
Clinical Pilot Series of Non-Self-Contained Periodontal Infrabony Defects Treated with a Slowly Resorbable Bovine Pericardium Membrane in Combination with Low-Temperature-Treated Decellularized Bovine Bone Particles

 , and
, and
Abstract
:1. Introduction
2. Case Series
2.1. Patient Information
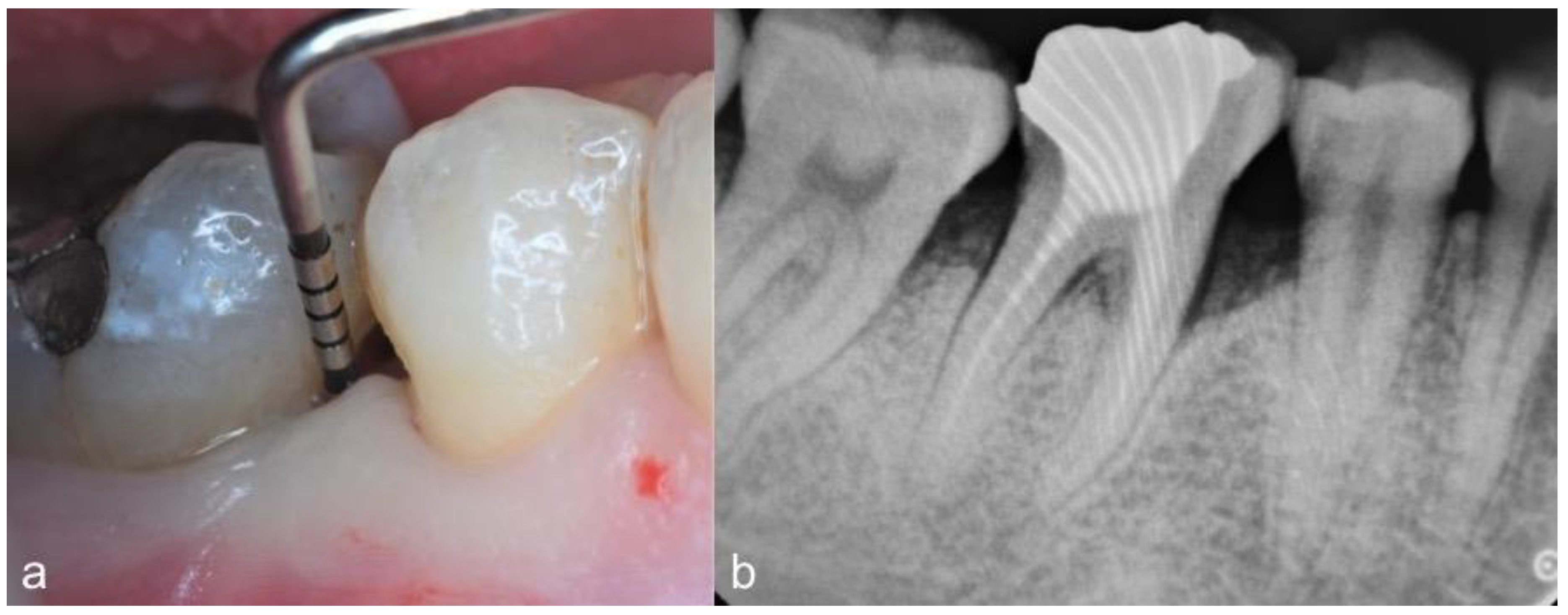
2.2. Clinical Findings
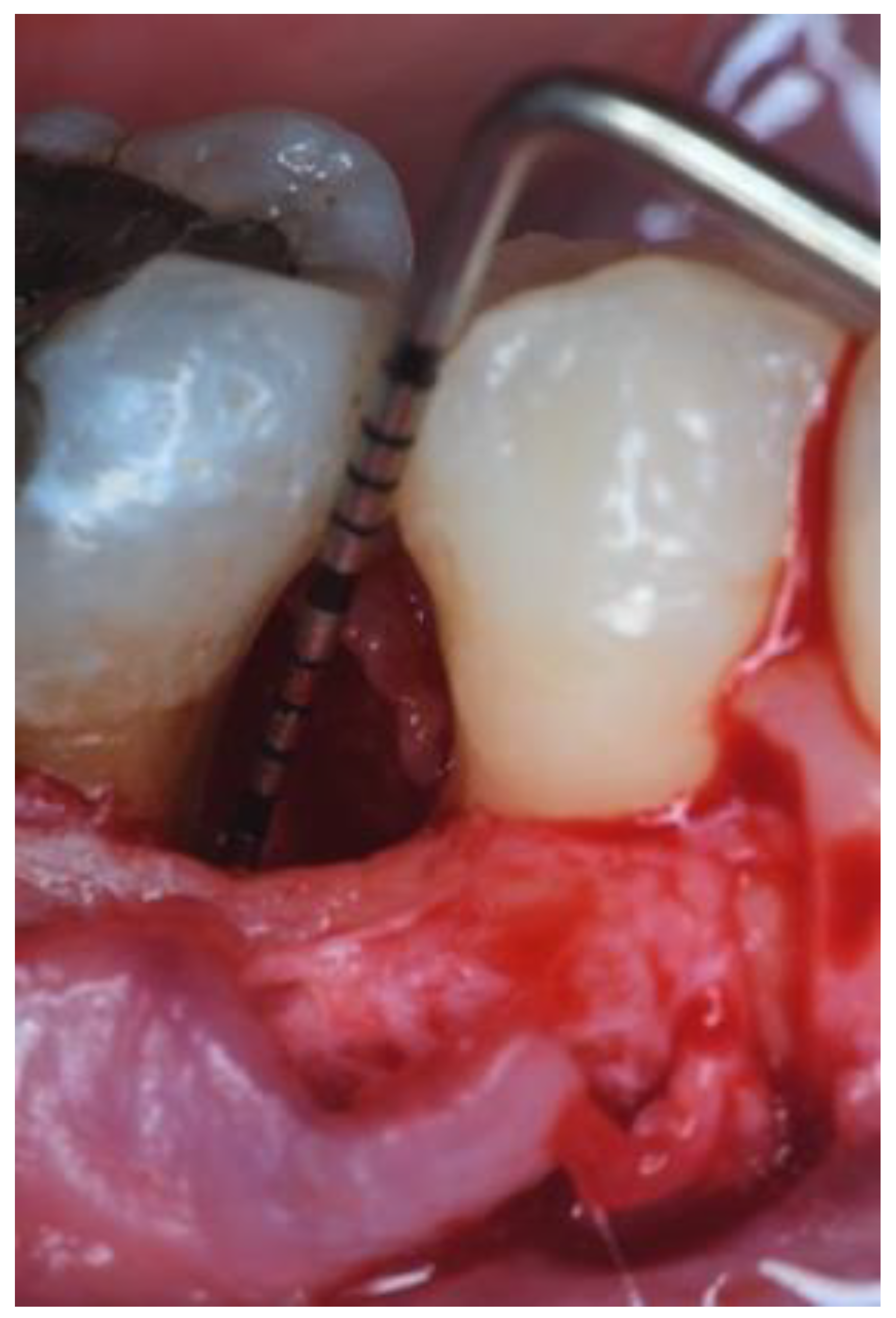
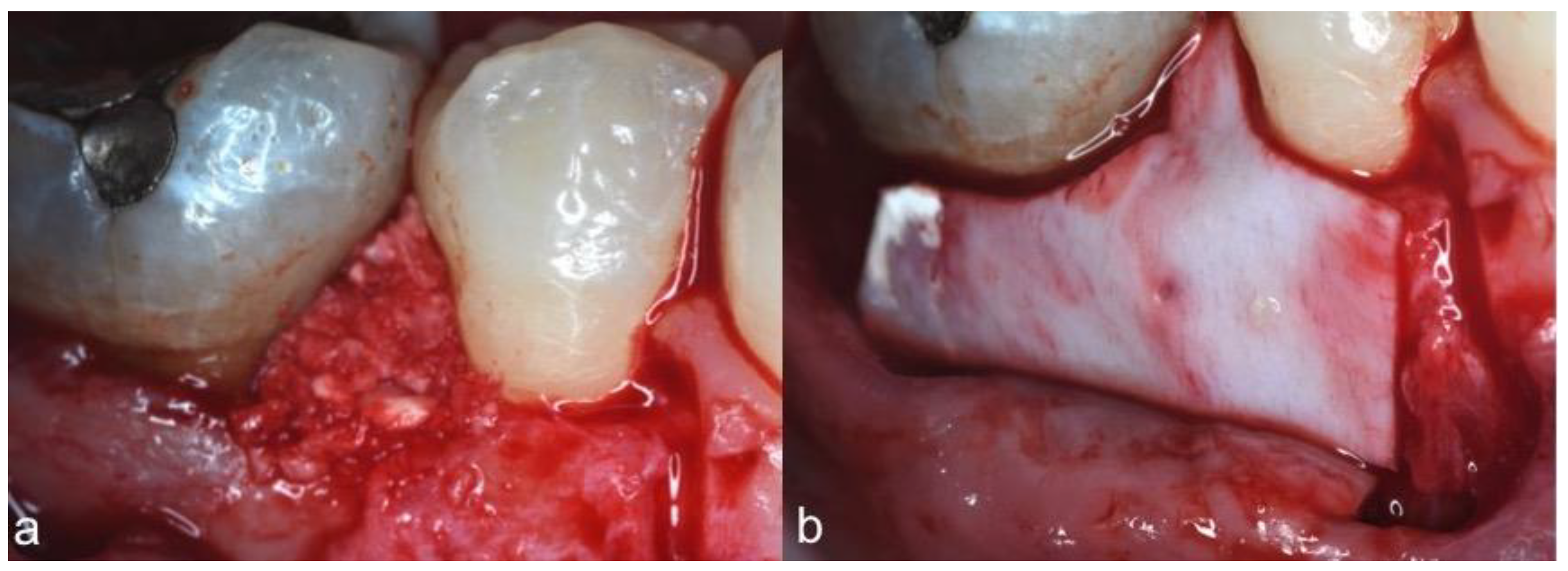
2.3. Therapeutic Intervention
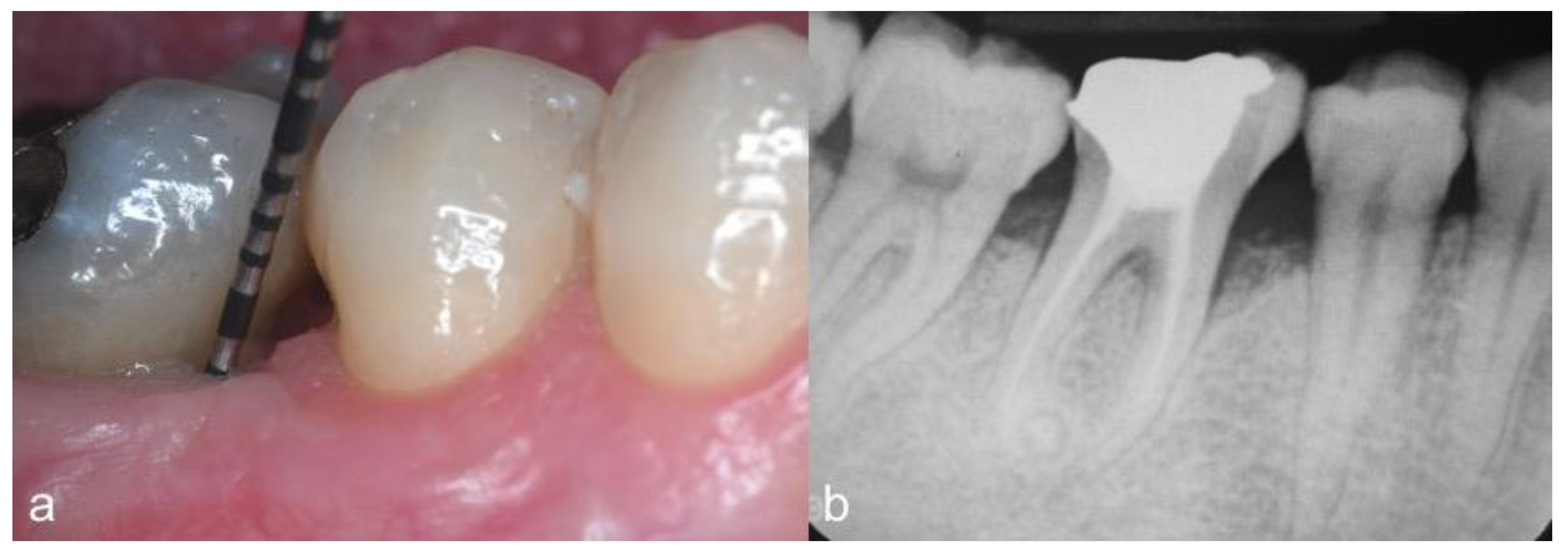
2.4. Follow-Up and Outcomes
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Loos, B.G.; Needleman, I. Endpoints of active periodontal therapy. J. Clin. Periodontol. 2020, 47, 61–71. [Google Scholar] [CrossRef] [Green Version]
- Tonetti, M.S.; Bottenberg, P.; Conrads, G.; Eickholz, P.; Heasman, P.; Huysmans, M.C.; López, R.; Madianos, P.; Müller, F.; Needleman, I.; et al. Dental caries and periodontal diseases in adult Lithuanians. Periodontol 2017, 44, S135–S144. [Google Scholar] [CrossRef] [Green Version]
- Papapanou, P.N.; Wennstrom, J.L. The angular bony defect as indicator of further alveolar bone loss. J. Clin. Periodontol. 1991, 18, 317–322. [Google Scholar] [CrossRef] [PubMed]
- Tu, Y.K.; Woolston, A.; Faggion, C.M. Do bone grafts or barrier membranes provide additional treatment effects for infrabony lesions treated with enamel matrix derivatives? A network meta-analysis of randomized-controlled trials. J. Clin. Periodontol. 2010, 37, 59–79. [Google Scholar] [CrossRef] [PubMed]
- Nibali, L.; Koidou, V.P.; Nieri, M.; Barbato, L.; Pagliaro, U.; Cairo, F. Regenerative surgery versus access flap for the treatment of intrabony periodontal defects. A systematic review and metaanalysis. J. Clin. Periodontol. 2020, 47, 320–351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cortellini, P.; Tonetti, M.S. Clinical concepts for regenerative therapy in intrabony defects. Periodontol. 2000 2015, 68, 282–307. [Google Scholar] [CrossRef] [PubMed]
