
Diagnostic Value of Fluorescence Methods, Visual Inspection and Photographic Visual Examination in Initial Caries Lesion: A Systematic Review and Meta-Analysis

 , ,
, , 
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Selection Criteria
2.3. Data Extraction and Quality Assessment
2.4. Statistical Analyses
3. Results
3.1. Study Selection
3.2. Study Characteristics
3.3. Study Quality Assessment
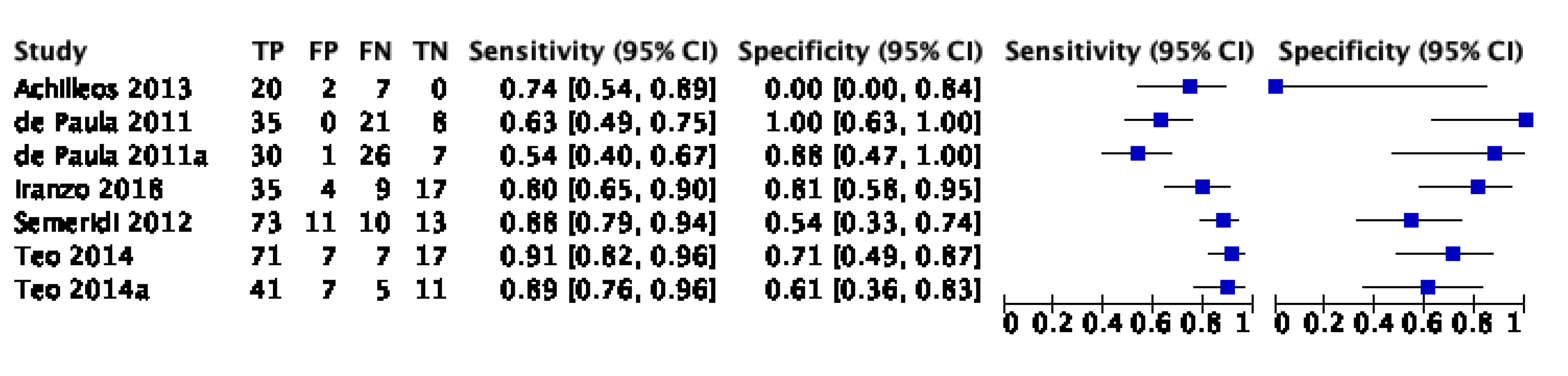
3.4. Sensitivity and Specificity
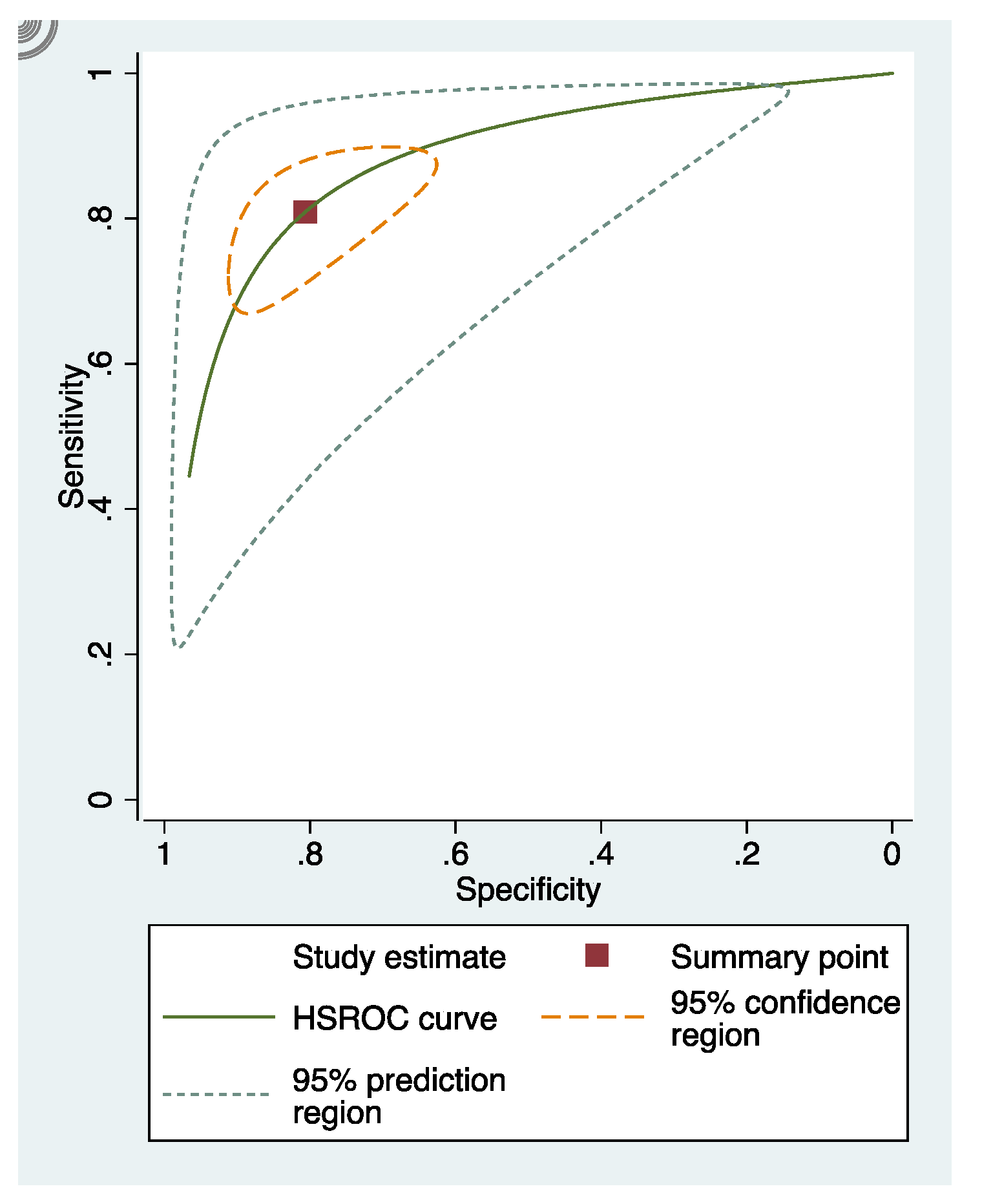
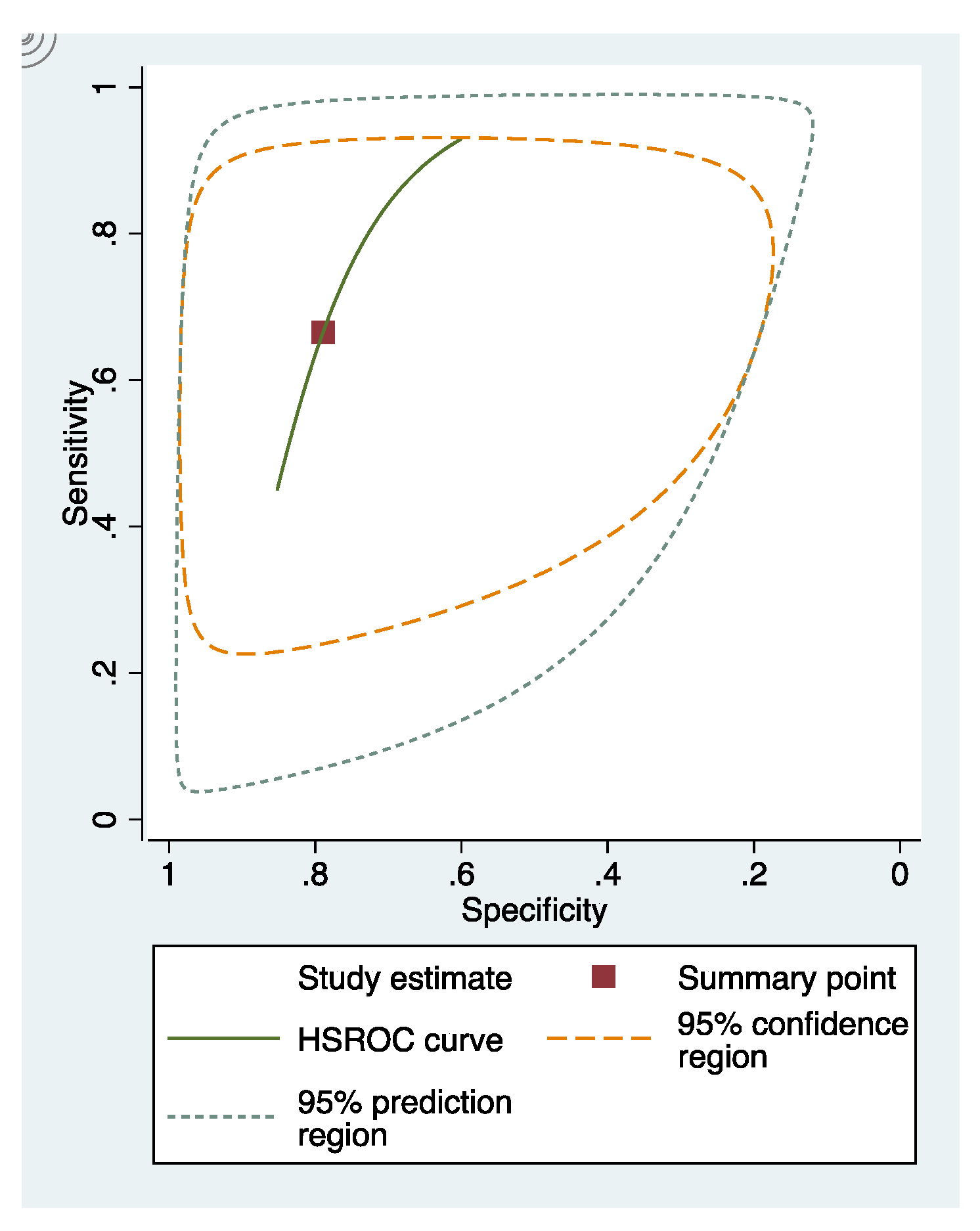
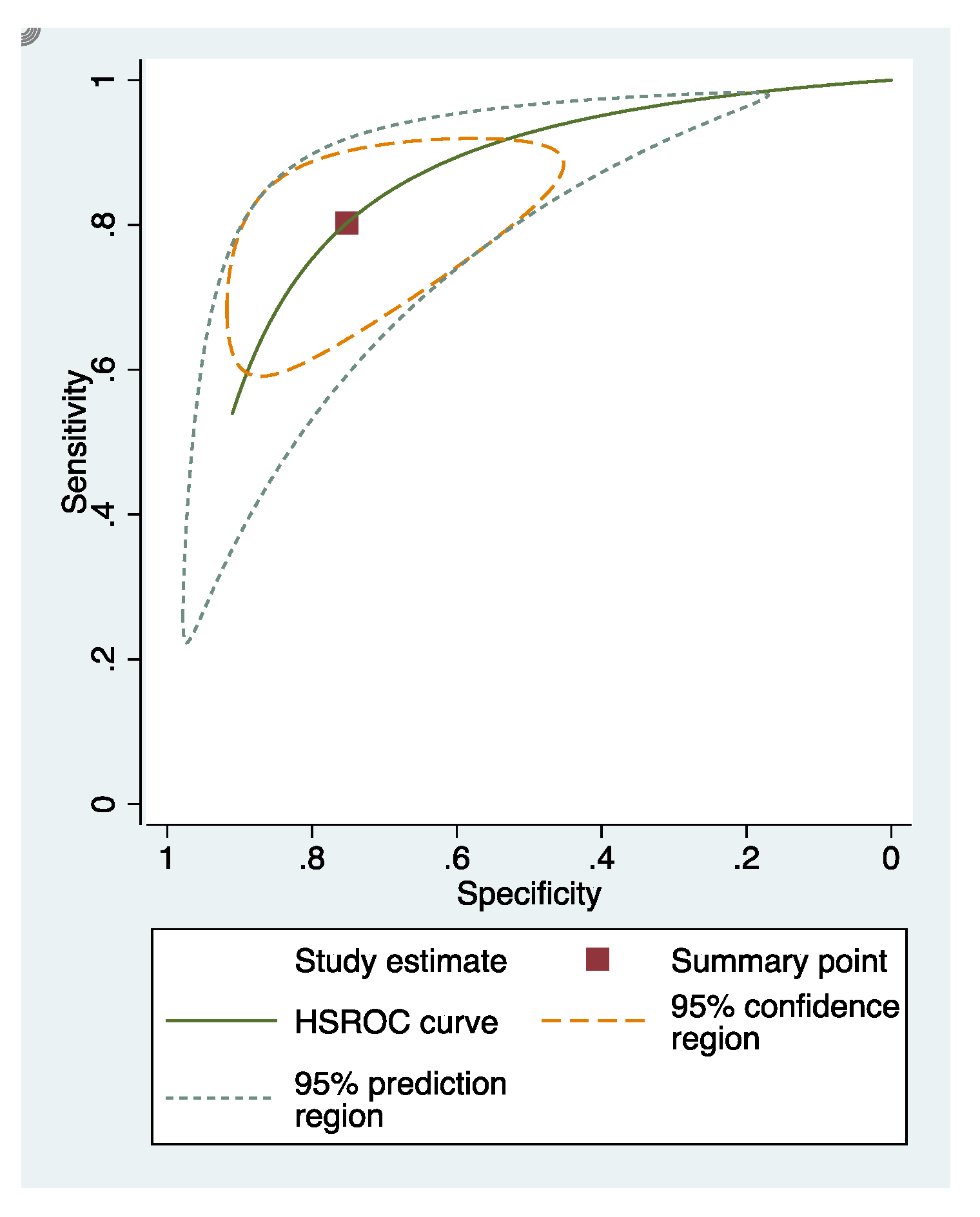
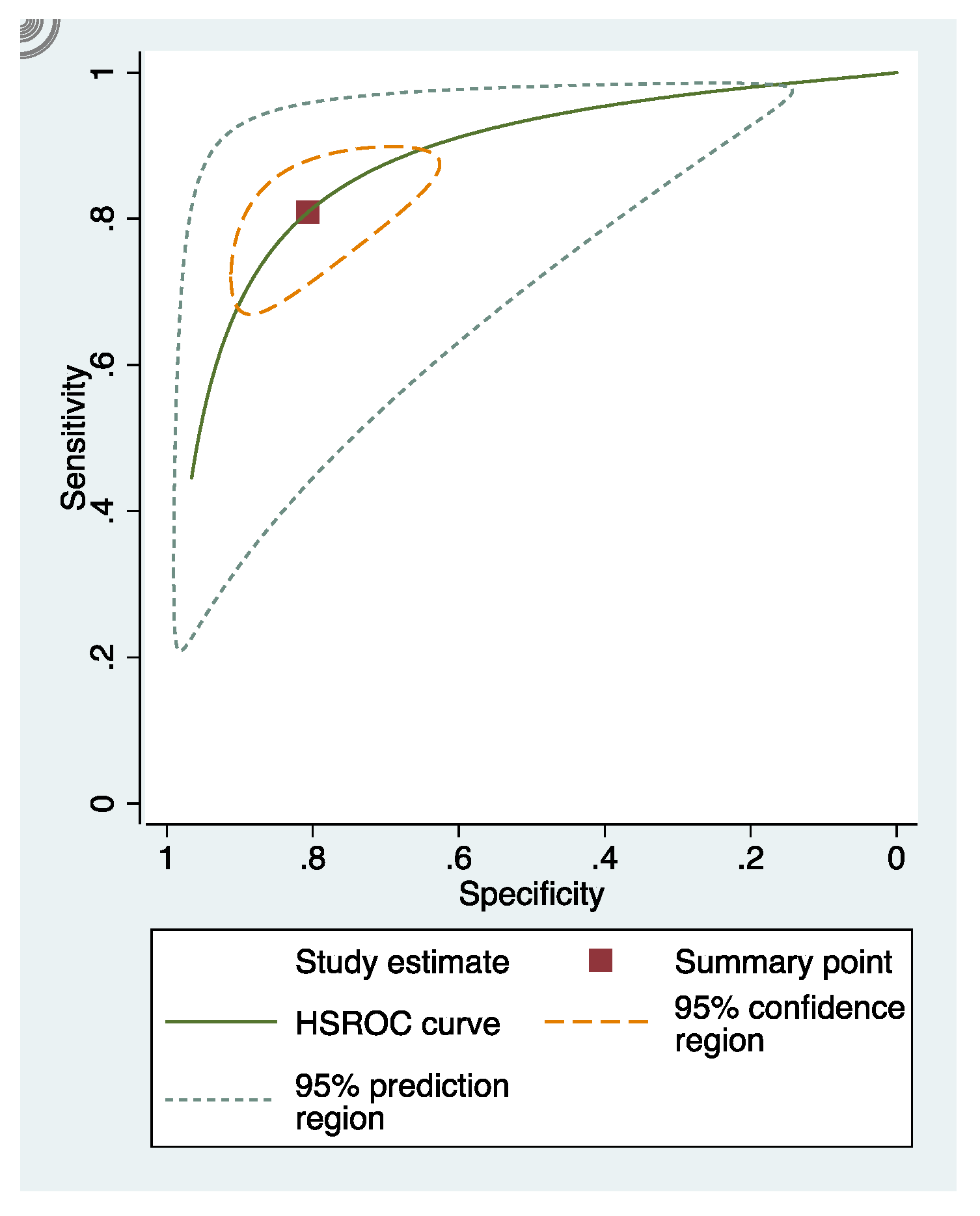
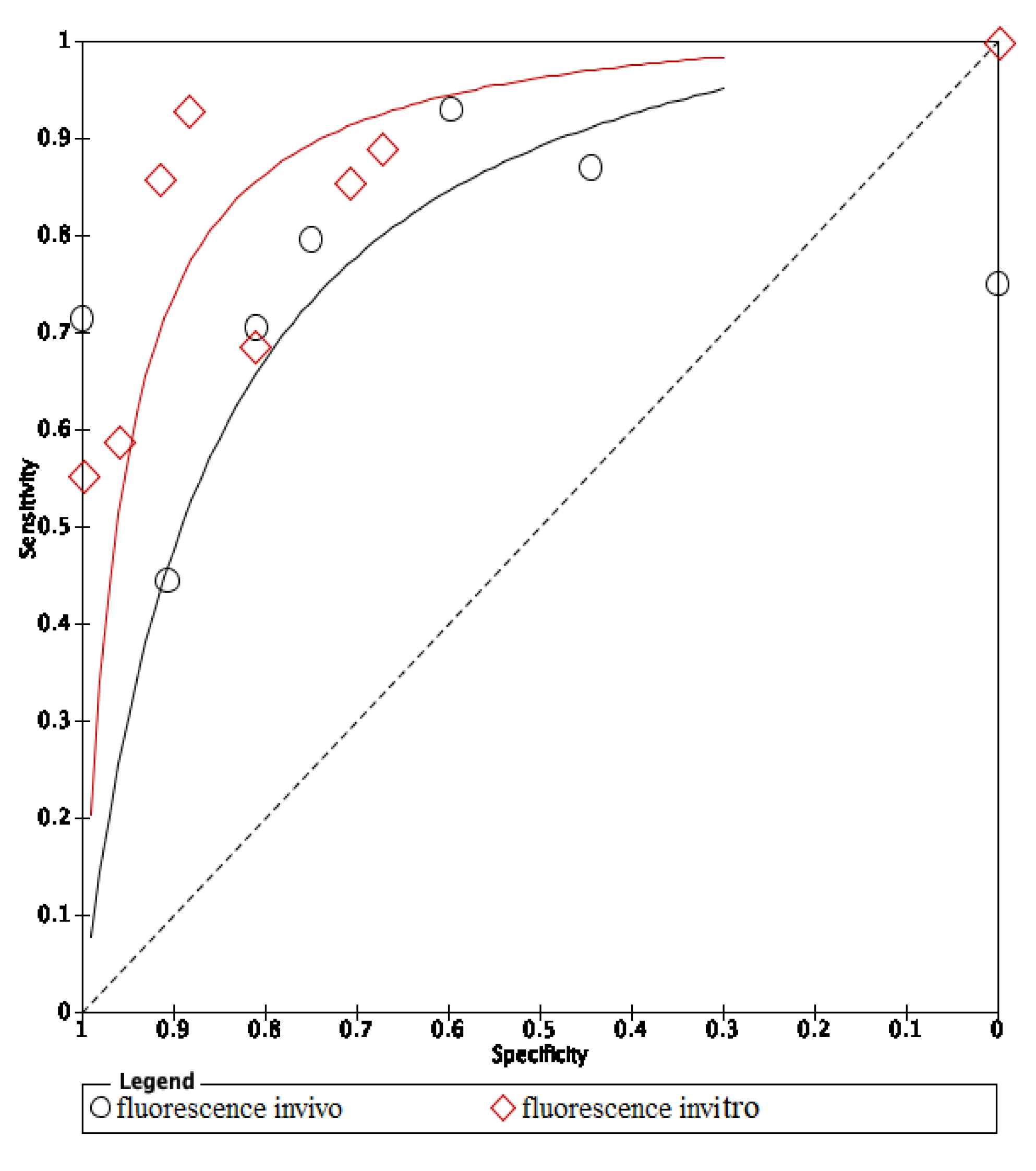
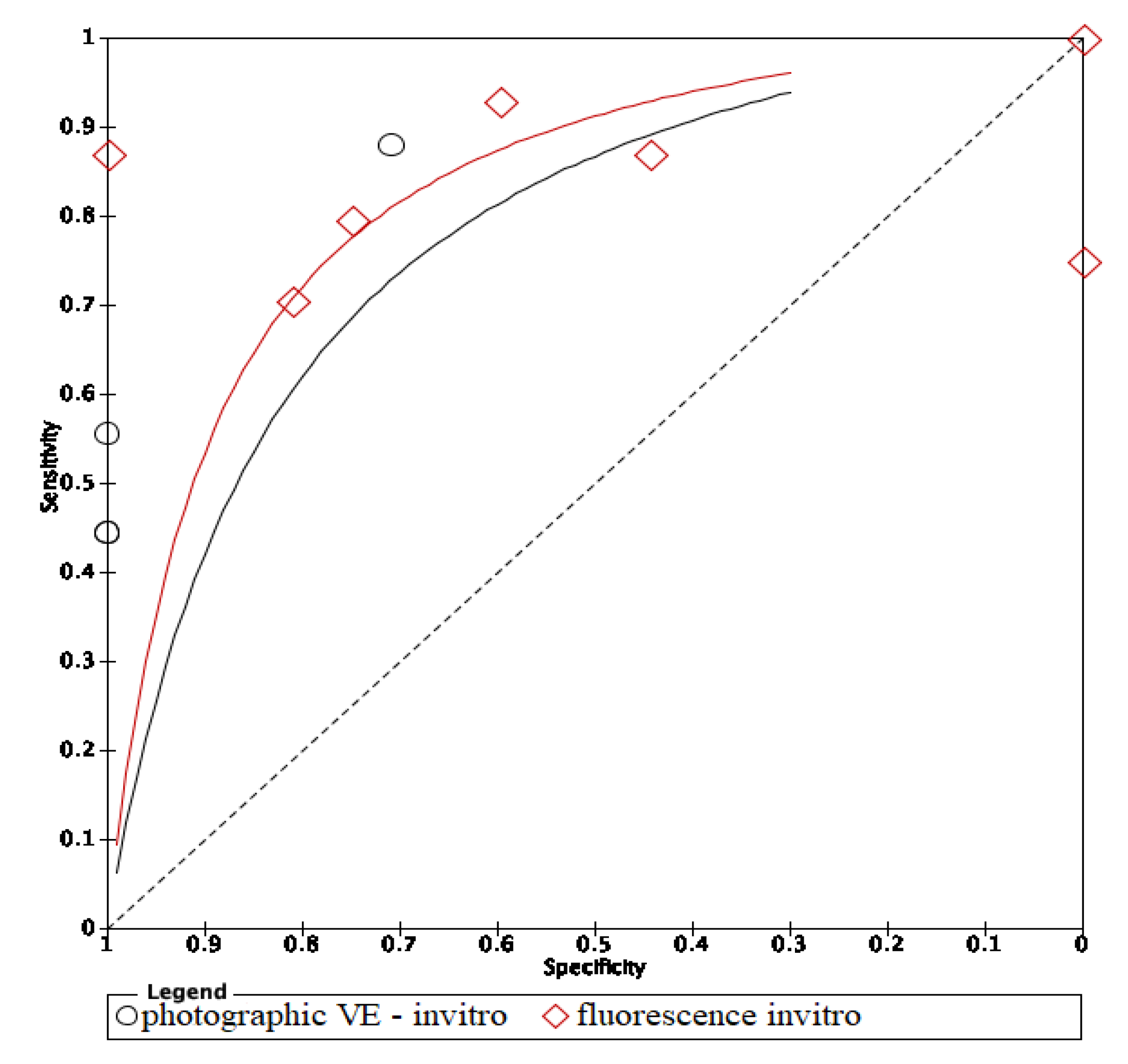
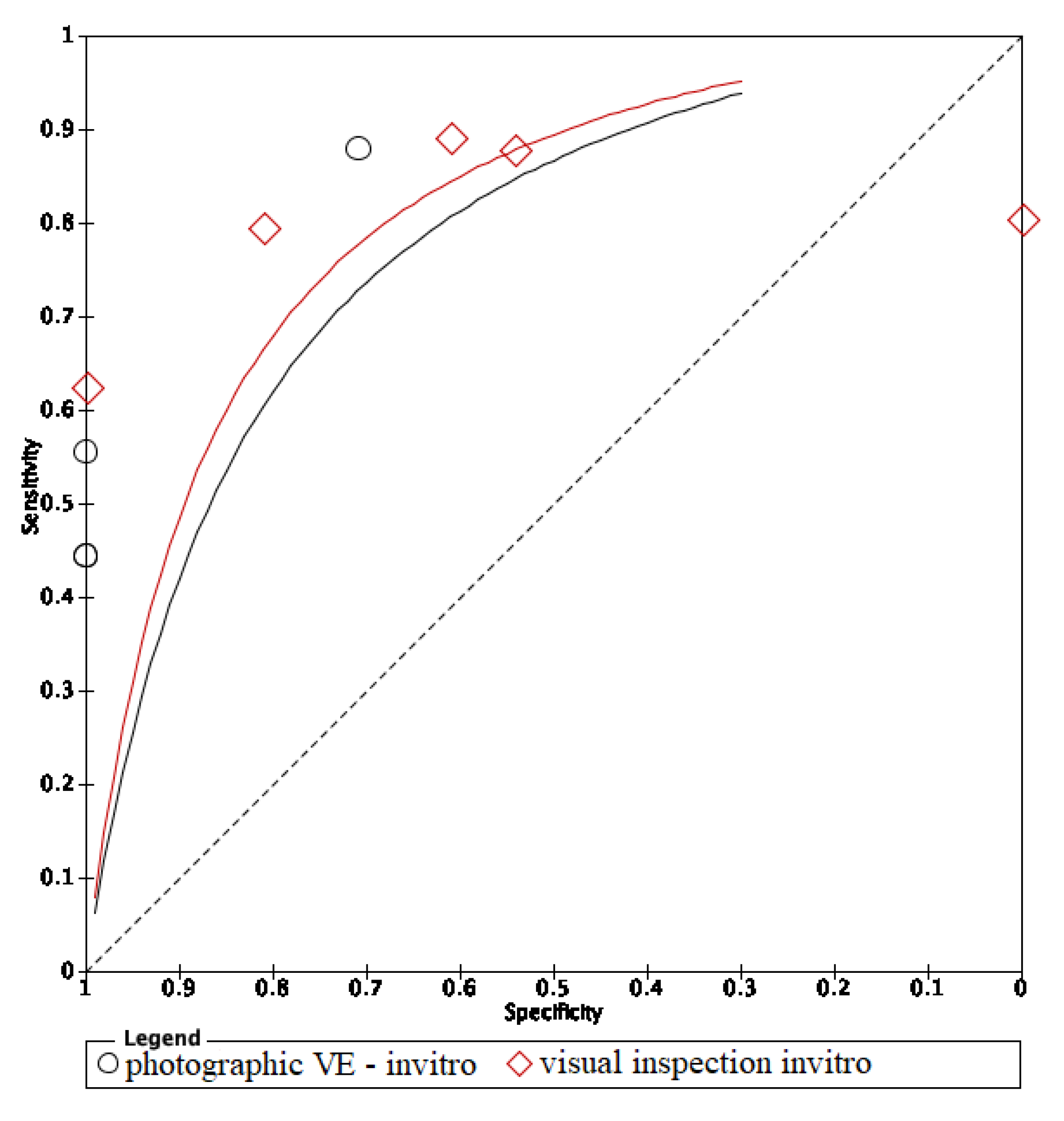
3.5. Summary Receiver Operating Characteristic (sROC) Curves
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. PubMed Search

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Search Name | Search Query | Type of Search | Results |
|---|---|---|---|
| #1 | Search ((((((sensitive and specificity[MeSH Terms])) OR (sensitivity[Title/Abstract] AND specificity[Title/Abstract] OR sensitivity[Title/Abstract] AND standard[Title/Abstract] OR specificity[Title/Abstract] OR screening[Title/Abstract] OR false positive[Title/Abstract] OR false negative[Title/Abstract] OR accuracy[Title/Abstract])) OR predictive value of tests[MeSH Terms]) OR (predictive value[Title/Abstract] OR predictive value of tests[Title/Abstract] OR predictive value of standard[Title/Abstract] OR predictive values[Title/Abstract] OR reference value[Title/Abstract] OR reference values[Title/Abstract] OR reference values[Title/Abstract] OR reference standards[Title/Abstract])) OR roc curve[MeSH Terms]) OR (roc[Title/Abstract] OR roc analyses[Title/Abstract] OR roc analysis[Title/Abstract] OR roc area[Title/Abstract] OR roc auc[Title/Abstract] OR roc characteristics[Title/Abstract] OR roc curve method[Title/Abstract] OR roc estimated[Title/Abstract] OR roc evaluation[Title/Abstract] OR likelihood ratio[Title/Abstract]) | MeSH terms Title/Abstract | 1,529,366 |
