saccucci, M. Clinical association between teeth malocclusions, wrong posture and ocular convergence disorders: An epidemiological investigation on primary school children. BMC Pediatr. 2013, 13, 12. [Google Scholar] [CrossRef]
- Meuli, S.; Tecco, S.; Nota, A.; Gatto, R.; Caruso, S. Allineatori in età pediatrica in un caso di recessione gengivale dovuta a malocclusione. Dent. Cadmos 2018, 86, 332. [Google Scholar] [CrossRef]
- Fiorillo, L. Chlorhexidine Gel Use in the Oral District: A Systematic Review. Gels 2019, 5, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salehi, P.; Pakshir, H.R.; Hoseini, S.A.R. Evaluating the Stability of Open Bite Treatments and Its Predictive Factors in the Retention Phase during Permanent Dentition. J. Dent. (Shiraz Iran.) 2015, 16, 22–29. [Google Scholar]
- Remmers, D.; Van’t Hullenaar, R.W.G.J.; Bronkhorst, E.M.; Bergé, S.J.; Katsaros, C. Treatment results and long-term stability of anterior open bite malocclusion. Orthod. Craniofac. Res. 2008, 11, 32–42. [Google Scholar] [CrossRef]
- Cassetta, M.; Altieri, F.; Pandolfi, S.; Giansanti, M. The combined use of computer-guided, minimally invasive, flapless corticotomy and clear aligners as a novel approach to moderate crowding: A case report. Korean J. Orthod. 2017, 47, 130–141. [Google Scholar] [CrossRef] [Green Version]
- Frost, H.M. The biology of fracture healing. An overview for clinicians. Part II. Clin. Orthop. Relat. Res. 1989, 248, 294–309. [Google Scholar]
- Cervino, G.; Fiorillo, L.; Arzukanyan, A.V.; Spagnuolo, G.; Cicciu, M. Dental Restorative Digital Workflow: Digital Smile Design from Aesthetic to Function. Dent. J. (Basel) 2019, 7, 2. [Google Scholar] [CrossRef] [Green Version]
- Miethke, R.-R.; Vogt, S. A comparison of the periodontal health of patients during treatment with the Invisalign system and with fixed orthodontic appliances. J. Orofac. Orthop. 2005, 66, 219–229. [Google Scholar] [CrossRef]
- Miethke, R.-R.; Brauner, K. A Comparison of the periodontal health of patients during treatment with the Invisalign system and with fixed lingual appliances. J. Orofac. Orthop. 2007, 68, 223–231. [Google Scholar] [CrossRef] [PubMed]
- Azaripour, A.; Weusmann, J.; Mahmoodi, B.; Peppas, D.; Gerhold-Ay, A.; Van Noorden, C.J.F.; Willershausen, B. Braces versus Invisalign®: Gingival parameters and patients’ satisfaction during treatment: A cross-sectional study. BMC Oral Health 2015, 15, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levrini, L.; Mangano, A.; Montanari, P.; Margherini, S.; Caprioglio, A.; Abbate, G.M. Periodontal health status in patients treated with the Invisalign(®) system and fixed orthodontic appliances: A 3 months clinical and microbiological evaluation. Eur. J. Dent. 2015, 9, 404–410. [Google Scholar] [CrossRef] [PubMed]
- Mummolo, S.; Tieri, M.; Nota, A.; Caruso, S.; Darvizeh, A.; Albani, F.; Gatto, R.; Marzo, G.; Marchetti, E.; Quinzi, V.; et al. Salivary concentrations of Streptococcus mutans and Lactobacilli during an orthodontic treatment. An observational study comparing fixed and removable orthodontic appliances. Clin. Exp. Dent. Res. 2019, cre2.261. [Google Scholar] [CrossRef] [Green Version]
- Giuca, M.R.; Pasini, M.; Tecco, S.; Giuca, G.; Marzo, G. Levels of salivary immunoglobulins and periodontal evaluation in smoking patients. BMC Immunol. 2014, 15, 5. [Google Scholar] [CrossRef] [Green Version]



















© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caruso, S.; Darvizeh, A.; Zema, S.; Gatto, R.; Nota, A. Management of a Facilitated Aesthetic Orthodontic Treatment with Clear Aligners and Minimally Invasive Corticotomy. Dent. J. 2020, 8, 19. https://0-doi-org.brum.beds.ac.uk/10.3390/dj8010019
Caruso S, Darvizeh A, Zema S, Gatto R, Nota A. Management of a Facilitated Aesthetic Orthodontic Treatment with Clear Aligners and Minimally Invasive Corticotomy. Dentistry Journal. 2020; 8(1):19. https://0-doi-org.brum.beds.ac.uk/10.3390/dj8010019
Chicago/Turabian StyleCaruso, Silvia, Atanaz Darvizeh, Stefano Zema, Roberto Gatto, and Alessandro Nota. 2020. "Management of a Facilitated Aesthetic Orthodontic Treatment with Clear Aligners and Minimally Invasive Corticotomy" Dentistry Journal 8, no. 1: 19. https://0-doi-org.brum.beds.ac.uk/10.3390/dj8010019