- Stavropoulos, A.; Chiantella, G.; Costa, D.; Steigmann, M.; Windisch, P.; Sculean, A. Clinical and histologic evaluation of a granular bovine bone biomaterial used as an adjunct to GTR with a bioresorbable bovine pericardium collagen membrane in the treatment of intrabony defects. J. Periodontol. 2011, 82, 462–470. [Google Scholar] [CrossRef]
- Mancini, L.; Romandini, M.; Fratini, A.; Americo, L.M.; Panda, S.; Marchetti, E. Biomaterials for periodontal and peri-implant regeneration. Materials 2021, 14, 3319. [Google Scholar] [CrossRef]
- Scarano, A. Maxillary sinus augmentation with decellularized bovine compact particles: A radiological, clinical, and histologic report of 4 cases. Biomed. Res. Int. 2017, 2017, 2594670. [Google Scholar] [CrossRef]
- Sbricoli, L.; Guazzo, R.; Annunziata, M.; Gobbato, L.; Bressan, E.; Nastri, L. Selection of collagen membranes for bone regeneration: A Literature Review. Materials 2020, 13, 786. [Google Scholar] [CrossRef] [Green Version]
- Aurer, A.; Jorgic-Srdjak, K. Membranes for periodontal regeneration. Acta Stomatol. Croat. 2005, 39, 107–112. [Google Scholar]
- Singh, A.K. GTR membranes: The barriers for periodontal regeneration. DHR Int. J. Med. Sci. 2013, 4, 31–38. [Google Scholar]
- Ludovichetti, F.S.; Ludovichetti, M. Utilizzo di osso bovino decellularizzato e delipidato e di una membrana in pericardio per la rigenerazione di alveoli post-estrattivi e successiva riabilitazione implanto-protesica: Risultati clinici e istologici. Dent. Trib. Ital. Ed. 2020, 4, 22–23. [Google Scholar]