| #2 | Search ((initial caries OR white spots[MeSH Terms])) OR (caries in early phase[Title/Abstract] OR initial phase of dental caries[Title/Abstract] OR first stage of tooth decay[Title/Abstract] OR White Spots[Title/Abstract] OR first stage of cavities[Title/Abstract] OR decay on the surface of the teeth[Title/Abstract] OR early stages caries[Title/Abstract] OR early stages decay[Title/Abstract] OR Early stage of carious lesion[Title/Abstract] OR early tooth decay[Title/Abstract] OR Early-stage tooth decay[Title/Abstract] OR initial phase of tooth decay[Title/Abstract]) | MeSH terms Title/Abstract | 46,540 |
| #3 | Search (((system[Title/Abstract] OR clinical[Title/Abstract] OR clinic[Title/Abstract] OR exams[Title/Abstract] OR examination[Title/Abstract] OR examinations[Title/Abstract] OR visual[Title/Abstract] OR inspection[Title/Abstract])) OR (laser fluorescence[Title/Abstract] OR DIAGNOdent[Title/Abstract] OR infrared[Title/Abstract] OR diode laser fluorescence[Title/Abstract] OR QLF[Title/Abstract] OR quantitative light-induced fluorescence system[Title/Abstract] OR quantitative light-induced fluorescence[Title/Abstract] OR fluorescence-bases methods[Title/Abstract] OR fluorescence camera[Title/Abstract] OR VistaProof-FC[Title/Abstract] OR VistaProof[Title/Abstract])) OR (“photographic[Title/Abstract] OR smartphone based method[Title/Abstract] OR photography[Title/Abstract] OR smartphone images[Title/Abstract] OR smartphone photograph[Title/Abstract] OR oral photographic [Title/Abstract] OR smartphone-based detection[Title/Abstract] OR smartphone-based diagnostics[Title/Abstract] OR image-based detection[Title/Abstract] OR smartphone-based tool[Title/Abstract] OR smartphone-based screening”[Title/Abstract]) | Title/Abstract | 8,967,806 |
| #4 | #1 AND #2 AND #3 | 684 |
Appendix B. Cochrane Search
| Search Name | Search Query | Type of Search | Results |
|---|---|---|---|
| #1 | Search ((((((sensitive and specificity[MeSH Terms])) OR (sensitivity[Title/Abstract] AND specificity[Title/Abstract] OR sensitivity[Title/Abstract] AND standard[Title/Abstract] OR specificity[Title/Abstract] OR screening[Title/Abstract] OR false positive[Title/Abstract] OR false negative[Title/Abstract] OR accuracy[Title/Abstract])) OR predictive value of tests[MeSH Terms]) OR (predictive value[Title/Abstract] OR predictive value of tests[Title/Abstract] OR predictive value of standard[Title/Abstract] OR predictive values[Title/Abstract] OR reference value[Title/Abstract] OR reference values[Title/Abstract] OR reference values[Title/Abstract] OR reference standards[Title/Abstract])) OR roc curve[MeSH Terms]) OR (roc[Title/Abstract] OR roc analyses[Title/Abstract] OR roc analysis[Title/Abstract] OR roc area[Title/Abstract] OR roc auc[Title/Abstract] OR roc characteristics[Title/Abstract] OR roc curve method[Title/Abstract] OR roc estimated[Title/Abstract] OR roc evaluation[Title/Abstract] OR likelihood ratio[Title/Abstract]) | MeSH terms Title/Abstract | 115,527 |