- Sanz, M.; Herrera, D.; Kebschull, M.; Chapple, I.; Jepsen, S.; Berglundh, T.; Sculean, A.; Tonetti, M.S. EFP workshop participants and methodological consultants. Treatment of stage I-III periodontitis—The EFP S3 level clinical practice guideline. J. Clin. Periodontol. 2020, 47, 4–60. [Google Scholar] [CrossRef]
- Marini, L.; Sahrmann, P.; Rojas, M.A.; Cavalcanti, C.; Pompa, G.; Papi, P.; Pilloni, A. Early Wound Healing Score (EHS): An intra- and inter-examiner reliability study. Dent. J. 2019, 7, 86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cortellini, P.; Pini Prato, G.; Tonetti, M. The simplified papilla preservation flap: A novel surgical approach for the management of the soft tissues in regenerative procedures. Int. J. Periodontics Restor. Dent. 1999, 19, 589–599. [Google Scholar]
- Cortellini, P.; Pini Prato, G.; Tonetti, M. The modified papilla preservation technique: A new surgical approach for interproxymal regenerative procedures. J. Periodontol. 1995, 66, 261–266. [Google Scholar] [CrossRef]
- Rakmanee, T.; Griffiths, G.S.; Auplish, G.; Darbar, U.; Petrie, A.; Olsen, I.; Donos, N. Treatment of intrabony defects with guided tissue regeneration in aggressive periodontitis: Clinical outcomes at 6 and 12 months. Clin. Oral Investig. 2016, 20, 1217–1225. [Google Scholar] [CrossRef] [PubMed]
- Cieplik, F.; Ihlenfeld, I.; Hiller, K.A.; Pummer, A.; Schmalz, G.; Buchalla, W.; Christgau, M. Tooth survival and clinical outcomes up to 26 years after guided tissue regeneration therapy in deep intra-bony defects: Follow-up investigation of three randomized clinical trials. J. Clin. Periodontol. 2020, 4, 863–874. [Google Scholar] [CrossRef] [PubMed]
- Cortellini, P.; Pini Prato, G.; Tonetti, M.S. Periodontal regeneration of human intrabony defects with bioresorbable membranes. A controlled clinical trial. J. Periodontol. 1996, 67, 217–223. [Google Scholar] [CrossRef]
- Christgau, M.; Schmalz, G.; Wenzel, A.; Hiller, K.A. Periodontal regeneration of intrabony defects with resorbable and non-resorbable membranes: 30-month results. J. Clin. Periodontol. 1997, 24, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Camargo, P.M.; Lekovic, V.; Weinlaender, M.; Nedic, M.; Vasilic, N.; Wolinsky, L.E.; Kenney, E.B. A controlled re-entry study on the effectiveness of bovine porous bone mineral used in combination with a collagen membrane of porcine origin in the treatment of intrabony defects in humans. J. Clin. Periodontol. 2000, 27, 889–896. [Google Scholar] [CrossRef]
- Smith, C.A.; Richardson, S.M.; Eagle, M.J.; Rooney, P.; Board, T.; Hoyland, J.A. The use of a novel bone allograft wash process to generate a biocompatible, mechanically stable and osteoinductive biological scaffold for use in bone tissue engineering. J. Tissue Eng. Regen. Med. 2015, 9, 595–604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramseier, C.A.; Rasperini, G.; Batia, S.; Giannobile, W.V. Advanced regenerative technologies for periodontal tissue repair. Periodontol. 2000 2012, 59, 185–202. [Google Scholar] [CrossRef] [Green Version]
- Hutmacher, D.; Hürzeler, M.B.; Schliephake, H. A review of material properties of biodegradable and bioresorbable polymers and devices for GTR and GBR applications. Int. J. Oral Maxillofac. Implants 1996, 11, 667–678. [Google Scholar] [PubMed]
- Polimeni, G.; Xiropaidis, A.V.; Wikesjö, U.M. Biology and principles of periodontal wound healing/regeneration. Periodontol. 2000 2006, 41, 30–47. [Google Scholar] [CrossRef]
- Magnusson, I.; Batich, C.; Collins, B.R. New attachment formation following controlled tissue regeneration using biodegradable membranes. J. Periodontol. 1988, 59, 1–6. [Google Scholar] [CrossRef]