| #2 | Search ((initial caries OR white spots[MeSH Terms])) OR (caries in early phase[Title/Abstract] OR initial phase of dental caries[Title/Abstract] OR first stage of tooth decay[Title/Abstract] OR White Spots[Title/Abstract] OR first stage of cavities[Title/Abstract] OR decay on the surface of the teeth[Title/Abstract] OR early stages caries[Title/Abstract] OR early stages decay[Title/Abstract] OR Early stage of carious lesion[Title/Abstract] OR early tooth decay[Title/Abstract] OR Early-stage tooth decay[Title/Abstract] OR initial phase of tooth decay[Title/Abstract]) | MeSH terms Title/Abstract | 2480 |
| #3 | Search (((system[Title/Abstract] OR clinical[Title/Abstract] OR clinic[Title/Abstract] OR exams[Title/Abstract] OR examination[Title/Abstract] OR examinations[Title/Abstract] OR visual[Title/Abstract] OR inspection[Title/Abstract])) OR (laser fluorescence[Title/Abstract] OR DIAGNOdent[Title/Abstract] OR infrared[Title/Abstract] OR diode laser fluorescence[Title/Abstract] OR QLF[Title/Abstract] OR quantitative light-induced fluorescence system[Title/Abstract] OR quantitative light-induced fluorescence[Title/Abstract] OR fluorescence-bases methods[Title/Abstract] OR fluorescence camera[Title/Abstract] OR VistaProof-FC[Title/Abstract] OR VistaProof[Title/Abstract])) OR (“photographic[Title/Abstract] OR smartphone based method[Title/Abstract] OR photography[Title/Abstract] OR smartphone images[Title/Abstract] OR smartphone photograph[Title/Abstract] OR oral photographic [Title/Abstract] OR smartphone-based detection[Title/Abstract] OR smartphone-based diagnostics[Title/Abstract] OR image-based detection[Title/Abstract] OR smartphone-based tool[Title/Abstract] OR smartphone-based screening”[Title/Abstract]) | Title/Abstract | 854,978 |
| #4 | #1 AND #2 AND #3 | 113 |
Appendix C. Summary of Characteristics of Included Studies
| Fluorescence Method | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Study ID | Database | N | TP | FP | FN | TN | Method | Primary/Permanent | Tooth Surface | In Vitro/In Vivo | Reference Standard | Cut-Off Value |
| Iranzo-Cortes et al. 2018 [1] | PubMed | 65 | 31 | 4 | 13 | 17 | FC | permanent | smooth | in vitro without frozen | histology | sound (1–1.49); initial caries (1.5–1.99); caries enamel (2–2.49); caries dentine (2.5 or higher) |
| Mansour et al. 2016 [3] | PubMed | 426 | 30 | 15 | 21 | 360 | LF pen | permanent | coronal | in vivo | visual and radiography | sound (0–13); outer half enamel (14–20); internal half enamel (21–29); dentinal (>30) |
| Ozsevik et al. 2015 [4] | Cochrane | 156 | 92 | 23 | 7 | 34 | LFpen | permanent | proximal caries | in vitro frozen | histology | sound (0–9); outer half enamel (9.1–15); internal half enamel (>15) |
| Zeitouny et al. 2014 [5] | PubMed | 164 | 104 | 6 | 8 | 46 | FC | permanent | occlusal | in vivo | visual | sound (shiny green); enamel (red–darker red); dentinal (dark red–red orange) |
| Teo et al. 2014a [6] | PubMed | 102 | 67 | 2 | 11 | 22 | LF pen | primary | occlusal | in vivo | histology | optimal cut off D1:10 |
| Teo et al. 2014a1 [6] | PubMed | 64 | 40 | 10 | 6 | 8 | LF pen | primary | occlusal | in vitro without frozen | histology | optimal cut off D1:10 |
| Achilleos et al. 2013a [7] | PubMed | 38 | 27 | 2 | 9 | 0 | LF pen | permanent | occlusal | in vitro without frozen | histology | sound (0–13); outer half enamel (14–20); internal half enamel (21–29); dentinal (>30) |
| Achilleos et al. 2013a1 [7] | PubMed | 38 | 36 | 2 | 0 | 0 | FC | permanent | occlusal | in vitro without frozen | histology | sound (≤ 1); beginning enamel (1–1.5); deep enamel (2–2.5); dentinal (2.5–5) |
| Seremidi et al. 2012a [9] | PubMed | 107 | 66 | 6 | 17 | 18 | LF pen | permanent | occlusal | in vitro without frozen | histology | sound (<9); enamel (9–44); dentinal (>=44) |
| Seremidi et al. 2012a1 [9] | PubMed | 107 | 71 | 7 | 12 | 17 | FC | permanent | occlusal | in vitro without frozen | histology | sound (<1.3); D1 (1.30); D2 (1.41); D3 (>1.59) |
| Duruturk et al. 2011 [10] | PubMed | 505 | 163 | 105 | 20 | 217 | LF | permanent | occlusal | in vivo | visual | Sound (0–14); enamel (15–20); dentinal (≥21) |
| Matos et al. 2011a [11] | PubMed | 383 | 241 | 6 | 110 | 26 | LFpen | primary | occlusal | in vivo | visual inspection | sound (0–4); NC lesions (>4) |
| Matos et al. 2011a1 [11] | PubMed | 383 | 156 | 3 | 195 | 29 | FC | primary | occlusal | in vivo | visual inspection | sound (0–1.1); NC lesions (>1.1) |