- Rojas, M.A.; Marini, L.; Pilloni, A.; Sahrmann, P. Early wound healing outcomes after regenerative periodontal surgery with enamel matrix derivatives or guided tissue regeneration: A systematic review. BMC Oral Health 2019, 19, 76. [Google Scholar] [CrossRef]
- Sculean, A.; Nikolidakis, D.; Nikou, G.; Ivanovic, A.; Chapple, I.L.; Stavropoulos, A. Biomaterials for promoting periodontal regeneration in human intrabony defects: A systematic review. Periodontol. 2000 2015, 68, 182–216. [Google Scholar] [CrossRef]
- Trombelli, L.; Farina, R.; Franceschetti, G.; Calura, G. Single flap approach with buccal access in periodontal reconstructive procedures. J. Periodontol. 2009, 80, 353–360. [Google Scholar] [CrossRef]
- Shirakata, Y.; Imafuji, T.; Nakamura, T.; Kawakami, Y.; Shinohara, Y.; Noguchi, K.; Pilloni, A.; Sculean, A. Periodontal wound healing/regeneration of two-wall intrabony defects following reconstructive surgery with cross-linked hyaluronic acid-gel with or without a collagen matrix: A preclinical study in dogs. Quintessence Int. 2021, 308–316. [Google Scholar] [CrossRef]
- Sculean, A.; Kiss, A.; Miliauskaite, A.; Schwarz, F.; Arweiler, N.B.; Hannig, M. Ten-year results following treatment of intra-bony defects with enamel matrix proteins and guided tissue regeneration. J. Clin. Periodontol. 2008, 35, 817–824. [Google Scholar] [CrossRef] [PubMed]
- Pilloni, A.; Rojas, M.A.; Marini, L.; Russo, P.; Shirakata, Y.; Sculean, A.; Iacono, R. Healing of intrabony defects following regenerative surgery by means of single-flap approach in conjunction with either hyaluronic acid or an enamel matrix derivative: A 24-month randomized controlled clinical trial. Clin. Oral Investig. 2021, 25, 5095–5107. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Tooth | Site | Baseline | Follow-Up | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| PD (mm) | REC (mm) | CAL (mm) | BoP (+/−) | PD (mm) | REC (mm) | CAL (mm) | BoP (+/−) | EHS | |||