| de Paula et al. 2011a [12] | PubMed | 64 | 40 | 0 | 16 | 8 | LF | permanent | occlusal | in vitro without frozen | histology | sound (0–10); enamel (11–20); dentin (21–99) |
| de Paula et al. 2011a1 [12] | PubMed | 64 | 31 | 0 | 25 | 8 | LF | permanent | occlusal | insitu without frozen | histology | sound (0–10); enamel (11–20); dentin (21–99) |
| Visual Inspection | ||||||||||||
| Study ID | Database | N | TP | FP | FN | TN | Criteria | Primary/Permanent | Tooth Surface | In Vitro/In Vivo | Reference Standard | Examiners’ Experience |
| Iranzo-Cortes et al. 2018 [1] | PubMed | 65 | 35 | 4 | 9 | 17 | ICDAS II | permanent | smooth | in vitro without frozen | histology | novices with training |
| Teo et al. 2014a [6] | PubMed | 102 | 71 | 7 | 7 | 17 | ICDAS | primary | occlusal | in vivo | histology | intermediate with training |
| Teo, et al. 2014a1 [6] | PubMed | 64 | 41 | 7 | 5 | 11 | ICDAS | primary | occlusal | in vitro without frozen | histology | intermediate with training |
| Achilleos, et al. 2013 [7] | PubMed | 38 | 29 | 2 | 7 | 0 | ICDAS | permanent | occlusal | in vitro without frozen | histology | experienced |
| Seremidi et al. 2012a [9] | PubMed | 107 | 73 | 11 | 10 | 13 | Ekstrand | permanent | occlusal | in vitro without frozen | histology | experienced |
| de Paula, et al. 2011a [12] | PubMed | 64 | 35 | 0 | 21 | 8 | permanent | occlusal | in vitro without frozen | histology | intermediate without training | |
| de Paula, et al. 2011a1 [12] | PubMed | 64 | 30 | 1 | 26 | 7 | permanent | occlusal | in situ | histology | intermediate without training | |
Appendix D. The Sensitivity and Specificity of Each Study Included in the Review
Appendix D.1. Visual Inspection

Appendix D.2. Photographic Visual Examination

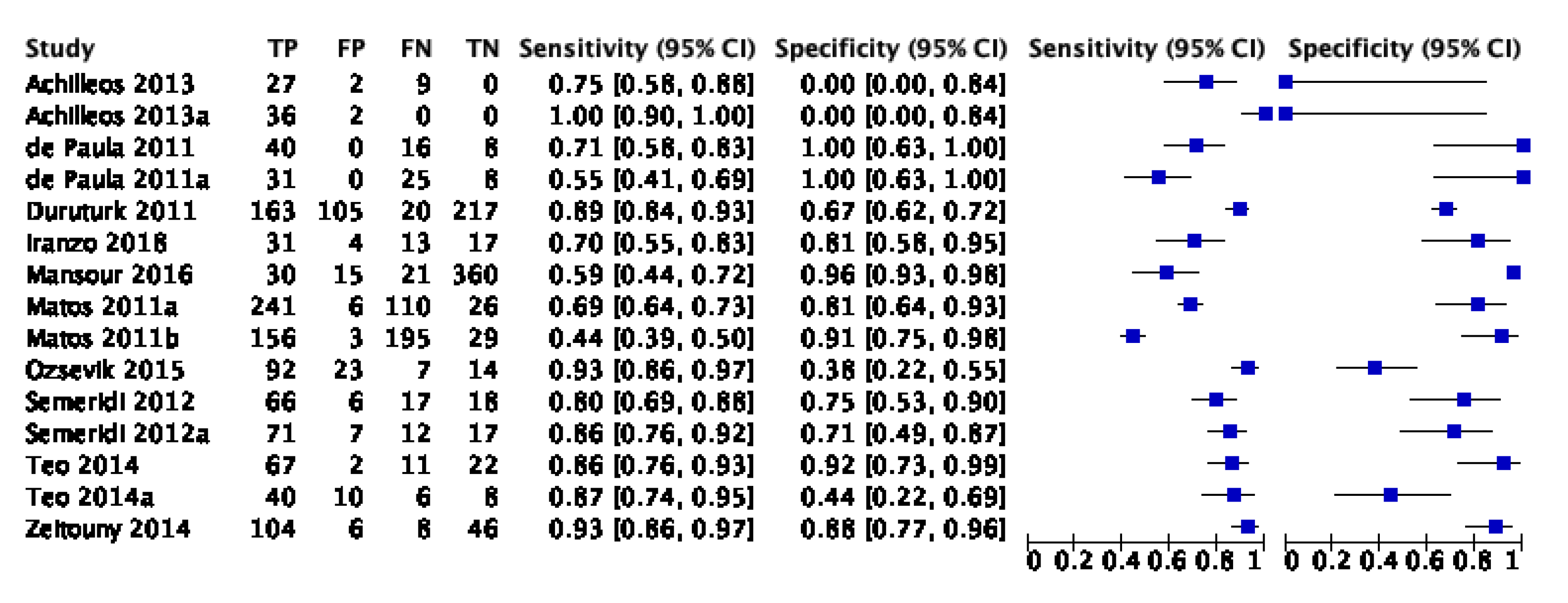
Appendix D.3. Fluorescence-Based Methods

References
- Young, D.A.; Nový, B.B.; Zeller, G.G.; Hale, R.; Hart, T.C.; Truelove, E.L. The American Dental Association Caries Classification System for clinical practice: A report of the American Dental Association Council on Scientific Affairs. J. Am. Dent. Assoc. 2015, 146, 79–86. [Google Scholar] [CrossRef]