| Anterior teeth | |||||||||||
| 1 | 1.3 | DV | 8 | 3 | 11 | − | 4 | 3 | 7 | − | 8 |
| 2 | 1.1 | MP | 10 | 0 | 10 | + | 4 | 2 | 6 | − | 9 |
| 3 | 1.1 | DP | 8 | 0 | 8 | − | 4 | 1 | 5 | − | 8 |
| 4 | 1.1 | MV | 6 | 0 | 6 | − | 3 | 1 | 4 | − | 10 |
| Posterior teeth | |||||||||||
| 5 | 4.6 | DV | 9 | 0 | 9 | + | 5 | 1 | 6 | + | 7 |
| 6 | 4.6 | ML | 11 | 0 | 11 | + | 4 | 2 | 6 | − | 8 |
| 7 | 4.6 | DV | 9 | 0 | 9 | − | 5 | 1 | 6 | − | 7 |
| 8 | 4.6 | MV | 9 | 0 | 9 | + | 3 | 2 | 5 | − | 8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rojas, M.A.; Marini, L.; Russo, P.; Blardi, V.; Schmidlin, P.R.; Pilloni, A. Clinical Pilot Series of Non-Self-Contained Periodontal Infrabony Defects Treated with a Slowly Resorbable Bovine Pericardium Membrane in Combination with Low-Temperature-Treated Decellularized Bovine Bone Particles. Dent. J. 2021, 9, 110. https://0-doi-org.brum.beds.ac.uk/10.3390/dj9100110
Rojas MA, Marini L, Russo P, Blardi V, Schmidlin PR, Pilloni A. Clinical Pilot Series of Non-Self-Contained Periodontal Infrabony Defects Treated with a Slowly Resorbable Bovine Pericardium Membrane in Combination with Low-Temperature-Treated Decellularized Bovine Bone Particles. Dentistry Journal. 2021; 9(10):110. https://0-doi-org.brum.beds.ac.uk/10.3390/dj9100110
Chicago/Turabian StyleRojas, Mariana A., Lorenzo Marini, Paola Russo, Vittorio Blardi, Patrick R. Schmidlin, and Andrea Pilloni. 2021. "Clinical Pilot Series of Non-Self-Contained Periodontal Infrabony Defects Treated with a Slowly Resorbable Bovine Pericardium Membrane in Combination with Low-Temperature-Treated Decellularized Bovine Bone Particles" Dentistry Journal 9, no. 10: 110. https://0-doi-org.brum.beds.ac.uk/10.3390/dj9100110