- Makhija, S.K.; Gilbert, G.H.; Funkhouser, E.; Bader, J.D.; Gordan, V.V.; Rindal, D.B.; Qvist, V.; Nørrisgaard, P. Twenty-month follow-up of occlusal caries lesions deemed questionable at baseline: Findings from the National Dental Practice-Based Research Network. J. Am. Dent. Assoc. 2014, 145, 1112–1118. [Google Scholar] [CrossRef] [Green Version]
- Nyvad, B. Diagnosis versus detection of caries. Caries Res. 2004, 38, 192–198. [Google Scholar] [CrossRef]
- Holtzman, J.S.; Ballantine, J.; Fontana, M.; Wang, A.; Calantog, A.; Benavides, E.; Gonzalez-Cabezas, C.; Chen, Z.; Wilder-Smith, P. Assessment of early occlusal caries pre- and post-sealant application—An imaging approach. Lasers Surg. Med. 2014, 46, 499–507. [Google Scholar] [CrossRef] [Green Version]
- Rodrigues, J.A.; Lussi, A.; Seemann, R.; Neuhaus, K.W. Prevention of crown and root caries in adults. Periodontology 2000 2011, 55, 231–249. [Google Scholar] [CrossRef] [PubMed]
- Meyer-Lueckel, H.; Paris, S.; Ekstrand, K. Caries Management—Science and Clinical Practice. Stomatol. Edu J. 2015, 2, 170. [Google Scholar] [CrossRef]
- Luong, M.N.; Shimada, Y.; Araki, K.; Yoshiyama, M.; Tagami, J.; Sadr, A. Diagnosis of occlusal caries with dynamic slicing of 3d optical coherence tomography images. Sensors 2020, 20, 1659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abogazalah, N.; Ando, M. Alternative methods to visual and radiographic examinations for approximal caries detection. J. Oral Sci. 2017, 59, 315–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gimenez, T.; Piovesan, C.; Braga, M.M.; Raggio, D.P.; Deery, C.; Ricketts, D.N.; Ekstrand, K.R.; Mendes, F.M. Visual Inspection for Caries Detection: A Systematic Review and Meta-analysis. J. Dent. Res. 2015, 94, 895–904. [Google Scholar] [CrossRef]
- Schwendicke, F.; Tzschoppe, M.; Paris, S. Radiographic caries detection: A systematic review and meta-analysis. J. Dent. 2015, 43, 924–933. [Google Scholar] [CrossRef]
- Hibst, R.; Paulus, R.; Lussi, A. Detection of Occlusal Caries by Laser Fluorescence: Basic and Clinical Investigations. Med. Laser Appl. 2001, 16, 205–213. [Google Scholar] [CrossRef]
- Rodrigues, J.A.; Hug, I.; Diniz, M.B.; Lussi, A. Performance of fluorescence methods, radiographic examination and ICDAS II on occlusal surfaces in vitro. Caries Res. 2008, 42, 297–304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thoms, M. Detection of intaoral lesions using a fluorescence camera. Proc. SPIE Lasers Dent. Xii 2006, 6137, 613705. [Google Scholar] [CrossRef]
- Angmar-Månsson, B.; Ten Bosch, J.J. Quantitative light-induced fluorescence (QLF): A method for assessment of incipient caries lesions. Dento Maxillo Facial Radiol. 2001, 30, 298–307. [Google Scholar] [CrossRef]
- Bader, J.D.; Shugars, D.A.; Bonito, A.J. A systematic review of the performance of methods for identifying carious lesions. J. Public Health Dent. 2002, 62, 201–213. [Google Scholar] [CrossRef] [PubMed]
- Braga, M.M.; Mendes, F.M.; Ekstrand, K.R. Detection activity assessment and diagnosis of dental caries lesions. Dent. Clin. 2010, 54, 479–493. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.; Ioannidis, J.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakane, M.; Kanazawa, H.; Ohara, A. Studies on the active site of papain. VII. States of tryptophan residues. Chem. Pharm. Bull. 1976, 24, 22–25. [Google Scholar] [CrossRef] [Green Version]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Gimenez, T.; Braga, M.M.; Raggio, D.P.; Deery, C.; Ricketts, D.N.; Mendes, F.M. Fluorescence-based methods for detecting caries lesions: Systematic review, meta-analysis and sources of heterogeneity. PLoS ONE 2013, 8, e60421. [Google Scholar] [CrossRef] [Green Version]
- Gomez, J.; Tellez, M.; Pretty, I.A.; Ellwood, R.P.; Ismail, A.I. Non-cavitated carious lesions detection methods: A systematic review. Community Dent. Oral Epidemiol. 2013, 41, 54–66. [Google Scholar] [CrossRef]
- Teo, T.K.; Ashley, P.F.; Louca, C. An in vivo and in vitro investigation of the use of ICDAS, DIAGNOdent pen and CarieScan PRO for the detection and assessment of occlusal caries in primary molar teeth. Clin. Oral Investig. 2014, 18, 737–744. [Google Scholar] [CrossRef]
- Mansour, S.; Ajdaharian, J.; Nabelsi, T.; Chan, G.; Wilder-Smith, P. Comparison of caries diagnostic modalities: A clinical study in 40 subjects. Lasers Surg. Med. 2016, 48, 924–928. [Google Scholar] [CrossRef] [Green Version]
- Zeitouny, M.; Feghali, M.; Nasr, A.; Abou-Samra, P.; Saleh, N.; Bourgeois, D.; Farge, P. SOPROLIFE system: An accurate diagnostic enhancer. Sci. World J. 2014, 2014. [Google Scholar] [CrossRef] [PubMed]
- Wong, H.M.; King, N.M. Diagnosis of developmental defects of enamel made from photographs. Pediatric Dent. J. 2011, 21, 6–16. [Google Scholar] [CrossRef]
- Kohara, E.K.; Abdala, C.G.; Novaes, T.F.; Braga, M.M.; Haddad, A.E.; Mendes, F.M. Is it feasible to use smartphone images to perform telediagnosis of different stages of occlusal caries lesions? PLoS ONE 2018, 13, e0202116. [Google Scholar] [CrossRef]
- Van Hilsen, Z.; Jones, R.S. Comparing potential early caries assessment methods for teledentistry. BMC Oral Health 2013, 13, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seremidi, K.; Lagouvardos, P.; Kavvadia, K. Comparative in vitro validation of VistaProof and DIAGNOdent pen for occlusal caries detection in permanent teeth. Oper. Dent. 2012, 37, 234–245. [Google Scholar] [CrossRef] [PubMed]













| Study | Risk of Bias | Applicability | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Patient Selection | Index Test | Reference Standard | Flow and Timing | Patient Selection | Index Test | Reference Standard | ||||||||
| N | % | n | % | N | % | N | % | N | % | N | % | n | % | |
| High | 9 | 75 | 6 | 50 | 7 | 58 | 1 | 8 | 0 | 0 | 0 | 0 | 0 | 0 |
| Low | 3 | 15 | 4 | 33 | 3 | 25 | 11 | 92 | 12 | 100 | 12 | 100 | 12 | 100 |
| Unclear | 0 | 0 | 2 | 17 | 2 | 17 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Total | 12 | 100 | 12 | 100 | 12 | 100 | 12 | 100 | 12 | 100 | 12 | 100 | 12 | 100 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thanh, M.T.G.; Van Toan, N.; Toan, D.T.T.; Thang, N.P.; Dong, N.Q.; Dung, N.T.; Hang, P.T.T.; Anh, L.Q.; Tra, N.T.; Ngoc, V.T.N. Diagnostic Value of Fluorescence Methods, Visual Inspection and Photographic Visual Examination in Initial Caries Lesion: A Systematic Review and Meta-Analysis. Dent. J. 2021, 9, 30. https://0-doi-org.brum.beds.ac.uk/10.3390/dj9030030
Thanh MTG, Van Toan N, Toan DTT, Thang NP, Dong NQ, Dung NT, Hang PTT, Anh LQ, Tra NT, Ngoc VTN. Diagnostic Value of Fluorescence Methods, Visual Inspection and Photographic Visual Examination in Initial Caries Lesion: A Systematic Review and Meta-Analysis. Dentistry Journal. 2021; 9(3):30. https://0-doi-org.brum.beds.ac.uk/10.3390/dj9030030
Chicago/Turabian StyleThanh, Mai Thi Giang, Ngo Van Toan, Do Thi Thanh Toan, Nguyen Phu Thang, Ngoc Quang Dong, Nguyen Tien Dung, Phung Thi Thu Hang, Le Quynh Anh, Nguyen Thu Tra, and Vo Truong Nhu Ngoc. 2021. "Diagnostic Value of Fluorescence Methods, Visual Inspection and Photographic Visual Examination in Initial Caries Lesion: A Systematic Review and Meta-Analysis" Dentistry Journal 9, no. 3: 30. https://0-doi-org.brum.beds.ac.uk/10.3390/dj9030030